Does Physical Activity Regulate Prostate Carcinogenesis and Prostate Cancer Outcomes? A Narrative Review

 , ,
, ,  , , , , ,
, , , , , {kind=link}
Abstract
:1. Introduction
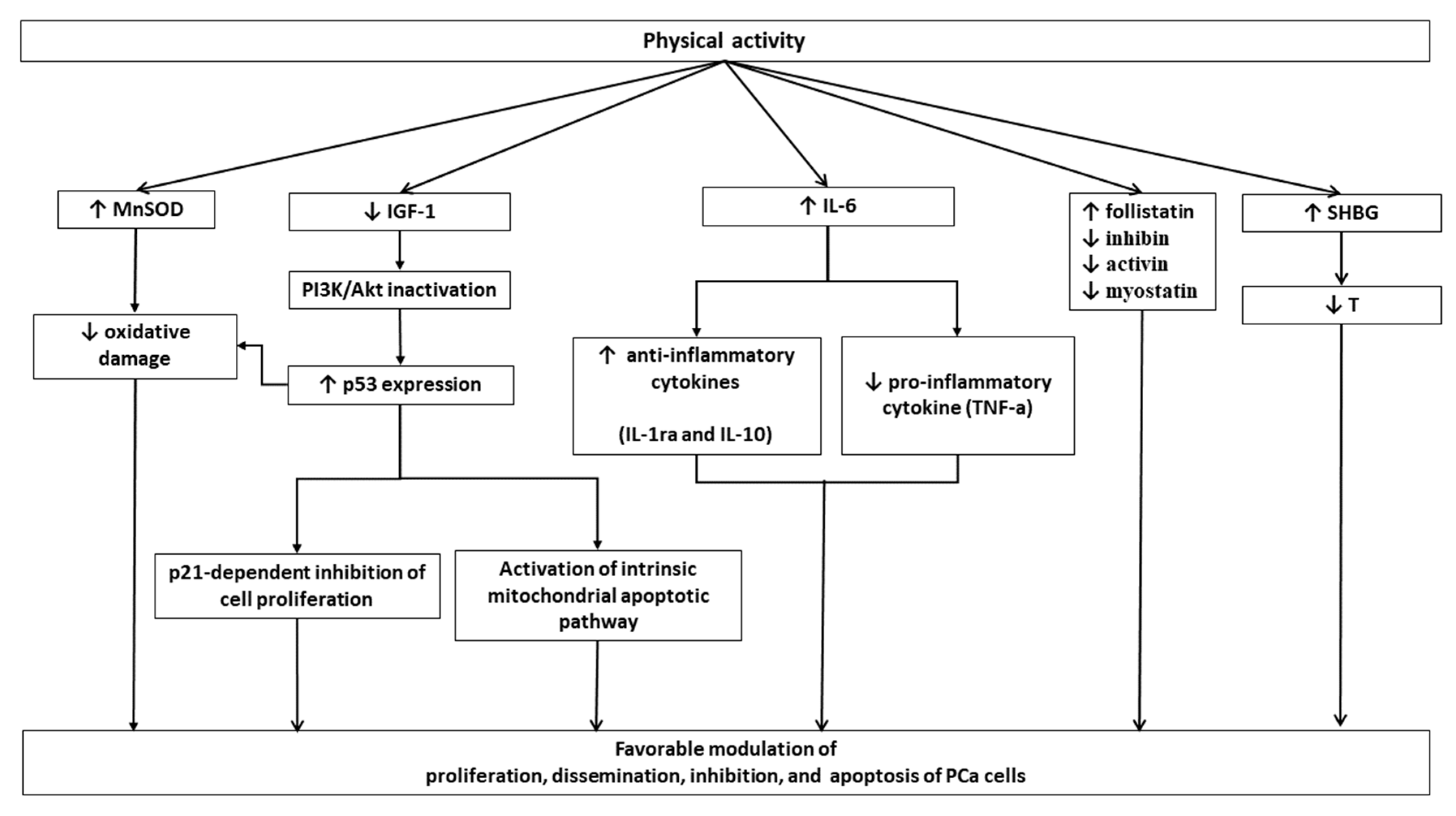
1.1. Physical Activity and Prostate Cancer: Pathophysiological Links
1.2. Physical Activity and Prostate Cancer Risk
1.3. Physical Activity and Prostate Cancer Mortality
1.4. Physical Activity and PCa-Related Functional Outcomes
1.5. Physical Activity and Androgen Deprivation Therapy—Related Toxicity
2. Discussion
3. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Stangelberger, A.; Waldert, M.; Djavan, B. Prostate cancer in elderly men. Rev. Urol. 2008, 10, 111–119. [Google Scholar]
- Moyad, M.A.; Newton, R.U.; Tunn, U.W.; Gruca, D. Integrating diet and exercise into care of prostate cancer patients on androgen deprivation therapy. Res. Rep. Urol. 2016, 8, 133–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rawla, P. Epidemiology of Prostate Cancer. World J. Oncol. 2019, 10, 63–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shephard, R.J. Physical Activity and Prostate Cancer: An Updated Review. Sports Med. 2017, 47, 1055–1073. [Google Scholar] [CrossRef] [PubMed]
- Thandi, M.K.G.; Phinney, A.; Oliffe, J.L.; Wong, S.; McKay, H.; Sims-Gould, J.; Sahota, S. Engaging Older Men in Physical Activity: Implications for Health Promotion Practice. Am. J. Men’s Health 2018, 12, 2064–2075. [Google Scholar] [CrossRef]
- Kushi, L.H.; Byers, T.; Doyle, C.; Bandera, E.V.; McCullough, M.; McTiernan, A.; Gansler, T.; Andrews, K.S.; Thun, M.J.; American Cancer Society 2006 Nutrition and Physical Activity Guidelines Advisory Committee. American Cancer Society guidelines on nutrition and physical activity for cancer prevention: Reducing the risk of cancer with healthy food choices and physical activity. CA Cancer J. Clin. 2006, 56, 254–281. [Google Scholar] [CrossRef]
- Wiseman, M. The second World Cancer Research Fund/American Institute for Cancer Research expert report. Food, nutrition, physical activity, and the prevention of cancer: A global perspective. Proc. Nutr. Soc. 2008, 67, 253–256. [Google Scholar] [CrossRef] [Green Version]
- McTiernan, A. Mechanisms linking physical activity with cancer. Nat. Rev. Cancer 2008, 8, 205–211. [Google Scholar] [CrossRef]
- Kruijsen-Jaarsma, M.; Revesz, D.; Bierlings, M.B.; Buffart, L.M.; Takken, T. Effects of exercise on immune function in patients with cancer: A systematic review. Exerc. Immunol. Rev. 2013, 19, 120–143. [Google Scholar]
- Laszlo, R.; Hartveg, P.; Laszlo, S.; Otto, S.; Procopchuk, D.; Steinacker, J.M. Physical activity and cancer. OA Sports Med. 2014, 2, 1. [Google Scholar]
