The Spatial Correlations of Health Resource Agglomeration Capacities and Their Influencing Factors: Evidence from China

Abstract
:1. Introduction
2. Methods and Data Sources
2.1. Methods
2.1.1. Measurement of Health Resource Agglomeration Capacities
2.1.2. Method for Constructing a Spatial Correlation Network of Health Resource Agglomeration Capacities
2.1.3. Network Characterization of Spatial Correlations between Health Resource Agglomeration Capacities
2.1.4. Block Model Analysis for the Spatial Correlation Network of Health Resource Agglomeration Capacities
2.2. Study Area and Data Sources
3. Spatial Correlation Analysis of China’s Health Resource Agglomeration Capacity
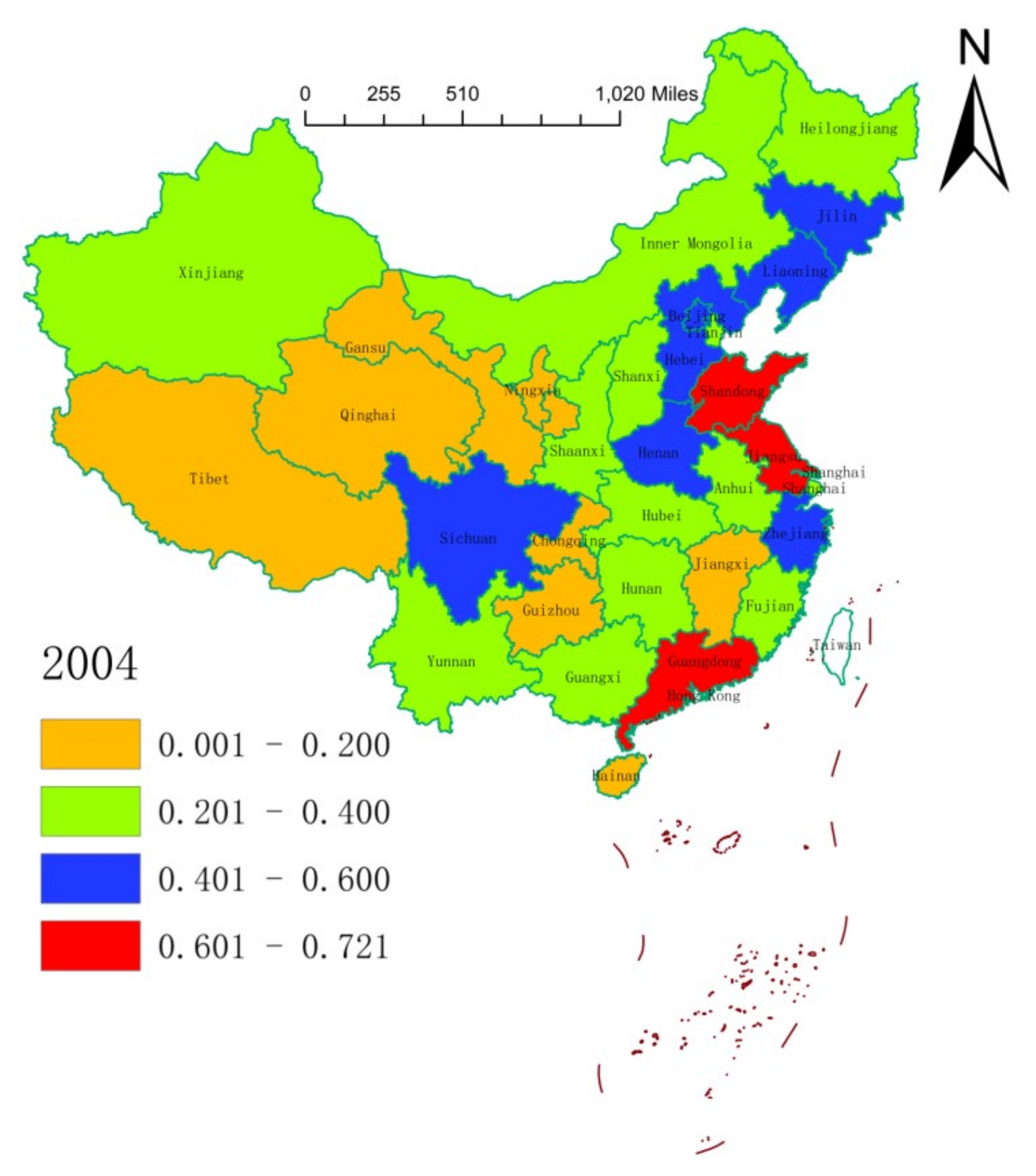
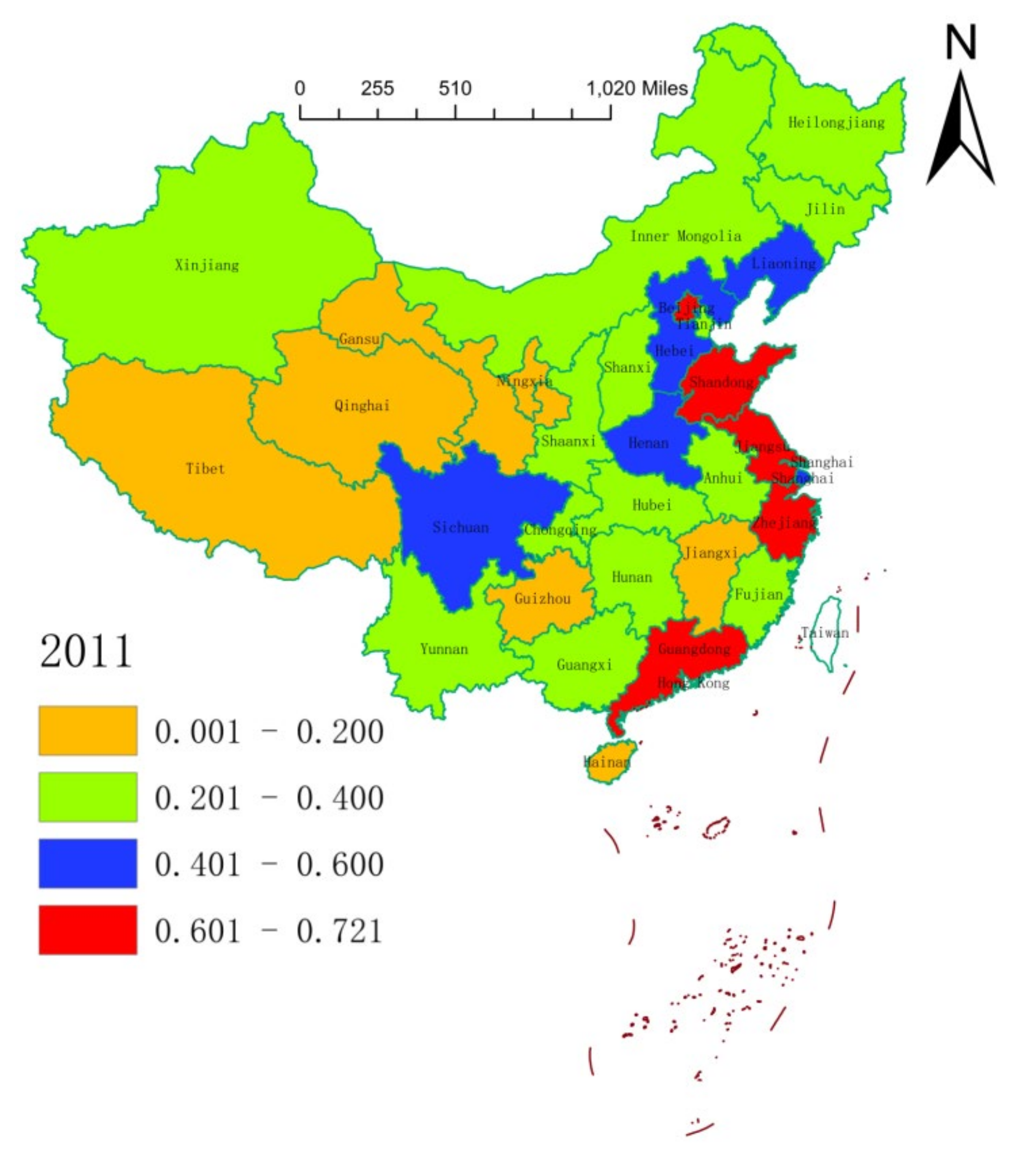
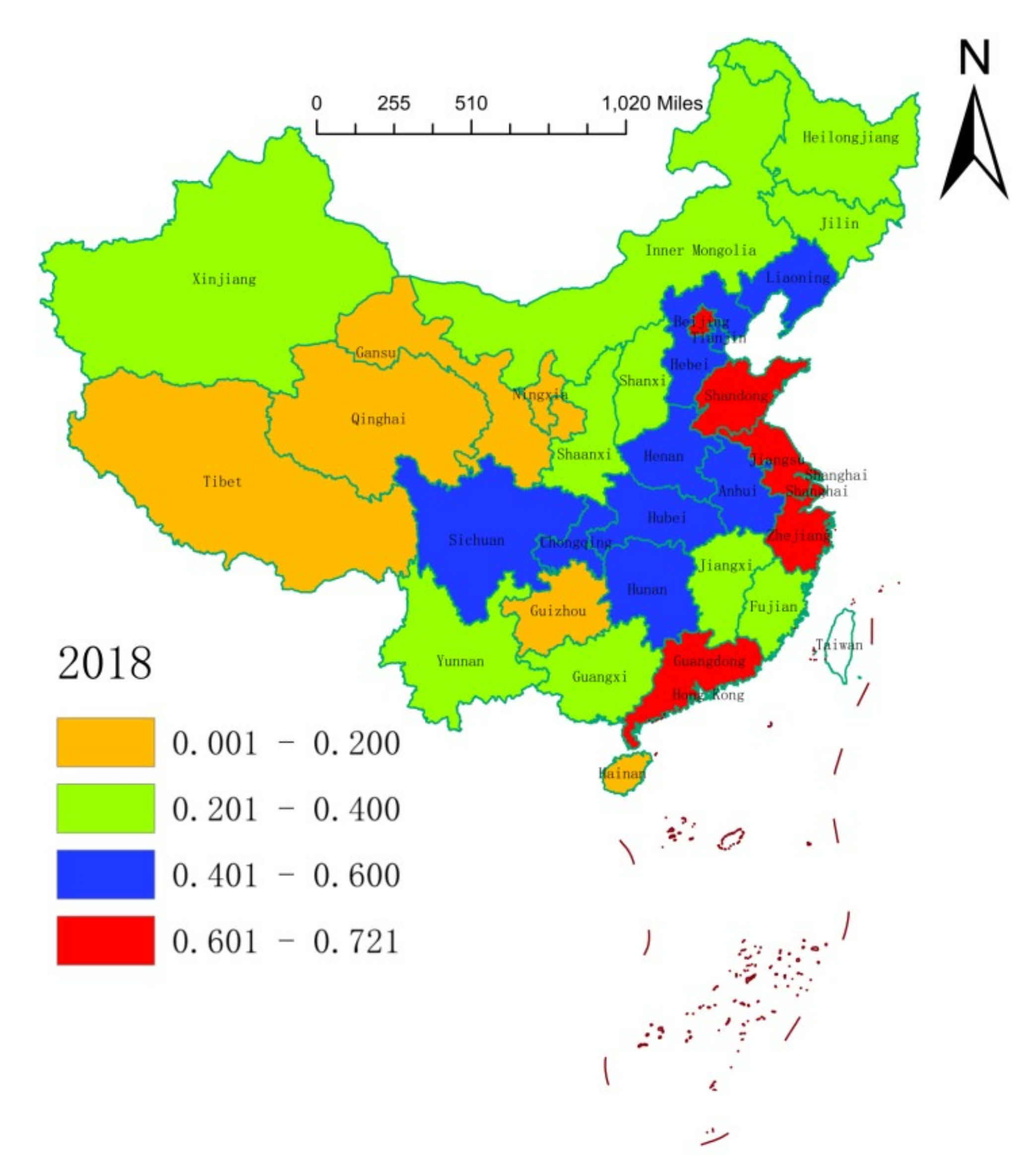
3.1. Spatial Distribution of the Health Resource Agglomeration Capacities in China
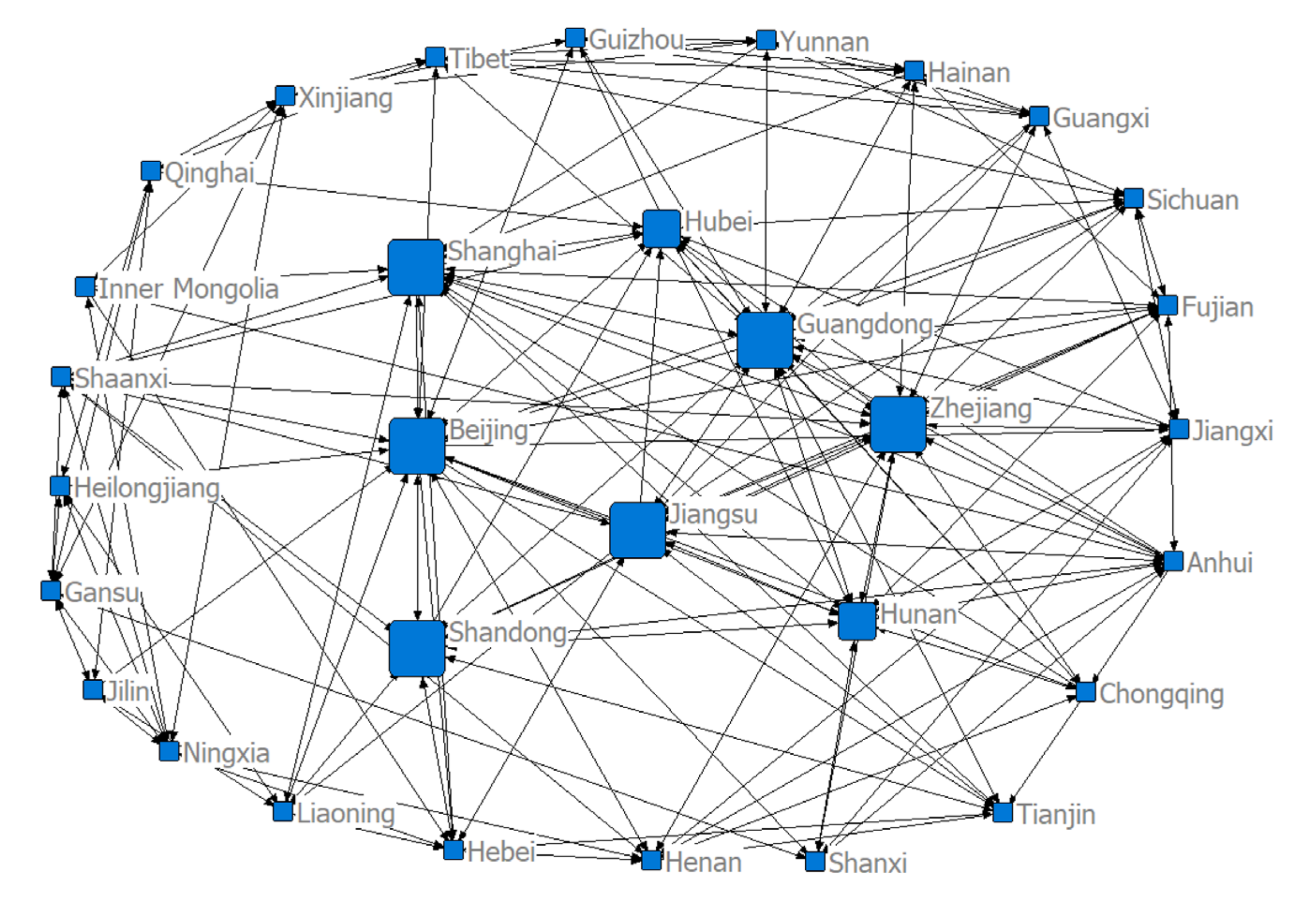
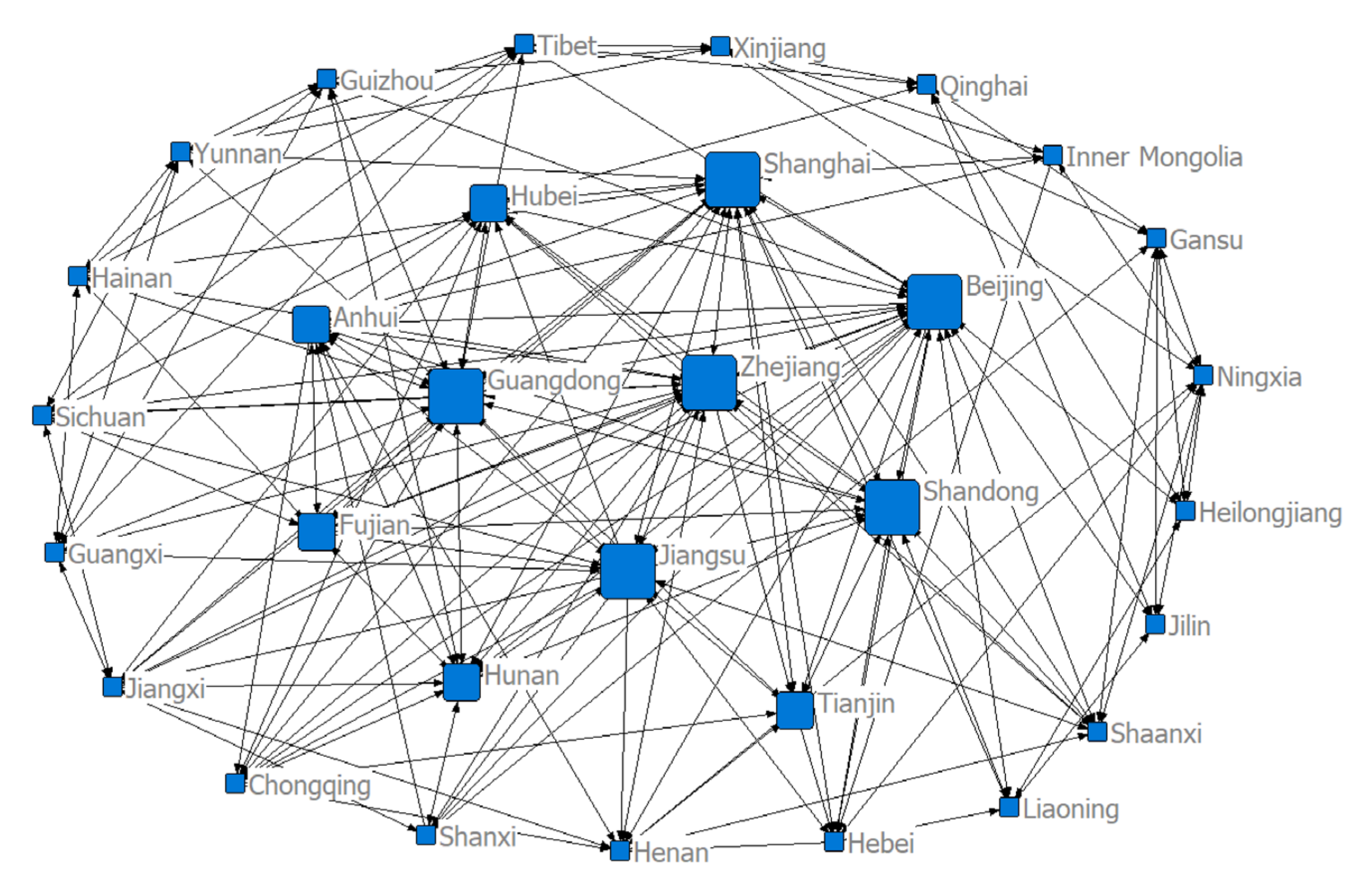
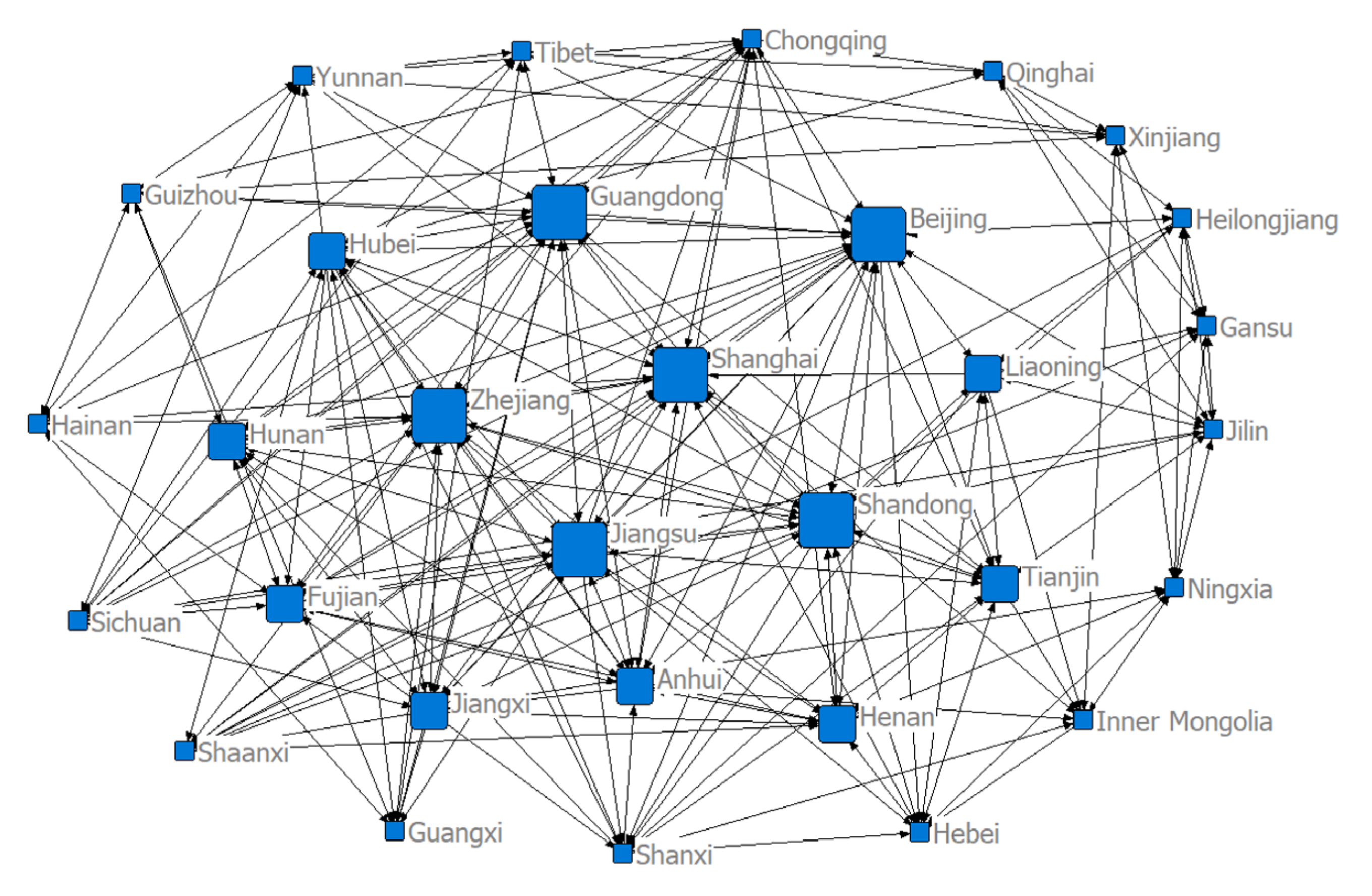
3.2. Structure of the Spatial Correlation Network of Health Resource Agglomeration Capacities in China
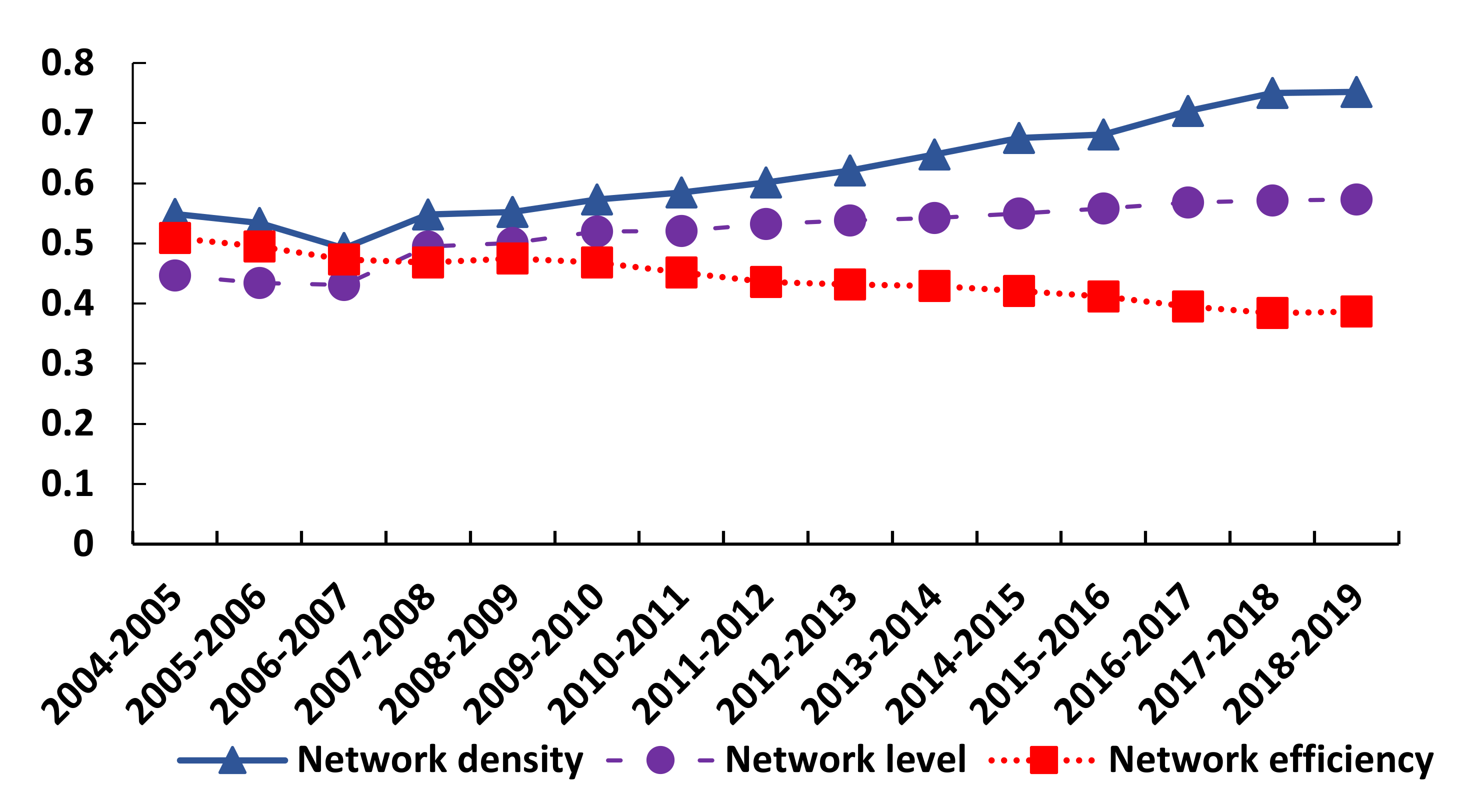
3.3. Time Series Changes in the Structure of the Spatial Correlation Network of Health Resource Agglomeration Capacities in China
3.4. Centrality of the Spatial Correlation Network of Health Resource Agglomeration Capacities in China
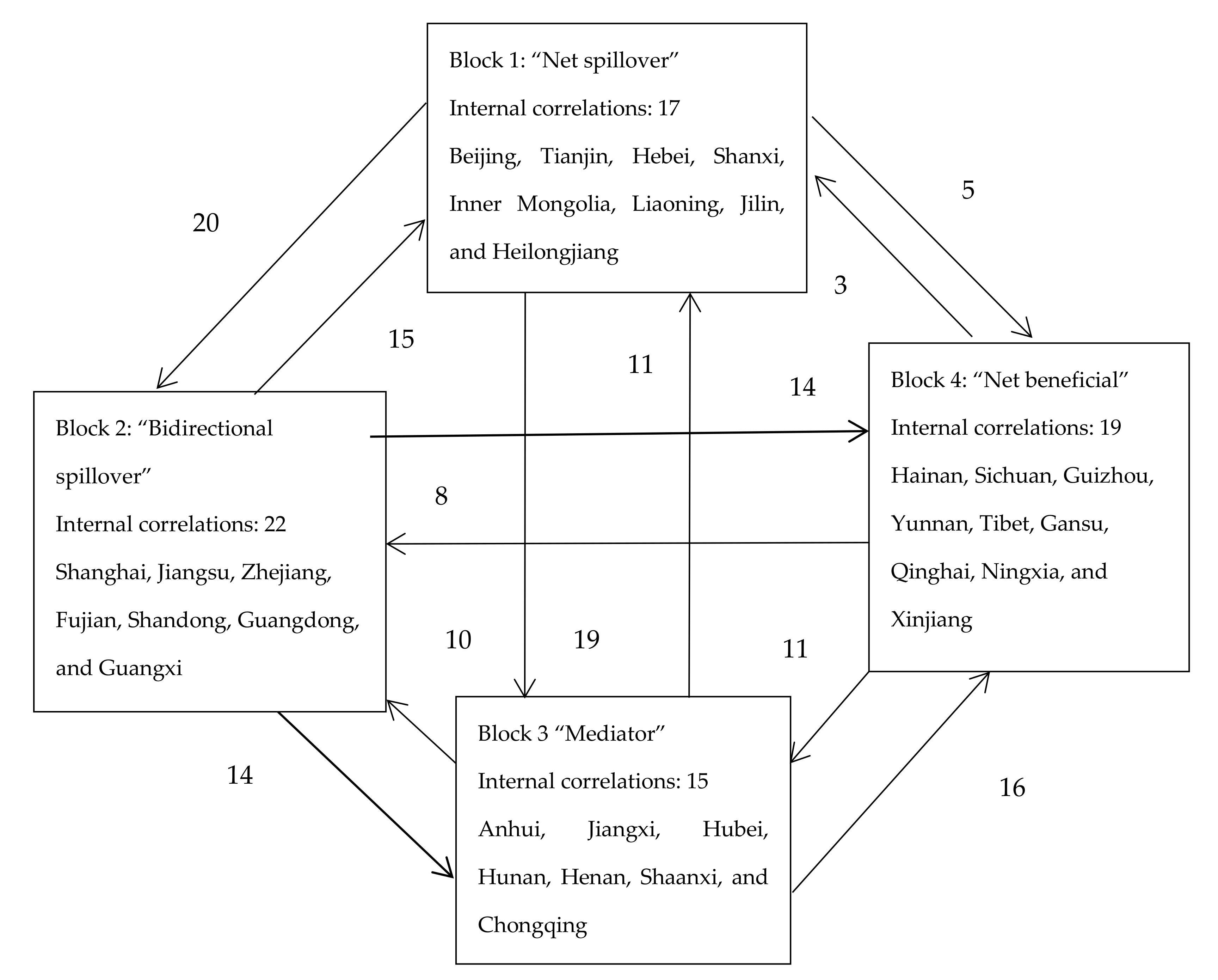
