Barriers and Facilitators for Screening Older Adults on Fall Risk in a Hospital Setting: Perspectives from Patients and Healthcare Professionals

Abstract
:1. Introduction
2. Materials and Methods
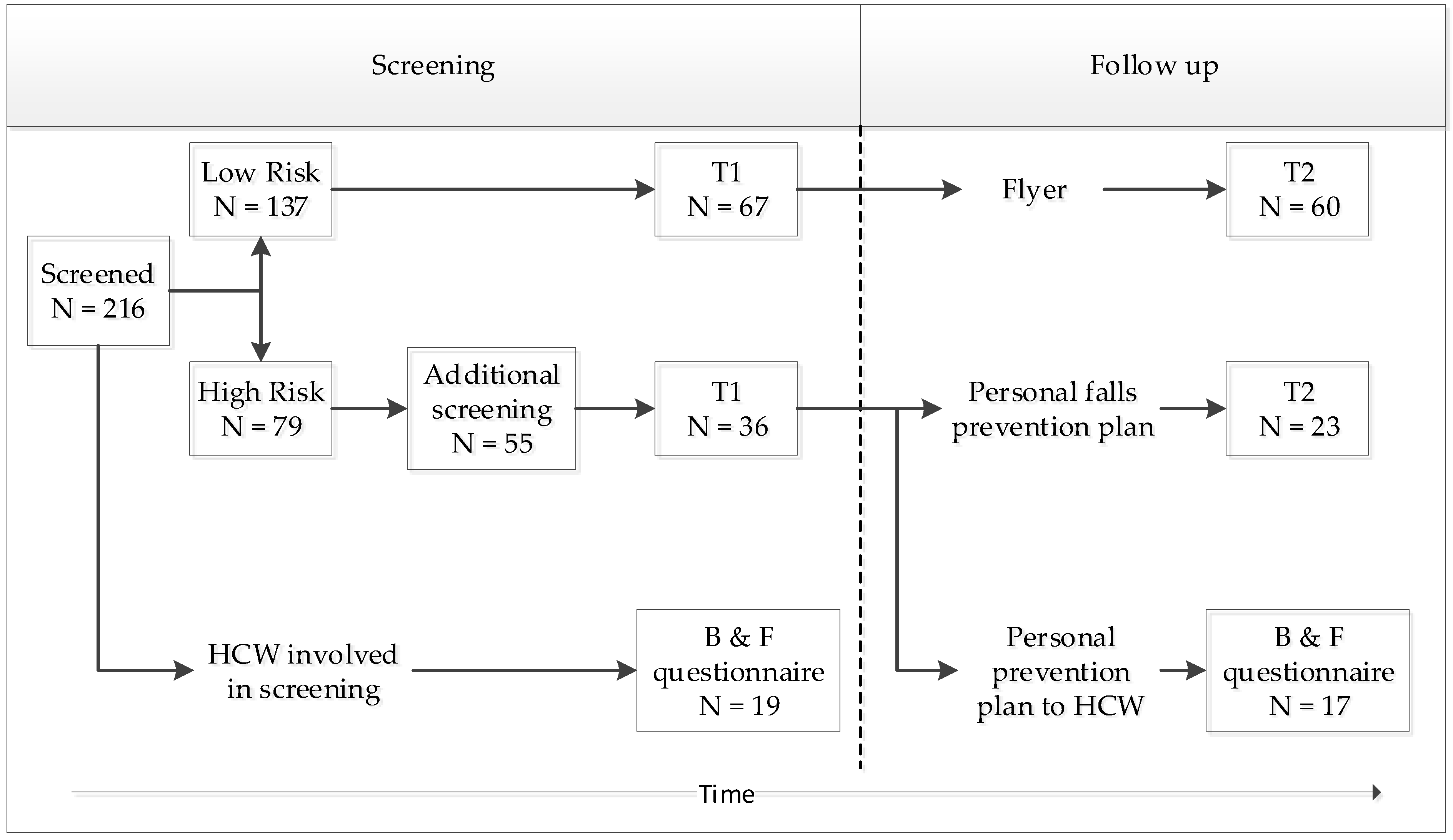
2.1. Study Design and Population
2.2. Screening Program
2.3. Patient Characteristics
2.4. Barriers and Facilitators
2.5. Data Analysis
3. Results
3.1. Sociodemographic Characteristics
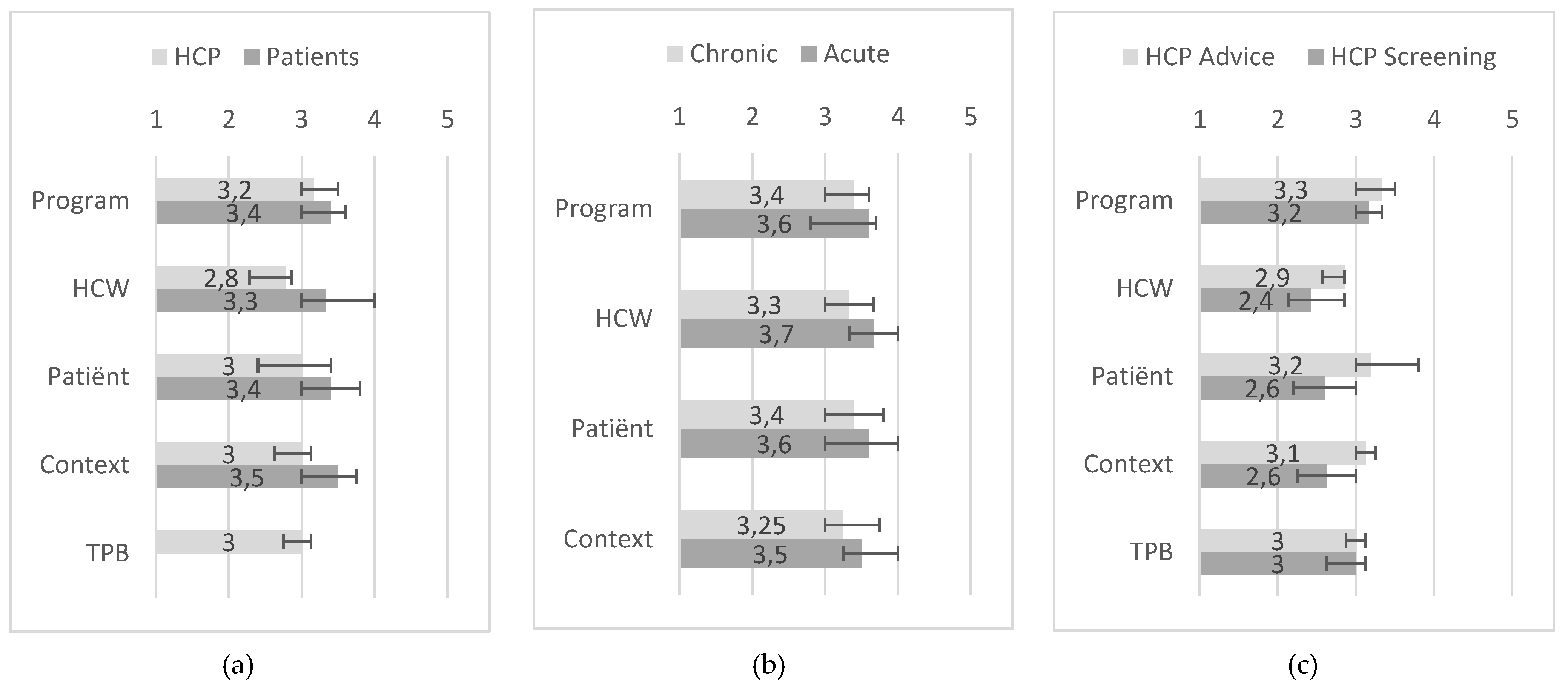
3.2. Barriers and Facilitators of Patients
3.3. Barriers and Facilitators of Healthcare Professionals
3.4. Similarities and Differences in Domains between Patients and Healthcare Professionals
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Statements | Totally Disagree | Disagree | Neutral | Agree | Totally Agree |
|---|---|---|---|---|---|
| 1. I am more open to receiving advice on how to prevent falling. | □ | □ | □ | □ | □ |
| 2. I have a more positive attitude toward fall risk screening and fall prevention. | □ | □ | □ | □ | □ |
| 3. I am more inclined to take action to prevent falling. | □ | □ | □ | □ | □ |
| 4. I can count on more understanding and/or help from those around me to prevent falling. | □ | □ | □ | □ | □ |