- Capece, M.; Gillo, A.; Cocci, A.; Garaffa, G.; Timpano, M.; Falcone, M. Management of refractory ischemic priapism: Current perspectives. Res. Rep. Urol. 2017, 9, 175–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neuhouser, M.L.; Schenk, J.; Song, Y.J.; Tangen, C.M.; Goodman, P.J.; Pollak, M.; Penson, D.F.; Thompson, I.M.; Kristal, A.R. Insulinlike growth factor-1, insulin-like growth factor binding protein-3 and risk of benign prostate hyperplasia in the prostate cancer prevention trial. Prostate 2008, 68, 1477–1486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leung, P.S.; Aronson, W.J.; Ngo, T.H.; Golding, L.A.; Barnard, R.J. Exercise alters the IGF axis in vivo and increases p53 protein in prostate tumor cells in vitro. J. Appl. Physiol. 2004, 96, 450–454. [Google Scholar] [CrossRef] [Green Version]
- Clarke, G.; Whittemore, A.S. Prostate cancer risk in relation to anthropometry and physical activity: The National Health and Nutrition Examination Survey I Epidemiological Follow-Up Study. Cancer Epidemiol. Biomark. Prev. 2000, 9, 875–881. [Google Scholar]
- Wiklund, F.; Lageros, Y.T.; Chang, E.; Bälter, K.; Johansson, J.-E.; Adami, H.-O.; Grönberg, H. Lifetime total physical activityand prostate cancer risk: A population-based case–control study in Sweden. Eur. J. Epidemiol. 2008, 23, 739–746. [Google Scholar] [CrossRef] [PubMed]
- MacInnis, R.; English, D. Body size and composition and prostate cancer risk: Systematic review and meta-regression analysis. Cancer Causes Control. 2006, 17, 989–1003. [Google Scholar] [CrossRef]
- Ngo, T.H.; Barnard, R.J.; Tymchuk, C.N.; Cohen, P.; Aronson, W.J. Effect of diet and exercise on serum insulin, IGF-I, and IGFBP-1 levels and growth of LNCaP cells in vitro (United States). Cancer Causes Control 2002, 13, 929–935. [Google Scholar] [CrossRef]
- Kruk, J.; Aboul-Enein, H. What Are the Links of Prostate Cancer with Physical Activity and Nutrition?: A Systematic Review Article. Iran. J. Public Health 2016, 45, 1558–1567. [Google Scholar]
- Winzer, B.M.; Whiteman, D.C.; Reeves, M.; Paratz, J.D. Physical activity and cancer prevention: A systematic review of clinical trials. Cancer Causes Control 2011, 22, 811–826. [Google Scholar] [CrossRef]
- Friedenreich, C.; Thune, I. A review of physical activity and prostate cancer risk. Cancer Causes Control 2001, 12, 461–475. [Google Scholar] [CrossRef]
- Rebillard, A.; Lefeuvre-Orfila, L.; Gueritat, J.; Cillard, J. Prostate cancer and physical activity: Adaptive response to oxidative stress. Free Radic. Biol. Med. 2013, 60, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Renehan, A.G.; Zwahlen, M.; Minder, C.; O’Dwyer, S.T.; Shalet, S.M.; Egger, M. Insulin-like growth factor (IGF)-I, IGF binding protein-3, and cancer risk: Systematic review and meta-regression analysis. Lancet 2004, 363, 1346–1353. [Google Scholar] [CrossRef]
- Cohen, D.H.; LeRoith, D. Obesity, type 2 diabetes, and cancer: The insulin and IGF connection. Endocr. Relat. Cancer 2012, 19, F27–F45. [Google Scholar] [CrossRef] [PubMed]
- Jones, J.I.; Clemmons, D.R. Insulin-like growth factors and their binding proteins: Biological actions. Endocr. Rev. 1995, 16, 3–34. [Google Scholar] [CrossRef]
