Impact of Urbanization on PM2.5-Related Health and Economic Loss in China 338 Cities


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Methodology
2.2.1. Health Risks Assessment
2.2.2. Relative Risk and Baseline Incidence Rate
2.2.3. Economic Loss Estimate
3. Results and Discussion
3.1. Spatial Distribution of PM2.5 Pollution and Urbanization
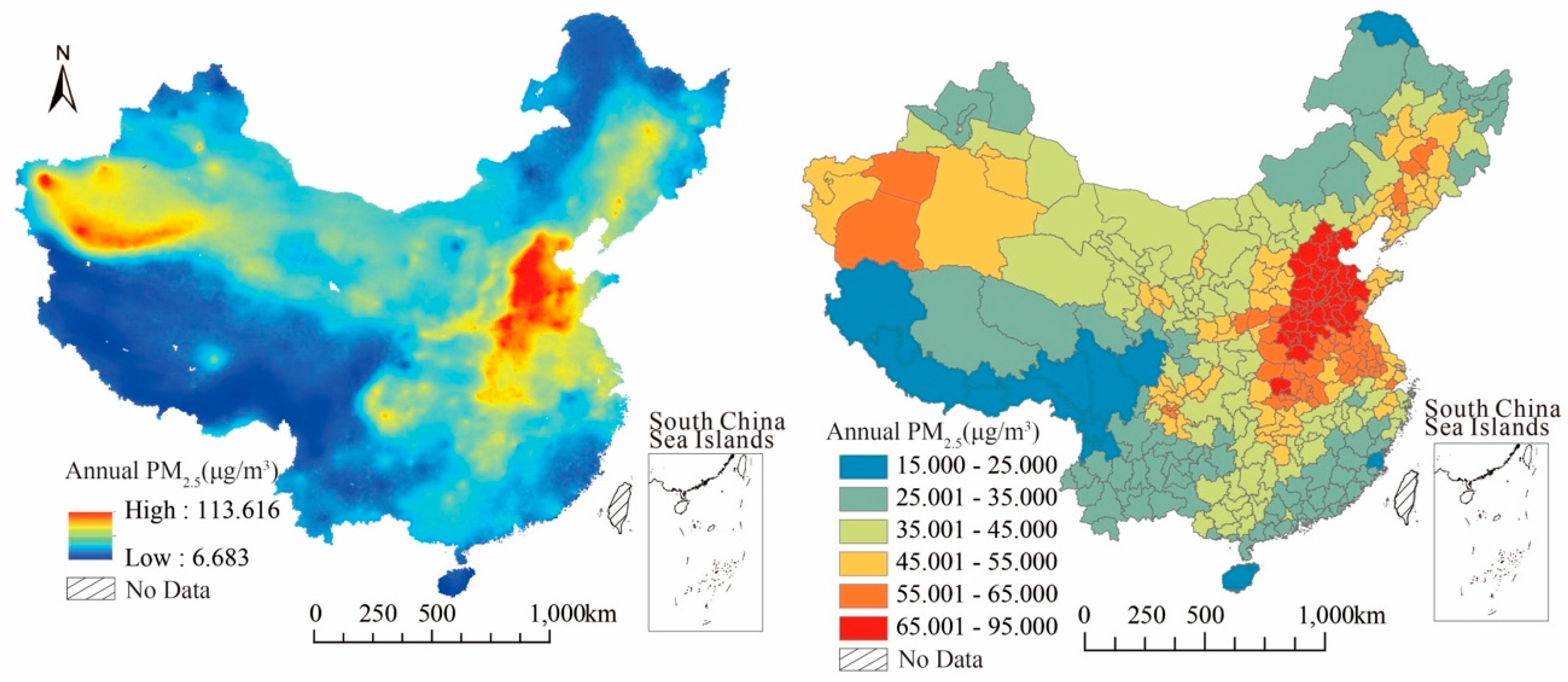
3.1.1. Spatial Distribution Characteristics of PM2.5 Concentration
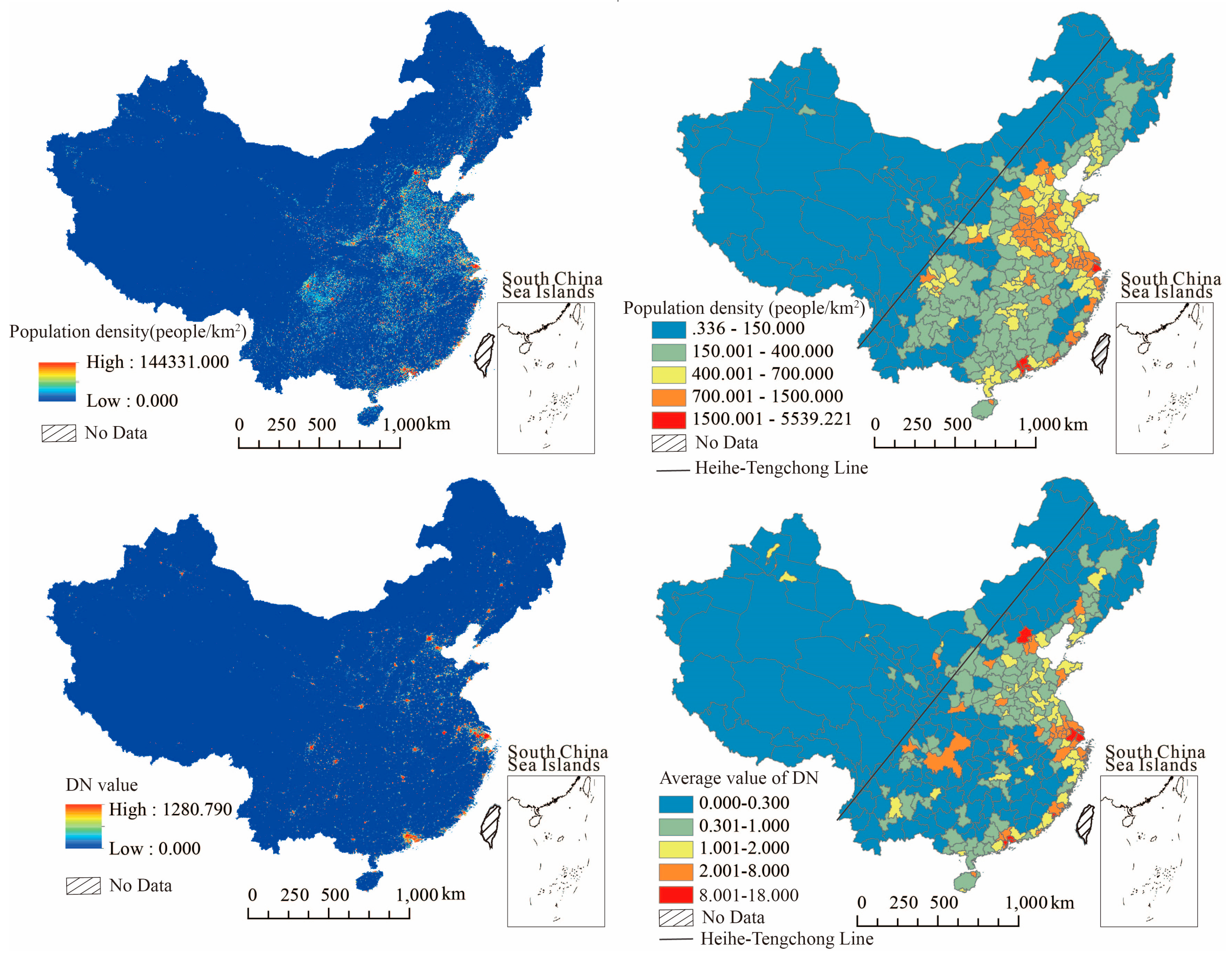
3.1.2. Spatial Distribution Characteristics of Population Density and Urbanization Level
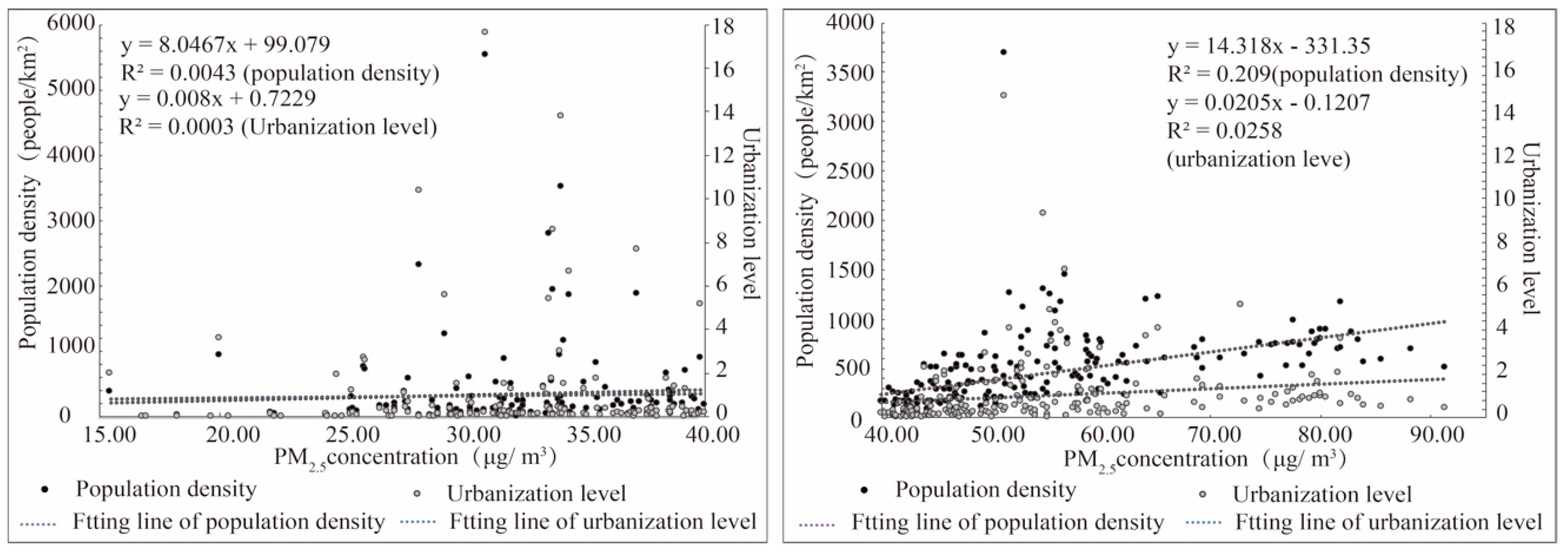
3.1.3. Relationship between PM2.5 Concentration and Population Density as Well as Urbanization
3.2. Health Risks and Economic Loss of PM2.5 Pollution
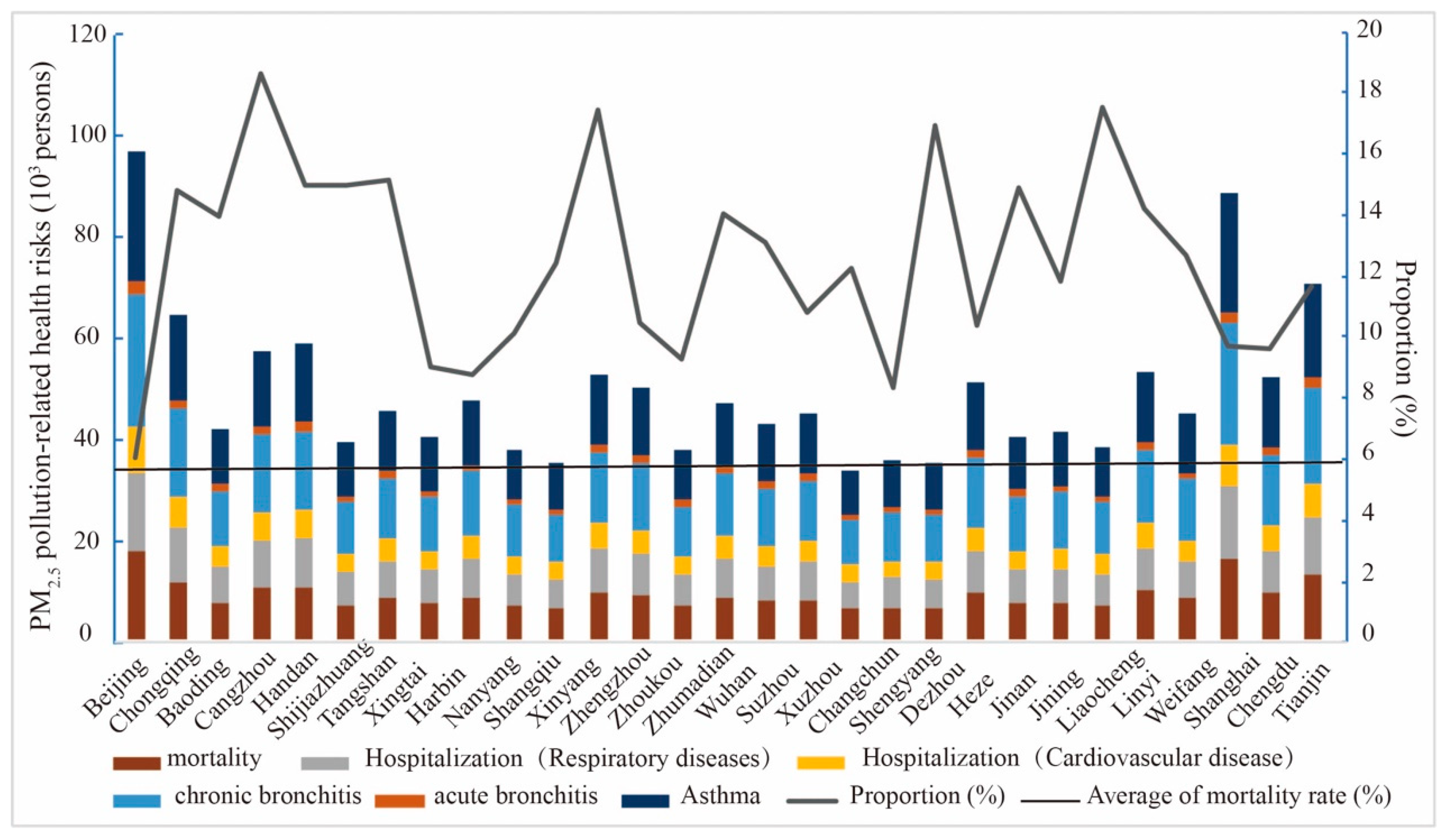
3.2.1. Assessment of Health Risks Changes Based on Exposure Response Function
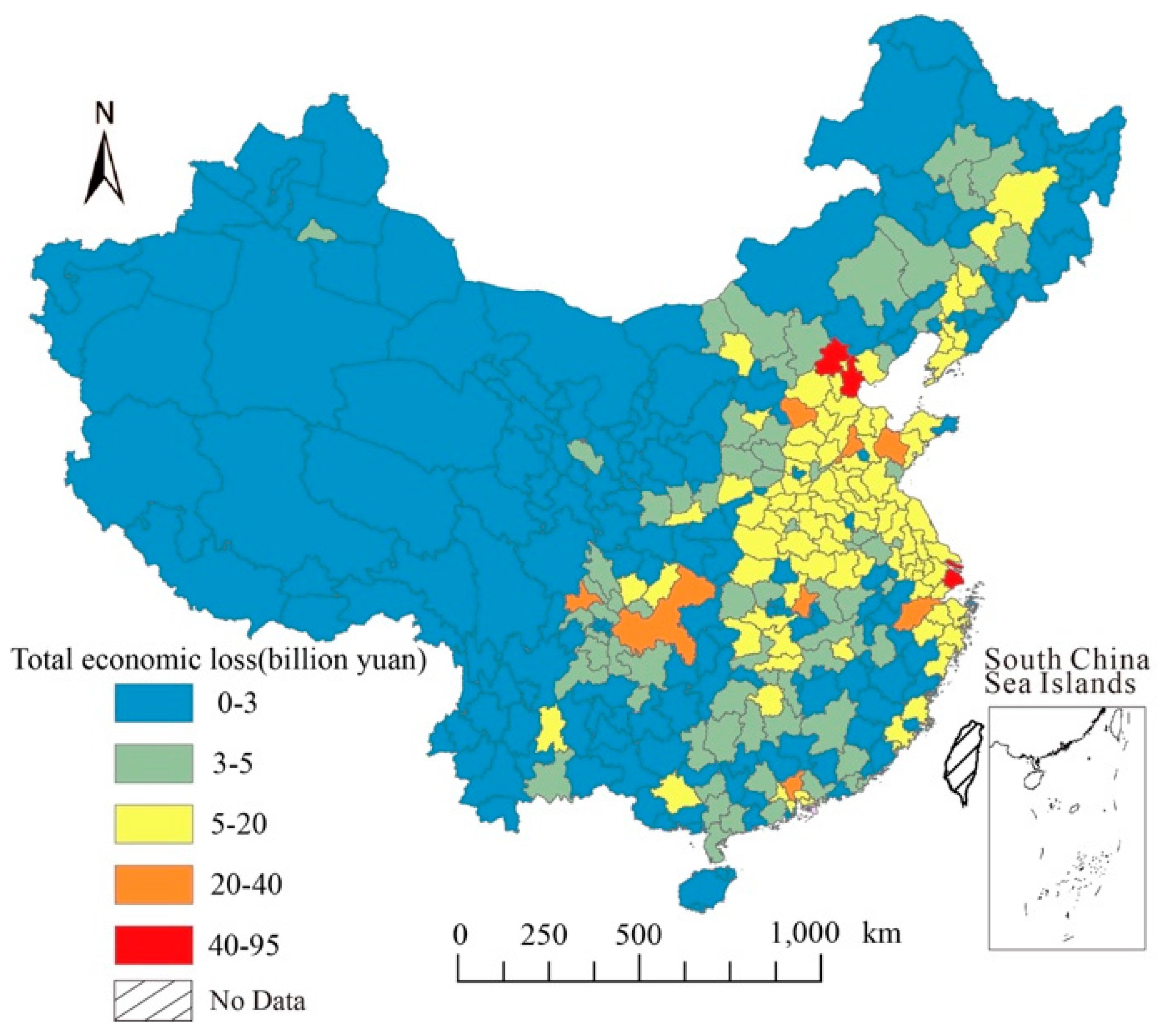
3.2.2. Economic Loss of Health Risks
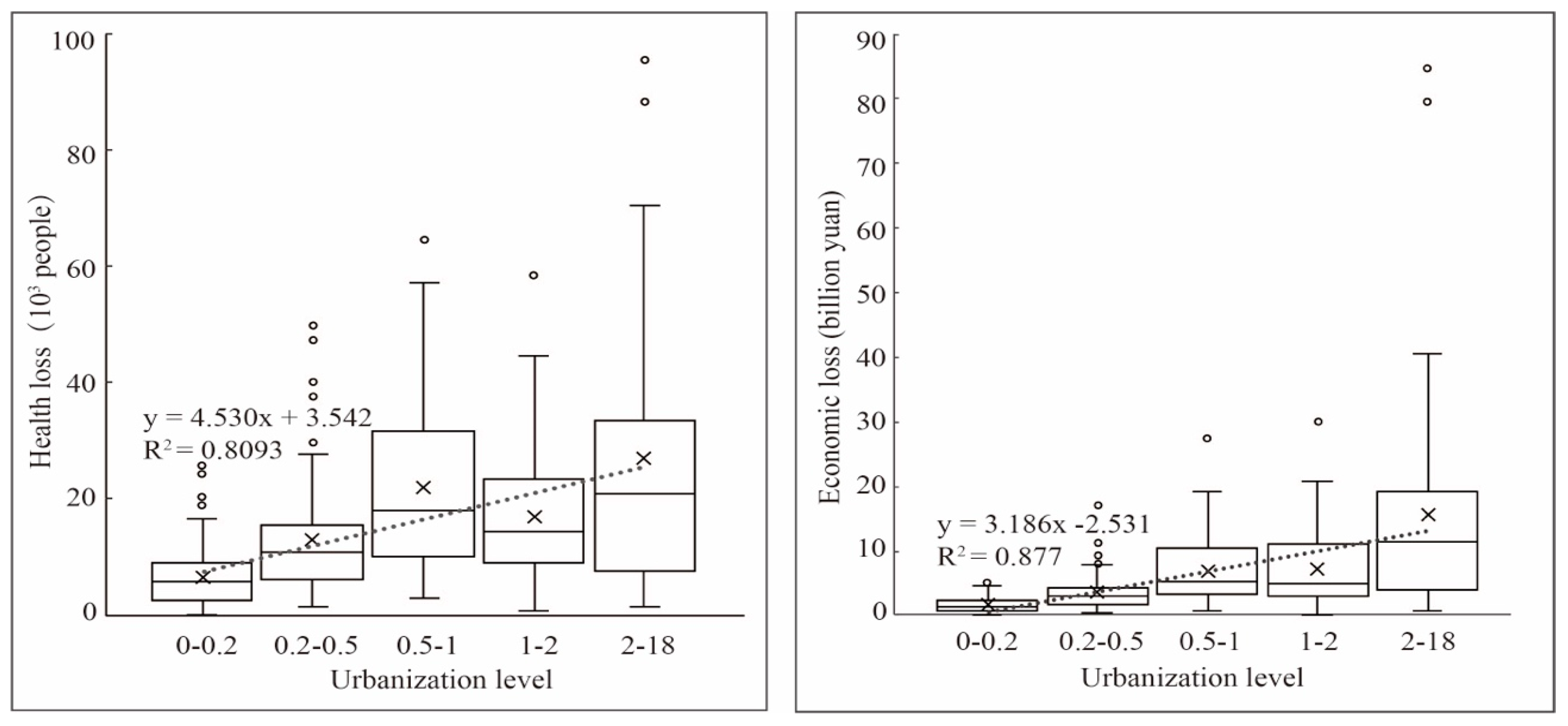
3.2.3. Health Risks and Economic Loss under Different Urbanization Levels
3.3. Zoning Control and Policy Recommendations
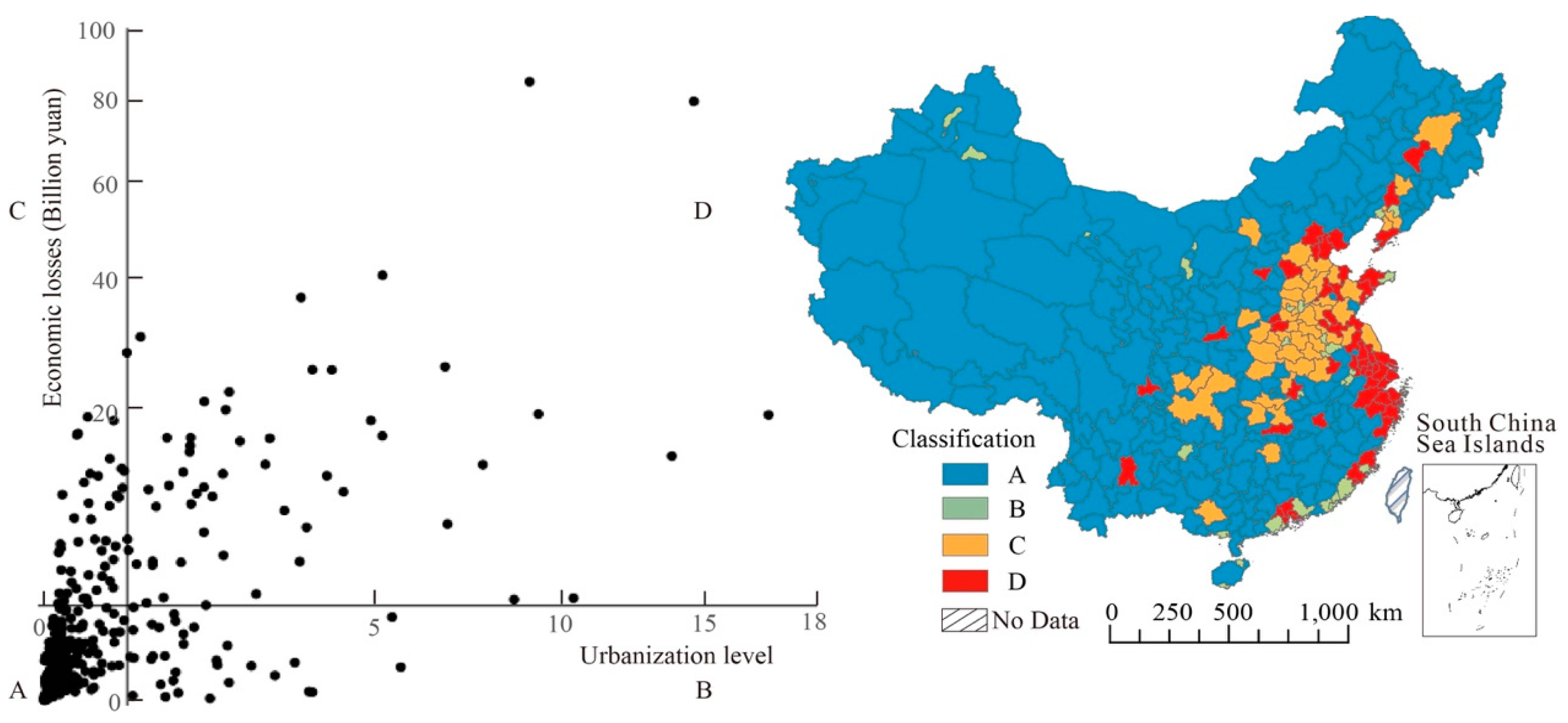
3.3.1. Regional Classification and Management
3.3.2. Policy Implications