| 5. I have more knowledge of actions I can take to prevent a fall. | □ | □ | □ | □ | □ |
| 6. I feel I am more self-sufficient. | □ | □ | □ | □ | □ |
| 7. I am more aware of the risk of falling. | □ | □ | □ | □ | □ |
| 8. I feel more capable of preventing a fall. | □ | □ | □ | □ | □ |
| 9. I did things to prevent falling. | □ | □ | □ | □ | □ |
References
- Haagsma, J.A.; Graetz, N.; Bolliger, I.; Naghavi, M.; Higashi, H.; Mullany, E.C.; Abera, S.F.; Abraham, J.P.; Adofo, K.; Alsharif, U.; et al. The global burden of injury: Incidence, mortality, disability-adjusted life years and time trends from the Global Burden of Disease study 2013. Inj. Prev. 2016, 22, 3–18. [Google Scholar] [CrossRef] [Green Version]
- Nachreiner, N.M.; Findorff, M.J.; Wyman, J.F.; McCarthy, T.C. Circumstances and consequences of falls in community-dwelling older women. J. Womens Health Larchmt 2007, 16, 1437–1446. [Google Scholar] [CrossRef] [PubMed]
- Hartholt, K.A.; Polinder, S.; Van der Cammen, T.J.; Panneman, M.J.; Van der Velde, N.; Van Lieshout, E.M.; Patka, P.; Van Beeck, E.F. Costs of falls in an ageing population: A nationwide study from the Netherlands (2007–2009). Injury 2012, 43, 1199–1203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bergen, G. Falls and fall injuries among adults aged ≥65 years—United States, 2014. MMWR Morb. Mortal. Wkly. Rep. 2016, 65, 993–998. [Google Scholar] [CrossRef] [PubMed]
