Trends in Suicide Mortality in South Africa, 1997 to 2016


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Data Management
2.2. Statistical Analysis
3. Results
3.1. Description of the Study Population
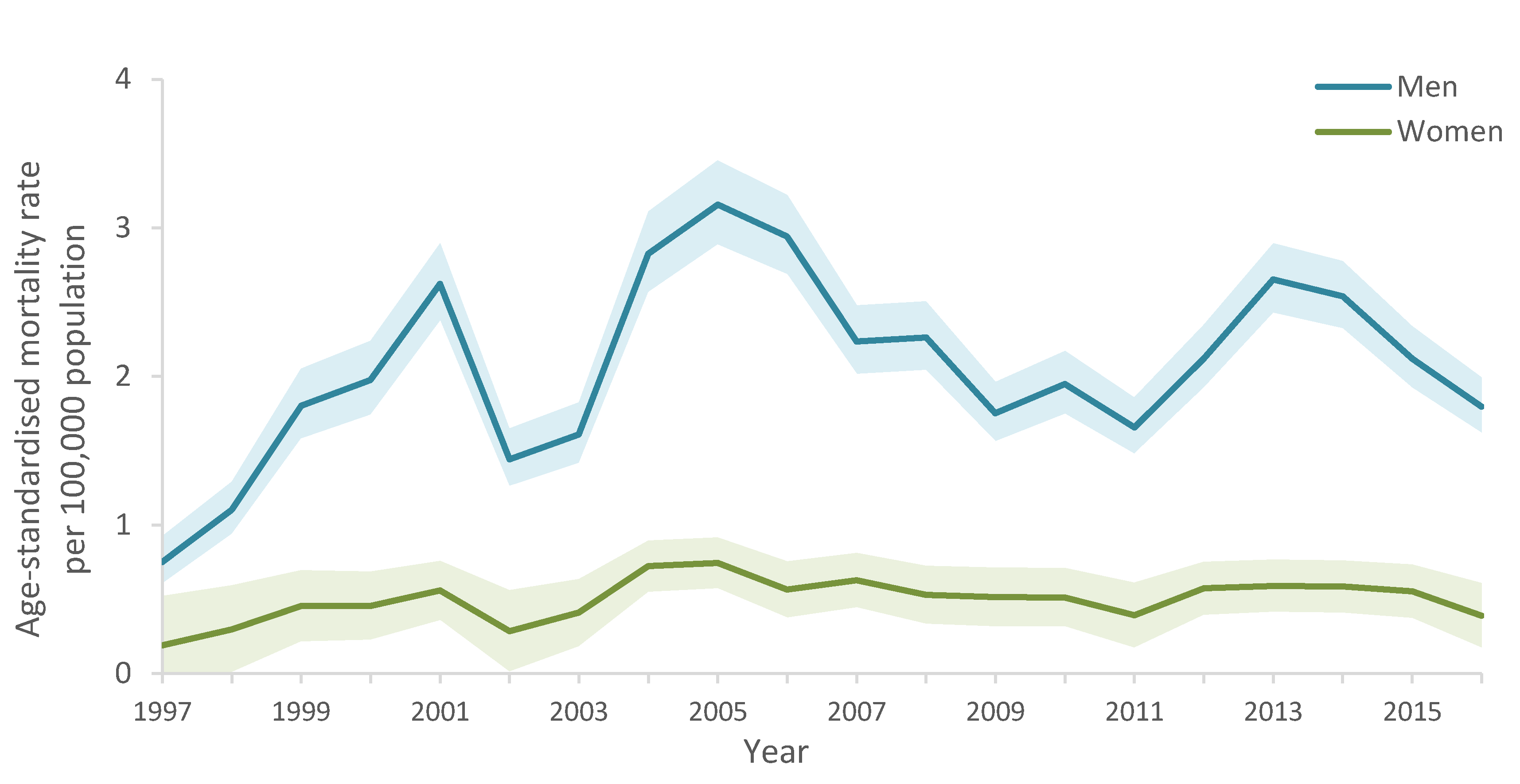
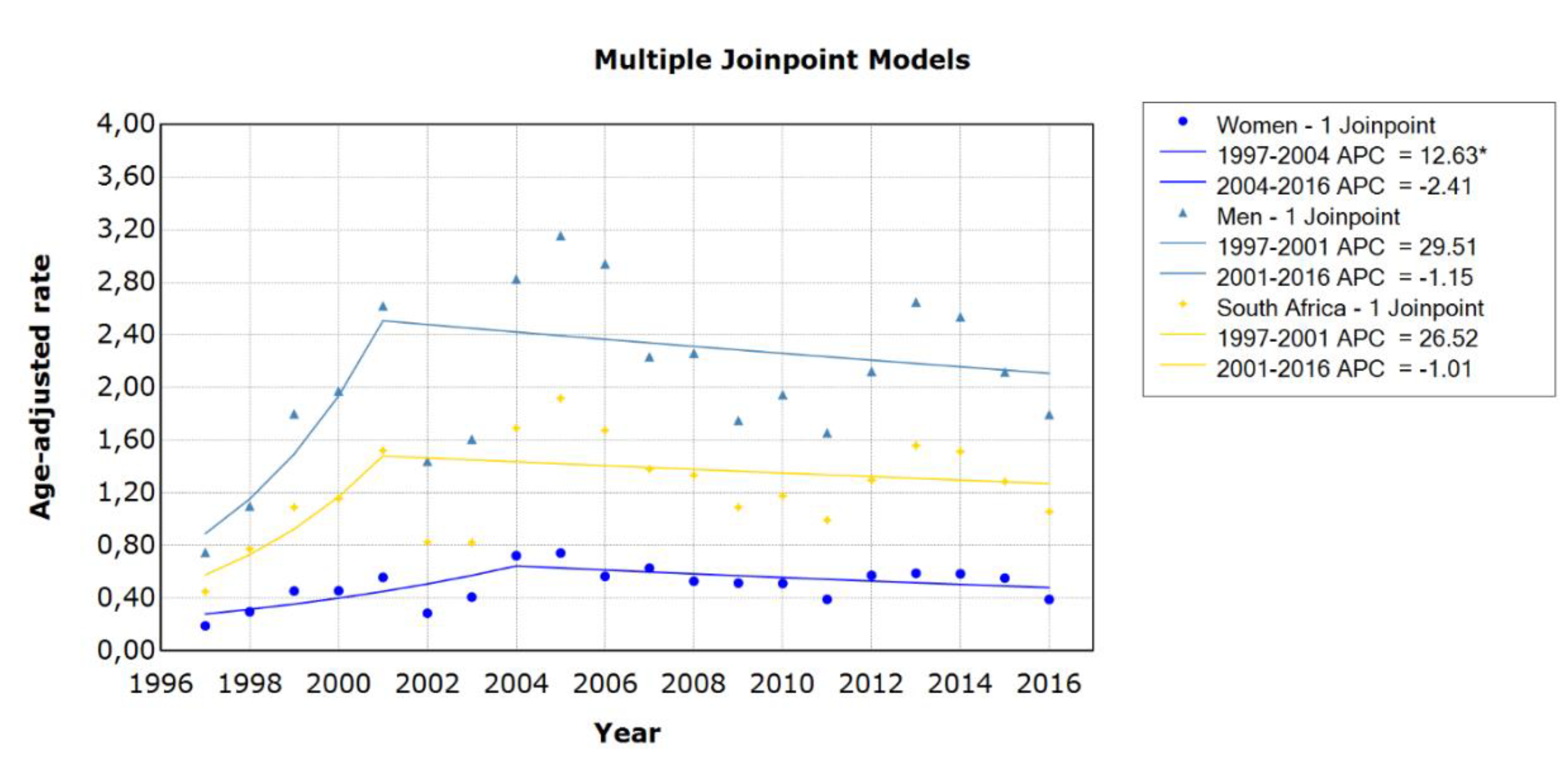
3.2. Trends in Suicide Mortality
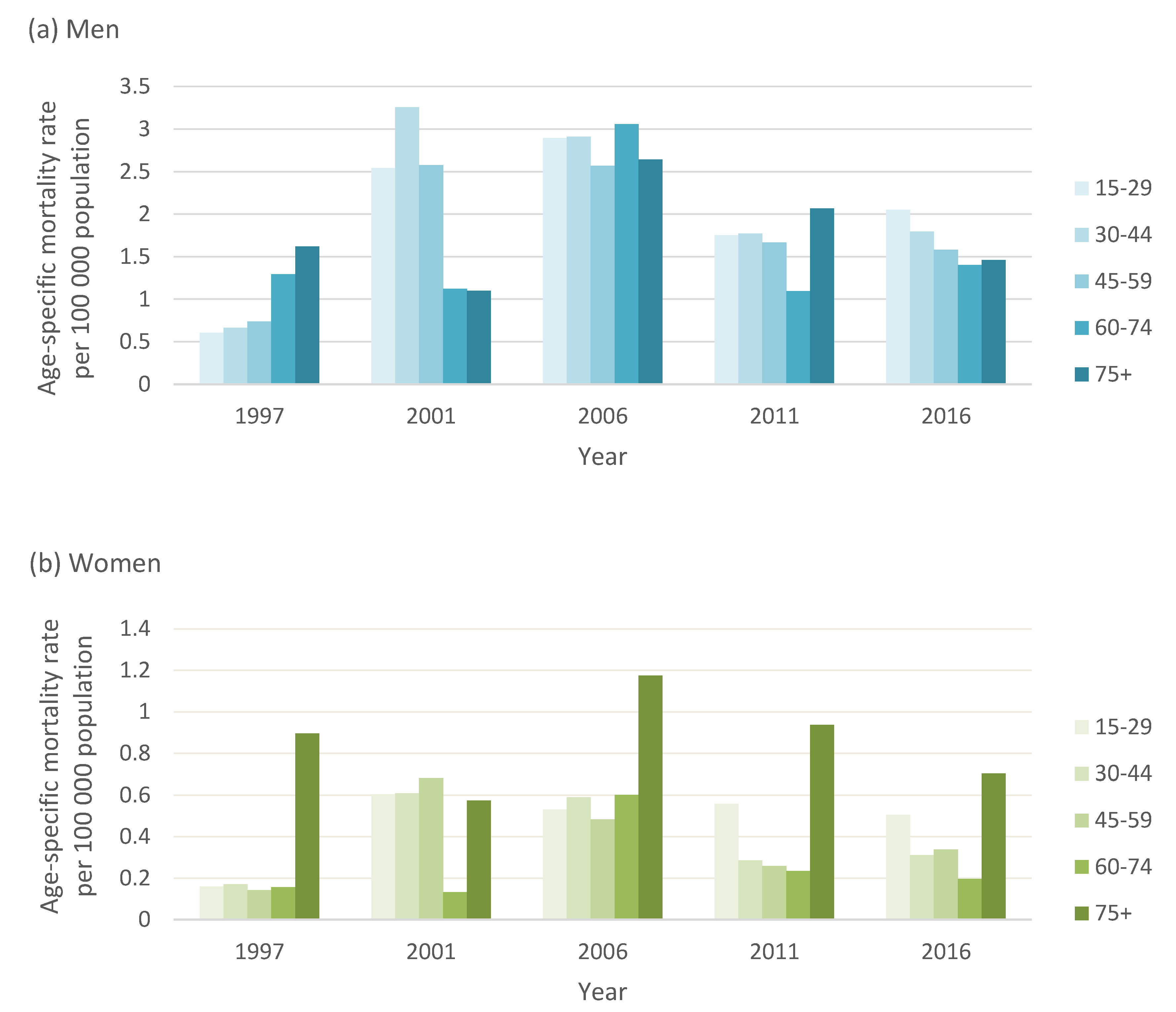
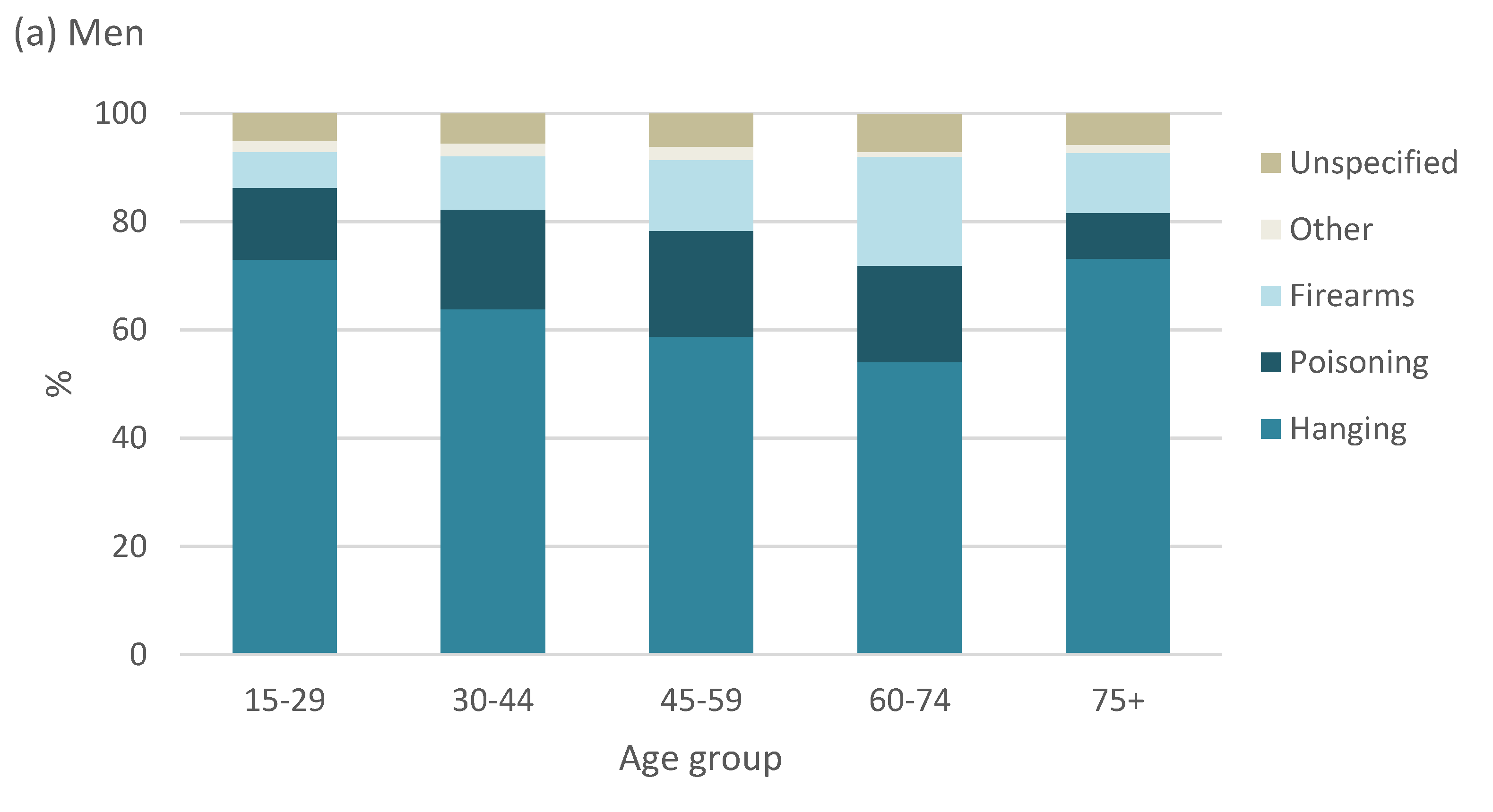
3.3. Suicide Patterns by Age
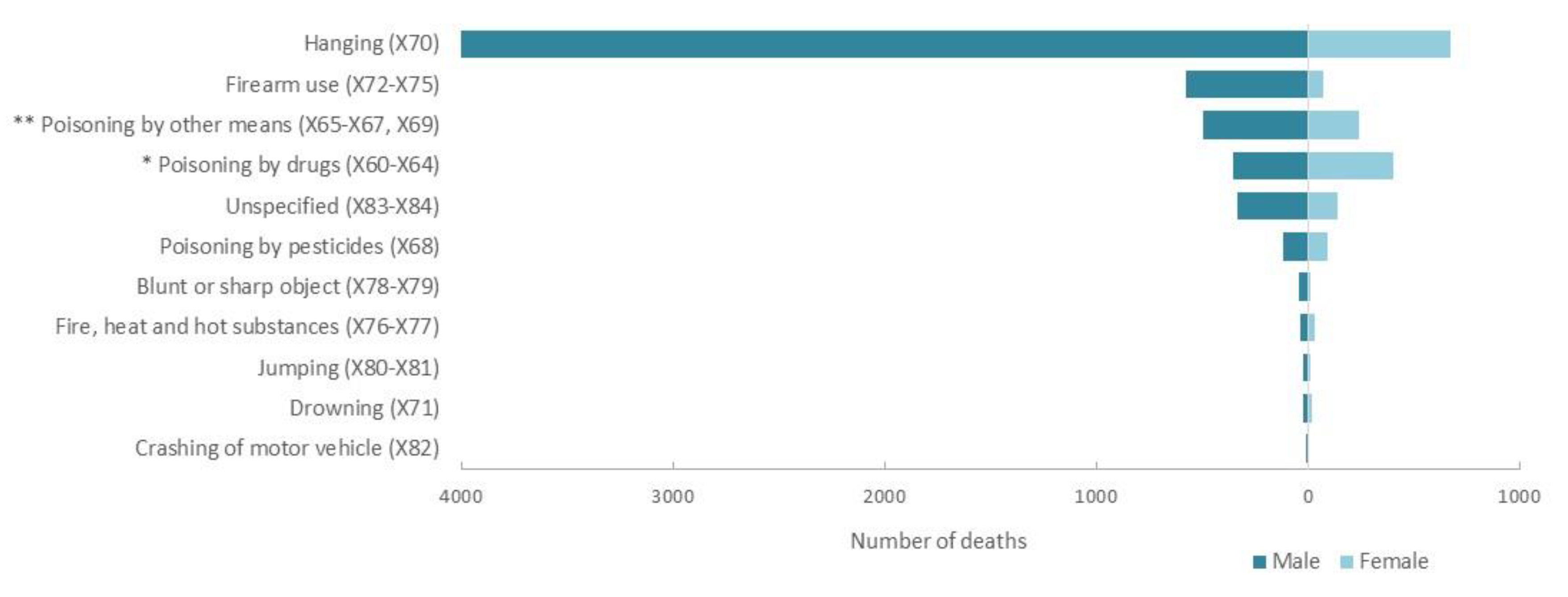
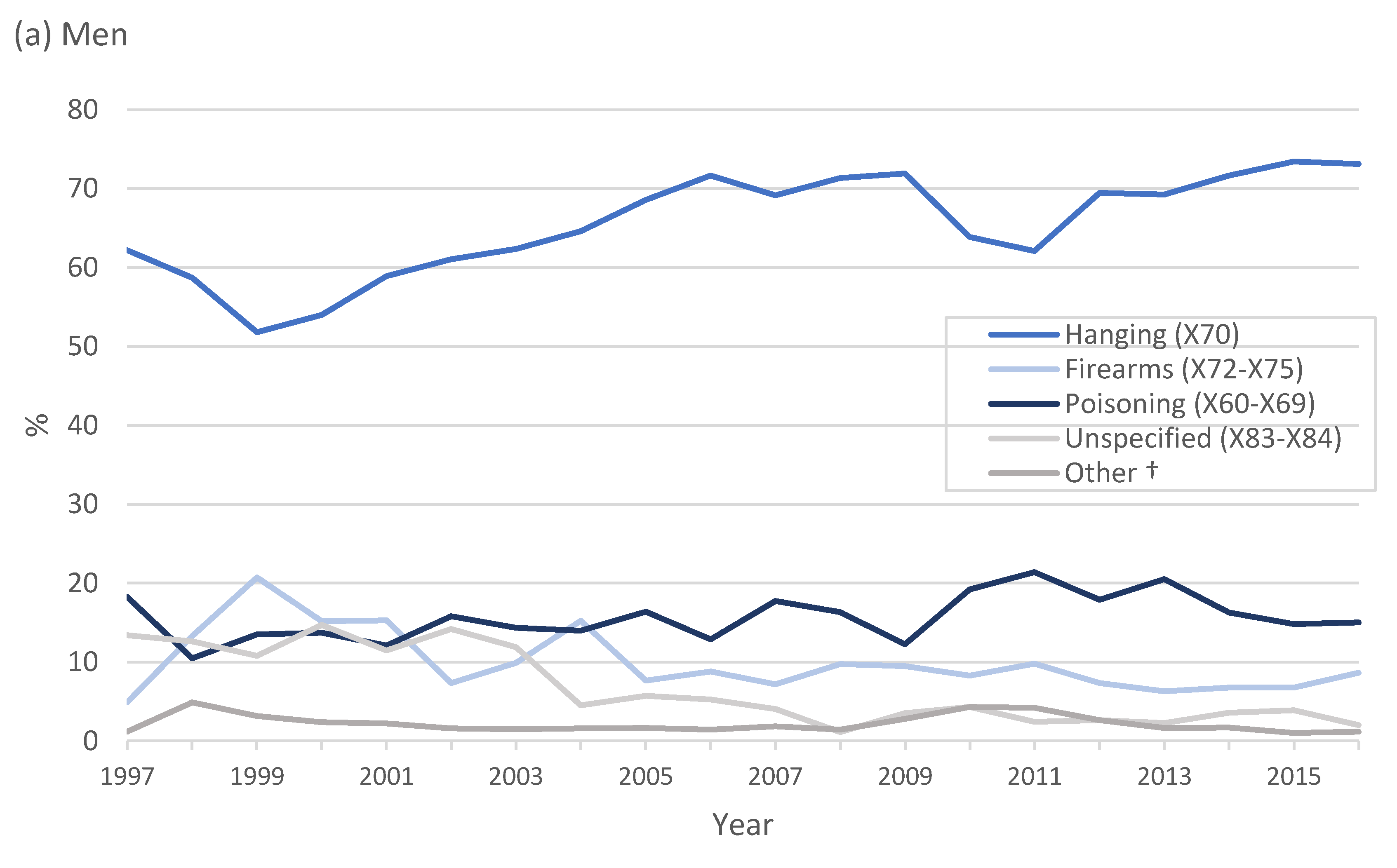
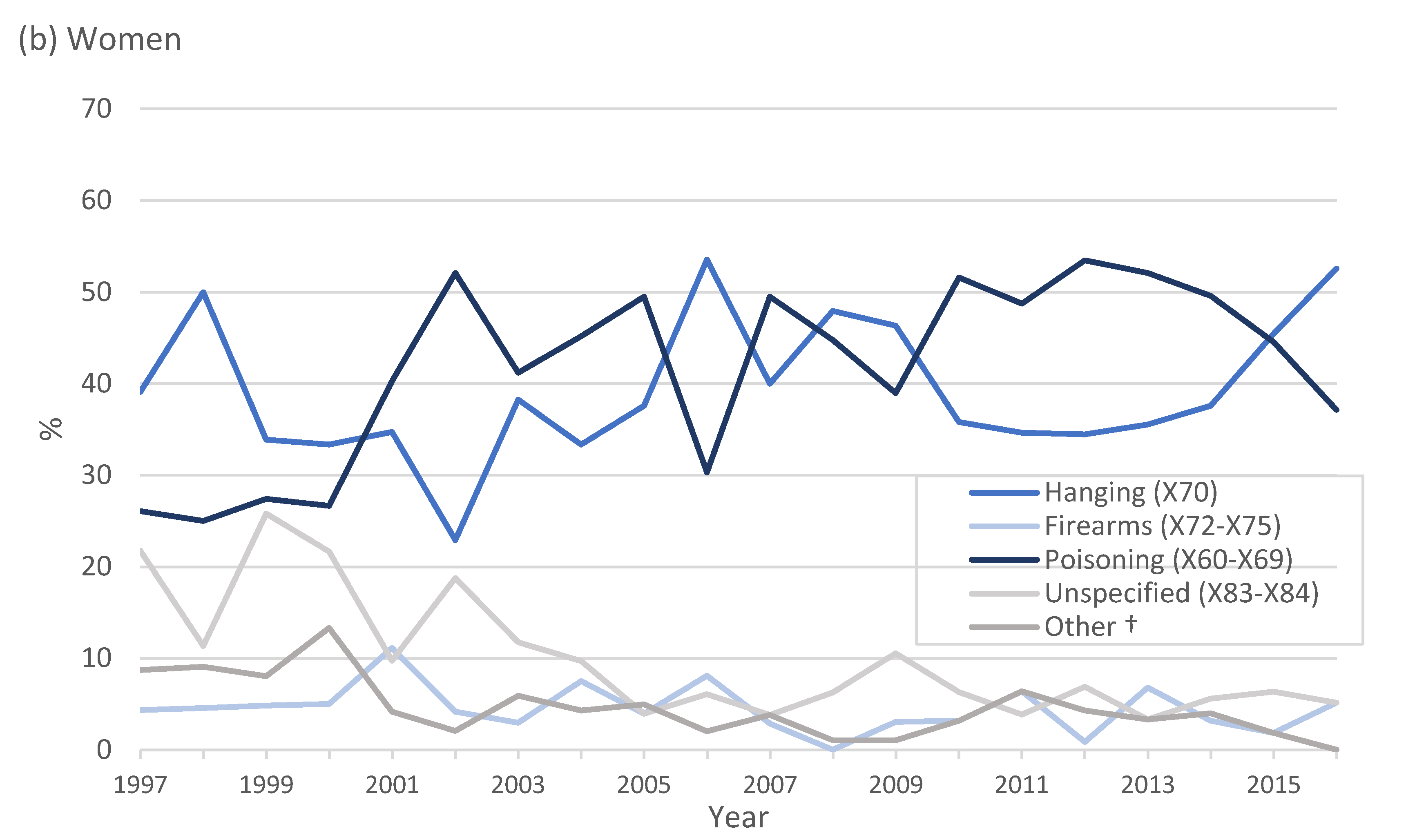
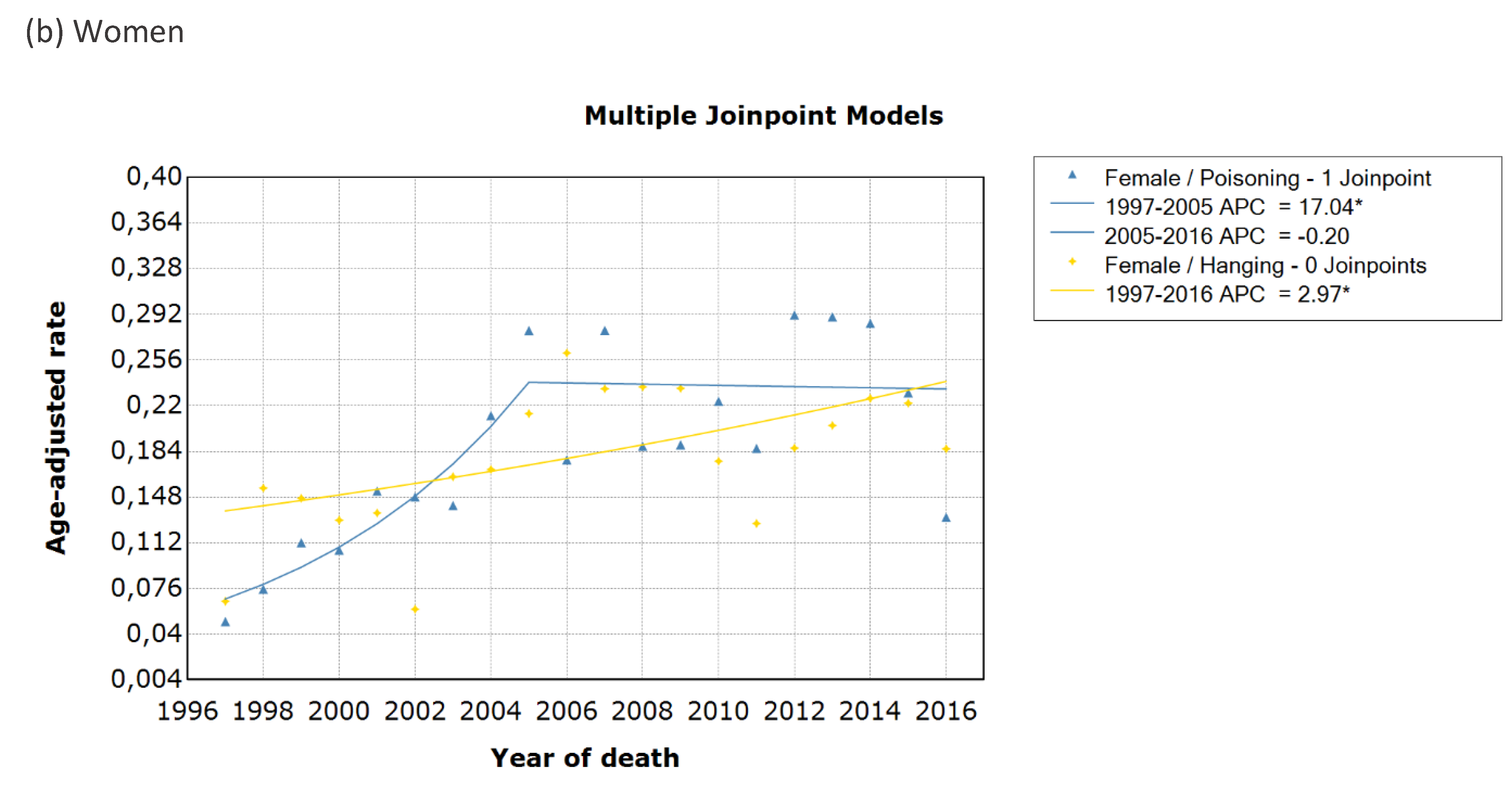
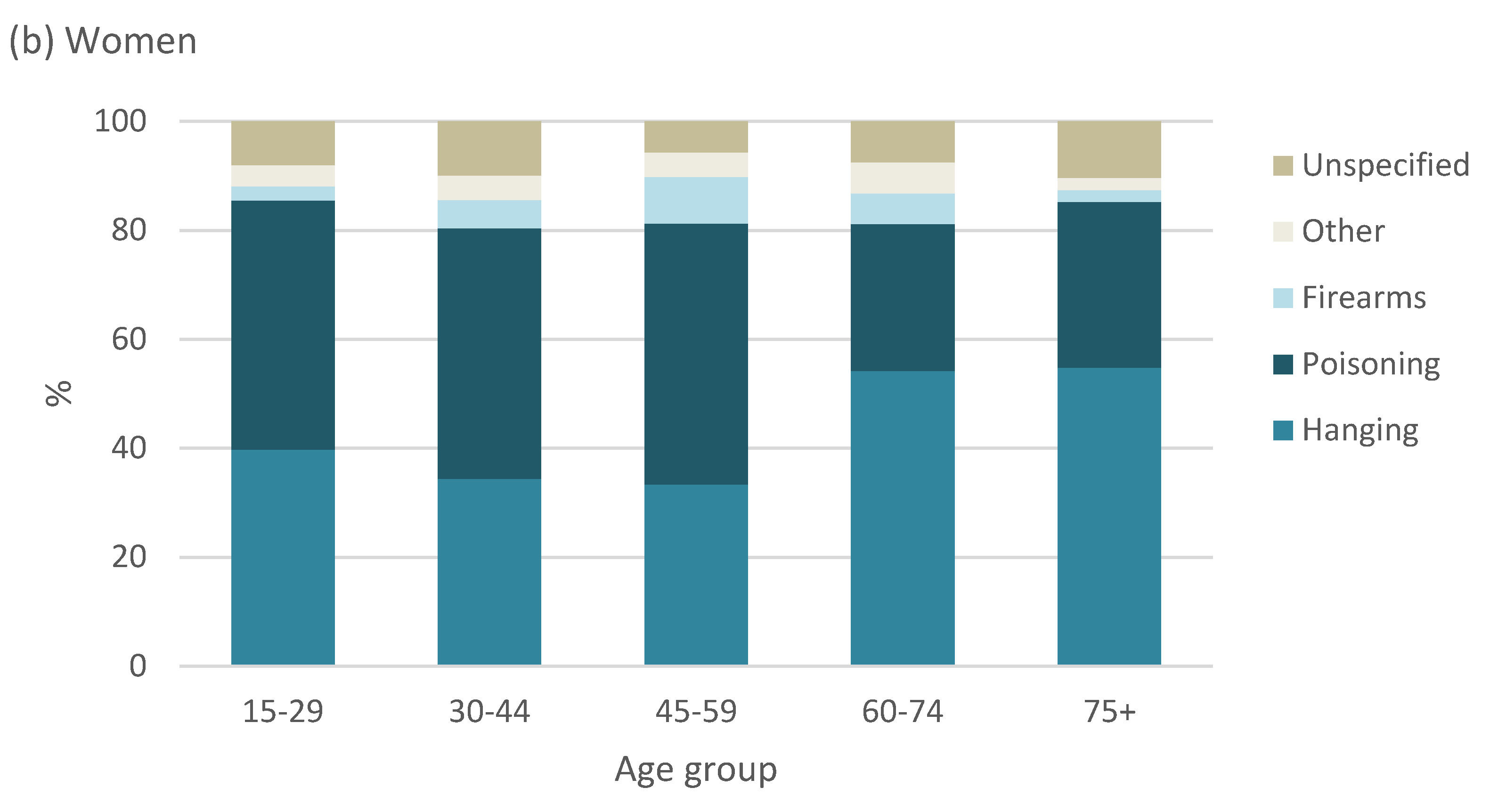
3.4. Trends in Suicide Methods
3.5. Years of Potential Life Lost
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Naghavi, M. Global, regional, and national burden of suicide mortality 1990 to 2016: Systematic analysis for the Global Burden of Disease Study 2016. Br. Med J. 2019, 364, 194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Preventing Suicide: A Global Imperative; World Health Organisation: Geneva, Switzerland, 2014; Available online: http://www.who.int/mental_health/suicid-eprevention/world_report_2014/en/ (accessed on 1 September 2019).
- van Heeringen, K. Stress–Diathesis Model of Suicidal Behavior. In The Neurobiological Basis of Suicide; Dwivedi, Y., Ed.; CRC Press/Taylor & Francis: Boca Raton, FL, USA, 2012. [Google Scholar]
- Bertolote, J.M. Suicide in the world: An epidemiological overview 1959–2000. In Suicide: An Unnecessary Death; Wasserman, D., Ed.; Martin Dunitz: London, UK, 2001; pp. 3–10. [Google Scholar]
- Mars, B.; Burrows, S.; Hjelmeland, H.; Gunnell, D. Suicidal behaviour across the African continent: A review of the literature. BMC Public Health 2014, 14, 606. [Google Scholar] [CrossRef]
- Matzopoulos, R.; Prinsloo, M.; Pillay-van Wyk, V.; Gwebushe, N.; Mathews, S.; Martin, L.J.; Laubscher, R.; Abrahmas, N.; Msemburi, W.; Lombard, C.; et al. Injury-related mortality in South Africa: A retrospective descriptive study of postmortem investigations. Bull. World Health Organ. 2015, 93, 303–313. [Google Scholar] [CrossRef] [PubMed]
- Burrows, S.; Laflamme, L. Suicide mortality in South Africa. Soc. Psychiatry Psychiatr. Epidemiol. 2006, 41, 108–114. [Google Scholar] [CrossRef] [PubMed]
- Bertolote, J.M.; Fleischmann, A. A global perspective in the epidemiology of suicide. Suicidologi 2002, 7, 6–8. [Google Scholar] [CrossRef] [Green Version]
