Quality of Life and Concerns in Parent Caregivers of Adult Children Diagnosed with Intellectual Disability: A Qualitative Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Procedure
2.4. Data Analysis
3. Results
3.1. Theme 1: Changes Produced After the Diagnosis
“I was with my mother at her house for a while with my daughter, until we went to live in an apartment, but my mother said that my daughter couldn’t live there. So, we stayed in the village until we could sell the apartment and buy a house in the village so that my daughter would inherit this place in the future, which would be better…”.(I01 Mother)
“We’ve always wanted to look for solutions, in fact, we moved to a village, because we saw that she was not comfortable with the previous house. [I’m] always thinking about her well-being. We also moved to a new house because we found this center nearby, and when you see that she’s well taken care of, then you relax, of course […]. Also, my mother was a very big pillar [of support], because I was working at that time and my mother was the one who helped me with her...”.(I02 Mother)
“Everything we have done has been for the good of the child. We have had to buy and change vehicles for the child, for his comfort. He did not want to be in the old apartment, he had many sudden crises, that’s why we bought the land, we did the construction, we changed the house, and we built a room on the ground floor, even a swimming pool, because, as he really likes the water, that was good for him...”.(I03 Father)
“My wife did have to quit her job, and she had a fairly good job… We had to weigh up between taking care of our son or earning money. And she made even more money than me, but we had to decide, so she had to leave her job and take care of our son”.(I11 Father)
“When I was working, the teachers weren’t able to control my daughter, so I had to come out of work [to pick her up]. Walking, it took me more than half an hour, and then I had to make up the lost hours at work afterwards. Although at work they did give me permission, and everything was fine…”.(I05 Mother)
“When she was discharged, the director told us: Get it into your head your daughter will have to be in a wheelchair [for the rest of her life]. We said that we would do everything possible to prevent this from happening, and so, her mother took her to rehabilitation for 7 years, and during those years, we paid 45,000 pesetas (€270.45) every month. Of course, on some occasions we had help from the grandparents…”.(I13 Father)
“I have the future sorted out with the residence. Yes, I am concerned about money, so what I do is [put some money aside] for him, so that he has money in the future when we are not there and he can pay them, but of course, it is complicated because we don’t earn that much, and so that worry is there...”.(I04 Mother)
“Her brother had to grow up, and he was only 4 years old. He has always had to live with that nightmare, and that my 24 h of attention were directed to my girl. They have a good relationship as siblings, but I think he did feel jealous, and still does nowadays. […] He lived through it in sorrow...”.(I14 Mother)