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Lin, R.S.; Sung, F.C.; Huang, S.L.; Gou, Y.L.; Gou, H.W.; Shaw, C.K. Role of urbanization and air pollution in adolescent asthma: A mass screening in Taiwan. J. Formos. Med. Assoc. 2001, 100, 649–655. Available online: http://www.fma.org.tw/jfma/PDF/2001-100/issue_10/Article_1.pdf (accessed on 10 July 2001).
- Guan, Y.; Kang, L.; Wang, Y.; Zhang, N.N.; Ju, M.T. Health loss attributed to PM2.5 pollution in China’s cities: Economic impact, annual change and reduction potential. J. Clean. Prod. 2019, 217, 284–294. [Google Scholar] [CrossRef]
- Liu, M.; Huang, Y.; Jin, Z.; Ma, Z.; Liu, X.; Zhang, B.; Kinney, P.L. The nexus between urbanization and PM2.5 related mortality in China. Environ. Pollut. 2017, 227, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Wang, C.; Zhang, G.; Xiao, L.; Dixon, J. Urbanization and human health in China: Spatial features and a systemic perspective. Environ. Sci. Pollut. Res. 2012, 19, 1375. [Google Scholar] [CrossRef] [PubMed]
- Gong, P.; Liang, S.; Carlton, E.J.; Jiang, Q.; Wu, J.; Wang, L.; Remais, J.V. Urbanisation and health in China. Lancet 2012, 379, 843–852. [Google Scholar] [CrossRef]
- Du, C.W.; Feng, K. Does urbanization cause air pollution? Empirical evidence from emerging economies. Comp. Econ. Soc. Syst. 2012, 9, 91–99. (In Chinese) [Google Scholar]
- Galea, S.; Vlahov, D. Urban health: Evidence, challenges, and directions. Annu. Rev. Public Health 2005, 26, 341–365. [Google Scholar] [CrossRef] [Green Version]