- Rangul, V.; Sund, E.R.; Mork, P.J.; Røe, O.D.; Bauman, A. The associations of sitting time and physical activity on total and site-specific cancer incidence: Results from the HUNT study, Norway. PLoS ONE 2018, 13. [Google Scholar] [CrossRef]
- Wekesa, A.; Harrison, M.; Watson, R.W. Physical activity and its mechanistic effects on prostate cancer. Prostate Cancer Prostatic Dis. 2015, 18, 197–207. [Google Scholar] [CrossRef]
- Khandrika, L.; Kumar, B.; Koul, S.; Maroni, P.; Koul, H.K. Oxidative stress in prostate cancer. Cancer Lett. 2009, 282, 125–136. [Google Scholar] [CrossRef] [Green Version]
- Ripple, M.O.; Henry, W.F.; Rago, R.P.; Wilding, G. Prooxidant- antioxidant shift induced by androgen treatment of human prostate carcinoma cells. J. Natl. Cancer Inst. 1997, 89, 40–48. [Google Scholar] [CrossRef] [Green Version]
- Wilding, G. Endocrine control of prostate cancer. Cancer Surv. 1995, 23, 43–62. [Google Scholar]
- Hayes, J.D.; Pulford, D.J. The glutathione S-transferase supergene family: Regulation of GST and the contribution of the isoenzymes to cancer chemo protection and drug resistance. Crit. Rev. Biochem. Mol. Biol. 1995, 30, 445–600. [Google Scholar] [CrossRef]
- Zhu, M.; Fahl, W.E. Functional characterization of transcription regulators that interact with the electrophile response element. Biochem. Biophys. Res. Commun. 2001, 289, 212–219. [Google Scholar] [CrossRef] [PubMed]
- Frohlich, D.A.; McCabe, M.T.; Arnold, R.S.; Day, M.L. The role of Nrf2 in increased reactive oxygen species and DNA damage in prostate tumorigenesis. Oncogene 2008, 27, 4353–4362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nelson, W.G.; deMarzo, A.M.; deWeese, T.L.; Isaacs, W.B. The role of inflammation in the pathogenesis of prostate cancer. J. Urol. 2004, 172, S6–S11. [Google Scholar] [CrossRef] [PubMed]
- Nomikos, N.N.; Nikolaidis, P.T.; Sousa, C.V.; Papalois, A.E.; Rosemann, T.; Knechtle, B. Exercise, Telomeres, and Cancer: “The Exercise-Telomere Hypothesis”. Front. Physiol. 2018, 9, 1798. [Google Scholar] [CrossRef] [Green Version]
- Zheng, Q.; Cui, G.; Chen, J.; Gao, H.; Wei, Y.; Uede, T.; Chen, Z.; Diao, H. Regular exercise enhances the immune response against microbial antigens through up-regulation of toll-like receptor signaling pathways. Cell Physiol. Biochem. 2015, 37, 735–746. [Google Scholar] [CrossRef] [PubMed]
- Etzioni, R.; Cha, R.; Feuer, E.; Davidov, O. Asymptomatic incidence and duration of prostate cancer. Am. J. Epidemiol. 1998, 148, 775–785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Hu, F.; Li, D.; Wang, F.; Zhu, L.; Chen, W.; Ge, J.; An, R.; Zha, Y. Does physical activity reduce the risk of prostate cancer? A systematic review and meta-analysis. Eur. Urol. 2011, 60. [Google Scholar] [CrossRef]
- Sormunen, J.; Talibov, M.; Sparén, P.; Martinsen, J.I.; Weiderpass, E.; Pukkala, E. Perceived Physical Strain at Work and Incidence of Prostate Cancer-a Case-Control Study in Sweden and Finland. Asian Pac. J. Cancer Prev. 2018, 19, 2331–2335. [Google Scholar] [CrossRef]
