Anthropometrical Features of Para-Footballers According to Their Cerebral Palsy Profiles and Compared to Controls

 ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Anthropometric Determinations
2.3. Body Composition
- Three skinfolds∑3Sk = Ch + A + Th
- Six skinfolds∑6Sk = Tr + Sb + Sp + A + Th + Ca
- Upper body skinfolds∑UpSk = Tr + Sb
- Lower body skinfolds∑LowSk = Th + Ca
2.4. Body Proportionality
2.5. Statistical Analyses
3. Results
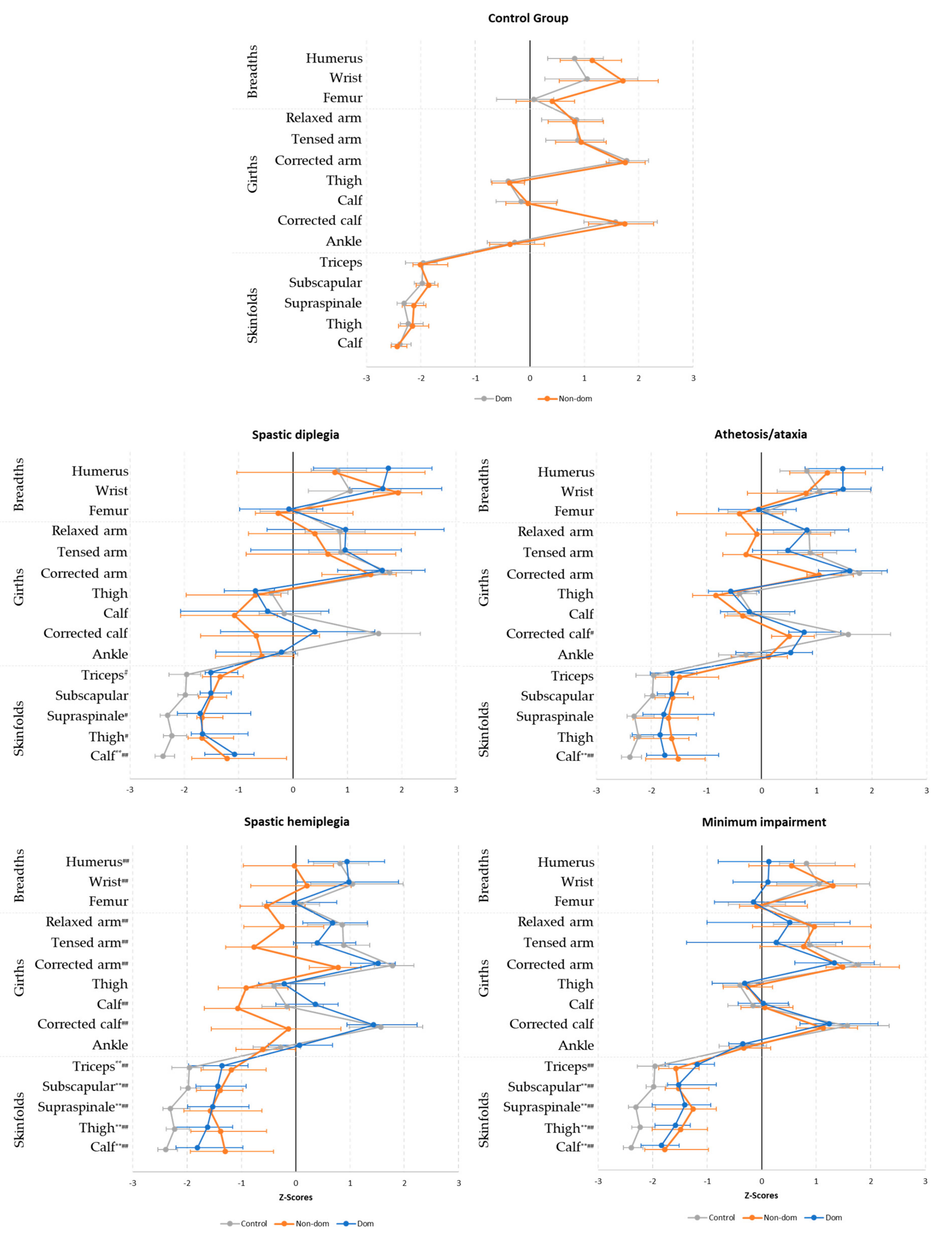
3.1. Dominant vs. Nondominant Sides
3.2. Comparison with the Control Group
3.3. Equation Comparison
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Gil, S.M.; Gil, J.; Ruiz, F.; Irazusta, A.; Irazusta, J. Physiological and anthropometric characteristics of young soccer players according to their playing position: Relevance for the selection process. J. Strength Cond. Res. 2007, 21, 438–445. [Google Scholar] [CrossRef]
- Rodríguez, F.J.R.; Flores, A.A.A.; Farias, T.Y.; Gutierrez, O.B.; Arce, P.L. Body composition and referential somatotype of physically active subjects. Int. J. Morphol. 2010, 28, 1159–1165. [Google Scholar] [CrossRef] [Green Version]
- Munguía-Izquierdo, D.; Suárez-Arrones, L.; Di Salvo, V.; Paredes-Hernández, V.; Ara, I.; Mendez-Villanueva, A. Estimating fat-free mass in elite youth male soccer players: Cross-validation of different field methods and development of prediction equation. J. Sports Sci. 2019, 37, 1197–1204. [Google Scholar] [CrossRef]
- Deprez, D.; Valente-Dos-Santos, J.; Coelho-E-Silva, M.J.; Lenoir, M.; Philippaerts, R.; Vaeyens, R. Longitudinal development of explosive leg power from childhood to adulthood in soccer players. Int. J. Sports Med. 2015, 36, 672–679. [Google Scholar] [CrossRef]
- Kemper, G.L.J.; Van Der Sluis, A.; Brink, M.S.; Visscher, C.; Frencken, W.G.P.; Elferink-Gemser, M.T. Anthropometric injury risk factors in elite-standard youth soccer. Int. J. Sports Med. 2015, 36, 1112–1117. [Google Scholar] [CrossRef]
- Nikolaidis, P.T. Association between body mass index, body fat per cent and muscle power output in soccer players. Cent. Eur. J. Med. 2012, 7, 783–789. [Google Scholar] [CrossRef]
- Slimani, M.; Nikolaidis, P.T. Anthropometric and physiological characteristics of male soccer players according to their competitive level, playing position and age group: A systematic review. J. Sports Med. Phys. Fit. 2019, 59, 141–163. [Google Scholar] [CrossRef]
- Torres-Luque, G.; Calahorro-Cañada, F.; Lara-Sánchez, A.J.; Garatachea, N.; Nikolaidis, P.T. Body composition using bioelectrical impedance analysis in elite young soccer players: The effects of age and playing position. Sport Sci. Health 2015, 11, 203–210. [Google Scholar] [CrossRef]
- Dingley, A.A.; Pyne, D.B.; Burkett, B. Relationships between propulsion and anthropometry in paralympic swimmers. Int. J. Sports Physiol. Perform. 2015, 10, 978–985. [Google Scholar] [CrossRef]