- Rydin, Y.; Bleahu, A.; Davies, M.; Dávila, J.D.; Friel, S.; De Grandis, G.; Lai, K.M. Shaping cities for health: Complexity and the planning of urban environments in the 21st century. Lancet 2016, 379, 2079–2108. [Google Scholar] [CrossRef] [Green Version]
- Miao, J.; Wu, X. Urbanization, socioeconomic status and health disparity in China. Health Place 2014, 42, 87–95. [Google Scholar] [CrossRef]
- Eckert, S.; Kohler, S. Urbanization and health in developing countries: A systematic review. World Health Popul. 2014, 15, 7–20. Available online: https://pdfs.semanticscholar.org/339c/8cbc6e87de9e41ae781fb217b85ea06bfe36.pdf (accessed on 1 February 2014). [CrossRef]
- Fischer, P.H.; Marra, M.; Ameling, C.B.; Hoek, G.; Beelen, R.; Hoogh, K.D.; Breugelmans, O.; Kruize, H.; Janssen, N.A.H.; Houthuijs, D. Air pollution and mortality in seven million adults: The Dutch Environmental Longitudinal Study (DUELS). Environ. Health Perspect. 2012, 123, 697–704. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maji, K.J.; Ye, W.F.; Arora, M.; Nagendra, S.M.S. PM2.5-related health and economic loss assessment for 338 Chinese cities. Environ. Int. 2018, 121, 392–403. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Zhu, Y.; Kelly, J.T.; Li, J.; Zhu, Y.; Kelly, J.T.; Jang, C.J.; Wang, S.; Hanna, A.; Yu, L. Health benefit assessment of PM2.5 reduction in Pearl River Delta region of China using a model-monitor data fusion approach. J. Environ. Manag. 2019, 233, 489–498. [Google Scholar] [CrossRef]