- Benke, I.N.; Leitzmann, M.F.; Behrens, G.; Schmid, D. Physical activity in relation to risk of prostate cancer: A systematic review and meta-analysis. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2018, 29, 1154–1179. [Google Scholar] [CrossRef]
- Liu, F.; Wang, J.; Wu, H.L.; Wang, H.; Wang, J.X.; Zhou, R.; Zhu, Z. Leisure time physical activity and risk of prostate cancer: A dose-response meta-analysis. Minerva Urol. Nefrol. 2018, 70, 152–161. [Google Scholar]
- Kazmi, N.; Haycock, P.; Tsilidis, K.; Lynch, B.M.; Truong, T.; Martin, R.M.; Lewis, S. Appraising causal relationships of dietary, nutritional and physical-activity exposures with overall and aggressive prostate cancer: Two-sample Mendelian-randomization study based on 79,148 prostate-cancer cases and 61,106 controls. Int. J. Epidemiol. 2019, dyz235. [Google Scholar] [CrossRef] [PubMed]
- Kenfield, S.A.; Stampfer, M.J.; Giovannucci, E.; Chan, J.M. Physical activity and survival after prostate cancer diagnosis in the health professionals follow-up study. J. Clin. Oncol. 2011, 29, 726–732. [Google Scholar] [CrossRef] [PubMed]
- Friedenreich, C.M.; Wang, Q.; Neilson, H.K.; Kopciuk, K.A.; McGregor, S.E.; Courneya, K.S. Physical Activity and Survival After Prostate Cancer. Eur. Urol. 2016, 70, 576–585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newton, R.U.; Kenfield, S.A.; Hart, N.H.; Chan, J.M.; Courneya, K.S.; Catto, J.; Finn, S.P.; Greenwood, R.; Hughes, D.C.; Mucci, L.; et al. Intense Exercise for Survival among Men with Metastatic Castrate-Resistant Prostate Cancer (INTERVAL-GAP4): A multicentre, randomised, controlled phase III study protocol. BMJ Open 2018, 8, e022899. [Google Scholar] [CrossRef] [PubMed]
- Langelier, D.M.; Cormie, P.; Bridel, W.; Grant, C.; Albinati, N.; Shank, J.; Daun, J.T.; Fung, T.S.; Davey, C.; Culos-Reed, S.N. Perceptions of masculinity and body image in men with prostate cancer: The role of exercise. Support Care Cancer 2018, 26, 3379–3388. [Google Scholar] [CrossRef] [PubMed]
- Livingston, P.M.; Craike, M.J.; Salmon, J.; Courneya, K.S.; Gaskin, C.J.; Fraser, S.F.; Mohebbi, M.; Broadbent, S.; Botti, M.; Kent, B.; et al. Effects of a clinician referral and exercise program for men who have completed active treatment for prostate cancer: A multicenter cluster randomized controlled trial (ENGAGE). Cancer 2015, 121, 2646–2654. [Google Scholar] [CrossRef] [Green Version]
- Boisen, S.; Krägeloh, C.; Shepherd, D.; Ryan, C.; Masters, J.; Osborne, S.; MacLeod, R.D.; Gray, M.; Keogh, J.W. A Cross-Sectional Comparison of Quality of Life Between Physically Active and Underactive Older Men With Prostate Cancer. J. Aging Phys. Act. 2016, 24, 642–648. [Google Scholar] [CrossRef] [Green Version]
- Neefjes, E.C.; Van Den Hurk, R.M.; Blauwhoff-Buskermolen, S.; van der Vorst, M.J.; Becker-Commissaris, A.; de van der Schueren, M.A.; Buffart, L.M.; Verheul, H.M.W. Muscle mass as a target to reduce fatigue in patients with advanced cancer. J. Cachexia Sarcopenia Muscle 2017, 8, 623–629. [Google Scholar] [CrossRef]
