The Impact of Childhood and Adult Educational Attainment and Economic Status on Later Depressive Symptoms and Its Intergenerational Effect

Abstract
:1. Introduction
1.1. Life-Course Perspective
1.2. The Effects of Childhood SES on Depressive Symptoms Later
1.3. Intergenerational Transmission of Adverse SES and Depressive Symptoms
1.4. Purpose
2. Method
2.1. Data and Sample
2.2. Measures
2.3. Analysis
3. Results
3.1. Descriptive Results and Bivariate Tests
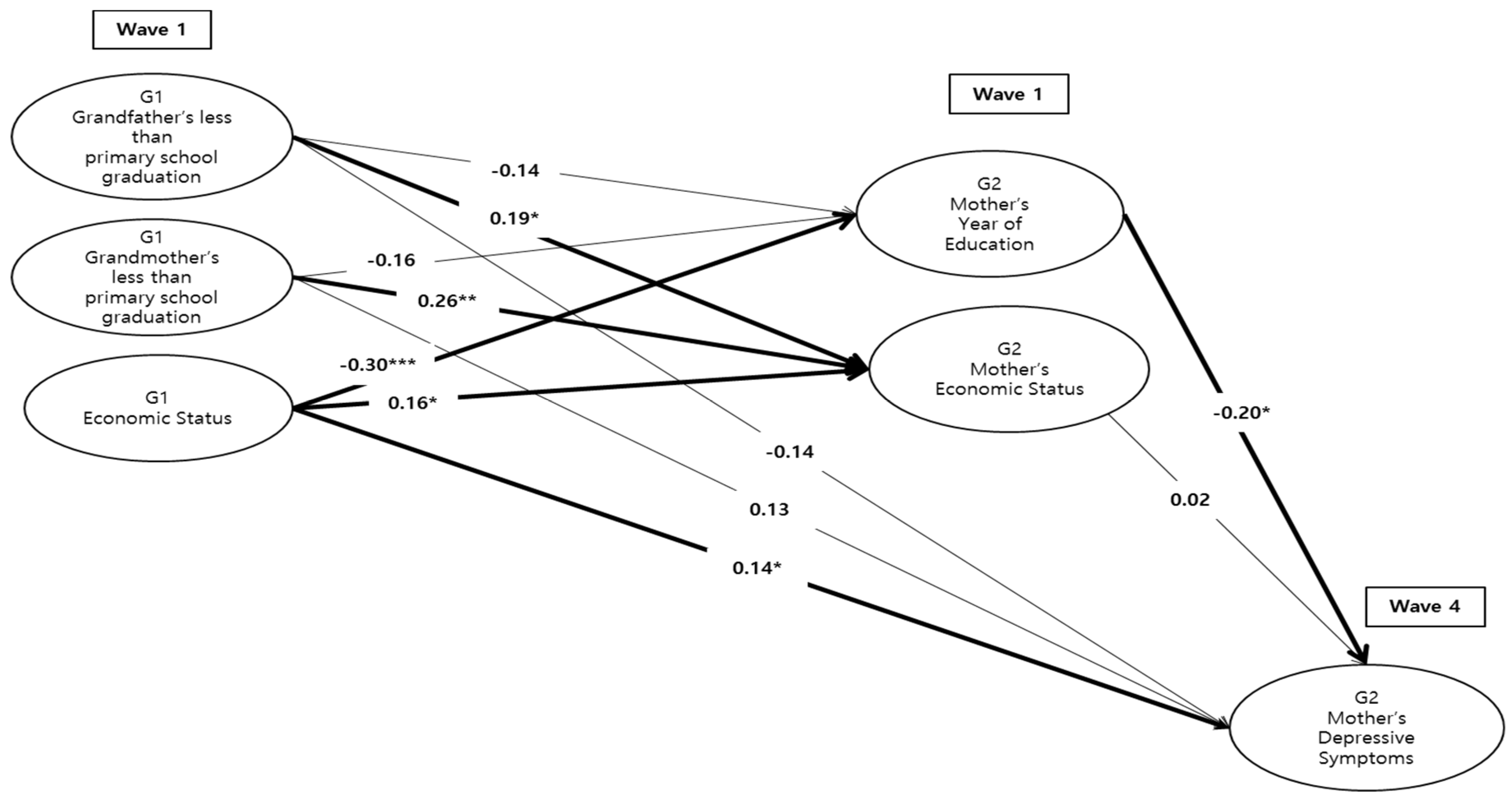
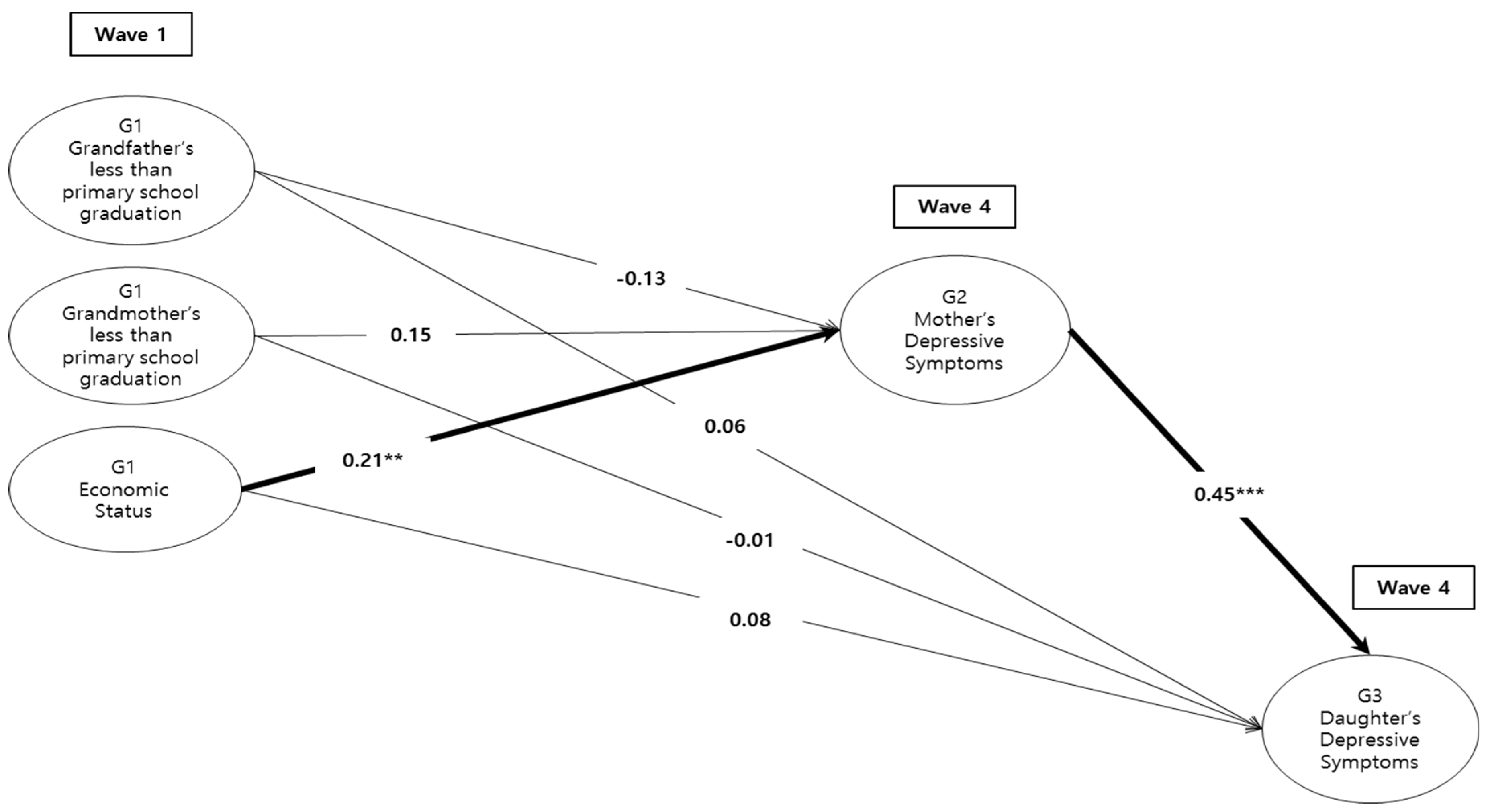
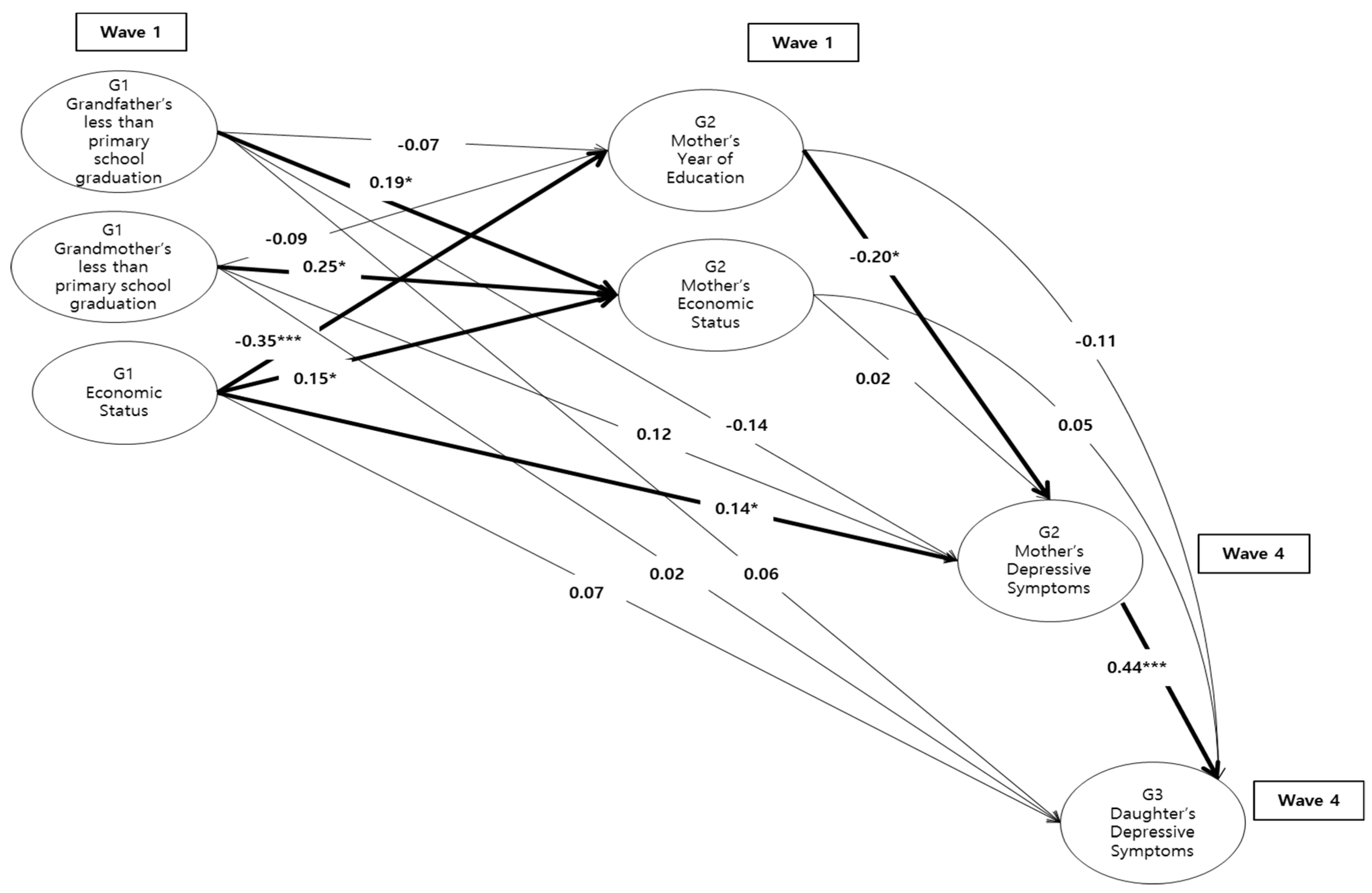
3.2. Testing the Mediating Effects
4. Discussion
5. Conclusions
Funding
Acknowledgments
Conflicts of Interest
References
- An, J.; Kim, H. A study on the determinants of children and adolescents’ health inequality in Korea. Stud. Korean Youth 2013, 24, 205–231. [Google Scholar]
- Kim, J. The relationship between socioeconomic status and health in Korea—Focusing on age variations. Korean J. Sociol. 2007, 41, 127–153. [Google Scholar]
- Lorant, V.; Deliege, D.; Eaton, W.; Robert, A.; Philipport, A.; Ansseau, M. Socioeconomic inequalities in depression: A meta-analysis. Am. J. Epidemiol. 2003, 157, 98–112. [Google Scholar] [CrossRef] [Green Version]
- Nishimura, J. Socioeconomic status and depression across Japan, Korea, and China: Exploring the impact of labor market structures. Soc. Sci. Med. 2011, 73, 604–614. [Google Scholar] [CrossRef]
- Schafer, M.H.; Ferraro, K.F. Childhood misfortune as a threat to successful aging avoiding disease. Gerontologist 2012, 52, 111–120. [Google Scholar] [CrossRef]
- Turner, R.J.; Lloyd, D.A. The stress process and the social distribution of depression. J. Health Soc. Behav. 1999, 40, 374–404. [Google Scholar] [CrossRef]
- Kang, S.K.; Kwon, T.Y. An exploratory study on the effects of socioeconomic status on depressive symptoms across lifespan. Ment. Health Soc. Work 2008, 30, 332–335. [Google Scholar]
- Luo, Y.; Waite, L.J. The impact of childhood and adult SES on physical, mental, cognitive well-being in later life. J. Gerontol. Soc. Sci. 2005, 60B, S93–S101. [Google Scholar] [CrossRef] [Green Version]