- Leem, J.H.; Kim, S.T.; Kim, H.C. Public-health impact of outdoor air pollution for 2nd air pollution management policy in Seoul metropolitan area, Korea. Ann. Occup. Environ. Med. 2015, 27, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, X.; Lin, C.; Li, W.; Chen, Y.; Huang, Y.; Fung, J.C.; Lau, A.K. Analysis of the adverse health effects of PM2.5 from 2001 to 2017 in China and the role of urbanization in aggravating the health burden. Sci. Total Environ. 2019, 652, 683–695. [Google Scholar] [CrossRef] [PubMed]
- Graff Zivin, J.; Neidell, M. The impact of pollution on worker productivity. Am. Econ. Rev. 2012, 102, 3652–3673. Available online: https://www.nber.org/papers/w17004.pdf (accessed on 1 December 2012). [CrossRef] [Green Version]
- Hanna, R.; Oliva, P. The effect of pollution on labor supply: Evidence from a natural experiment in Mexico City. J. Public Econ. 2015, 122, 68–79. [Google Scholar] [CrossRef] [Green Version]
- Deryugina, T.; Heutel, G.; Miller, N.H.; Molitor, D.; Reif, J. The mortality and medical costs of air pollution: Evidence from changes in wind direction. Natl. Bur. Econ. Res. 2019, 109, 4178–4219. Available online: https://www.nber.org/papers/w22796 (accessed on 1 December 2019). [CrossRef]
- Pope, C.A., III; Ezzati, M.; Dockery, D.W. Fine-particulate air pollution and life expectancy in the United States. N. Eng. J. Med. 2016, 360, 376–386. [Google Scholar] [CrossRef] [Green Version]