- Ajdacic-Gross, V.; Weiss, M.G.; Ring, M.; Hepp, U.; Bopp, M.; Gutzwiller, F.; Rossler, W. Methods of suicide: International suicide patterns derived from the WHO mortality database. Bull. World Health Organ. 2008, 86, 726–732. [Google Scholar] [CrossRef] [Green Version]
- Meltzer, H.; Griffiths, C.; Brock, A.; Rooney, C.; Jenkins, R. Patterns of suicide by occupation in England and Wales: 2001–2005. Br. J. Psychiatry 2008, 193, 73–76. [Google Scholar] [CrossRef]
- Scribante, L.; Blumenthal, R.; Saayman, G.; Roos, J.L. A retrospective review of 1018 suicide cases from the capital city of South Africa for the period 1997–2000. Am. J. Forensic Med. Pathol. 2004, 25, 52–55. [Google Scholar] [CrossRef]
- Stark, K.; Joubert, G.; Struwig, M.; Pretorius, M.; Van der Merwe, N.; Botha, H.; Kotzé, J.; Krynauw, D. Suicide cases investigated at the state mortuary in Bloemfontein, 2003–2007. S. Afr. Fam. Pract. 2010, 52, 332–335. [Google Scholar] [CrossRef]
- Lopez, A.D.; AbouZahr, C.; Shibuya, K.; Gollogly, L. Keeping count: Births, deaths, and causes of death. Lancet 2007, 370, 1744–1746. [Google Scholar] [CrossRef]
- Mathers, C.D.; Ma Fat, D.; Inoue, M.; Rao, C.; Lopez, A.D. Counting the dead and what they died from: An assessment of the global status of cause of death data. Bull. World Health Organ. 2005, 83, 171c–177c. [Google Scholar]
- Joubert, J.; Rao, C.; Bradshaw, D.; Vos, T.; Lopez, A.D. Evaluating the quality of national mortality statistics from civil registration in South Africa, 1997–2007. PLoS ONE 2013, 8, e64592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Statistics South Africa Datasets. Mortality and Causes of Death 1997–2016. Available online: http://nesstar.statssa.gov.za:8282/webview/ (accessed on 1 September 2019).