3.5. Block Model Analysis of the Spatial Correlation Network of Health Resource Agglomeration Capacities in China
4. Analysis of Factors Influencing the Spatial Correlation Network of Health Resource Agglomeration Capacities in China
4.1. Selection of Influencing Factors
4.2. Correlation Analysis of Factors Influencing the Spatial Network of Health Resource Agglomeration Capacities in China
5. Conclusions
Policy Recommendations
Author Contributions
Funding
Conflicts of Interest
References
- Song, X.; Deng, W.; Liu, Y. Spatial spillover and the factors influencing public service supply in Sichuan province, China. J. Mt. Sci. 2014, 11, 1356–1371. [Google Scholar] [CrossRef]
- Lee, W.-Y.; Shaw, I. The Impact of Out-of-Pocket Payments on Health Care Inequity: The Case of National Health Insurance in South Korea. Int. J. Environ. Res. Public Heal. 2014, 11, 7304–7318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savedoff, W.; De Ferranti, D.; Smith, A.L.; Fan, V. Political and economic aspects of the transition to universal health coverage. Lancet 2012, 380, 924–932. [Google Scholar] [CrossRef]
- Yip, W.C.-M.; Hsiao, W.C.; Chen, W.; Hu, S.; Ma, J.; Maynard, A. Early appraisal of China’s huge and complex health-care reforms. Lancet 2012, 379, 833–842. [Google Scholar] [CrossRef]
- Morales-Briones, D.F.; Gehrke, B.; Huang, C.-H.; Liston, A.; Ma, H.; Marx, H.E.; Tank, D.C.; Yang, Y. Analysis of paralogs in target enrichment data pinpoints multiple ancient polyploidy events in Alchemilla s.l. (Rosaceae). In Trends in Access to Health Services and Financial Protection in China Between 2003 and 2011: A Cross-Sectional Study. Lancet 2012; Cold Spring Harbor Laboratory: New York, NY, USA, 2020; Volume 379, pp. 805–814. [Google Scholar]
