Chained Risk Assessment for Life-Long Disease Burden of Early Exposures–Demonstration of Concept Using Prenatal Maternal Smoking


Abstract
:1. Introduction
2. Materials and Methods
2.1. Identification of Relevant Health Endpoints
- Meta-analysis with statistically significant pooled risk estimate;
- Background disease burden of reported endpoint is available;
- Free full text is available in English.
2.2. Nested Risk Model
3. Results
4. Discussion
4.1. Biological Plausibility
4.2. Uncertainties
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- GBD 2017 Risk Factor Collaborators. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1923–1994. [Google Scholar] [CrossRef] [Green Version]
- Global Burden of Disease Collaborative Network and Institute for Health Metrics and Evaluation. Global Burden of Disease Study 2017 (GBD 2017) Results. Available online: http://ghdx.healthdata.org/gbd-results-tool (accessed on 16 November 2018).
- Dennis, K.K.; Jones, D.P. The exposome: A new frontier for education. Am. Biol. Teach. 2016, 78, 542–548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuh, D.; Ben-Shlomo, Y.; Lynch, J.; Hallqvist, J.; Power, C. Life course epidemiology. J. Epidemiol. Community Health 2003, 57, 778–783. [Google Scholar] [CrossRef] [PubMed]
- Barker, D.J. The origins of the developmental origins theory. J. Intern. Med. 2007, 261, 412–417. [Google Scholar] [CrossRef] [PubMed]
- Barker, D.J.P.; Osmond, C. Infant mortality, childhood nutrition and ischaemic heart disease in England and Wales. Lancet 1986, 1, 1077–1081. [Google Scholar] [CrossRef]
- Ravelli, G.-P.; Stein, Z.; Susser, M. Obesity in young men after famine exposure in utero and early infancy. New Engl. J. Med. 1976, 295, 349–353. [Google Scholar] [CrossRef]
- Rosenboom, T.; de Rooij, S.; Painter, R. The Dutch famine and its long-term consequences for adult health. Early Hum. Dev. 2006, 82, 485–491. [Google Scholar] [CrossRef]
- Gluckman, P.D.; Hanson, M.A. Developmental origins of disease paradigm: A mechanistic and evolutionary perspective. Pediatr. Res. 2004, 56, 311–317. [Google Scholar] [CrossRef]
- Hanson, M.A.; Gluckman, P.D. Early developmental conditioning of later health and disease: Physiology or pathophysiology? Physiol. Rev. 2014, 94, 1027–1076. [Google Scholar] [CrossRef]
- Schug, T.T.; Barouki, R.; Gluckman, P.D.; Grandjean, P.; Hanson, M.; Heindel, J.J. Proceedings of PPTOX III: Environmental stressors in the developmental origins of disease-evidence and mechanisms. Toxicol. Sci. 2013, 131, 343–350. [Google Scholar] [CrossRef] [Green Version]
- Anderson, L.M.; Diwan, B.A.; Fear, N.T.; Roman, E. Critical windows of exposure for children’s health: Cancer in human epidemiological studies and neoplasms in experimental animal models. Environ. Health Perspect. 2000, 108, 573–594. [Google Scholar] [PubMed]
- Godfrey, K.M.; Gluckman, P.D.; Hanson, M.A. Developmental origins of metabolic disease: Life course and intergenerational perspectives. Trends Endocrinol. Metab. 2010, 21, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Räisänen, S.; Sankilampi, U.; Gissler, M.; Kramer, M.R.; Hakulinen-Viitanen, T.; Saari, J.; Heinonen, S. Smoking cessation in the first trimester reduces most obstetric risks, but not the risks of major congenital anomalies and admission to neonatal care: A population-based cohort study of 1,164,953 singleton pregnancies in Finland. J. Epidemiol. Community Health 2014, 68, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Rumrich, I.K.; Vähäkangas, K.; Viluksela, M.; Gissler, M.; de Ruyter, H.; Hänninen, O. Effects of maternal smoking on body size and proportions at birth: A register-based cohort study of 1.4 million births. BMJ Open 2019. [Google Scholar] [CrossRef] [Green Version]