- Galvão, D.A.; Taaffe, D.R.; Spry, N.; Cormie, P.; Joseph, D.; Chambers, S.K.; Chee, R.; Peddle-McIntyre, C.J.; Hart, N.H.; Baumann, F.T.; et al. Exercise Preserves Physical Function in Prostate Cancer Patients with Bone Metastases. Med. Sci. Sports Exerc. 2018, 50, 393–399. [Google Scholar] [CrossRef] [Green Version]
- Vashistha, V.; Singh, B.; Kaur, S.; Prokop, L.J.; Kaushik, D. The Effects of Exercise on Fatigue, Quality of Life, and Psychological Function for Men with Prostate Cancer: Systematic Review and Meta-analyses. Eur. Urol. Focus 2016, 2, 284–295. [Google Scholar] [CrossRef]
- Hojan, K.; Kwiatkowska-Borowczyk, E.; Leporowska, E.; Górecki, M.; Ozga-Majchrzak, O.; Milecki, T.; Milecki, P. Physical exercise for functional capacity, blood immune function, fatigue, and quality of life in high-risk prostate cancer patients during radiotherapy: A prospective, randomized clinical study. Eur. J. Phys. Rehabil. Med. 2016, 52, 489–501. [Google Scholar] [PubMed]
- Phillips, S.M.; Stampfer, M.J.; Chan, J.M.; Giovannucci, E.L.; Kenfield, S.A. Physical activity, sedentary behavior, and health-related quality of life in prostate cancer survivors in the health professionals follow-up study. J. Cancer Surviv. 2015, 9, 500–511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Falcone, M.; Pucci, L.; Garaffa, G.; Cocci, A.; Gillo, A.; Capece, M.; Ceruti, C.; Timpano, M.; Sedigh, O.; Preto, M.; et al. An outcomes analysis of penile prosthesis implantation following radical cystoprostatectomy and urinary diversion: A multicentric retrospective cohort study. Int. J. Impot. Res. 2019. [Google Scholar] [CrossRef] [PubMed]
- Verze, P.; Capece, M.; Califano, G.; La Rocca, R. Two-piece inflatable and semi-rigid penile implants: An effective alternative? Int. J. Impot. Res. 2019. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, P.L.; Alibhai, S.M.; Basaria, S.; D’Amico, A.V.; Kantoff, P.W.; Keating, N.L.; Penson, D.F.; Rosario, D.J.; Tombal, B.; Smith, M.R. Adverse effects of androgen deprivation therapy and strategies to mitigate them. Eur. Urol. 2015, 67, 825–836. [Google Scholar] [CrossRef] [PubMed]
- Verze, P.; Greco, F.; Scuzzarella, S.; Bottone, F.; Palmieri, A.; Cucchiara, V.; Arcaniolo, D.; Imperatore, V.; Creta, M.; Mirone, V. The impact of previous prostate surgery on the outcomes of laparoscopic radical prostatectomy. Minerva Urol. Nefrol. 2017, 69, 76–84. [Google Scholar] [CrossRef]
- Cormie, P.; Zopf, E.M. Exercise medicine for the management of androgen deprivation therapy-related side effects in prostate cancer. Urol. Oncol. 2018. [Google Scholar] [CrossRef]
- Bourke, L.; Doll, H.; Crank, H.; Daley, A.; Rosario, D.; Saxton, J.M. Lifestyle intervention in men with advanced prostate cancer receiving androgen suppression therapy: A feasibility study. Cancer Epidemiol. Biomark. Prev. 2011, 20, 647–657. [Google Scholar] [CrossRef] [Green Version]