- Medeiros, R.M.V.; Alves, E.S.; Lemos, V.A.; Schwingel, P.A.; da Silva, A.; Vital, R.; Vieira, A.S.; Barreto, M.M.; Rocha, E.A.; Tufik, S.; et al. Assessment of body composition and sport performance of brazilian paralympic swim team athletes. J. Sport Rehabil. 2016, 25, 364–370. [Google Scholar] [CrossRef]
- Lemos, V.D.A.; Alves, E.D.S.; Schwingel, P.A.; Rosa, J.P.P.; Da Silva, A.; Winckler, C.; Vital, R.; De Almeida, A.A.; Tufik, S.; De Mello, M.T. Analysis of the body composition of Paralympic athletes: Comparison of two methods. Eur. J. Sport Sci. 2016, 16, 955–964. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, G.L.; Oliveira, T.A.P.; Penello, F.M.; Fernandes Filho, J. Anthropometric characteristics and aerobic fitness of blind athletes of 5-a-side football. Rev. Peru. Cienc. Act. Física Deporte 2020, 7, 10. [Google Scholar]
- Runciman, P.; Tucker, R.; Ferreira, S.; Albertus-Kajee, Y.; Micklesfield, L.; Derman, W. Site-specific bone mineral density is unaltered despite differences in fat-free soft tissue mass between affected and nonaffected sides in hemiplegic paralympic athletes with cerebral palsy: Preliminary findings. Am. J. Phys. Med. Rehabil. 2016, 95, 771–778. [Google Scholar] [CrossRef] [PubMed]
- Juzwiak, C.R.; Winckler, C.; Joaquim, D.P.; Silva, A.; De Mello, M.T. Comparison of measured and predictive values of basal metabolic rate in brazilian paralympic track and field athletes. Int. J. Sport Nutr. Exerc. Metab. 2016, 26, 330–337. [Google Scholar] [CrossRef] [PubMed]
- Flueck, J.L. Body composition in Swiss elite wheelchair athletes. Front. Nutr. 2020, 7. [Google Scholar] [CrossRef]
- Keil, M.; Totosy de Zepetnek, J.O.; Brooke-Wavell, K.; Goosey-Tolfrey, V.L. Measurement precision of body composition variables in elite wheelchair athletes, using dual-energy X-ray absorptiometry. Eur. J. Sport Sci. 2016, 16, 65–71. [Google Scholar] [CrossRef]
- Willems, A.; Thomas, T.A.; Keil, M.; Brooke-Wavell, K.; Goosey-Tolfrey, V.L. Dual-energy X-ray absorptiometry, skinfold thickness, and waist circumference for assessing body composition in ambulant and non-ambulant wheelchair games players. Front. Physiol. 2015, 6. [Google Scholar] [CrossRef] [Green Version]
- Porto, Y.C.; Almeida, M.; De Sá, C.C.; Schwingel, P.A.; Zoppi, C.C. Anthropometric and physical characteristics of motor disabilited paralympic rowers. Res. Sports Med. 2008, 16, 203–212. [Google Scholar] [CrossRef]
- Reina, R.; Sarabia, J.M.; Caballero, C.; Yanci, J. How does the ball influence the performance of change of direction and sprint tests in para-footballers with brain impairments? Implications for evidence-based classification in CP-Football. PLoS ONE 2017, 12, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Reina, R.; Iturricastillo, A.; Sabido, R.; Campayo-Piernas, M.; Yanci, J. Vertical and horizontal jump capacity in international cerebral palsy football players. Int. J. Sports Physiol. Perform. 2018, 13, 597–603. [Google Scholar] [CrossRef]