- Hu, H.; Chen, D.; Gao, Q.; Liu, P. Evaluation on Health Resources Allocation in Zhejiang Based on Agglomeration Degree. Chinese Heal. Econ. 2016, 7, 56–59. [Google Scholar]
- Gong, H.; Wu, Z.; Wu, B.; Ye, Q.; Luo, Z. Analysis on Spatial Aggregation Feature of Health Resources in Guangdong. Chinese Heal. Econ. 2017, 5, 52–55. [Google Scholar]
- Tang, Q.M.; Nie, J. Research on the Medical Investment Gap, Medical Development Indexes and the Influencing Factors of the Western Region. Chinese J. Heal. Stat. 2015, 4, 47–49. [Google Scholar]
- Song, S.; Yuan, B.; Zhang, L.; Cheng, G.; Zhu, W.; Hou, Z.; He, L.; Ma, X.; Meng, Q. Increased Inequalities in Health Resource and Access to Health Care in Rural China. Int. J. Environ. Res. Public Health 2019, 1, 49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romanilos, T.; Roser, M.; Diego, V.; Badiella, L.; Boada, M. Protected natural Areas: In Sickness and in Health. Int. J. Environ. Res. Public Health 2018, 15, 2182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anand, S.; Fan, V.Y.; Zhang, J.; Zhang, L.; Ke, Y.; Dong, Z.; Chen, L.C. China’s human resources for health: Quantity, quality, and distribution. Lancet 2008, 372, 1774–1781. [Google Scholar] [CrossRef]