- Rumrich, I.K.; Vähäkangas, K.; Viluksela, M.; Gissler, M.; Surcel, H.M.; Korhonen, A.; de Ruyter, H.; Hänninen, O. Smoking during Pregnancy in Finland-Trends in the MATEX cohort. Scand. J. Public Health 2019, 47, 890–898. [Google Scholar] [CrossRef] [PubMed]
- Suter, M.A.; Anders, A.M.; Aagaard, K.M. Maternal smoking as a model for environmental epigenetic changes affecting birthweight and fetal programming. Mol. Hum. Reprod. 2013, 19, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Knopik, V.S.; Maccani, M.A.; Francazio, S.; McGeary, J.E. The epigenetics of maternal cigarette smoking during pregnancy and effects on child development. Dev. Psychopathol. 2012, 24, 1377–1390. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, D.A.; Green, B.B.; Blair, B.A.; Guerin, D.J.; Litzky, J.F.; Chavan, N.R.; Pearson, K.J.; Marsit, C.J. Maternal smoking during pregnancy is associated with mitochondrial DNA methylation. Environ. Epigenetics 2016, 2, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Witt, S.H.; Frank, J.; Gilles, M.; Lang, M.; Treutlein, J.; Streit, F.; Wolf, I.A.C.; Peus, V.; Scharnholz, B.; Send, T.S.; et al. Impact on Birth weight of Maternal Smoking throughout Pregnancy Mediated by DNA Methylation. BMC Genom. 2018, 19, 7. [Google Scholar] [CrossRef] [Green Version]
- Abraham, M.; Alramadhan, S.; Iniguez, C.; Duijts, L.; Jaddoe, V.W.; Den Dekker, H.T.; Crozier, S.; Godfrey, K.M.; Hindmarsh, P.; Vik, T. A systematic review of maternal smoking during pregnancy and fetal measurements with meta-analysis. PLoS ONE 2017, 12, e0170946. [Google Scholar] [CrossRef] [Green Version]
- Notkola, V.; Punsar, S.; Karvonen, M.J.; Haapakoski, J. Socio-economic conditions in childhood and mortality and morbidity caused by coronary heart disease in adulthood in rural Finland. Soc. Sci. Med. 1985, 21, 517–523. [Google Scholar] [CrossRef]
- Forsdahl, A. Are poor housing conditions in childhood and adolescence an important risk factor for areriosclerotic heart disease? Br. J. Prev. Soc. Med. 1977, 31, 91–95. [Google Scholar] [PubMed] [Green Version]
- Knight, A.K.; Smith, A.K. Epigenetic biomarkers of preterm birth and its risk factors. Genes 2016, 7, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simpson, W.J.; Linda, L. A preliminary report on cigarette smoking and the incidence of prematurity. Am. J. Obstet. Gynecol. 1957, 73, 807–815. [Google Scholar] [CrossRef]
- Kramer, M.S. Determinants of Low Birth Weight: Methodological Assessment and Meta-Analysis. Bull. World Health Organ. 1987, 65, 663–737. [Google Scholar]
- Hänninen, O.; Knol, A.B.; Jantunen, M.; Lim, T.A.; Conrad, A.; Rappolder, M.; Carrer, P.; Fanetti, An.; Kim, R.; Buekers, J.; et al. Environmental Burden of Disease in Europe: Assessing Nine Risk Factors in Six Countries. Environ. Health Perspect. 2014, 122, 439–446. [Google Scholar] [CrossRef] [Green Version]
- Saari, A.; Sankilampi, U.; Hannila, M.L.; Kiviniemi, V.; Kesseli, K.; Dunkel, L. New Finnish growth references for children and adolescents aged 0 to 20 years: Length/height-for-age, weight-for-length/height, and body mass index-for-age. Ann. Med. 2011, 43, 235–248. [Google Scholar] [CrossRef]
- Rayfield, S.; Plugge, E. Systematic review and meta-analysis of the association between maternal smoking in pregnancy and childhood overweight and obesity. J. Epidemiol. Community Health 2017, 71, 162–173. [Google Scholar] [CrossRef] [Green Version]
- Llewellyn, A.; Simmonds, M.; Owen, S.G.; Woolacott, N. Childhood obesity as a predictor of morbidity in adultood: A systematic review and meta-analysis. Obes. Rev. 2016, 17, 56–67. [Google Scholar] [CrossRef]
- Global Burden of Disease Collaborative Network and Institute for Health Metrics and Evaluation. Global Burden of Disease Study 2017 (GBD 2017) Results-Metabolic risks. Available online: http://ghdx.healthdata.org/gbd-results-tool?params=gbd-api-2017-permalink/df22cc38ff90b236a500b83b95b9f408 (accessed on 3 May 2019).