- Gorla, J.; Nogueira, C.D.; Gonçalves, H.R.; De Faria, F.R.; Buratti, J.R.; Nunes, N.; do Rêgo, J.T.P.; Borges, M.; Vieira, I.B.; Roca, V.L. Composición corporal y perfil somatotípico de jugadores brasileños de fútbol siete con Parálisis Cerebral de acuerdo con la clasificación funcional. Contribución al deporte paralímpico. Retos Nuevas Tendencias en Educación física Deporte y Recreación 2019, 35, 326–328. [Google Scholar]
- Yanci, J.; Los Arcos, A.; Grande, I.; Santalla, A.; Figueroa, J.; Gil, E.; Cámara, J. Jump capacity in cerebral palsy soccer players. Int. J. Med. Sci. Phys. Act. Sport 2014, 14, 199–211. [Google Scholar]
- Durstine, J.L.; Moore, G.E.; Painter, P.L.; Roberts, S.O. ACSM’s Exercise Management for Persons with Chronic Diseases and Disabilities, 3rd ed.; ACSM: Champaign, IL, USA, 2009. [Google Scholar]
- Reina, R.; Elvira, J.; Valverde, M.; Roldán, A.; Yanci, J. Kinematic and kinetic analyses of the vertical jump with and without header as performed by para-footballers with cerebral palsy. Sports 2019, 7, 209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oftedal, S.; Davies, P.S.W.; Boyd, R.N.; Stevenson, R.D.; Ware, R.S.; Keawutan, P.; Benfer, K.A.; Bell, K.L. Body composition, diet, and physical activity: A longitudinal cohort study in preschoolers with cerebral palsy. Am. J. Clin. Nutr. 2017, 105, 369–378. [Google Scholar] [CrossRef] [PubMed]
- Hildreth, H.G.; Johnson, R.K.; Goran, M.I.; Contompasis, S.H. Body composition in adults with cerebral palsy by dual-energy X-ray absorptiometry, bioelectrical impedance analysis, and skinfold anthropometry compared with the 18O isotope-dilution technique. Am. J. Clin. Nutr. 1997, 66, 1436–1442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Snik, D.A.C.; de Roos, N.M. Criterion validity of assessment methods to estimate body composition in children with cerebral palsy: A systematic review. Ann. Phys. Rehabil. Med. 2020. [Google Scholar] [CrossRef]
- Iversen, E.; Hassager, C.; Christiansen, C. The effect of hemiplegia on bone mass and soft tissue body composition. Acta Neurol. Scand. 1989, 79, 155–159. [Google Scholar] [CrossRef]
- De Brito, C.M.M.; Garcia, A.C.F.; Takayama, L.; Fregni, F.; Battistella, L.R.; Pereira, R.M.R. Bone loss in chronic hemiplegia: A longitudinal cohort study. J. Clin. Densitom. 2013, 16, 160–167. [Google Scholar] [CrossRef]
- Hafer-Macko, C.E.; Ryan, A.S.; Ivey, F.M.; Macko, R.F. Skeletal muscle changes after hemiparetic stroke and potential beneficial effects of exercise intervention strategies. J. Rehabil. Res. Dev. 2008, 45, 261–272. [Google Scholar] [CrossRef]