- Taaffe, D.R.; Newton, R.U.; Spry, N.; Joseph, D.; Chambers, S.K.; Gardiner, R.A.; Wall, B.A.; Cormie, P.; Bolam, K.A.; Galvão, D.A. Effects of Different Exercise Modalities on Fatigue in Prostate Cancer Patients Undergoing Androgen Deprivation Therapy: A Year-long Randomised Controlled Trial. Eur. Urol. 2017, 72, 293–299. [Google Scholar] [CrossRef] [Green Version]
- Cormie, P.; Galvão, D.A.; Spry, N.; Joseph, D.; Chee, R.; Taaffe, D.R.; Chambers, S.K.; Newton, R.U. Can supervised exercise prevent treatment toxicity in patients with prostate cancer initiating androgen-deprivation therapy: A randomised controlled trial. BJU Int. 2015, 115, 256–266. [Google Scholar] [CrossRef] [Green Version]
- Mennen-Winchell, L.J.; Grigoriev, V.; Alpert, P.; Dos Santos, H.; Tonstad, S. Self-reported exercise and bone mineral density in prostate cancer patients receiving androgen deprivation therapy. J. Am. Assoc. Nurse Pract. 2014, 26, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, K.; Chambers, S.K.; Legg, M.; Oliffe, J.L.; Cormie, P. Sexuality and exercise in men undergoing androgen deprivation therapy for prostate cancer. Support. Care Cancer 2015, 23, 133–142. [Google Scholar] [CrossRef] [PubMed]
- Palmieri, A.; Silvani, M.; Giammusso, B.; Liguori, G.; Mondaini, N.; Palumbo, F. A “real life” investigation on the prescriptive habits among Italian andrologists: The “CONSER” survey from Italian Society of Andrology (SIA) on Sildenafil oral film. Arch. Ital. Urol. Androl. 2019, 91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Z.; Zhang, Y.; Lu, C.; Zeng, H.; Schumann, M.; Cheng, S. Supervised Physical Training Enhances Muscle Strength but Not Muscle Mass in Prostate Cancer Patients Undergoing Androgen Deprivation Therapy: A Systematic Review and Meta-Analysis. Front. Physiol. 2019, 10, 843. [Google Scholar] [CrossRef] [Green Version]

© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Capece, M.; Creta, M.; Calogero, A.; La Rocca, R.; Napolitano, L.; Barone, B.; Sica, A.; Fusco, F.; Santangelo, M.; Dodaro, C.; et al. Does Physical Activity Regulate Prostate Carcinogenesis and Prostate Cancer Outcomes? A Narrative Review. Int. J. Environ. Res. Public Health 2020, 17, 1441. https://doi.org/10.3390/ijerph17041441
Capece M, Creta M, Calogero A, La Rocca R, Napolitano L, Barone B, Sica A, Fusco F, Santangelo M, Dodaro C, et al. Does Physical Activity Regulate Prostate Carcinogenesis and Prostate Cancer Outcomes? A Narrative Review. International Journal of Environmental Research and Public Health. 2020; 17(4):1441. https://doi.org/10.3390/ijerph17041441
Chicago/Turabian StyleCapece, Marco, Massimiliano Creta, Armando Calogero, Roberto La Rocca, Luigi Napolitano, Biagio Barone, Antonello Sica, Ferdinando Fusco, Michele Santangelo, Concetta Dodaro, and et al. 2020. "Does Physical Activity Regulate Prostate Carcinogenesis and Prostate Cancer Outcomes? A Narrative Review" International Journal of Environmental Research and Public Health 17, no. 4: 1441. https://doi.org/10.3390/ijerph17041441