- Silveira, V.M.F.D.; Horta, B.L. Birth weight and metabolic syndrome in adults: Meta-analysis. Rev. Saude Publica. 2008, 42, 10–18. [Google Scholar] [CrossRef] [Green Version]
- Global Burden of Disease Collaborative Network and Institute for Health Metrics and Evaluation. Global Burden of Disease Study 2017 (GBD 2017) Results-Preterm birth. Available online: http://ghdx.healthdata.org/gbd-results-tool?params=gbd-api-2017-permalink/2ff246b03df37395ee98307face1a4c8 (accessed on 3 May 2019).
- Global Burden of Disease Collaborative Network. Global Burden of Disease Study 2017 (GBD 2017) Disability Weights; Institute for Health Metrics and Evaluation (IHME): Seattle, DC, USA, 2018. [Google Scholar]
- Accordini, S.; Calciano, L.; Johannessen, A.; Portas, L.; Benediktsdóttir, B.; Bertelsen, R.J.; Bråbäck, L.; Carsin, An.; Dharmage, S.C.; Dratva, J.; et al. A three-generation study on the association of tobacco smoking with asthma. Int. J. Epidemiol. 2018, 47, 1106–1117. [Google Scholar] [CrossRef] [PubMed]
- Mattsson, K.; Kallen, K.; Longnecker, M.P.; Rignell-Hydbom, A.; Rylander, L. Maternal Smoking during Pregnancy and Daughters’ Risk of Gestational Diabetes and Obesity. Diabetologia 2013, 56, 1689–1695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ajala, O.; Mold, F.; Boughton, C.; Cooke, D.; Whyte, M. Childhood predictors of cardiovascular disease in adulthood. A systematic review and meta-analysis. Obes. Rev. 2017, 18, 1061–1070. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ul-Haq, Z.; Mackay, D.F.; Fenwick, E.; Pell, J.P. Meta-analysis of the association between body mass index and health-related quality of life among adults, assessed by the SF-36. Obesity 2013, 21, E322–E327. [Google Scholar] [CrossRef]
- Twilhaar, E.S.; de Kieviet, J.F.; Aarnoudse-Moens, C.S.; van Elburg, R.M.; Oosterlaan, J. Academic performance of children born preterm: A meta-analysis and meta-regression. Arch. Dis. Child. Fetal Neonatal Ed. 2018, 103, F322–F330. [Google Scholar] [CrossRef] [Green Version]
- Bilgin, A.; Mendonca, M.; Wolke, D. Preterm Birth/Low Birth Weight and Markers Reflective of Wealth in Adulthood: A Meta-analysis. Pediatrics 2018, 142, e20173625. [Google Scholar] [CrossRef] [Green Version]
- Kormos, C.E.; Wilkinson, A.J.; Davey, C.J.; Cunningham, A.J. Low birth weight and intelligence in adolescence and early adulthood: A meta-analysis. J. Public Health 2014, 36, 213–224. [Google Scholar] [CrossRef] [Green Version]
- Pratt, T.C.; McGloin, J.M.; Fearn, N.E. Maternal cigarette smoking during pregnancy and criminal/deviant behavior: A meta-analysis. Int. J. Offender Ther. Comp. Criminol. 2006, 50, 672–690. [Google Scholar] [CrossRef]
- Vardavas, C.I.; Hohmann, C.; Patelarou, E.; Martinez, D.; Henderson, A.J.; Granell, R.; Sunyer, J.; Torrent, M.; Fantini, M.P.; Gori, D.; et al. The independent role of prenatal and postnatal exposure to active and passive smoking on the development of early wheeze in children. Eur. Respir. J. 2016, 48, 115–124. [Google Scholar] [CrossRef]
- Silvestri, M.; Franchi, S.; Pistorio, A.; Petecchia, L.; Rusconi, F. Smoke exposure, wheezing, and asthma development: A systematic review and meta-analysis in unselected birth cohorts. Pediatr. Pulmonol. 2015, 50, 353–362. [Google Scholar] [CrossRef]