- Marfell-Jones, M.J.; Stewart, A.; De Ridder, J. International Standards for Anthropometric Assessment; International Society for the Advancement of Kinanthropometry: Potchefstroom, South Africa, 2012. [Google Scholar]
- Heyward, V.H.; Wagner, D.R. Applied Body Composition Assessment; Human Kinetics: Champaign, IL, USA, 2004; ISBN 0736046305. [Google Scholar]
- Alvero Cruz, J.R.; Cabañas Armesilla, M.D.; Herrero de Lucas, A.; Martinez Riaza, L.; Moreno Pascual, C.; Porta Manzañino, J.; Sillero Quintana, M.; Sirvent Belando, J.E. Protocolo de valoración de la composición corporal para el reconocimiento médico-deportivo. Documento de consenso del grupo español de cineantropometría de la federación española de medicina del deporte. Rev. Arch. Med. Deporte 2009, 16, 166–179. [Google Scholar]
- Faulkner, J.A. Physiology of swimming. Res. Q. Am. Assoc. Heal. Phys. Educ. Recreat. 1966, 37, 41–54. [Google Scholar] [CrossRef]
- Carter, J.L. Body composition of Montreal olympic athletes. In Physical Structure of Olympic Athletes; Carter, J.E.L., Ed.; Basel Karger Publishers: Basel, Switzerland, 1982; pp. 107–116. [Google Scholar]
- Withers, R.T.; Craig, N.P.; Bourdon, P.C.; Norton, K.I. Relative body fat and anthropometric prediction of body density of male athletes. Eur. J. Appl. Physiol. Occup. Physiol. 1987, 56, 191–200. [Google Scholar] [CrossRef] [PubMed]
- Siri, W.E. Body composition from fluid spaces and density: Analysis of methods. Tech. Meas. Body Compos. 1961, 61, 223–244. [Google Scholar]
- Martin, A. Anthropometric assessment of bone mineral. In Anthropometric Assessment of Nutritional Status; Himes, J., Ed.; Wiley-Liss: New York, NY, USA, 1991; pp. 185–196. [Google Scholar]
- Valensise, H.; Andreoli, A.; Lello, S.; Magnani, F.; Romanini, C.; De Lorenzo, A. Total-body skeletal muscle mass: Development and cross-validation of anthropometric prediction models. Am. J. Clin. Nutr. 2000, 72, 796–803. [Google Scholar] [CrossRef]
- Garrido-Chamorro, R.; Sirvent-Belando, J.E.; González-Lorenzo, M.; Blasco-Lafarga, C.; Roche, E. Sumatorio de Pliegues Subcutáneos: Valores de Referencia para Atletas de Élite. Int. J. Morphol. 2012, 30, 803–809. [Google Scholar] [CrossRef] [Green Version]
- Ross, W.D.; Wilson, N.C. A stratagem for proportional growth assessment. Acta Paediatr. Belg. 1974, 28, 169–182. [Google Scholar]
- Bacciotti, S.; Baxter-Jones, A.; Gaya, A.; Maia, J. Body physique and proportionality of Brazilian female artistic gymnasts. J. Sports Sci. 2018. [Google Scholar] [CrossRef]
- Alacid, F.; Marfell-Jones, M.; Muyor, J.M.; López-Miñarro, P.A.; Martínez, I. Kinanthropometric comparison between young elite kayakers and canoeists. Coll. Antropol. 2015, 39, 119–124. [Google Scholar]
- Ross, W.D. Kinanthropometry. In Physiological Testing of the High-Performance Athlete; Human Kinetics: Champaign, IL, USA, 1991. [Google Scholar]