- Wang, W.; Loban, E.; Dionne, E. Public Hospitals in China: Is There a Variation in Patient Experience with Inpatient Care. Int. J. Environ. Res. Public Heal. 2019, 16, 193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jenkinson, C.; Coulter, A.; Bruster, S. The Picker Patient Experience Questionnaire: Development and validation using data from in-patient surveys in five countries. Int. J. Qual. Heal. Care 2002, 14, 353–358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jenkinson, C.; Coulter, A.; Reeves, R.; Bruster, S.; Richards, N. Properties of the Picker Patient Experience questionnaire in a randomized controlled trial of long versus short form survey instruments. J. Public Heal. Med. 2003, 25, 197–201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.H.; Park, I.Y.; Kwun, Y.C.; Tan, X. Extension of the TOPSIS method for decision making problems under interval-valued intuitionistic fuzzy environment. Appl. Math. Model. 2011, 35, 2544–2556. [Google Scholar] [CrossRef]
- Wei, F.Q.; Ma, J. Analysis of the Agglomeration Degree of Health Resources in Traditional Chinese Medicine. Chin. J. of Hosp. Adm. 2016, 10, 789–792. [Google Scholar]
- Guo, Q.; Luo, K. Concentration of Healthcare Resources in China: The Spatial–Temporal Evolution and Its Spatial Drivers. Int. J. Environ. Res. Public Heal. 2019, 16, 4606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nikzad, R. Canadian worldwide patent activity: An industrial level analysis. World Pat. Inf. 2014, 38, 12–18. [Google Scholar] [CrossRef]