- Sonnenschein-Van Der Voort, A.M.; Arends, L.R.; de Jongste, J.C.; Annesi-Maesano, I.; Arshad, S.H.; Barros, H.; Basterrechea, M.; Bisgaard, H.; Chatzi, L.; Corpeleijn, E.; et al. Preterm birth, infant weight gain, and childhood asthma risk: A meta-analysis of 147,000 European children. J. Allergy Clin. Immunol. 2014, 133, 1317–1329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mebrahtu, T.F.; Feltbower, R.G.; Greenwood, D.C.; Parslow, R.C. Birth weight and childhood wheezing disorders: A systematic review and meta-analysis. J. Epidemiol. Community Health 2015, 69, 500–508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herman, T.; Sonnenschein-Van Der Voort, A.M.; De Jongste, J.C.; Anessi-Maesano, I.; Arshad, S.H.; Barros, H.; Beardsmore, C.S.; Bisgaard, H.; Phar, S.C.; Craig, L.; et al. Early growth characteristics and the risk of reduced lung function and asthma: A meta-analysis of 25,000 children. J. Allergy Clin. Immunol. 2016, 137, 1026–1035. [Google Scholar]
- Lawlor, D.A.; Ebrahim, S.; Davey, S.G. Association of birth weight with adult lung function: Findings from the British Women’s Heart and Health Study and a meta-analysis. Thorax 2005, 60, 851–858. [Google Scholar] [CrossRef] [Green Version]
- Pearson, J.; Tarabulsy, G.M.; Bussières, E.L. Foetal programming and cortisol secretion in early childhood: A meta-analysis of different programming variables. Infant Behav. Dev. 2015, 40, 204–215. [Google Scholar] [CrossRef]
- Van Montfoort, N.; Finken, M.J.J.; le Cessie, S.; Dekker, F.W.; Wit, J.M. Could cortisol explain the association between birth weight and cardiovascular disease in later life? A meta-analysis. Eur. J. Endocrinol. 2005, 153, 811–817. [Google Scholar] [CrossRef]
- Kim, J.; Lee, I.; Lim, S. Overweight or obesity in children ages 0 to 6 and the risk of adult metabolic syndrome: A systematic review and meta-analysis. J. Clin. Nurs. 2017, 26, 3869–3880. [Google Scholar] [CrossRef]
- Lawlor, D.A.; Owen, C.G.; Davies, A.A.; Whincup, P.H.; Ebrahim, S.; Cook, D.G.; Smith, G.D. Sex differences in the association between birth weight and total cholesterol. A meta-analysis. Ann. Epidemiol. 2006, 16, 19–25. [Google Scholar] [CrossRef]
- Friedemann, C.; Heneghan, C.; Mahtani, K.; Thompson, M.; Perera, R.; Ward, A.M. Cardiovascular disease risk in healthy children and its association with body mass index: Systematic review and meta-analysis. BMJ 2012, 345, e4759. [Google Scholar] [CrossRef] [Green Version]
- Meng, X.; Sun, Y.; Duan, W.; Jia, C. Meta-analysis of the association of maternal smoking and passive smoking during pregnancy with neural tube defects. Int. J. Gynaecol. Obstet. 2018, 140, 18–25. [Google Scholar] [CrossRef]
- Yermachenko, A.; Dvornyk, V. A meta-analysis provides evidence that prenatal smoking exposure decreases age at menarche. Reprod. Toxicol. 2015, 58, 222–228. [Google Scholar] [CrossRef] [PubMed]
- Van Leeuwen, J.; Koes, B.W.; Paulis, W.D.; van Middelkoop, M. Differences in bone mineral density between normal-weight children and children with overweight and obesity: A systematic review and meta-analysis. Obes. Rev. 2017, 18, 526–546. [Google Scholar] [CrossRef] [PubMed]
- Martens, L.; De Smet, S.; Yusof MY, P.M.; Rajasekharan, S. Association between overweight/obesity and periodontal disease in children and adolescents: A systematic review and meta-analysis. Eur. Arch. Paediatr. Dent. 2017, 18, 69–82. [Google Scholar] [CrossRef] [PubMed]
- Lehtomäki, H.; Korhonen, A.; Asikainen, A.; Karvosenoja, N.; Kupiainen, K.; Paunu, V.; Savolahti, M.; Sofiev, M.; Palamarchuk, Y.; Karppinen, A.; et al. Health Impacts of Ambient Air Pollution in Finland. Int. J. Environ. Res. Public Health 2018, 15, 736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO 2016. Sixty-ninth world health assembly A69/18. Provisional agenda item 13.5 6 May 2016. Health and the Environment: Draft Road Map for an Enhanced Global Response to the Adverse Health Effects of Air Pollution. Available online: http://apps.who.int/gb/ebwha/pdf_files/WHA69/A69_18-en.pdf?ua=1&ua=1&ua=1 (accessed on 3 May 2019).