- Pérez, L.; Sunyer, J.; Künzli, N. Estimating the health and economic benefits associated with reducing air pollution in the Barcelona metropolitan area (Spain). Gac. Sanit. 2009, 23, 287–294. [Google Scholar] [CrossRef] [Green Version]
- Li, H.J.; Zhou, D.Q.; Wei, Y.J. An assessment of PM2.5-related health risks and associated economic losses in Chinese cities. Environ. Sci. 2018, 39, 3467. [Google Scholar] [CrossRef]
- Crouse, D.L.; Peters, P.A.; Hystad, P.; Brook, J.R.; Donkelaar, A.V.; Martin, R.V.; Villeneuve, P.J.; Jerrett, M.; Goldberg, M.S.; Pope, C.A., III; et al. Ambient PM2.5, O3, and NO2 exposures and associations with mortality over 16 years of follow-up in the Canadian census health and environment cohort. Environ. Health Perspect. 2015, 123, 1180–1186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fang, D.; Wang, Q.; Li, H.; Yu, Y.; Lu, Y.; Qian, X. Mortality effects assessment of ambient PM2.5 pollution in the 74 leading cities of China. Sci. Total Environ. 2016, 569, 1545–1552. [Google Scholar] [CrossRef] [PubMed]
- Jaafar, H.; Razi, N.A.; Azzeri, A.; Isahak, K.; Dahlui, M. A systematic review of financial implications of air pollution on health in Asia. Environ. Sci. Pollut. Res. 2018, 25, 30009–30020. [Google Scholar] [CrossRef] [PubMed]