- Arcaya, M.C.; Arcaya, A.L.; Subramania, S.V. Inequalities in health: Definitions, concepts, and theories. Glob. Health Action 2015, 8, 27106. [Google Scholar] [CrossRef]
- Turrell, G.; Lynch, J.W.; Kaplan, G.A.; Everson, S.A.; Helkaka, E.L.; Kauhanen, J.; Salonen, J.T. Socioeconomic position across the lifecourse and cognitive function in late middle age. J. Gerontol. Soc. Sci. 2002, 57B, S43–S51. [Google Scholar] [CrossRef]
- House, J.S. Understanding social factors and inequalities in health: 20th century progress and 21th century prospects. J. Health Soc. Behav. 2002, 43, 125–142. [Google Scholar] [CrossRef] [Green Version]
- Ayre, D. Poor Mental Health: The Links between Child Poverty and Mental Health Problems. Available online: https://www.childrenssociety.org.uk/sites/default/files/poor_mental_healthreport.pdf (accessed on 10 September 2020).
- Choi, J.H.; Jun, J.A. Adolescents’ mental health and its relationship with health behavior. Health Welf. Policy Forum 2017, 245, 72–83. [Google Scholar]
- Jun, H.J.; Kim, M.Y. Childhood socioeconomic risk factors and depression in old age: A latent class analysis. J. Korean Gerontol. Soc. 2013, 33, 439–460. [Google Scholar]
- Lee, H.J.; Jung, E.H. Socioeconomic status and elderly health in life course perspective: Testing of multi-mediational effects of socioeconomic status in early adult and middle aged. Health Soc. Welf. Rev. 2016, 36, 53–84. [Google Scholar]
- Kang, Y.; Jung, K. Income inequality and health in Korea. Korean Public Adm. Rev. 2012, 46, 265–291. [Google Scholar]
- Park, H. Prevalence and related risk factors of depressive symptoms for adults in Korea: Results from the Korean National Health and Nutrition Examination Survey, 2009. In Korea Centers for Disease Control & Prevention; Ministry of Health and Welfare: Sejong, Korea, 2011. [Google Scholar]
- Braveman, P.; Barclay, C. Health disparities beginning in childhood: A life-course perspective. Pediatrics 2009, 124, S163–S175. [Google Scholar] [CrossRef] [Green Version]