- Lange, S.; Probst, C.; Rehm, L.; Popova, S. National, Regional, and Global Prevalence of Smoking during Pregnancy in the General Population: A Systematic Review and Meta-Analysis. Lancet Glob. Health 2018, 6, e776. [Google Scholar] [CrossRef] [Green Version]
- Ekblad, M.; Gissler, M.; Korkeila, J.; Lehtonen, L. Trends and Risk Groups for Smoking during Pregnancy in Finland and Other Nordic Countries. Eur. J. Public Health 2013, 24, 544–551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reitan, T.; Callinan, S. Changes in Smoking Rates among Pregnant Women and the General Female Population in Australia, Finland, Norway, and Sweden. Nicotine Tob. Res. 2017, 19, 282–289. [Google Scholar] [CrossRef] [Green Version]
- OECD-Social Policy Division-Directorate of Employment, Labour and Social Affairs. CO1.3: Low birth Weight. 2018. Available online: https://www.oecd.org/els/family/CO_1_3_Low_birth_weight.pdf (accessed on 3 May 2019).
- Chawanpaiboon, S.; Vogel, J.P.; Moller, A.B.; Lumbiganon, P.; Petzold, M.; Hogan., D.; Landoulsi, S.; Jampathong, N.; Kongwattanakul, K.; Laopaiboon, M.; et al. Global, regional and national estimates of levels of preterm birth in 2014: A systematic review and modelling analysis. Lancet Glob. Health 2018. [Google Scholar] [CrossRef] [Green Version]
- OECD Obesity Update 2017. Available online: https://www.oecd.org/els/health-systems/Obesity-Update-2017.pdf (accessed on 3 May 2019).
- Gage, S.H.; Munafò, M.R.; Smith, G.D. Causal inference in developmental origin of health and disease (DOHaD) research. Ann. Rev. Psychol. 2016, 67, 657–685. [Google Scholar] [CrossRef] [Green Version]
- Mandy, M.; Nyirenda, M. Developmental Origins of Health and Disease: The relevance to developing nations. Int. Health 2018, 10, 66–70. [Google Scholar] [CrossRef] [Green Version]
- Gordijn, S.J.; Beune, I.M.; Thilaganathan, B.; Papageorghiou, A.; Baschat, A.A.; Baker, P.N.; Silver, R.M.; Wynia, K.; Ganzevoort, W. Consensus Definition of Fetal Growth Restriction: A Delphi Procedure. Ultrasound Obstet. Gynecol. 2016, 48, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Sharma, D.; Shastri, S.; Farahbakhsh, N.; Sharma, P. Intrauterine Growth Restriction-Part 1. J. Matern. Fetal Neonatal Med. 2016, 29, 3977–3987. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Population Attributable Fraction Input | Maternal Smoking | Preterm Birth (PTB) | Low Birth Weight (LBW) | Childhood Overweight and Obesity (12–18 Years) | |