- Zeng, X.G.; Xie, F.; Zong, Q. Behavior selection and willingness to pay of reducing PM2.5 health risk: Taking residents in Beijing as an example. China Pop. Res. Environ. 2015, 2015, 127–133. (In Chinese) [Google Scholar]
- Huang, D.S.; Zhang, S.Q. Health benefit evaluation for PM2.5 pollution control in Beijing-Tianjin-Hebei region of China. China Environ. Sci. 2013, 33, 166–174. (In Chinese) [Google Scholar]
- Wang, Q.; Wang, J.; He, M.Z.; Kinney, P.L.; Li, T. A county-level estimate of PM2.5 related chronic mortality risk in China based on multi-model exposure data. Environ. Int. 2018, 110, 105–112. [Google Scholar] [CrossRef] [Green Version]
- Li, T.; Zhang, Y.; Wang, J.; Xu, D.; Yin, Z.; Chen, H.; Kinney, P.L. All-cause mortality risk associated with long-term exposure to ambient PM2.5 in China: A cohort study. Lancet Public Health 2016, 3, e470–e477. [Google Scholar] [CrossRef] [Green Version]
- Zheng, Y.; Zhang, Q.; Liu, Y.; Geng, G.; He, K. Estimating ground-level PM2.5 concentrations over three megalopolises in China using satellite-derived aerosol optical depth measurements. Atmos. Environ. 2018, 124, 232–242. [Google Scholar] [CrossRef]
- Dobson, J.; Bright, E.; Coleman, P.; Durfee, R.; Worley, B. A global population database for estimating populations at risk. Photogramm. Eng. Remote Sens. 2000, 66, 849–857. Available online: https://www.researchgate.net/publication/267450852 (accessed on 16 May 2019).