- Tomczak, M.; Tomczak, E. The need to report effect size estimates revisited. An overview of some recommended measures of effect size. Trends Sport Sci. 2014, 1, 19–25. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: Abingdon, UK, 2013. [Google Scholar]
- Portal, S.; Rabinowitz, J.; Adler-Portal, D.; Burstein, R.P.; Lahav, Y.; Meckel, Y.; Nemet, D.; Eliakim, A. Body fat measurements in elite adolescent volleyball players: Correlation between skinfold thickness, bioelectrical impedance analysis, air-displacement plethysmography, and body mass index percentiles. J. Pediatr. Endocrinol. Metab. 2010, 23, 395–400. [Google Scholar] [CrossRef]
- Ferrang, T.M.; Johnson, R.K.; Ferrara, M.S. Dietary and anthropometric assessment of adults with cerebral palsy. J. Am. Diet. Assoc. 1992, 92, 1083–1086. [Google Scholar] [PubMed]
- Oliveira, C.; Ferreira, D.; Caetano, C.; Granja, D.; Pinto, R.; Mendes, B.; Sousa, M. Nutrition and supplementation in soccer. Sports 2017, 5, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ackland, T.R.; Ong, K.B.; Kerr, D.A.; Ridge, B. Morphological characteristics of Olympic sprint canoe and kayak paddlers. J. Sci. Med. Sport 2003. [Google Scholar] [CrossRef]
- Sanchis-Moysi, J.; Calbet, J.A.L. Ghost or real musculoskeletal asymmetries in football players? Med. Sci. Sports Exerc. 2016, 48. [Google Scholar] [CrossRef] [PubMed]
- Oberhofer, K.; Stott, N.S.; Mithraratne, K.; Anderson, I.A. Subject-specific modelling of lower limb muscles in children with cerebral palsy. Clin. Biomech. 2010, 25, 88–94. [Google Scholar] [CrossRef]
- Monbaliu, E.; De Cock, P.; Mailleux, L.; Dan, B.; Feys, H. The relationship of dystonia and choreoathetosis with activity, participation and quality of life in children and youth with dyskinetic cerebral palsy. Eur. J. Paediatr. Neurol. 2017, 21, 327–335. [Google Scholar] [CrossRef]
- Chad, K.E.; McKay, H.A.; Zello, G.A.; Bailey, D.A.; Faulkner, R.A.; Snyder, R.E. Body composition in nutritionally adequate ambulatory and non-ambulatory children with cerebral palsy and a healthy reference group. Dev. Med. Child Neurol. 2000. [Google Scholar] [CrossRef]
- Verschuren, O.; Peterson, M.D.; Balemans, A.C.J.; Hurvitz, E.A. Exercise and physical activity recommendations for people with cerebral palsy. Dev. Med. Child Neurol. 2016, 58, 798–808. [Google Scholar] [CrossRef]
- Reina, R.; Sarabia, J.M.; Yanci, J.; García-Vaquero, M.P.; Campayo-Piernas, M. Change of direction ability performance in cerebral palsy football players according to functional profiles. Front. Physiol. 2016, 6, 409. [Google Scholar] [CrossRef] [Green Version]
- Cans, C. Surveillance of cerebral palsy in Europe: A collaboration of cerebral palsy surveys and registers. Dev. Med. Child Neurol. 2000, 42, 816–824. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Total Sample | Spastic Diplegia | Athetosis/Ataxia | Spastic Hemiplegia | Minimum Impairment | Control Group |