|---|---|---|---|---|---|
| Overweight | Obesity | ||||
| Definition | Tobacco smoking | Gestational age < 37 weeks | Birth weight < 2500 g | BMI ≥ 25 at | BMI ≥ 30 |
| Exposure only during 1st trimester throughout pregnancy | 6.8 % a [16] 7.0 % b [16] | n/a [15] 4 %[16] | 3 % [16] 3 % [16] | n/a 14% [28] | n/a 3% [28] |
| Risk estimate (RR) | 1.38 [15] | 1.11 a [15] 2.22 b [15] | 1.37 [29] | 1.55 [29] | |
| Population attributable fraction only during 1st trimester throughout pregnancy | n/a 0.03 b | 0.01 a 0.08 b | n/a 0.03 b | n/a 0.04 b | |
| Endpoint | Age Group | Background Burden (in DALY) | Attributable Disease Burden (in DALY) | |||||
|---|---|---|---|---|---|---|---|---|
| Maternal Smoking | Preterm Birth | Low Birth Weight | Childhood Overweight & Obesity | Total | ||||
| 1 | Cancer | |||||||
| 1.1 | Acute leukemia | <20 years | 806 | 3.9 | 6.8 | n/a | 32 | 43 |
| 1.2 | Lymphoma | <20 years | 238 | 7 | n/a | n/a | n/a | 7 |
| 1.3 | Nervous system cancer | <20 years | 832 | 5.2 | n/a | n/a | n/a | 5.2 |
| 1.4 | Testicular cancer | <20 years | 11 | n/a | n/a | 0.22 | n/a | 0.22 |
| 1.5 | Wilms’ tumor | <20 years | 95 | n/a | 1.6 | n/a | n/a | 1.6 |
| 1.6 | Other cancer a | ≥20 years | 41,647 | n/a | n/a | n/a | 2570 | 2570 |
| 2 | Cardiovascular | |||||||
| 2.1 | Coronary heart disease | All ages | 157,588 | n/a | n/a | 2066 | 3184 | 5250 |
| 2.2 | Essential hypertension | All ages | 12,532 | n/a | 153 | n/a | 1323 | 1477 |
| 2.3 | Stroke | All ages | 71,952 | n/a | n/a | n/a | 5088 | 5088 |
| 3 | Mental & cognitive disorders | |||||||
| 3.1 | Depression | ≥20 years | 292 | n/a | n/a | 2.6 | 3.5 | 6.1 |
| 3.2 | Autism | All ages | 4528 | n/a | 55 | 167 | n/a | 223 |
| 3.3 | Attention Deficit/Hyperactivity Disorder | All ages | 703 | n/a | 43 | n/a | 4.2 | 47 |
| 3.4 | Intellectual disability | All ages | 1059 | n/a | 42 | n/a | n/a | 42 |
| 4 | Other groups | |||||||
| 4.1 | Diabetes | All ages | 55,898 | n/a | 1059 | 977 | 15,987 | 18,023 |
| 4.2 | Asthma | All ages | 13,809 | 39 | 14 | 189 | 47 | 290 |