- Xie, Y.; Dai, H.; Dong, H.; Hanaoka, T.; Masui, T. Economic impacts from PM2.5 pollution-related health effects in China: A provincial-level analysis. Environ. Sci. Technol. 2016, 50, 4836–4843. [Google Scholar] [CrossRef] [PubMed]
- Van Donkelaar, A.; Martin, R.V.; Li, C.; Burnett, R.T. Regional estimates of chemical composition of fine particulate matter using a combined geoscience-statistical method with information from satellites, models, and monitors. Environ. Sci. Technol. 2019, 53, 2595–2611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, L.; Zhou, W.; Li, W.; Li, L. Impact of urbanization level on urban air quality: A case of fine particles (PM2.5) in Chinese cities. Environ. Pollut. 2014, 194, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Seto, K.C. Mapping urbanization dynamics at regional and global scales using multi-temporal DMSP/OLS nighttime light data. Remote Sens. Environ. 2011, 115, 2320–2329. [Google Scholar] [CrossRef]
- Shao, S.; Li, X.; Cao, J.H. Urbanization promotion and haze pollution governance in China. Econ. Res. 1999, 54, 148–165. (In Chinese) [Google Scholar]
- Elvidge, C.D.; Baugh, K.E.; Dietz, J.B.; Bland, T.; Sutton, P.C.; Kroehl, H. Radiance calibration of DMSP-OLS low-light imaging data of human settlements. Remote Sens. Environ. 2019, 68, 77–88. [Google Scholar] [CrossRef]
- Ma, T.; Zhou, C.; Pei, T.; Haynie, S.; Fan, J. Quantitative estimation of urbanization dynamics using time series of DMSP/OLS nighttime light data: A comparative case study from China’s cities. Remote Sens. Environ. 2012, 124, 99–107. [Google Scholar] [CrossRef]
- Zhao, M.; Cheng, W.; Zhou, C.; Li, M.; Huang, K.; Wang, N. Assessing spatiotemporal characteristics of urbanization dynamics in southeast Asia using time series of DMSP/OLS nighttime light data. Remote Sens. 2018, 10, 47. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Wang, Y.; Peng, J.; Du, Y.; Liu, X.; Li, S.; Zhang, D. Correlations between urbanization and vegetation degradation across the world’s metropolises using DMSP/OLS nighttime light data. Remote Sens. 2015, 7, 2067–2088. [Google Scholar] [CrossRef] [Green Version]
- Ma, T.; Yin, Z.; Zhou, A. Delineating spatial patterns in human settlements using VIIRS nighttime light data: A watershed-based partition approach. Remote Sens. 2018, 10, 465. [Google Scholar] [CrossRef] [Green Version]
- Apte, J.S.; Marshall, J.D.; Cohen, A.J.; Brauer, M. Addressing global mortality from ambient PM2.5. Environ. Sci. Technol. Lett. 2015, 49, 8057–8066. [Google Scholar] [CrossRef] [PubMed]
- Apte, J.S.; Brauer, M.; Cohen, A.J.; Ezzati, M.; Pope, C.A. Ambient PM2.5 reduces global and regional life expectancy. Environ. Sci. Technol. Lett. 2018, 5, 546–551. [Google Scholar] [CrossRef] [Green Version]
- Zheng, S.; Pozzer, A.; Cao, C.X.; Lelieveld, J. Long-term (2001–2012) concentrations of fine particulate matter (PM2.5) and the impact on human health in Beijing, China. Atmos. Chem. Phys. 2015, 15, 5715. [Google Scholar] [CrossRef] [Green Version]
- Pope, C.A., III; Burnett, R.T.; Thun, M.J.; Calle, E.E.; Krewski, D.; Ito, K.; Thurston, G.D. Lung cancer, cardiopulmonary mortality, and long-term exposure to fine particulate air pollution. JAMA 2002, 287, 1132–1141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dockery, D.W.; Pope, C.A.; Xu, X.P.; Spengler, J.D. An association between air pollution and mortality in six US cities. N. Engl. J. Med. 1993, 329, 1753–1759. [Google Scholar] [CrossRef] [Green Version]
- Abrahamowicz, M.; Schopflocher, T.; Leffondré, K.; du Berger, R.; Krewski, D. Flexible modeling of exposure-response relationship between long-term average levels of particulate air pollution and mortality in the American Cancer Society study. J. Toxicol. Environ. Health A 2003, 66, 1625. [Google Scholar] [CrossRef]
- Wang, G.Z.; Wu, L.Y.; Chen, J.B.; Song, Y.X.; Chen, R.R. A CGE-based analysis on PM2.5-induced health-related economic effect in Beijing. China Environ. Sci. 2017, 37, 2779–2785. (In Chinese) [Google Scholar]
- Li, P.; Xin, J.; Wang, Y.; Wang, S.; Li, G.; Pan, X.; Liu, Z.; Wang, L. The acute effects of fine particles on respiratory mortality and morbidity in Beijing, 2004–2009. Environ. Sci. Pollut. Res. 2013, 20, 6433–6444. [Google Scholar] [CrossRef]
- Zhang, X.; Ou, X.; Yang, X.; Qi, T.; Nam, K.-M.; Zhang, D.; Zhang, X. Socioeconomic burden of air pollution in China: Province-level analysis based on energy economic model. Energy Econ. 2017, 68, 478–489. [Google Scholar] [CrossRef]