- Teow, K.L.; Tan, K.B.; Phua, H.P.; Zhu, Z. Applying Gravity model to predict demand of public hospital beds. Oper. Res. Heal. Care 2018, 17, 65–70. [Google Scholar] [CrossRef]
- Babri, S.; Jørnsten, K.; Viertel, M. Application of gravity models with a fixed component in the international trade flows of coal, iron ore and crude oil. Marit. Econ. Logist. 2017, 19, 334–351. [Google Scholar] [CrossRef]
- Lundmark, R. Analysis and projection of global iron ore trade: A panel data gravity model approach. Miner. Econ. 2017, 31, 191–202. [Google Scholar] [CrossRef] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Indicator | Weight | |
|---|---|---|
| Evaluation Indicators | Number of Hospitals | 0.128 |
| Number of Community Health Service Centers/Stations | 0.173 | |
| Number of Certified Physician Assistants | 0.080 | |
| Number of Certified Physicians | 0.084 | |
| Number of Registered Nurses | 0.075 | |
| Number of Managers in Medical Institutions | 0.080 | |
| Number of Workers in Medical Institutions | 0.082 | |
| Number of Healthcare Practitioners / 1,000 People | 0.088 | |
| Total Assets of Health Institutions (RMB 1,000) | 0.093 | |
| Number of Hospital Beds / 1,000 People | 0.117 |
| Province or Municipality | 2004 | 2011 | 2018 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Degree Centrality | Betweenness Centrality | Closeness Centrality | Degree Centrality | Betweenness Centrality | Closeness Centrality | Degree Centrality | Betweenness Centrality | Closeness Centrality | |