| 4.3 | Congenital anomalies b | All ages | 8593 | 115 | n/a | n/a | n/a | 115 |
| 4.4 | Chronic kidney disease | All ages | 11,807 | n/a | n/a | 506 | n/a | 506 |
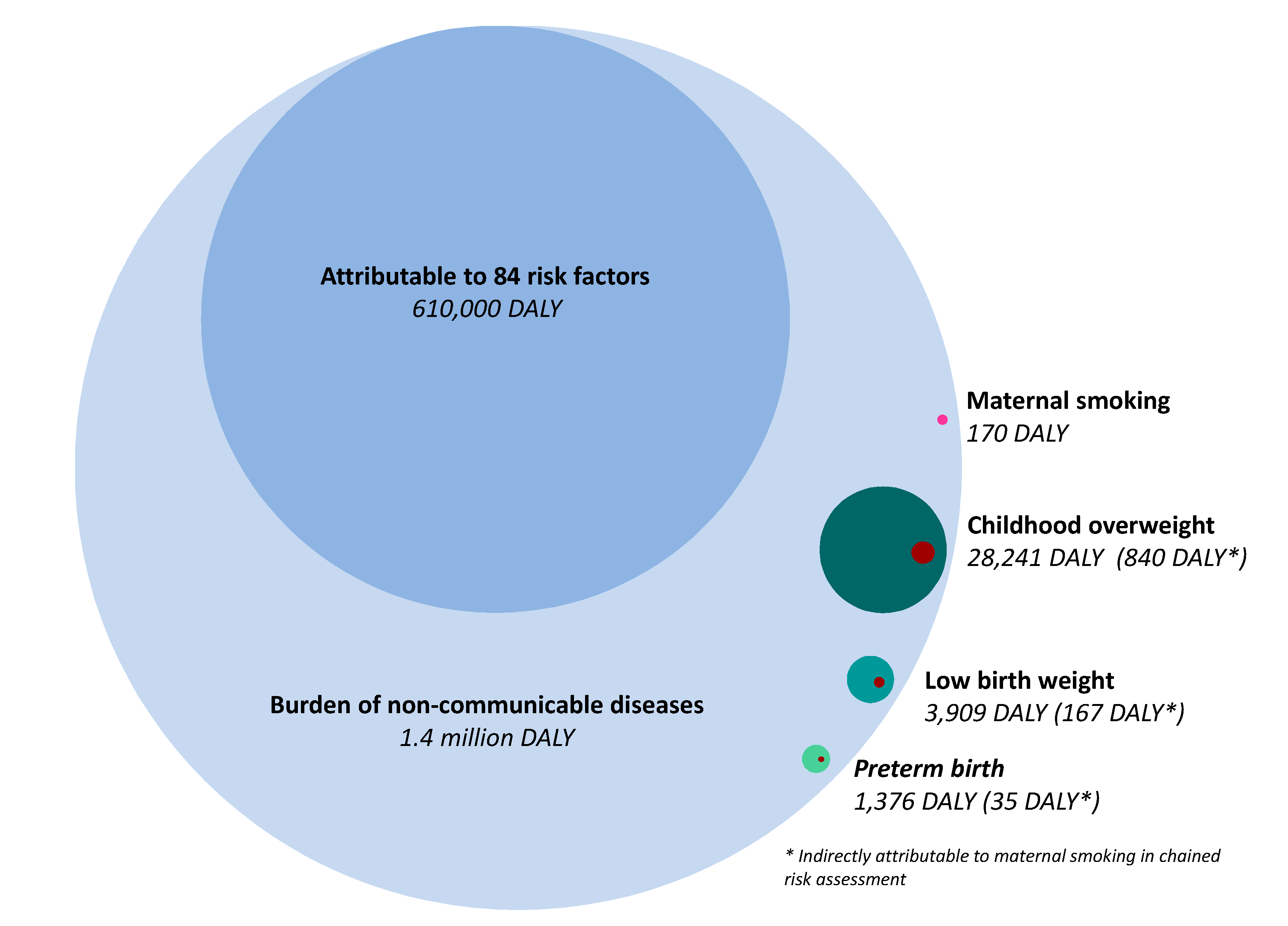
| Sum | 382,388 | 170 | 1376 | 3909 | 28,241 | 33,696 | ||
| Indirectly attributable to maternal smoking | 170 | 35 | 167 | 839 | 1211 | |||
| Indirectly attributable to maternal smoking (%) | 3 % | 4 % | 3 % | 4 % | ||||
| Health Effect | Maternal Smoking | Risk Factor | ||
|---|---|---|---|---|
| Preterm Birth | Low Birth Weight | Childhood Overweight/Obesity | ||
| Cardiovascular diseases | ||||
| Atherosclerosis | [37] | |||
| Cognitive and Mental | ||||
| Pediatric Quality of Life Inventory Index | [38] | |||
| Academic performance | [39] | |||
| Higher education qualification | [40] | |||
| Intelligence | [41] | |||
| Criminal/Deviant behaviour | [42] | |||
| Social benefits | [40] | |||
| Respiratory | ||||
| Wheezing | [43,44] | [45] | [45,46] | |
| Decreased lung function (FEF75, FEV1, FVC) | [47] | [47,48] | ||
| Metabolic | ||||
| Cortisol secretion | [49] | [50] | ||
| Metabolic syndrome | [32] | [51] | ||
| Total cholesterol | [52] | [53] | ||
| Other | ||||
| Congenital anomalies | [54] | |||
| Age at menarche | [55] | |||
| Bone mineral density | [56] | |||
| Periodontal disease | [57] | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rumrich, I.K.; Vähäkangas, K.; Viluksela, M.; Hänninen, O. Chained Risk Assessment for Life-Long Disease Burden of Early Exposures–Demonstration of Concept Using Prenatal Maternal Smoking. Int. J. Environ. Res. Public Health 2020, 17, 1472. https://doi.org/10.3390/ijerph17051472
Rumrich IK, Vähäkangas K, Viluksela M, Hänninen O. Chained Risk Assessment for Life-Long Disease Burden of Early Exposures–Demonstration of Concept Using Prenatal Maternal Smoking. International Journal of Environmental Research and Public Health. 2020; 17(5):1472. https://doi.org/10.3390/ijerph17051472
Chicago/Turabian StyleRumrich, Isabell K., Kirsi Vähäkangas, Matti Viluksela, and Otto Hänninen. 2020. "Chained Risk Assessment for Life-Long Disease Burden of Early Exposures–Demonstration of Concept Using Prenatal Maternal Smoking" International Journal of Environmental Research and Public Health 17, no. 5: 1472. https://doi.org/10.3390/ijerph17051472