- Statistics South Africa. South African Standard Classification of Occupations (SASCO). Pretoria Statistics South Africa. Available online: http://www.statssa.gov.za/classifications/codelists/SASCO_2012.pdf (accessed on 1 September 2019).
- Ahmad, O.B.; Boschi-Pinto, C.; Lopez, A.D.; Murray, C.J.; Lozano, R.; Inoue, M. Age standardization of rates: A new WHO standard. Geneva World Health Organ. 2001, 31, 1–14. [Google Scholar]
- Gardner, J.W.; Sanborn, J.S. Years of potential life lost (YPLL)—What does it measure? Epidemiology 1990, 1, 322–329. [Google Scholar] [CrossRef] [PubMed]
- Cleophas, T.J.; Zwinderman, A.H. Spline Regression Modeling. In Regression Analysis in Medical Research; Springer: Berlin, Germany, 2018; pp. 267–277. [Google Scholar]
- Kim, H.J.; Fay, M.P.; Feuer, E.J.; Midthune, D.N. Permutation tests for joinpoint regression with applications to cancer rates. Stat. Med. 2000, 19, 335–351. [Google Scholar] [CrossRef]
- JoinPoint Regression Program Version 4.0.4. Surveillance Research Program: Statistical Research and Applications Branch, National Cancer Institute; National Cancer Institute: Bethesda, MD, USA, 2013. [Google Scholar]
- Lerman, P. Fitting segmented regression models by grid search. J. R. Stat. Soc. Ser. C (Appl. Stat.) 1980, 29, 77–84. [Google Scholar] [CrossRef]
- Flisher, A.J.; Liang, H.; Laubscher, R.; Lombard, C.F. Suicide trends in South Africa, 1968–1990. Scand. J. Public Health 2004, 32, 411–418. [Google Scholar] [CrossRef]
- Vijayakumar, L. Suicide in women. Indian J. Psychiatry 2015, 57 (Suppl. S2), S233. [Google Scholar] [CrossRef]
- Phillips, M.R.; Li, X.; Zhang, Y. Suicide rates in China, 1995–1999. Lancet 2002, 359, 835–840. [Google Scholar] [CrossRef]
- Park, S.; Ahn, M.H.; Lee, A.; Hong, J.P. Associations between changes in the pattern of suicide methods and rates in Korea, the, U.S.; and Finland. Int. J. Ment. Health Syst. 2014, 8, 22. [Google Scholar] [CrossRef] [Green Version]
- Puzo, Q.; Qin, P.; Mehlum, L. Long-term trends of suicide by choice of method in Norway: A joinpoint regression analysis of data from 1969 to 2012. BMC Public Health 2016, 16, 255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daigle, M.S. Suicide prevention through means restriction: Assessing the risk of substitution: A critical review and synthesis. Accid. Anal. Prev. 2005, 37, 625–632. [Google Scholar] [CrossRef] [PubMed]
- Denning, D.G.; Conwell, Y.; King, D.; Cox, C. Method choice, intent, and gender in completed suicide. Suicide Life-Threat. Behav. 2000, 30, 282–288. [Google Scholar] [PubMed]
- Gunnell, D.; Bennewith, O.; Hawton, K.; Simkin, S.; Kapur, N. The epidemiology and prevention of suicide by hanging: A systematic review. Int. J. Epidemiol. 2005, 34, 433–442. [Google Scholar] [CrossRef] [PubMed]
- Biddle, L.; Donovan, J.; Owen-Smith, A.; Potokar, J.; Longson, D.; Hawton, K.; Kapur, N.; Gunnell, D. Factors influencing the decision to use hanging as a method of suicide: Qualitative study. Br. J. Psychiatry 2010, 197, 320–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eddleston, M. Patterns and problems of deliberate self-poisoning in the developing world. QJM Int. J. Med. 2000, 93, 715–731. [Google Scholar] [CrossRef] [Green Version]
- Veale, D.J.H.; Wium, C.A.; Müller, G.J. Toxicovigilance I: A survey of acute poisonings in South Africa based on Tygerberg Poison Information Centre data. S. Afr. Med. J. 2013, 103, 293–297. [Google Scholar] [CrossRef] [Green Version]
- Bertolote, J.M.; Fleischmann, A.; Eddleston, M.; Gunnell, D. Deaths from Pesticide Poisoning: Are we lacking a global response? Br. J. Psychiatry 2006, 189, 201–203. [Google Scholar] [CrossRef]
- Shibre, T.; Hanlon, C.; Medhin, G.; Alem, A.; Kebede, D.; Teferra, S.; Kullgren, G.; Jacobsson, L.; Fekadu, A. Suicide and suicide attempts in people with severe mental disorders in Butajira, Ethiopia: 10 year follow-up of a population-based cohort. BMC Psychiatry 2014, 14, 150. [Google Scholar] [CrossRef] [Green Version]
- Kinyanda, E.; Wamala, D.; Musisi, S.; Hjelmeland, H. Suicide in urban Kampala, Uganda: A preliminary exploration. Afr. Health Sci. 2011, 11, 219–227. [Google Scholar]
- Patience, M. Retrospective Analysis of Suspected Pesticide-Related Fatalities Admitted to Salt River Mortuary in the West Metropole of Cape Town; University of Cape Town: Cape Town, South Africa, 2018. [Google Scholar]
- Mahon, M.J.; Tobin, J.P.; Cusack, D.A.; Kelleher, C.; Malone, K.M. Suicide among regular-duty military personnel: A retrospective case-control study of occupation-specific risk factors for workplace suicide. Am. J. Psychiatry 2005, 162, 1688–1696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- London, L.; Flischer, A.J.; Wesseling, C.; Mergler, D.; Kromhout, H. Suicide and exposure to organophosphate insecticides: Cause or effect? Am. J. Ind. Med. 2005, 47, 308–321. [Google Scholar] [CrossRef] [PubMed]
- Hawton, K.; Fagg, J.; Simkin, S.; Harriss, L.; Malmberg, A.; Smith, D. The geographical distribution of suicides in farmers in England and Wales. Soc. Psychiatry Psychiatr. Epidemiol. 1999, 34, 122–127. [Google Scholar] [CrossRef] [PubMed]
- Iemmi, V.; Bantjes, J.; Coast, E.; Channer, K.; Leone, T.; McDaid, D.; Palfreyman, A.; Stephens, B.; Lund, C. Suicide and poverty in low-income and middle-income countries: A systematic review. Lancet Psychiatry 2016, 3, 774–783. [Google Scholar] [CrossRef] [Green Version]
- Blakely, T.A.; Collings, S.C.; Atkinson, J. Unemployment and suicide. Evidence for a causal association? J. Epidemiol. Community Health 2003, 57, 594–600. [Google Scholar] [CrossRef] [Green Version]
- Nordt, C.; Warnke, I.; Seifritz, E.; Kawohl, W. Modelling suicide and unemployment: A longitudinal analysis covering 63 countries, 2000–2011. Lancet Psychiatry 2015, 2, 239–245. [Google Scholar] [CrossRef]
- WHO. Global Health Estimates 2015: Deaths by Cause, Age, Sex, by Country and by Region, 2000–2015. Geneva World Health Organ. 2016. Available online: https://www.who.int/gho/mortality_burden_disease/mortality_adult/situation_trends/en/ (accessed on 2 February 2020).