|---|---|---|---|---|---|---|
| n | 141 | 8 | 14 | 64 | 16 | 39 |
| Laterality (R/L) | 77/64 | 3/5 | 8/6 | 24/40 | 9/7 | 33/6 |
| Ethnicity (CA/AF) | 135/6 | 8/0 | 13/1 | 62/2 | 16/0 | 36/3 |
| Training experience (year) | 11 (6, 16) | 12 (5, 15) | 10 (10, 12) | 10 (5, 14) | 17 (5, 22) | 15 (15, 16) |
| Age (year) | 23 (20, 29) | 23.5 (18, 33.3) | 24.5 (19.8, 34) | 23 (21, 30) | 26.5 (21.3, 38.3) | 22 (20, 23) |
| Weight (kg) | 70.9 (64, 76.7) | 63.4 (60.1, 73.3) † | 68.1 (62.2, 73) | 67.3 (62.4, 75) †† | 73.6 (69.4, 78.7) † | 74.5 (69.3, 80) |
| Height (cm) | 176 (172, 181) | 171.5 (168.3, 178.8) | 173 (170.8, 179.3) † | 174 (172, 178.9) †† | 179 (170.4, 183.8) | 181 (176, 184) |
| BMI (kg·m−2) | 22.6 (21.5, 23.9) | 21.9 (19.7, 24.4) | 22.5 (20.4, 23.9) | 22.1 (21, 23.7) | 23.4 (21.6, 25.6) | 23.2 (22.1, 24) |
| Spastic Diplegia (n = 8) | Athetosis/Ataxia (n = 14) | Spastic Hemiplegia (n = 64) | Minimum Impairment (n = 16) | Control Group (n = 39) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Dom | Non-Dom | Dom | Non-Dom | Dom | Non-Dom | Dom | Non-Dom | Dom | Non-Dom | |
| Breadths (cm) | ||||||||||
| Humerus | 7.2 (6.8, 7.4) * | 7 (6.4, 7.3) | 7 (6.8, 7.5) | 7.1 (6.8, 7.3) | 7 (6.6, 7.3) ** | 6.6 (6.4, 6.9) | 7 (6.6, 7.5) | 6.9 (6.4, 7.2) | 7.2 (7, 7.5) * | 7.2 (6.9, 7.4) |
| Wrist | 5.9 (5.6, 6.1) | 5.9 (5.7, 6) | 5.7 (5.5, 6.1) ** | 5.5 (5.2, 5.7) | 5.6 (5.4, 5.9) ** | 5.4 (5.1, 5.6) | 5.9 (5.5, 6) | 5.6 (5.4, 5.8) | 6 (5.8, 6.2) | 5.9 (5.5, 6.1) |
| Femur | 9.5 (9.3, 10) | 9.7 (9.6, 10) | 9.7 (9.4, 10) | 9.7 (9.2, 9.8) | 9.8 (9.5, 10.1) ** | 9.5 (9.3, 9.8) | 10 (9.7, 10.3) ** | 9.9 (9.5, 10.1) | 10.2 (10, 10.5) ** | 10.1 (9.7, 10.4) |
| Ankle | 7.5 (7.3, 7.8) | 7.4 (7.1, 7.5) | 7.5 (7.3, 7.7) | 7.5 (7.2, 7.8) | 7.4 (7.2, 7.8) ** | 7.2 (7, 7.5) | 7.4 (7.2, 7.8) | 7.4 (7.1, 7.7) | 7.6 (7.2, 8) | 7.6 (7.2, 8) |
| Girths (cm) | ||||||||||
| Relaxed arm | 29.2 (26.3, 33.3) | 27.8 (26.1, 32) | 29.3 (27.6, 30.9) ** | 27.7 (26.3, 29.1) | 29.6 (27.3, 30.6) ** | 26.9 (25.3, 28.6) | 30 (28.1, 32.6) | 29 (25.7, 32.9) | 30.2 (29.3, 31.7) | 30.2 (28.9, 32.1) |
| Flexed arm | 32.4 (28.7, 33.8) | 30.7 (28.7, 33.8) | 30.6 (30.3, 33.7) * | 29.5 (28.8, 31.7) | 31.2 (29.8, 32.6) ** | 28.7 (27.4, 30.1) | 33.3 (30.7, 34.7) | 31.8 (27.8, 35) | 33.3 (32.3, 34.8) | 33.2 (31.3, 34.6) |
| Neck | 370.0 (360.0, 37.9) | 36.8 (35.4, 37.8) | 36.5 (35.2, 37.7) | 36.4 (35.9, 38.4) | 37.2 (35.6, 38.3) | |||||
| Thigh | 49.9 (49.6, 53.9) | 50.2 (45.4, 52.6) | 51.7 (49.8, 54.1) * | 50.7 (48.3, 53.5) | 53.7 (51.3, 56.3) ** | 50.6 (47.9, 53.7) | 54.9 (52.7, 55.8) | 54.2 (52.7, 55.2) | 54.4 (53.3, 55.7) | 54.2 (51.6, 56.2) |
| Calf | 34.5 (31.5, 37.3) | 32.5 (31.3, 35.7) | 35.6 (35, 36.9) * | 35.1 (34.2, 36) | 36.8 (35, 38.2) ** | 34.2 (32.1, 35.7) | 37.1 (36.1, 37.9) | 37 (35.7, 38.6) | 37.3 (35.9, 38.7) | 37.3 (35.7, 38.8) |