| Beijing | 0.5 | 98.37 | 0.612 | 0.633 | 137.396 | 0.769 | 0.65 | 108.253 | 0.769 |
| Tianjin | 0.216 | 5.317 | 0.484 | 0.333 | 21.418 | 0.588 | 0.367 | 20.369 | 0.6 |
| Hebei | 0.233 | 16.459 | 0.484 | 0.267 | 15.605 | 0.508 | 0.283 | 13.529 | 0.526 |
| Shanxi | 0.150 | 13.326 | 0.484 | 0.183 | 19.621 | 0.536 | 0.283 | 17.175 | 0.536 |
| Inner Mongolia | 0.133 | 8.158 | 0.5 | 0.2 | 19.358 | 0.508 | 0.2 | 12.531 | 0.517 |
| Liaoning | 0.2 | 25.769 | 0.508 | 0.2 | 7.416 | 0.517 | 0.267 | 8.386 | 0.566 |
| Jilin | 0.15 | 7.405 | 0.484 | 0.183 | 11.353 | 0.508 | 0.25 | 15.426 | 0.556 |
| Heilongjiang | 0.15 | 7.405 | 0.484 | 0.167 | 9.046 | 0.508 | 0.217 | 8.59 | 0.536 |
| Shanghai | 0.4 | 50.962 | 0.6 | 0.458 | 47.906 | 0.638 | 0.517 | 43.681 | 0.667 |
| Jiangsu | 0.35 | 33.408 | 0.6 | 0.458 | 35.011 | 0.652 | 0.517 | 32.574 | 0.698 |
| Zhejiang | 0.433 | 41.043 | 0.577 | 0.533 | 45.835 | 0.682 | 0.55 | 38 | 0.682 |
| Anhui | 0.3 | 29.588 | 0.566 | 0.284 | 13.577 | 0.536 | 0.384 | 16.443 | 0.6 |
| Fujian | 0.316 | 12.606 | 0.536 | 0.333 | 9.997 | 0.536 | 0.383 | 10.603 | 0.556 |
| Jiangxi | 0.267 | 14.938 | 0.517 | 0.316 | 9.483 | 0.566 | 0.333 | 7.474 | 0.577 |
| Shandong | 0.317 | 23.705 | 0.6 | 0.417 | 24.51 | 0.6 | 0.467 | 31.974 | 0.625 |
| Henan | 0.317 | 30.353 | 0.545 | 0.3 | 21.461 | 0.556 | 0.333 | 19.728 | 0.577 |
| Hubei | 0.3 | 29.38 | 0.526 | 0.383 | 28.556 | 0.625 | 0.433 | 27.405 | 0.652 |