- Adler, N.E.; Stewart, J.; Cohen, S.; Cullen, M.; Roux, A.D.; Dow, W.; Evans, G.; Kawachi, I.; Marmot, M.; Matthews, K.; et al. Reaching for a Healthier Life: Facts on Socioeconomic Status and Health in the U.S.; MacArthur Foundation Research Network on Socioeconomic Status and Health: San Francisco, CA, USA, 2007. [Google Scholar]
- Reynolds, J.R.; Ross, C.E. Social stratification and health: Education’s benefit beyond economic status and social origins. Soc. Probl. 1998, 45, 221–247. [Google Scholar] [CrossRef]
- Moccia, L.; Mazza, M.; Di Nicola, M.; Janiri, L. The experience of pleasure: A perspective between neuroscience and psychoanalysis. Front. Hum. Neurosci. 2018, 12, 359. [Google Scholar] [CrossRef]
- Wickrama, K.A.S.; Surjadi, F.F.; Lorenz, F.O.; Conger, R.D.; O’Neal, C.W. Family economic hardship and progression of poor mental health in middle-aged husbands and wives. Fam. Relat. 2012, 61, 297–312. [Google Scholar] [CrossRef] [Green Version]
- Zahn-Waxler, C.; Polanichka, N. All things interpersonal: Socialization and female aggression. In Aggression, Antisocial Behavior, and Violence among Girls: A Developmental Perspective; Putallaz, K., Bierman, K.L., Eds.; The Guilford Press: New York, NY, USA, 2004; pp. 48–70. [Google Scholar]
- Araya, R.; Lewis, G.; Rojas, G.; Fritsch, R. Education and income: Which is more important for mental health? J. Epidemiol. Community Health 2003, 57, 575–581. [Google Scholar] [CrossRef] [Green Version]
- Kosidou, K.; Dalman, C.; Lundberg, M.; Hallqvist, J.; Isacsson, G.; Magnusson, C. Socioeconomic status and risk of psychological distress and depression in the Stockholm Public Health Cohort: A population-based study. J. Affect. Disord. 2011, 134, 160–167. [Google Scholar] [CrossRef]
- Lewis, G.; Bebbington, P.; Brugha, T.; Farrell, M.; Gill, B.; Jenkins, R.; Meltzer, H. Socio-economic status, standard of living and neurotic disorder. Lancet 1998, 352, 605–609. [Google Scholar] [CrossRef]
- Mojtabai, R.; Olfson, M. Major depression in community-dwelling middle-aged and older adults: Prevalence and 2- and 4-year follow-up symptoms. Psychol. Med. 2004, 34, 623–634. [Google Scholar] [CrossRef]