- Turner, S.; Kisser, R.; Rogmans, W. Falls among Older Adults in the EU-28: Key Facts from the Available Statistics; EuroSafe: Amsterdam, The Netherlands, 2015. [Google Scholar]
- Rubenstein, L.Z.; Josephson, K.R. The epidemiology of falls and syncope. Clin. Geriatr. Med. 2002, 18, 141–158. [Google Scholar] [CrossRef]
- Hartholt, K.A.; van Beeck, E.F.; van der Cammen, T.J.M. Mortality from falls in dutch adults 80 years and older, 2000–2016. JAMA 2018, 319, 1380–1382. [Google Scholar] [CrossRef]
- Houry, D.; Florence, C.; Baldwin, G.; Stevens, J.; McClure, R. The CDC injury center’s response to the growing public health problem of falls among older adults. Am. J. Lifestyle Med. 2016, 10, 74–77. [Google Scholar] [CrossRef]
- VeiligheidNL. Cijferrapportage Valongevallen Ouderen in de Privesfeer 2018. Report Fall Accidents for Older Adults in Private Settings 2018. Available online: https://www.veiligheid.nl/valpreventie/feiten-cijfers/cijferrapportage-valongevallen-ouderen-65--in-priv--sfeer--2018- (accessed on 24 November 2019).