| Hunan | 0.4 | 33.194 | 0.577 | 0.367 | 16.258 | 0.577 | 0.384 | 11.851 | 0.577 |
| Guangdong | 0.517 | 69.654 | 0.612 | 0.533 | 62.078 | 0.652 | 0.567 | 54.294 | 0.682 |
| Guangxi | 0.25 | 9.257 | 0.526 | 0.233 | 6.974 | 0.508 | 0.25 | 6.321 | 0.508 |
| Hainan | 0.25 | 7.668 | 0.526 | 0.25 | 7.287 | 0.517 | 0.25 | 5.191 | 0.526 |
| Chongqing | 0.25 | 6.131 | 0.526 | 0.284 | 13.956 | 0.556 | 0.35 | 12.386 | 0.556 |
| Sichuan | 0.267 | 13.566 | 0.526 | 0.267 | 11.559 | 0.556 | 0.317 | 14.451 | 0.556 |
| Guizhou | 0.216 | 16.716 | 0.536 | 0.217 | 19.358 | 0.556 | 0.25 | 17.61 | 0.577 |
| Yunnan | 0.25 | 13.939 | 0.536 | 0.25 | 13.044 | 0.508 | 0.25 | 8.395 | 0.517 |
| Tibet | 0.267 | 33.671 | 0.556 | 0.217 | 21.096 | 0.492 | 0.267 | 25.743 | 0.577 |
| Shaanxi | 0.267 | 27.029 | 0.477 | 0.284 | 18.293 | 0.366 | 0.22 | 13.473 | 0.566 |
| Gansu | 0.233 | 24.873 | 0.5 | 0.217 | 17.25 | 0.5 | 0.284 | 13.843 | 0.517 |
| Qinghai | 0.2 | 26.005 | 0.462 | 0.217 | 23.835 | 0.545 | 0.217 | 15.67 | 0.556 |
| Ningxia | 0.267 | 40.32 | 0.517 | 0.217 | 14.998 | 0.476 | 0.267 | 21.142 | 0.536 |
| Xinjiang | 0.233 | 39.786 | 0.492 | 0.167 | 21.465 | 0.476 | 0.217 | 27.489 | 0.5 |
| Block | Number of Correlations Received | Number of Correlations Sent | Expected Proportion of Internal Correlations (%) | Actual Proportion of Internal Correlations (%) | ||
|---|---|---|---|---|---|---|
| Intra-block | Off-block | Intra-block | Off-block | |||
| Block 1 | 17 | 29 | 17 | 44 | 23.33% | 27.87% |