- Turney, K. Maternal depression and childhood health inequalities. J. Health Soc. Behav. 2011, 52, 314–332. [Google Scholar] [CrossRef] [Green Version]
- Bowen, N.K.; Guo, S. Structural Equation Modeling; Oxford University Press: New York, NY, USA, 2011. [Google Scholar]
- Brown, G.W.; Harris, T.O. Depression and the serotonin transporter 5-HTTLPR polymorphism: A review and a hypothesis concerning gene-environment interaction. J. Affect. Disord. 2008, 111, 1–12. [Google Scholar] [CrossRef]
- Ji, E.J. A study of the income inequality of the aged in OECD 10 countries: Focusing on the life course perspective. Korean J. Soc. Welf. Stud. 2011, 42, 333–370. [Google Scholar]
- Lynch, S.M. Cohort and life-course patterns in the relationship between education and health: A hierarchical approach. Demography 2003, 40, 309–331. [Google Scholar] [CrossRef]
- Weissman, M.M.; Warner, V.; Wickramaratne, P.; Moreau, D.; Olfson, M. Offspring of depressed parents: 10 years later. Arch. Gen. Psychiatry 1997, 54, 932–940. [Google Scholar] [CrossRef]
- Marot, M.; Shipley, M.; Brunner, E.; Hemingway, H. Relative contribution of early life and adult socioeconomic factors to adult morbidity in the Whitehall II Study. J. Epidemiol. Community Health 2001, 55, 301–307. [Google Scholar] [CrossRef] [Green Version]
- Davies, P.T.; Windle, M. Gender-specific pathways between maternal depressive symptoms, family discord, and adolescent adjustment. Dev. Psychol. 1997, 33, 657–668. [Google Scholar] [CrossRef]
- Fergusson, D.M.; Horwood, L.J.; Lynskey, M.T. Maternal depressive symptoms and depressive symptoms in adolescents. J. Child Psychol. Psychiatry 1995, 36, 1161–1178. [Google Scholar] [CrossRef]
- Hammen, C. The generation of stress in the course of unipolar depression. J. Abnorm. Psychol. 1991, 100, 555–561. [Google Scholar] [CrossRef]
- Hammen, C.; Hazel, N.A.; Brennan, P.A.; Najman, J. Intergenerational transmission and continuity of stress and depression: Depressed women and their offspring in 20 years of follow-up. Psychol. Med. 2012, 42, 931–942. [Google Scholar] [CrossRef] [Green Version]