- Yang, Z.; Liu, P.; Xu, X. Estimation of social value of statistical life using willingness-to-pay method in Nanjing, China. Accid. Anal. Prev. 2016, 95, 308–316. [Google Scholar] [CrossRef]
- Hammitt, J.K. Valuing mortality risk: Theory and practice. Environ. Sci. Technol. 2000, 367, 50–57. [Google Scholar] [CrossRef] [Green Version]
- Puig-Junoy, J.; Zamora, A.R. Socio-economic costs of osteoarthritis: A systematic review of cost-of-illness studies. In Seminars in Arthritis and Rheumatism; WB Saunders: Philadelphia, PA, USA, 2015; Volume 44, pp. 531–541. [Google Scholar] [CrossRef]
- Aldy, J.E.; Viscusi, W.K. Adjusting the value of a statistical life for age and cohort effects. Rev. Econ. Stat. 1991, 90, 573–581. [Google Scholar] [CrossRef]
- Viscusi, W.K.; Magat, W.A.; Huber, J. Pricing environmental health risks: Survey assessments of risk-risk and risk-dollar trade-offs for chronic bronchitis. J. Environ. Econ. Manag. 2008, 21, 32–51. [Google Scholar] [CrossRef]
- Cheng, Z.; Jiang, J.; Fajardo, O.; Wang, S.X.; Hao, J.M. Characteristics and health impacts of particulate matter pollution in China (2001–2011). Atmos. Environ. 2013, 65, 186–194. [Google Scholar] [CrossRef]
- Fang, C.; Wang, Z.; Xu, G. Spatial-temporal characteristics of PM2.5 in China: A city-level perspective analysis. J. Geogr. Sci. 2016, 26, 1519–1532. [Google Scholar] [CrossRef]
- Wang, S.; Fang, C.; Guan, X.; Pang, B.; Ma, H. Urbanization, energy consumption, and carbon dioxide emissions in China: A panel data analysis of China’s provinces. Appl. Energy 2014, 136, 738–749. [Google Scholar] [CrossRef]
- Lin, B.; Zhu, J. Changes in urban air quality during urbanization in China. J. Clean. Prod. 2014, 188, 312–321. [Google Scholar] [CrossRef]
- Sadorsky, P. The effect of urbanization on CO2 emissions in emerging economies. Energy Econ. 2018, 41, 147–153. [Google Scholar] [CrossRef]
- Wang, D.W. Changes in the relationship between labor supply and labor demand and china’s economic growth in the low-fertility era. Chin. J. Pop. Sci. 2007, 1, 44–52. (In Chinese) [Google Scholar]
- Long, R.; Shao, T.; Chen, H. Spatial econometric analysis of China’s province-level industrial carbon productivity and its influencing factors. Appl. Energy 2016, 166, 210–219. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Health Risk | Health Outcomes | RR (10 μg/m3, 95% CI) | BIR Per 105 | Reference |
|---|---|---|---|---|
| Mortality | All-cause mortality | 1.019 (1.003, 1.081) | 711.0 | Wang et al. [47] |
| Hospitalization | Respiratory diseases | 1.022 (1.013, 1.032) | 550.9 | Li et al. [48] |
| Cardiovascular diseases | 1.013 (1.007, 1.019) | 546.0 | Maji et al. [12] | |
| Disease | Chronic bronchitis | 1.029 (1.014, 1.044) | 694.0 | Li et al. [48] |
| Acute bronchitis | 1.01 (1.005, 1.016) | 204.5 | Zhang et al. [49] | |
| Asthma | 1.021 (1.015, 1.028) | 940.0 | Maji et al. [12] |
| City | PM2.5 Concentration (μg/m3) | Urbanization Level (DN Value) | Health Outcomes Change (People) | Economic Loss (Billion Yuan) |
|---|---|---|---|---|
| Beijing | 65.221 | 9.062 | 95,816.420 | 84.904 |
| Shanghai | 51.235 | 14.615 | 88,523.473 | 79.595 |
| Tianjin | 72.756 | 5.1604 | 70,459.693 | 40.503 |
| Chongqing | 44.663 | 3.481 | 96,563.499 | 36.513 |
| Shijiazhuang | 77.086 | 1.137 | 58,607.663 | 30.034 |
| Weifang | 65.886 | 1.253 | 44,934.157 | 27.624 |
| Guangzhou | 34.442 | 6.673 | 32,836.113 | 25.585 |
| Wuhan | 64.222 | 3.696 | 46,945.370 | 25.189 |
| Chengdu | 51.681 | 4.076 | 51,813.849 | 25.142 |
| Hangzhou | 43.935 | 2.274 | 28,526.093 | 21.167 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Diao, B.; Ding, L.; Zhang, Q.; Na, J.; Cheng, J. Impact of Urbanization on PM2.5-Related Health and Economic Loss in China 338 Cities. Int. J. Environ. Res. Public Health 2020, 17, 990. https://doi.org/10.3390/ijerph17030990
Diao B, Ding L, Zhang Q, Na J, Cheng J. Impact of Urbanization on PM2.5-Related Health and Economic Loss in China 338 Cities. International Journal of Environmental Research and Public Health. 2020; 17(3):990. https://doi.org/10.3390/ijerph17030990
Chicago/Turabian StyleDiao, Beidi, Lei Ding, Qiong Zhang, Junli Na, and Jinhua Cheng. 2020. "Impact of Urbanization on PM2.5-Related Health and Economic Loss in China 338 Cities" International Journal of Environmental Research and Public Health 17, no. 3: 990. https://doi.org/10.3390/ijerph17030990