| Ankle | 21.4 (20.3, 22.7) | 21 (20.6, 22.4) | 22.7 (21.8, 23.2) * | 22.2 (21.4, 22.6) | 22.3 (21.4, 23.4) ** | 21.5 (20.7, 22.3) | 22.3 (21.6, 23.2) | 22.6 (21.3, 23) | 22.7 (21.9, 23.1) | 22.5 (21.9, 23.4) |
| Corrected arm | 26.1 (23.5, 29.4) | 25.1 (22.6, 27.2) | 26.3 (24.9, 28) * | 24.5 (23.9, 25.5) | 26 (24.8, 27.7) ** | 23.5 (21.9, 24.9) | 26.7 (25.5, 29.9) | 26.2 (22.6, 29.8) | 28 (26.5, 29.1) | 28.2 (26.5, 29.9) |
| Corrected thigh | 45.9 (42.6, 48.7) | 44.3 (41, 47.3) | 48 (46.4, 50) | 47.2 (44.5, 48.9) | 49.1 (47.1, 51.4) ** | 44.8 (43.1, 47.7) | 50.2 (47.2, 51.1) | 49.7 (47.6, 52.1) | 51.5 (49.3, 52.4) | 50.8 (49, 52.9) |
| Corrected calf | 31.1 (28.2, 34.2) | 28.7 (27.2, 31.9) | 32.7 (31.7, 33.9) | 31.9 (31.5, 33.4) | 34 (32.6, 35.5) ** | 30.6 (28.1, 33.2) | 34.8 (32.3, 35.4) | 34.2 (33.1, 36.7) | 35.8 (34.4, 36.9) * | 35.3 (33.7, 37.1) |
| Skinfolds (mm) | ||||||||||
| Triceps | 8.8 (8.3, 10.8) | 9.4 (8.1, 11.9) | 8.5 (6.5, 10.1) | 9.4 (7.1, 12.1) | 9.3 (6.7, 11.9) ** | 10.4 (7.6, 13.6) | 8.9 (7.2, 11.1) | 9.9 (8.1, 12) | 6.9 (6.3, 8.7) | 7 (5.3, 8.4) |
| Subscapular | 9.6 (8.9, 11.5) | 9.9 (8.3, 11.1) | 8.9 (7.8, 10.6) | 9.2 (7.6, 11.3) | 10 (8.2, 12.8) | 10.2 (8.2, 12.5) | 9.8 (8.7, 12.5) | 10.2 (8.9, 13.3) | 8.5 (7.1, 9.2) | 7.6 (6.9, 8.6) |
| Chest | 6.5 (5.6, 9.2) | 7 (6.5, 7.5) | 6.7 (5.8, 11.2) | 7.2 (4.5, 10.9) | 7.9 (5.7, 11.7) | 8.1 (5.1, 11.8) | 8.3 (6, 12) | 8.4 (5.6, 11.3) | 4.2 (2.9, 4.9) | 4.1 (3.1, 4.6) |
| Supraspinale | 7.7 (6.1, 120.0) | 8.1 (7.6, 9.8) | 7.7 (6.1, 11.3) | 7.9 (5, 10.4) | 8.6 (6.6, 11.7) | 8.6 (6.7, 13.2) | 9.9 (7.2, 12.4) | 9.7 (6.5, 11.8) | 6.3 (5.1, 7.4) * | 5.6 (4.8, 7.1) |
| Abdominal | 17.8 (11.5, 20.8) | 15.4 (9, 25.2) | 18 (10.2, 26.2) | 19.3 (12.6, 29.7) | 9.2 (7.4, 10.3) | |||||
| Thigh | 13.4 (11.4, 200.0) | 13.1 (11, 18.9) | 11.9 (7.6, 17.3) | 13.9 (8.1, 16.1) | 13.7 (8.5, 17.7) ** | 15.8 (11.1, 22.4) | 15 (10.5, 19.8) | 14.7 (11.1, 16.6) | 9.3 (7.6, 12) | 9 (7.6, 11.1) |
| Calf | 11.2 (8.5, 12.6) | 10.5 (7.5, 15.5) | 7.9 (6.6, 12.6) | 9.2 (6.2, 11.4) | 7.7 (5.9, 12) ** | 10.1 (7.1, 14.2) | 7.7 (6.1, 12) | 7.7 (6, 9.5) | 4.9 (4.2, 5.9) | 5.3 (4.3, 6.4) |
| Spastic Diplegia (n = 8) | Athetosis/Ataxia (n = 14) | Spastic Hemiplegia (n = 64) | Minimum Impairment (n = 16) | Control Group (n = 39) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Dom | Non-Dom | Dom | Non-Dom | Dom | Non-Dom | Dom | Non-Dom | Dom | Non-Dom | |
| Fat mass (%) | ||||||||||
| Carter’s equation | 9.6 (9, 11.6) | 9.6 (9.3, 10.1) | 9 (7.7, 11.3) | 9.2 (7.6, 12.5) | 9.7 (7.7, 120.0) ** | 10.5 (8.2, 13.1) | 10.8 (8.9, 12.2) | 10.4 (8.6, 11.9) | 7.5 (6.6, 8.2) | 7.1 (6.6, 8.1) |
| Faulkner’s equation | 12.7 (11.1, 13.8) | 12.4 (11.7, 13.2) | 12.1 (10.7, 14.5) | 12.5 (10.2, 14.7) | 13.1 (10.9, 15.2) ** | 13.4 (10.9, 15.5) | 13.6 (11.7, 15.2) | 13.3 (11.8, 15.8) | 10.6 (9.9, 11.2) * | 10.3 (9.6, 11.2) |