- Chang, J.T.; Morton, S.C.; Rubenstein, L.Z.; Mojica, W.A.; Maglione, M.; Suttorp, M.J.; Roth, E.A.; Shekelle, P.G. Interventions for the prevention of falls in older adults: Systematic review and meta-analysis of randomised clinical trials. BMJ 2004, 328, 680. [Google Scholar] [CrossRef] [Green Version]
- Karlsson, M.K.; Magnusson, H.; von Schewelov, T.; Rosengren, B.E. Prevention of falls in the elderly--a review. Osteoporos. Int. 2013, 24, 747–762. [Google Scholar] [CrossRef]
- Stubbs, B.; Brefka, S.; Denkinger, M.D. What works to prevent falls in community-dwelling older adults? umbrella review of meta-analyses of randomized controlled trials. Phys. Ther. 2015, 95, 1095–1110. [Google Scholar] [CrossRef] [Green Version]
- Tricco, A.C.; Thomas, S.M.; Veroniki, A.A.; Hamid, J.S.; Cogo, E.; Strifler, L.; Khan, P.A.; Robson, R.; Sibley, K.M.; MacDonald, H.; et al. Comparisons of interventions for preventing falls in older adults: A systematic review and meta-analysis. JAMA 2017, 318, 1687–1699. [Google Scholar] [CrossRef] [PubMed]
- Proctor, E.; Silmere, H.; Raghavan, R.; Hovmand, P.; Aarons, G.; Bunger, A.; Griffey, R.; Hensley, M. Outcomes for implementation research: Conceptual distinctions, measurement challenges, and research agenda. Adm. Policy Ment. Health Ment. Health Serv. Res. 2011, 38, 65–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koppelaar, E.; Knibbe, J.J.; Miedema, H.S.; Burdorf, A. Determinants of implementation of primary preventive interventions on patient handling in healthcare: A systematic review. Occup. Environ. Med. 2009, 66, 353–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Child, S.; Goodwin, V.; Garside, R.; Jones-Hughes, T.; Boddy, K.; Stein, K. Factors influencing the implementation of fall-prevention programmes: A systematic review and synthesis of qualitative studies. Implement Sci. 2012, 7, 91. [Google Scholar] [CrossRef]
- Dickinson, A.; Horton, K.; Machen, I.; Bunn, F.; Cove, J.; Jain, D.; Maddex, T. The role of health professionals in promoting the uptake of fall prevention interventions: A qualitative study of older people’s views. Age Ageing 2011, 40, 724–730. [Google Scholar] [CrossRef] [Green Version]
- Southerland, L.T.; Slattery, L.; Rosenthal, J.A.; Kegelmeyer, D.; Kloos, A. Are triage questions sufficient to assign fall risk precautions in the ED? Am. J. Emerg. Med. 2017, 35, 329–332. [Google Scholar] [CrossRef] [Green Version]
- Vrolings, E.G.R. Veiligheidsbarometer 2007: Veiligheidsbeleving van zelfstandig wonende senioren; ResCon: Haarlem, The Netherlands, 2007. [Google Scholar]
- Milisen, K.; Geeraerts, A.; Dejaeger, E. Use of a fall prevention practice guideline for community-dwelling older persons at risk for falling: A feasibility study. Gerontology 2009, 55, 169–178. [Google Scholar] [CrossRef]
- Chou, W.C.; Tinetti, M.E.; King, M.B.; Irwin, K.; Fortinsky, R.H. Perceptions of physicians on the barriers and facilitators to integrating fall risk evaluation and management into practice. J. Gen. Inte. Med. 2006, 21, 117–122. [Google Scholar] [CrossRef]
- Koh, S.S.; Manias, E.; Hutchinson, A.M.; Donath, S.; Johnston, L. Nurses’ perceived barriers to the implementation of a Fall Prevention Clinical Practice Guideline in Singapore hospitals. BMC Health Serv. Res. 2008, 8, 105. [Google Scholar] [CrossRef] [Green Version]
- Bunn, F.; Dickinson, A.; Barnett-Page, E.; McInnes, E.; Horton, K. A systematic review of older people’s perceptions of facilitators and barriers to participation in falls-prevention interventions. Ageing Soc. 2008, 28, 449–472. [Google Scholar] [CrossRef] [Green Version]
- Yardley, L.; Kirby, S.; Ben-Shlomo, Y.; Gilbert, R.; Whitehead, S.; Todd, C. How likely are older people to take up different falls prevention activities? Prev. Med. 2008, 47, 554–558. [Google Scholar] [CrossRef] [PubMed]
- Sibley, K.M.; Voth, J.; Munce, S.E.; Straus, S.E.; Jaglal, S.B. Chronic disease and falls in community-dwelling Canadians over 65 years old: A population-based study exploring associations with number and pattern of chronic conditions. BMC Geriatr. 2014, 14, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- VeiligheidNL. Valanalyse Screeningstool Valrisico Voor De Eerstelijnszorg Fall Analysis, Fall Risk Screening Tool for Primary Care. Available online: https://intranet.onzehuisartsen.nl/file/download/default/A0990575496919D58AF03796C9263DFC/VNL-valanalyse-2017-ONLINE.pdf (accessed on 13 June 2017).