“Her brother, delighted as always, sits down and listens to her. When he has a moment, he comes and sits with her and he loves it, and he laughs with her. He likes it when she tells him what she is and isn’t doing. He spends his time with her, and he loves it, and she already feels so integrated and so good too. Since he was little, he’s spent a lot of time with her, he even preferred doing that to going out with his friends. Today I can rest and assure that if something happens to me, I know her brother will be there with her”.(I06 Mother)
3.2. Theme 2: Interpersonal Relationships
“It’s that, they all say they love him a lot, but I feel that they’re not being honest. And I have my daughter, and she says that we should solve our own problems, but I already have enough with mine […]. In the village, I used to say, let his cousins come over and play with him and he can learn things, but his cousins have their own lives and they don’t think about coming to see their cousin or to help their aunt…”.(I10 Mother)
“Her brother has lived his life, but he has not been caring. That still bugs me, because he says he’s going to take care of her, but I won’t be here to see it, and that scares me. I’ll believe it when I see it, right? That’s my way of thinking...”.(I07 Mother)
“We don’t have anyone; I don’t know if this happens a lot in these situations. With any help or simply being able to speak to someone we would be very grateful, but when people see our situation, they move away, they continue their lives, they don’t have the same life as you and they don’t empathize with you, it is easier to run away…”.(I15 Father)
“What friends? You have no friends; nobody wants to listen... If you aren’t well, nobody wants to be by your side... Before, when I had to ask for help, it was when the children were boys and I was alone because my husband was working, and I had a friend who, from that moment, became very distant, we barely speak to each other now...”.(I16 Mother)
“We don’t go out, we don’t have a life, because we have to be with him, and we are locked up 24 h a day, the time he’s here in the center, is the only free time we have. Of course, we can’t have a married life, we’ve been like this for 37 years. And we have more and more arguments…”.(I03 Father)
“The usual thing when there is a problem of this type is separation, but it united us more, it united us a lot, because we believed that the person who was really in need was him, not us, and so we dedicated ourselves to him, and that dedication made us unite more…”.(I11-Father)
3.3. Theme 3: Physical and Emotional Well-Being as a Caregiver
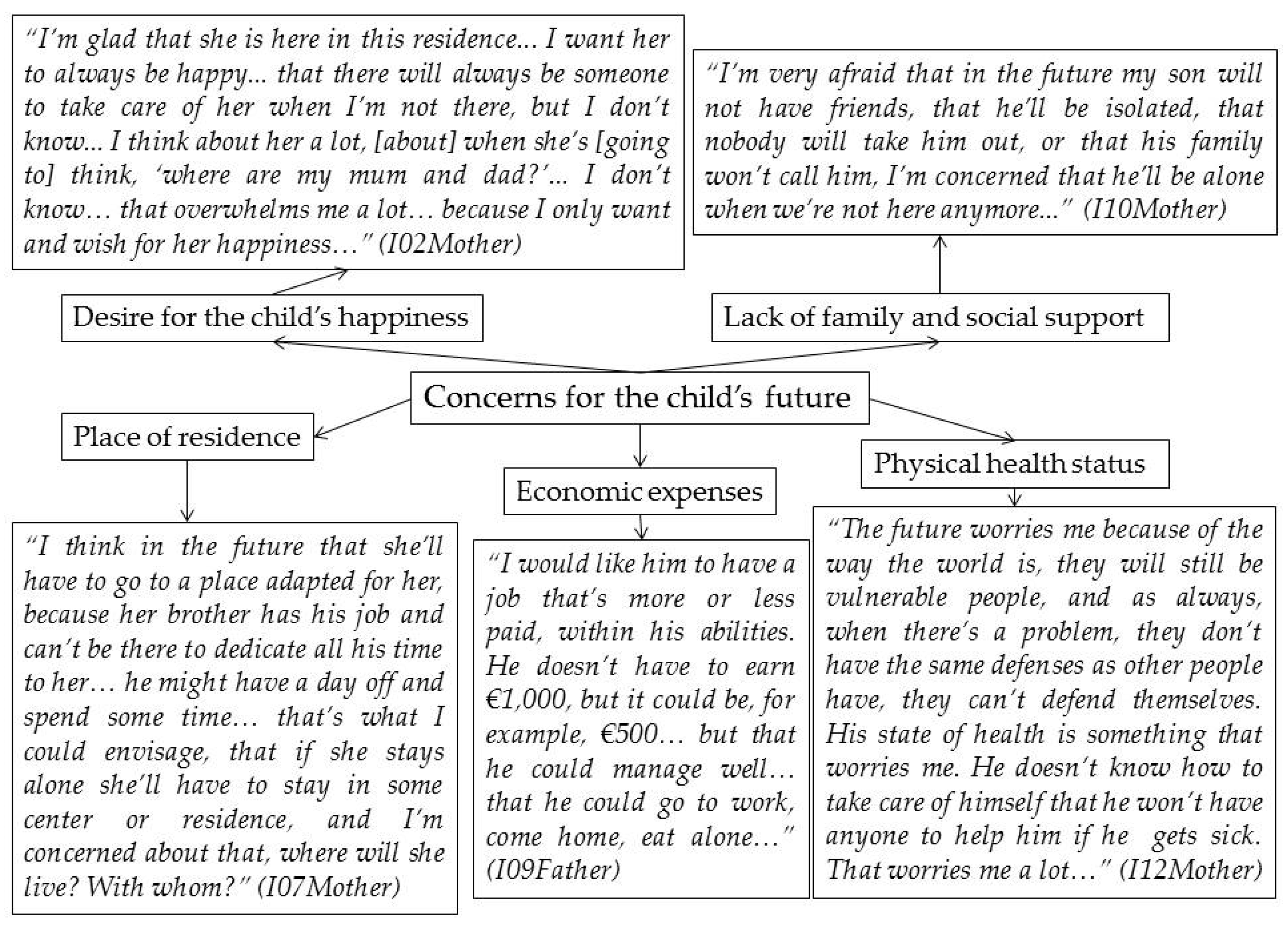
3.4. Theme 4: Concerns about the Future
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Broberg, M. Expectations and reactions to disability and normality experienced by parents of children with intellectual disability in Sweden. Child Care Health Dev. 2011, 37, 410–417. [Google Scholar] [CrossRef] [PubMed]