- Wheaton, B. The sociogenesis of psychological disorder: An attributional theory. J. Health Soc. Behav. 1980, 21, 100–124. [Google Scholar] [CrossRef]
- Hops, H. Intergenerational transmission of depressive symptoms: Gender and developmental consideration. In Interpersonal Factors in the Origin and Course of Affective Disorders; Mundt, C., Goldstein, M.J., Hahlweg, K., Fiedler, P., Eds.; The Royal College of Psychiatrist: London, UK, 1990; pp. 113–129. [Google Scholar]
- Zhao, X.; Lynch, J.G.; Chen, Q. Reconsidering Baron and Kenny: Myths and truths about mediation analysis. J. Consum. Res. 2010, 37, 197–206. [Google Scholar] [CrossRef]
- Ritsher, J.E.; Warner, V.; Johnson, J.G.; Dohrenwend, B.P. Inter-generational longitudinal study of social class and depression: A test of social causation and social selection models. Br. J. Psychiatry 2001, 178 (Suppl. 40), S84–S90. [Google Scholar] [CrossRef] [Green Version]
- Hoe, M.; Park, B.; Bae, S. Testing measurement invariance of the 11-item Korean Version CES-D Scale. Ment. Health Soc. Work 2015, 43, 313–339. [Google Scholar]
- Radloff, L.S. The CES-D Scale: A self-report depression scale for research in the general population. J. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Muthen, L.K.; Muthen, B.O. Mplus User’s Guide; Muthen&Muthen: Los Angeles, CA, USA, 2007. [Google Scholar]
- Dalgaard, P. Introductory Statistics with R. Statistics and Computing; Springer: New York, NY, USA, 2008. [Google Scholar]
- Lavrakas, P.J. Encyclopedia of Survey Research Methods; SAGE: Thousand Oaks, CA, USA, 2008. [Google Scholar]
- MacKinnon, D.P.; Lockwood, C.M.; Hoffman, J.M.; West, S.G.; Sheets, V. A comparison of methods to test mediation and other intervening variable effects. Psychol. Methods 2002, 7, 83–104. [Google Scholar] [CrossRef]
- Gulseren, L.; Erol, A.; Gulseren, S.; Kuey, L.; Kilic, B.; Ergor, G. From antepartum to postpartum: A prospective study on the prevalence of peripartum depression in a semiurban Turkish community. J. Reprod. Med. 2006, 51, 955–960. [Google Scholar]