- Peeters, G.; Deeg, D.; Elders, P.; Lips, P. Snelle inschatting van de kans op herhaald vallen bij ouderen. Huisarts Wet. 2012, 2011, 186–191. [Google Scholar] [CrossRef]
- Van der Veen, R.; Kuiper, J.; Martens, M.; Hesseling, A. Screening op Valrisico (Factoren) van Thuiswonende Ouderen Screening of fall Risk (Factors) in Community Dwelling Older Adults; VeiligheidNL: Amsterdam, The Netherlands, 2017. [Google Scholar]
- Saliba, D.; Elliott, M.; Rubenstein, L.Z.; Solomon, D.H.; Young, R.T.; Kamberg, C.J.; Roth, C.; MacLean, C.H.; Shekelle, P.G.; Sloss, E.M.; et al. The Vulnerable Elders Survey: A tool for identifying vulnerable older people in the community. J. Am. Geriatr. Soc. 2001, 49, 1691–1699. [Google Scholar] [CrossRef] [Green Version]
- Peters, M.A.J.; Harmsen, M.; Laurant, M.G.H.; Wensing, M. Ruimte Voor Verandering? Knelpunten en Mogelijkheden voor Verbetering in de Patientenzorg. Room for change? Bottlenecks and Opportunities to Improve Patient Care; UMC St Radboud: Nijmegen, The Netherlands, 2003. [Google Scholar]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Elskamp, A.B.; Hartholt, K.A.; Patka, P.; van Beeck, E.F.; van der Cammen, T.J. Why older people refuse to participate in falls prevention trials: A qualitative study. Exp. Gerontol. 2012, 47, 342–345. [Google Scholar] [CrossRef] [Green Version]
- Carpenter, C.R.; Avidan, M.S.; Wildes, T.; Stark, S.; Fowler, S.A.; Lo, A.X. Predicting geriatric falls following an episode of emergency department care: A systematic review. Acad. Emerg. Med. 2014, 21, 1069–1082. [Google Scholar] [CrossRef] [Green Version]
- Gaboreau, Y.; Imbert, P.; Jacquet, J.P.; Royer De Vericourt, G.; Couturier, P.; Gavazzi, G. Barriers to and promoters of screening for falls in elderly community-dwelling patients by general practitioners: A large cross-sectional survey in two areas of France. Arch. Gerontol. Geriatr. 2016, 65, 85–91. [Google Scholar] [CrossRef]
- Baker, D.I.; King, M.B.; Fortinsky, R.H.; Graff, L.G.t.; Gottschalk, M.; Acampora, D.; Preston, J.; Brown, C.J.; Tinetti, M.E. Dissemination of an evidence-based multicomponent fall risk-assessment and -management strategy throughout a geographic area. J. Am. Geriatr. Soc. 2005, 53, 675–680. [Google Scholar] [CrossRef]
- Flodgren, G.; Hall, A.M.; Goulding, L.; Eccles, M.P.; Grimshaw, J.M.; Leng, G.C.; Shepperd, S. Tools developed and disseminated by guideline producers to promote the uptake of their guidelines. Cochrane Database Syst. Rev. 2016. [Google Scholar] [CrossRef]
- Laws, R.A.; Kemp, L.A.; Harris, M.F.; Davies, G.P.; Williams, A.M.; Eames-Brown, R. An exploration of how clinician attitudes and beliefs influence the implementation of lifestyle risk factor management in primary healthcare: A grounded theory study. Implement. Sci. IS 2009, 4, 66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leeman, J.; Birken, S.A.; Powell, B.J.; Rohweder, C.; Shea, C.M. Beyond “implementation strategies”: Classifying the full range of strategies used in implementation science and practice. Implement. Sci. 2017, 12, 125. [Google Scholar] [CrossRef] [PubMed]
- DeCorby-Watson, K.; Mensah, G.; Bergeron, K.; Abdi, S.; Rempel, B.; Manson, H. Effectiveness of capacity building interventions relevant to public health practice: A systematic review. BMC Public Health 2018, 18, 684. [Google Scholar] [CrossRef] [PubMed] [Green Version]


| Total (n = 103) | Chronic Care (n = 74) | Acute Care (n = 29) | X2 | p-Value | |
|---|---|---|---|---|---|
| N (%) | N (%) | N (%) | |||