- Rehkopf, D.H.; Buka, S.L. The association between suicide and the socio-economic characteristics of geographical areas: A systematic review. Psychol. Med. 2006, 36, 145–157. [Google Scholar] [CrossRef]
- Grigoriev, P.; Doblhammer-Reiter, G.; Shkolnikov, V. Trends, patterns, and determinants of regional mortality in Belarus, 1990–2007. Popul. Stud. 2013, 67, 61–81. [Google Scholar] [CrossRef] [Green Version]
- Khan, M.M.; Mahmud, S.; Karim, M.S.; Zaman, M.; Prince, M. Case–control study of suicide in Karachi, Pakistan. Br. J. Psychiatry 2008, 193, 402–405. [Google Scholar] [CrossRef] [Green Version]
- Gururaj, G.; Isaac, M.; Subbakrishna, D.; Ranjani, R. Risk factors for completed suicides: A case-control study from Bangalore, India. Inj. Control. Saf. Promot. 2004, 11, 183–191. [Google Scholar] [CrossRef]
- Knipe, D.W.; Carroll, R.; Thomas, K.H.; Pease, A.; Gunnell, D.; Metcalfe, C. Association of socio-economic position and suicide/attempted suicide in low and middle income countries in South and South-East Asia —A systematic review. BMC Public Health 2015, 15, 1055. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pompili, M.; Vichi, M.; Qin, P.; Innamorati, M.; De Leo, D.; Girardi, P. Does the level of education influence completed suicide? A nationwide register study. J. Affect. Disord. 2013, 147, 437–440. [Google Scholar] [CrossRef] [PubMed]
- Devries, K.; Watts, C.; Yoshihama, M.; Kiss, L.; Schraiber, L.B.; Deyessa, N.; Heise, L.; Durand, J.; Mbwambo, J.; Jansen, H.; et al. Violence against women is strongly associated with suicide attempts: Evidence from the WHO multi-country study on women’s health and domestic violence against women. Soc. Sci. Med. 2011, 73, 79–86. [Google Scholar] [CrossRef]
- Flisher, A.J.; Parry, C.D.; Bradshaw, D.; Juritz, J.M. Seasonal variation of suicide in South Africa. Psychiatry Res. 1997, 66, 13–22. [Google Scholar] [CrossRef]
- Burrows, S.; Laflamme, L. Assessment of accuracy of suicide mortality surveillance data in South Africa: Investigation in an urban setting. Crisis 2007, 28, 74–81. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | n (%) | Crude MOR a | 95% CI | Adjusted MOR a | 95% CI | p-Value |
|---|---|---|---|---|---|---|
| Years | ||||||
| 1997–2001 | 1405 (16.4) | Reference | Reference | |||
| 2002–2006 | 2318 (27.1) | 1.12 | 1.05–1.20 | 1.03 | 0.93–1.14 | 0.571 |
| 2007–2011 | 2142 (24.9) | 1.03 | 0.96–1.10 | 1.07 | 0.96–1.18 | 0.215 |
| 2012–2016 | 2708 (31.6) | 1.57 | 1.47–1.67 | 1.67 | 1.15–1.85 | <0.001 |
| Sex | ||||||
| Female | 1855 (21.9) | Reference | Reference | |||
| Male | 6699 (78.1) | 3.33 | 3.16–3.50 | 2.68 | 2.49–2.89 | <0.001 |
| Broad age-group | ||||||
| 15–29 | 3656 (42.7) | 17.57 | 15.99–19.28 | 8.42 | 7.31–9.70 | <0.001 |
| 30–44 | 2581 (30.1) | 6.50 | 5.90–7.16 | 3.79 | 3.29–4.33 | <0.001 |
| 45–59 | 1301 (15.2) | 4.02 | 3.62–4.45 | 2.19 | 1.91–2.53 | <0.001 |
| 60–74 | 536 (6.3) | 1.75 | 1.54–1.98 | 0.84 | 0.69–1.01 | 0.065 |
| 75 and over | 499 (5.82) | Reference | ||||
| Population group | ||||||
| Black African | 5594 (65.3) | Reference | Reference | |||
| Indian or Asian | 156 (1.8) | 1.24 | 1.15–1.35 | 1.36 | 1.13–1.64 | 0.001 |
| White | 763 (8.9) | 1.25 | 1.07–1.47 | 2.52 | 1.13–1.64 | <0.001 |
| Coloured | 958 (11.2) | 2.12 | 1.99–2.27 | 1.64 | 1.45–1.84 | <0.001 |
| Unspecified or unknown | 1102 (12.8) | 0.48 | 0.44–0.51 | 0.66 | 0.59–0.73 | <0.001 |
| Marital status | ||||||
| Widowed/divorced | 531 (6.2) | Reference | Reference | |||
| Never married | 5739 (67.2) | 2.88 | 2.64–3.16 | 1.02 | 0.90–1.17 | 0.670 |
| Married | 1610 (18.8) | 1.77 | 1.60–1.96 | 1.13 | 0.99–1.29 | 0.065 |
| Educational attainment | ||||||
| None/Grade R | 420 (8.7) | Reference | Reference | |||
| Primary education | 1221 (25.1) | 1.83 | 1.63–2.04 | 1.13 | 1.02–1.28 | 0.024 |
| Secondary | 2897 (59.7) | 3.23 | 2.91–3.58 | 1.49 | 1.34–1.67 | <0.001 |
| Tertiary | 313 (6.5) | 3.46 | 2.99–4.00 | 1.63 | 1.39–1.91 | <0.001 |
| Smoking status of deceased | ||||||
| No | 2150 (25.1) | Reference | Reference | |||
| Yes | 1966 (22.9) | 2.05 | 1.93–2.19 | 1.24 | 1.15–1.32 | <0.001 |
| Unknown/unspecified | 4457(51.9) | 1.02 | 0.97–1.07 | 1.37 | 0.73–2.55 | 0.321 |
| Province of death | ||||||
| Free State | 489 (5.7) | Reference | Reference | |||
| Kwa-Zulu Natal | 2690 (31.5) | 1.99 | 1.81–2.19 | 1.98 | 1.77–2.21 | <0.001 |
| Western Cape | 1094 (12.8) | 2.02 | 1.82–2.25 | 1.10 | 0.93–1.31 | 0.252 |
| Eastern Cape | 972 (11.4) | 1.09 | 0.98–1.22 | 1.00 | 0.88–1.16 | 0.899 |
| Northern Cape | 932 (10.9) | 5.70 | 5.11–6.36 | 5.15 | 4.48–5.91 | <0.001 |
| Mpumalanga | 683 (8.0) | 1.51 | 1.34–1.69 | 1.00 | 0.86–1.16 | 0.987 |
| North West | 612 (7.2) | 1.07 | 1.21–1.53 | 1.37 | 1.18–1.61 | <0.001 |
| Limpopo | 571 (6.7) | 1.31 | 0.95–1.21 | 1.00 | 0.87–1.17 | 0.939 |
| Gauteng | 482 (5.7) | 0.39 | 0.34–0.44 | 0.34 | 0.28–0.39 | <0.001 |
| Occupation groups | ||||||