- Brown, J. Recurrent grief in mothering a child with an intellectual disability to adulthood: Grieving is the healing. Child Fam. Soc. Work 2013, 21, 113–122. [Google Scholar] [CrossRef]
- Fernández-Alcántara, M.; García-Caro, M.P.; Laynez-Rubio, C.; Pérez-Marfil, M.N.; Martí-García, C.; Benítez-Feliponi, Á.; Berrocal-Castellano, M.; Cruz-Quintana, F. Feelings of loss in parents of children with infantile cerebral palsy. Disabil. Health J. 2015, 8, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Van der Steen, S.L.; Riedijk, S.R.; Verhagen-Visser, J.; Govaerts, L.C.P.; Srebniak, M.I.; Van Opstal, D.; Joosten, M.; Knapen, M.F.C.M.; Tibben, A.; Diderich, K.E.M.; et al. The Psychological Impact of Prenatal Diagnosis and Disclosure of Susceptibility Loci: First Impressions of Parents´ experiences. J. Genet. Couns. 2016, 25, 1227–1234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schalock, R.L.; Borthwick-Duffy, S.A.; Bradley, V.J.; Buntinx, W.H.E.; Coulter, D.L.; Craig, E.M.; Gómez, S.C.; Lachapelle, Y.; Luckasson, R.; Reeve, A.; et al. Intellectual Disability: Definition, Classification, and Systems of Supports, 11th ed.; American Association on Intellectual and Developmental Disabilities: Washington, DC, USA, 2010. [Google Scholar]
- Costanzo, F.; Varuzza, C.; Menghini, D.; Addona, F.; Giane, T.; Vicari, S. Executive functions in intellectual disabilities: A comparison between Williams syndrome and Down syndrome. Res. Dev. Disabil. 2013, 34, 1770–1780. [Google Scholar] [CrossRef]
- Lott, I.T.; Dierssen, M. Cognitive deficits and associated neurological complications in individuals with Down´s syndrome. Lancet. Neurol. 2010, 9, 623–633. [Google Scholar] [CrossRef]
- Takenoshita, S.; Terada, S.; Kuwano, R.; Inoue, T.; Cyoju, A.; Suemitsu, S.; Yamada, N. Prevalence of dementia in people with intellectual disabilities: Cross-sectional study. Int. J. Geriatr. Psychiatry 2020. [Google Scholar] [CrossRef] [Green Version]
- Spindler, U.P.; Hotopp, L.C.; Bach, V.A.; Hornemann, F.; Syrbe, S.; Merkenschlager, A.; Kiess, W.; Bernhard, M.K.; Bertsche, T.; Neininger, M.P.; et al. Seizure disorders and developmental disorders: Impact on life of affected families-a structured interview. Eur. J. Pediatr. 2017, 176, 1121–1129. [Google Scholar] [CrossRef]
- Luijkx, J.; van der Putten, A.A.J.; Vlaskamp, C. Time use of parents raising children with severe or profound intellectual and multiple disabilities. Child Care Health Dev. 2017, 43, 518–526. [Google Scholar] [CrossRef]
- Thompson, R.; Kerr, M.; Glynn, M.; Linehan, C. Caring for a family member with intellectual disability and epilepsy: Practical, social and emotional perspectives. Seizure 2014, 23, 856–863. [Google Scholar] [CrossRef] [Green Version]
- Gallagher, S.; Whiteley, J. Social support is associated with blood pressure responses in parents caring for children with developmental disabilities. Res. Dev. Disabil. 2012, 33, 2099–2105. [Google Scholar] [CrossRef] [Green Version]