| Block 2 | 22 | 38 | 22 | 43 | 20.00% | 33.85% |
| Block 3 | 15 | 44 | 15 | 37 | 20.00% | 28.85% |
| Block 4 | 19 | 35 | 19 | 22 | 26.67% | 46.34% |
| Influencing Factor | Correlation Coefficient | Significance Level | Standard Deviation | Minimum Value | Maximum Value |
|---|---|---|---|---|---|
| PGDP | 0.3012 | 0.000 | 0.0012 | −0.1803 | 0.3429 |
| Pop | 0.2705 | 0.011 | 0.0000 | −0.1004 | 0.2906 |
| Urb | 0.2245 | 0.002 | 0.0026 | −0.1107 | 0.3771 |
| Stu | 0.1204 | 0.110 | 0.0001 | −0.2107 | 0.2005 |
| Wag | 0.1905 | 0.050 | 0.0006 | −0.1503 | 0.2702 |
| Exp | 0.2265 | 0.013 | 0.0003 | −0.1095 | 0.3045 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, Q.; Luo, K.; Hu, R. The Spatial Correlations of Health Resource Agglomeration Capacities and Their Influencing Factors: Evidence from China. Int. J. Environ. Res. Public Health 2020, 17, 8705. https://doi.org/10.3390/ijerph17228705
Guo Q, Luo K, Hu R. The Spatial Correlations of Health Resource Agglomeration Capacities and Their Influencing Factors: Evidence from China. International Journal of Environmental Research and Public Health. 2020; 17(22):8705. https://doi.org/10.3390/ijerph17228705
Chicago/Turabian StyleGuo, Qingbin, Kang Luo, and Ruodi Hu. 2020. "The Spatial Correlations of Health Resource Agglomeration Capacities and Their Influencing Factors: Evidence from China" International Journal of Environmental Research and Public Health 17, no. 22: 8705. https://doi.org/10.3390/ijerph17228705