| Technicians | 25 (0.3) | Reference | Reference | |||
| Managers | 36 (0.4) | 1.37 | 0.82–2.82 | 1.54 | 0.86–3.06 | 0.138 |
| Professionals | 70 (0.8) | 1.03 | 0.65–1.63 | 1.63 | 0.97–2.73 | 0.064 |
| Clerks | 36 (0.4) | 1.09 | 0.65–1.81 | 1.69 | 0.57–1.81 | 0.338 |
| Service workers and armed forces | 139 (1.6) | 1.85 | 1.21–2.84 | 1.88 | 1.16–3.06 | 0.011 |
| Skilled agricultural workers | 92 (1.1) | 2.62 | 1.68–4.09 | 2.72 | 1.64–4.51 | <0.001 |
| Craft & related trade workers | 101 (1.2) | 1.24 | 0.80–1.92 | 1.26 | 0.76–2.08 | 0.361 |
| Plant & machine operators | 107 (1.3) | 1.40 | 0.91–2.18 | 1.52 | 0.61–1.91 | 0.096 |
| Elementary occupations | 332 (3.9) | 1.25 | 0.83–1.88 | 1.69 | 1.06–2.71 | 0.027 |
| Unspecified occupations or not economically active | 7635 (89.1) | 0.90 | 0.61–1.33 | 1.94 | 1.23–3.06 | 0.004 |
| Place of death | ||||||
| Hospital | 1628 (19.0) | Reference | Reference | |||
| Home | 2301 (26.8) | 2.21 | 2.08–2.36 | 2.26 | 2.08–2.46 | <0.001 |
| Dead on arrival | 597 (7.0) | 6.94 | 6.31–7.62 | 3.84 | 3.40–4.31 | <0.001 |
| Emergency room | 165 (1.9) | 2.62 | 2.23–3.08 | 1.84 | 1.48–2.27 | <0.001 |
| Nursing home | 77 (0.9) | 0.96 | 0.76–1.21 | 1.21 | 0.87–1.67 | 0.256 |
| Unspecified | 3805 (44.4) | 4.34 | 4.09–4.60 | 3.37 | 3.11–3.66 | <0.001 |
| Occupation Group | Hanging | Firearms | Pesticide Poisoning | Poisoning by other Means | Unspecified or Other Means |
|---|---|---|---|---|---|
| Managers | 8 (1.6) | 12 (10.4) | 0 (0) | 8 (4.8) | 2 (3.8) |
| Professionals | 32 (6.2) | 10 (8.7) | 1 (3.9) | 15 (8.9) | 6 (11.3) |
| Technicians | 14 (2.7) | 1 (0.8) | 0 (0) | 7 (4.2) | 2 (3.8) |
| Clerks | 15 (2.9) | 7 (6.1) | 1 (3.9) | 8 (4.8) | 3 (5.7) |
| Service workers and armed forces | 65 (12.6) | 40 (34.8) | 2 (7.7) | 24 (14.4) | 4 (7.5) |
| Skilled agricultural workers | 53 (10.3) | 16 (13.9) | 7 (26.9) | 11 (6.6) | 3 (5.7) |
| Craft and trade workers | 51 (9.9) | 8 (6.9) | 2 (7.7) | 23 (13.7) | 10 (18.9) |
| Plant and machine operators | 64 (12.5) | 11 (9.6) | 3 (11.5) | 17 (10.2) | 2 (3.8) |
| Elementary occupation | 212 (41.3) | 10 (8.7) | 10 (38.5) | 54 (32.3) | 23 (43.4) |
| Year | Male | Female | ||||||
|---|---|---|---|---|---|---|---|---|
| All Causes (YPLL) | Suicide-Specific (YPLL) | All Causes (YPLL) | Suicide-Specific (YPLL) | |||||
| Total YPLL | Rate Per | Total PYLL | Rate Per | Total PYLL | Rate Per | Total PYLL | Rate Per | |
| 1000 | 1000 a | 1000 a | 1000 a | |||||
| 1997 | 2,398,233 | 209,88 | 2325 | 0.20 | 1,471,662 | 116.12 | 595 | 0.04 |
| 1998 | 2,792,467 | 244,48 | 3912 | 0.29 | 1,862,922 | 145.78 | 1237 | 0.09 |
| 1999 | 2,997,012 | 262,39 | 6595 | 0.51 | 2,223,997 | 172.00 | 1805 | 0.13 |
| 2000 | 3,263,040 | 286,10 | 6625 | 0.52 | 2,694,757 | 207.61 | 2035 | 0.14 |
| 2001 | 3,598,960 | 274,09 | 11,635 | 0.78 | 3,135,470 | 207.78 | 2712 | 0.17 |
| 2002 | 3,988,685 | 296,95 | 6297 | 0.42 | 3,737,317 | 248.45 | 1667 | 0.09 |
| 2003 | 4,421,255 | 323,76 | 6967 | 0.45 | 4,295,517 | 281.71 | 2007 | 0.12 |
| 2004 | 4,555,435 | 328,59 | 11,152 | 0.72 | 4,638,935 | 300.71 | 3330 | 0.20 |
| 2005 | 4,653,162 | 330,58 | 13,457 | 0.85 | 4,725,847 | 302.97 | 3322 | 0.19 |
| 2006 | 4,717,585 | 328,82 | 13,370 | 0.81 | 4,707,187 | 297.83 | 2712 | 0.16 |
| 2007 | 4,671,250 | 319,02 | 10,507 | 0.62 | 4,483,875 | 279.87 | 3237 | 0.18 |
| 2008 | 4,580,495 | 306,39 | 10,565 | 0.62 | 4,307,242 | 264.37 | 2920 | 0.16 |
| 2009 | 4,386,215 | 276,70 | 8305 | 0.47 | 4,725,847 | 282.27 | 2885 | 0.16 |
| 2010 | 4,058,652 | 260,99 | 8822 | 0.50 | 3,661,447 | 216.78 | 2852 | 0.15 |
| 2011 | 3,705,815 | 233,27 | 8767 | 0.48 | 3,164,912 | 184.45 | 2422 | 0.13 |
| 2012 | 3,505,240 | 214,99 | 11,500 | 0.60 | 2,860,962 | 163.65 | 3532 | 0.18 |
| 2013 | 3,356,222 | 201,23 | 14,272 | 0.75 | 2,605,087 | 146.71 | 3265 | 0.17 |
| 2014 | 3,284,210 | 192,78 | 14,370 | 0.75 | 2,457,035 | 136.29 | 4065 | 0.21 |
| 2015 | 3,249,292 | 186,68 | 11,252 | 0.58 | 2,331,967 | 127.35 | 3227 | 0.17 |
| 2016 | 3,133,707 | 175,98 | 10,485 | 0.53 | 2,187,140 | 117.53 | 2422 | 0.13 |
| Total | 28,015,087 | 262,68 | 191,180 | 0.57 b | 9,295,898 | 210.01 b | 52,249 | 0.15 b |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kootbodien, T.; Naicker, N.; Wilson, K.S.; Ramesar, R.; London, L. Trends in Suicide Mortality in South Africa, 1997 to 2016. Int. J. Environ. Res. Public Health 2020, 17, 1850. https://doi.org/10.3390/ijerph17061850
Kootbodien T, Naicker N, Wilson KS, Ramesar R, London L. Trends in Suicide Mortality in South Africa, 1997 to 2016. International Journal of Environmental Research and Public Health. 2020; 17(6):1850. https://doi.org/10.3390/ijerph17061850
Chicago/Turabian StyleKootbodien, Tahira, Nisha Naicker, Kerry S. Wilson, Raj Ramesar, and Leslie London. 2020. "Trends in Suicide Mortality in South Africa, 1997 to 2016" International Journal of Environmental Research and Public Health 17, no. 6: 1850. https://doi.org/10.3390/ijerph17061850