- Maselko, J.; Bates, L.; Bhalotra, S.; Gallis, J.A.; O’Donnell, K.; Sikander, S.; Turner, E.L. Socioeconomic status indicators and common mental disorders: Evidence from a study of prenatal depression in Pakistan. SSM Popul. Health 2018, 4, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Patel, V.; Kirkwood, B.R.; Pednekar, S.; Weiss, H.; Mabey, D. Risk factors for common mental disorders in women: Population-based longitudinal study. Br. J. Psychiatry 2006, 189, 547–555. [Google Scholar] [CrossRef]
- Seplaki, C.L.; Goldman, M.; Weinstein, M.; Lin, Y.H. Before and after the 1999 chi-chi earthquake: Traumatic events and depressive symptoms in an older population. Soc. Sci. Med. 2006, 62, 3121–3132. [Google Scholar] [CrossRef] [Green Version]
- Perlin, L.; Schieman, S.; Fazio, E.; Meersman, S. Stress, health, and the life course: Some conceptual perspectives. J. Health Soc. Behav. 2005, 46, 205–219. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Selected (n = 189) | Unselected (n = 462) | t-Value | p-Value |
|---|---|---|---|---|
| M(SD) | M(SD) | |||
| G1 Economic Status (range = 1–5) | 3.2 (0.9) | 3.3 (0.9) | 1.86 | p > 0.05 |
| G2 Mother’s year of education (range = 1–18) | 10.6 (2.9) | 10.0 (3.1) | −1.38 | p > 0.05 |
| G2 Mother’s depressive symptoms (range = 0–24) | 9.7 (4.6) | 9.9 (4.8) | 0.55 | p > 0.05 |
| G2 Mother’s age (range = 40–63) | 50.2 (5.1) | 50.8 (5.3) | 1.27 | p > 0.05 |
| G2 Mother’s number of sibling (range = 1–10) | 5.4 (1.7) | 5.2 (1.8) | −1.20 | p > 0.05 |
| G2 Mother’s household yearly income | 1906.9 (1207.1) | 1893.1 (1239.7) | 0.13 | p > 0.05 |
| ( | ||||
| G3 Daughter’s depressive symptoms (range = 0–20) | 8.6 (4.5) | 9.5 (3.8) | 1.50 | p > 0.05 |
| G3 Daughter’s age (range = 19–39) | 23.8 (4.3) | 24.6 (4.2) | 1.94 | p > 0.05 |
| G3 Daughter’s number of sibling (range = 1–5) | 2.4 (0.7) | 2.5 (0.9) | 1.72 | p > 0.05 |
| G3 Daughter’s year of education (range = 9–22) | 14.6 (1.8) | 14.4 (1.9) | −0.89 | p > 0.05 |