| Age in years, median (IQR) | 74.0 (71.0–77.0) | 73.0 (71.0–77.0) | 75.0 (72.5–78.0) | 854.5 | 0.107 |
| Gender | 0.384 | 0.535 | |||
| Female | 27 (26.7) | 18 (25.0) | 9 (31.0) | ||
| Male | 74 (73.3) | 54 (75.0) | 20 (69.0) | ||
| Ethnicity | 0.341 | 0.559 | |||
| Dutch | 87 (89.7) | 62 (88.6) | 25 (92.6) | ||
| Other | 10 (10.3) | 8 (11.4) | 2 (7.4) | ||
| Education level | 0.963 | 0.618 | |||
| Low | 48 (51.6) | 37 (54.4) | 11 (44.0) | ||
| Intermediate | 27 (29.0) | 18 (26.5) | 9 (36.0) | ||
| High | 18 (19.4) | 13 (19.1) | 5 (20.0) | ||
| Living situation | 4.637 | 0.098 | |||
| Independent | 84 (86.6) | 62 (89.9) | 22 (78.6) | ||
| Independent with care | 11 (11.3) | 5 (7.2) | 6 (21.4) | ||
| Care institution | 2 (2.1) | 2 (2.9) | 0 (0.0) | ||
| Living together | 0.687 | 0.407 | |||
| Yes | 75 (76.5) | 52 (74.3) | 23 (82.1) | ||
| No | 23 (23.5) | 18 (25.7) | 5 (17.9) | ||
| Housing type | 1.113 | 0.573 | |||
| Ground floor | 10 (10.3) | 8 (11.6) | 2 (7.1) | ||
| House or flat with stairs | 46 (47.4) | 34 (49.3) | 12 (42.9) | ||
| House or flat with elevator | 41 (42.3) | 27 (39.1) | 14 (50.0) | ||
| Chronic conditions | 3.198 | 0.074 | |||
| At least one | 81 (81.8) | 55 (77.5) | 26 (92.9) | ||
| None | 18 (18.2) | 16 (22.5) | 2 (7.1) | ||
| Elevated fall risk | 0.272 | 0.602 | |||
| Yes | 36 (35.0) | 27 (36.5) | 9 (31.0) | ||
| No | 67 (65.0) | 47 (63.5) | 20 (69.0) | ||
| Fall risk questions (Yes) | |||||
| Fallen in the past year | 36 (35.0) | 24 (32.4) | 12 (41.4) | 0.734 | 0.392 |
| Fallen multiple times | 16 (15.5) | 14 (18.9) | 2 (6.9) | 2.295 | 0.13 |
| Problems moving | 48 (46.6) | 37 (50.0) | 11 (37.9) | 1.22 | 0.269 |
| Afraid of falling | 20 (19.8) | 16 (22.2) | 4 (13.8) | 0.925 | 0.336 |
| All Patients (n = 103) | Chronic Care (n = 74) | Acute Care (n = 29) | Chi-Square | |||||
|---|---|---|---|---|---|---|---|---|
| Negative statements | Domain | agree | disagree | agree | disagree | agree | disagree | p-value |
| % | % | % | % | % | % | |||
| Skills: HCWs do not have the right skills for FRS. | HCW | 16.5 | 44.7 | 18.9 | 39.2 | 10.3 | 58.6 | 0.190 |
| Knowledge: HCWs do not have the right knowledge for FRS. | HCW | 17.6 | 41.2 | 21.9 | 35.6 | 6.9 | 55.2 | 0.096 |
| Health status: I do not appreciate it when people interfere with my health when I did not ask for it. | Patient | 35.3 | 46.1 | 38.4 | 45.2 | 27.6 | 48.3 | 0.500 |
| Ethnicity: Early detection of disease is not concordant with my culture/values. | Patient | 11.0 | 76.0 | 8.3 | 79.2 | 17.9 | 67.9 | 0.359 |
| Financial status: I am afraid FRS will cost me money. | Patient | 19.0 | 58.0 | 22.5 | 57.7 | 10.3 | 58.6 | 0.252 |
| Compatibility: I think FRS is executed at an inconvenient time. | Program | 16.0 | 44.0 | 15.5 | 45.1 | 17.2 | 41.4 | 0.941 |
| Attractiveness: I have negative expectations of FRS. | Program | 11.9 | 59.4 | 12.5 | 59.7 | 10.3 | 58.6 | 0.922 |
| Specificity, flexibility: I do not believe that FRS can detect fall risk at an early stage and prevent deterioration. | Program | 33.3 | 32.4 | 34.2 | 31.5 | 31.0 | 34.5 | 0.941 |
| Didactive benefit: Since I have been screened for fall risk, I am not going to prevent falling in a more active manner. | Program | 28.2 | 30.1 | 25.7 | 29.7 | 34.5 | 31.0 | 0.578 |
| Positive statements | Domain | agree | disagree | agree | disagree | agree | disagree | p-value |
| % | % | % | % | % | % | |||
| Specificity, flexibility: FRS belongs to the duties of nephrology/ED HCWs. | Program | 48.0 | 16.7 | 42.5 | 19.2 | 62.1 | 10.3 | 0.191 |