| Withers’ equation | 10 (9, 14) | 10.2 (9.6, 12.2) | 10 (8.1, 12.5) | 9.8 (7.9, 13.8) | 10.8 (8.3, 140.0) ** | 11.7 (8.7, 15.1) | 11.9 (9.2, 16.1) | 10.7 (9.2, 14.6) | 6.7 (6.1, 7.6) | 6.7 (6.1, 7.5) |
| ∑3 Sk | 36.1 (32.1, 51.2) | 37.6 (34.6, 38.5) | 37.4 (27.4, 50.2) | 36.4 (23.1, 52.2) | 38.9 (27.5, 54.4) ** | 41.1 (28.2, 57.9) | 43.7 (33.8, 61.3) | 41.1 (32.7, 56.5) | 23 (18.9, 26.7) | 22 (18.7, 26.1) |
| ∑6 Sk | 67.1 (60.7, 85.6) | 66.4 (63.9, 71.4) | 61.2 (49.1, 82.6) | 63.3 (47.6, 94) | 67.7 (48.8, 89.3) ** | 75.3 (53.6, 100.2) | 78.4 (60.3, 91.6) | 74.2 (57.6, 88.3) | 46.5 (38.2, 53.1) | 42.8 (38.5, 52.9) |
| ∑Upper body Sk | 18.7 (16.9, 20.9) | 19 (18.2, 19.8) | 17.4 (14, 19.9) | 18.8 (14.8, 22.6) | 19.6 (15.3, 25.7) ** | 21 (17.1, 25.8) | 18.7 (17.6, 22.6) | 21 (18.3, 24.1) | 15.2 (13.9, 17.5) * | 14.9 (12.6, 16.6) |
| ∑Lower body Sk | 24.1 (19.6, 33.8) | 24.7 (19.9, 30) | 19.8 (14.8, 32.7) | 23.7 (15.7, 28.2) | 22.1 (14.5, 31.2) ** | 25.7 (18.2, 36.3) | 25.5 (16.5, 32) | 23 (16.8, 25.1) | 14.2 (12.2, 18.4) | 14 (12.4, 16.2) |
| Muscle mass (%) | ||||||||||
| Lee’s equation | 43.7 (42.2, 45.4) | 41.3 (39.5, 43.6) | 43.8 (41.9, 46.8) * | 41.5 (38.9, 45.8) | 44.8 (42.8, 47.9) ** | 39 (36, 42.3) | 42.9 (41, 43.9) | 41.8 (40.1, 43.3) | 45.8 (44.4, 47.2) | 45.5 (44.1, 47.2) |
| Bone mass (%) | ||||||||||
| Rocha’s equation | 17.3 (16.7, 19.8) | 17.6 (16.5, 19.7) | 17.6 (16, 18.2) * | 16.5 (15.3, 17.8) | 17.5 (16, 18.6) ** | 16.3 (15.4, 17.4) | 17.1 (16.1, 18.1) * | 16.5 (15.2, 17.4) | 17.6 (16.9, 18.4) * | 17.1 (16.3, 17.9) |
| Martin’s equation | 14.4 (13.6, 15.4) | 13.7 (12.8, 14.7) | 13.6 (13.3, 14.6) * | 13.5 (13.1, 14.1) | 13.9 (12.6, 15) ** | 12.7 (12, 13.5) | 13.7 (12.4, 14.3) ** | 12.3 (11.8, 13.5) | 13.8 (13.3, 14.4) * | 13.6 (12.8, 14) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sarabia, J.M.; Doménech, C.; Roche, E.; Vicente-Salar, N.; Reina, R. Anthropometrical Features of Para-Footballers According to Their Cerebral Palsy Profiles and Compared to Controls. Int. J. Environ. Res. Public Health 2020, 17, 9071. https://doi.org/10.3390/ijerph17239071
Sarabia JM, Doménech C, Roche E, Vicente-Salar N, Reina R. Anthropometrical Features of Para-Footballers According to Their Cerebral Palsy Profiles and Compared to Controls. International Journal of Environmental Research and Public Health. 2020; 17(23):9071. https://doi.org/10.3390/ijerph17239071
Chicago/Turabian StyleSarabia, José M., Carmen Doménech, Enrique Roche, Néstor Vicente-Salar, and Raul Reina. 2020. "Anthropometrical Features of Para-Footballers According to Their Cerebral Palsy Profiles and Compared to Controls" International Journal of Environmental Research and Public Health 17, no. 23: 9071. https://doi.org/10.3390/ijerph17239071