| (%) | (%) | x2 | ||
| G1 Grandfather’s less than primary school graduation | 19.0 | 24.1 | 1.85 | p > 0.05 |
| G1 Grandmother’s less than primary school graduation | 31.2 | 34.8 | 0.75 | p > 0.05 |
| G2 Mother’s employment (employed) | 48.1 | 43.1 | 1.40 | p > 0.05 |
| G2 Mother’s living with spouse (yes) | 78.8 | 84.4 | 2.93 | p > 0.05 |
| G3 Daughter’s employment (employed) | 43.4 | 49.6 | 2.05 | p > 0.05 |
| Socioeconomic Factors | Depressive Symptoms | |
|---|---|---|
| G2 Mothers | G3 Daughters | |
| G1 grandfather’s less than primary school graduation | 0.003 | 0.04 |
| G1 grandmother’s less than primary school graduation | 0.12 | 0.07 |
| G1 economic status | 0.22 ** | 0.18 *** |
| G2 mother’s year of education | −0.27 *** | −0.13 |
| G2 mother’s economic status | 0.47 | 0.09 |
| Pathways | Standardized Estimate | Standard Error | t-Value |
|---|---|---|---|
| FromG1 SES to G2 Depressive Symptoms | |||
| G1 economic status→G2 year of education→G2 depression | 0.071 * | 0.031 | 2.276 |
| FromG1 SES to G3 Depressive Symptoms | |||
| G1 economic status→G2 depression→G3 depression | 0.061 * | 0.031 | 1.990 |
| G1 economic status→G2 year of education→G2 depression→G3 depression | 0.031 * | 0.015 | 2.158 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, A. The Impact of Childhood and Adult Educational Attainment and Economic Status on Later Depressive Symptoms and Its Intergenerational Effect. Int. J. Environ. Res. Public Health 2020, 17, 8970. https://doi.org/10.3390/ijerph17238970
Park A. The Impact of Childhood and Adult Educational Attainment and Economic Status on Later Depressive Symptoms and Its Intergenerational Effect. International Journal of Environmental Research and Public Health. 2020; 17(23):8970. https://doi.org/10.3390/ijerph17238970
Chicago/Turabian StylePark, Aely. 2020. "The Impact of Childhood and Adult Educational Attainment and Economic Status on Later Depressive Symptoms and Its Intergenerational Effect" International Journal of Environmental Research and Public Health 17, no. 23: 8970. https://doi.org/10.3390/ijerph17238970