| Attractiveness: I expect to benefit from FRS. | Program | 59.8 | 10.8 | 54.8 | 11.0 | 72.4 | 10.3 | 0.210 |
| Time investment: I have enough time to be screened for fall risk. | Context | 75.2 | 13.9 | 75.3 | 15.1 | 75.0 | 10.7 | 0.709 |
| Supportive staff: There are enough staff at the nephrology/ED department to screen for fall risk. | Context | 35.4 | 18.2 | 32.9 | 17.1 | 41.4 | 20.7 | 0.547 |
| Facilities: The nephrology/ED department is an appropriate place for FRS. | Context | 47.5 | 25.3 | 43.1 | 27.8 | 59.3 | 18.5 | 0.350 |
| Group norms, socialization: People in my surroundings that are important to me would participate in FRS. | Context | 40.6 | 15.8 | 36.1 | 13.9 | 51.7 | 20.7 | 0.121 |
| Motivation to change: I feel a need to be screened for fall risk. | Patient | 43.6 | 32.7 | 40.3 | 34.7 | 51.7 | 27.6 | 0.575 |
| Motivation to change: Since I have been screened for fall risk, I am more aware of my risks of falling. | Patient | 37.9 | 26.2 | 35.1 | 27.0 | 44.8 | 24.1 | 0.653 |
| Screening (n = 19) | Follow up Advice (n = 17) | ||||
|---|---|---|---|---|---|
| Negative statements | Domain | agree | disagree | agree | disagree |
| % | % | % | % | ||
| Compatibility: The fall-prevention program does not fit into my ways of working at my practice. | Program | 36.8 | 21.1 | 11.8 | 5.9 |
| Time investment: Working to the fall-prevention program is too time consuming. | Program | 36.8 | 36.8 | 11.8 | 35.3 |
| Attitude, role perception: I have a general resistance to working according protocols. | HCW | 78.9 | 5.3 | 52.9 | 0.0 |
| Doubts about innovation: I think parts of the fall-prevention program are incorrect. | HCW | 47.4 | 5.3 | 47.1 | 0.0 |
| Lifestyle, working style: I have problems changing my old routines. | HCW | 73.7 | 15.8 | 76.5 | 0.0 |
| Education: It is difficult to give preventive care because I am not trained in giving preventive care. | HCW | 42.1 | 21.1 | 17.6 | 47.1 |
| Practice involvement: I did not thoroughly read nor remember the fall-prevention program. | HCW | 78.9 | 10.5 | 52.9 | 17.6 |
| Setup involvement: It is difficult to give preventive care because I have not been involved in setting up the preventive care. | HCW | 31.6 | 47.4 | 5.9 | 64.7 |
| Knowledge, motivation: I wish to know more about this fall-prevention program before I decide to apply it. | HCW | 36.8 | 21.1 | 29.4 | 52.9 |
| Ethnicity: It is difficult to give this preventive care to patients with a different cultural background. | Patient | 31.6 | 57.9 | 11.8 | 41.2 |
| Financial situation, economic status: It is difficult to give this preventive care to patients with a low socioeconomic status. | Patient | 52.6 | 26.3 | 17.6 | 35.3 |
| Number of patient contacts: It is difficult to give this preventive care to patients who rarely visit the clinic. | Patient | 52.6 | 26.3 | 5.9 | 58.8 |
| Health status: It is difficult to give this preventive care to patients who seem healthy. | Patient | 47.4 | 26.3 | 5.9 | 58.8 |
| Motivation to change: Patients do not cooperate in applying this fall-prevention program. | Patient | 84.2 | 5.3 | 29.4 | 17.6 |
| Group norms, socialization: Colleagues from my discipline do not cooperate in applying the fall-prevention program. | Context | 36.8 | 15.8 | 47.1 | 11.8 |
| Group norms, socialization: Colleagues from other disciplines do not cooperate in applying the fall-prevention program. | Context | 21.1 | 21.1 | 17.6 | 5.9 |
| Group norms, socialization: Managers/directors do not cooperate in applying the fall-prevention program. | Context | 57.9 | 5.3 | 35.3 | 0.0 |
| Reimbursement, insurance system: Working according to this fall-prevention program requires financial compensation. | Context | 15.8 | 21.1 | 11.8 | 5.9 |
| Opening hours of practice: It is difficult to give preventive care because the timing of the preventative care is awkward. | Context | 36.8 | 26.3 | 11.8 | 41.2 |
| Supportive staff: It is difficult to give preventive care if there are not enough supportive staff. | Context | 26.3 | 42.1 | 11.8 | 76.5 |
| Facilities: It is difficult to give preventive care if instruments needed are not available. | Context | 63.2 | 15.8 | 5.9 | 41.2 |
| Practice building: It is difficult to give preventive care if physical space is lacking (e.g., rooms). | Context | 57.9 | 21.1 | 23.5 | 47.1 |
| Attitude: This fall-prevention program is useless. | TPB | 73.7 | 5.3 | 29.4 | 11.8 |
| Attitude: This fall-prevention program is unwise. | TPB | 68.4 | 0.0 | 35.3 | 0.0 |
| Positive statements | Domain | agree | disagree | agree | disagree |
| % | % | % | % | ||
| Specificity, flexibility: This fall-prevention program leaves enough room for me to make my own conclusions. | Program | 47.4 | 5.3 | 41.2 | 11.8 |
| Specificity, flexibility: This fall-prevention program leaves enough room to weigh the wishes of the patient. | Program | 47.4 | 5.3 | 47.1 | 5.9 |
| Didactive benefit: This fall-prevention program is a good starting point for my self-study. | Program | 15.8 | 21.1 | 47.1 | 29.4 |
| Attractiveness: The layout of this fall-prevention program makes it handy for use. | Program | 63.2 | 15.8 | 47.1 | 11.8 |
| Attitude: This fall-prevention program is appropriate. | TPB | 73.7 | 0.0 | 29.4 | 5.9 |
| Attitude: This fall-prevention program important. | TPB | 63.2 | 5.3 | 29.4 | 0.0 |
| Subjective norm: Colleagues that I identify with would apply this fall-prevention program. | TPB | 31.6 | 10.5 | 0.0 | 17.6 |
| Perceived behavioral control: I believe that when I apply this fall-prevention program I can prevent falls. | TPB | 21.1 | 15.8 | 52.9 | 5.9 |
| Intention: I am willing to structurally apply this fall-prevention program to all my future patients aged 70 years and older. | TPB | 36.8 | 21.1 | 5.9 | 23.5 |
| Behavior: I have applied this fall-prevention program to patients in the past. | TPB | 31.6 | 63.2 | 41.2 | 41.2 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barmentloo, L.M.; Dontje, M.L.; Koopman, M.Y.; Olij, B.F.; Oudshoorn, C.; Mackenbach, J.P.; Polinder, S.; Erasmus, V. Barriers and Facilitators for Screening Older Adults on Fall Risk in a Hospital Setting: Perspectives from Patients and Healthcare Professionals. Int. J. Environ. Res. Public Health 2020, 17, 1461. https://doi.org/10.3390/ijerph17051461
Barmentloo LM, Dontje ML, Koopman MY, Olij BF, Oudshoorn C, Mackenbach JP, Polinder S, Erasmus V. Barriers and Facilitators for Screening Older Adults on Fall Risk in a Hospital Setting: Perspectives from Patients and Healthcare Professionals. International Journal of Environmental Research and Public Health. 2020; 17(5):1461. https://doi.org/10.3390/ijerph17051461
Chicago/Turabian StyleBarmentloo, Lotte M., Manon L. Dontje, Moniek Y. Koopman, Branko F. Olij, Christian Oudshoorn, Johan P. Mackenbach, Suzanne Polinder, and Vicki Erasmus. 2020. "Barriers and Facilitators for Screening Older Adults on Fall Risk in a Hospital Setting: Perspectives from Patients and Healthcare Professionals" International Journal of Environmental Research and Public Health 17, no. 5: 1461. https://doi.org/10.3390/ijerph17051461