- Pisula, E.; Porębowicz-Do Èrsmann, A. Family functioning, parenting stress and quality of life in mothers and fathers of Polish children with high functioning autism or Asperger syndrome. PLoS ONE 2017, 12. [Google Scholar] [CrossRef]
- Bompori, E.; Niakas, D.; Nakou, I.; Siamopoulou-Mavridou, A.; Tzoufi, M.S. Comparative study of the health-realted quality of life of children with epilepsy and their parents. Epilepsy Behav. 2014, 41. [Google Scholar] [CrossRef] [PubMed]
- Matteucci, M.C.; Scalone, L.; Tomasetto, C.; Cavrini, G.; Selleri, P. Health-related quality of life and psychological wellbeing of children with Specific Learning Disorders and their mothers. Res. Dev. Disabil. 2019, 87. [Google Scholar] [CrossRef]
- Sim, A.; Cordier, R.; Sharmila, V.; Torbojorn, F. Relationship satisfaction in couples raising a child with autism spectrum disorder: A systematic review of the literature. Res. Autism Spectr. Disord. 2016, 31, 30–52. [Google Scholar] [CrossRef]
- Somanadham, S.; Larkin, P.J. Parents´ experiences of living with, and caring for children, adolescents, and Young adults with Mucopolysaccharidosis. Orphanet J. Rare Dis. 2016, 11. [Google Scholar] [CrossRef] [Green Version]
- Badu, E. Experiences of parents of children with intellectual disabilities in the Ashanti Region of Ghana. J. Soc. Incl. 2016, 7, 20–30. [Google Scholar] [CrossRef]
- Kimura, M.; Yamazaki, Y. The Lived Experience of Mothers of Multiple Children with Intellectual Disabilities. Qual. Health Res. 2013, 23, 1307–1319. [Google Scholar] [CrossRef] [PubMed]
- Oti-Boadi, M. Exploring the Lived Experiences of Mothers of Children with Intellectual Disability in Ghana. SAGE Open 2017. [Google Scholar] [CrossRef] [Green Version]
- Meirsschaut, M.; Roeyers, H.; Warreyn, P. Parenting in families with a child with autism spectrum disorder and a typically developing child: Mothers’ experiences and cognition. Res. Autism Spectr. Disord. 2010, 4, 661–669. [Google Scholar] [CrossRef] [Green Version]
- Pinquart, M. Do the Parent Child Relationship and Parenting Behaviors Differ Between Families With a Child With and Without Chronic Illness? A Meta-Analysis. J. Pediatr. Psychol. 2013, 38, 708–721. [Google Scholar] [CrossRef] [Green Version]
- Fernández-Alcántara, M.; Correa-Delgado, C.; Muñoz, A.; Salvatierra, M.T.; Fuentes-Hélices, T.; Laynez-Rubio, C. Parenting a Child with a Learning Disability: A Qualitative Approach. Int. J. Disabil. Dev. Educ. 2017, 64, 526–543. [Google Scholar] [CrossRef]
- Thwala, S.K.; Ntinda, K.; Hlanze, B. Lived Experiences of Parents’ of Children with Disabilities in Swaziland. J. Educ. Train. Stud. 2015, 3, 206–215. [Google Scholar] [CrossRef] [Green Version]
- Dyson, L. Unanticipated effects of children with learning disabilities on their families. Learn. Disabil. Q. 2010, 33, 43–55. [Google Scholar] [CrossRef]
- Gallagher, S.; Phillips, A.C.; Oliver, C.; Carroll, D. Predictors of psychological morbidity in parents of children with intellectual disabilities. J. Paediatr. Psychol. 2008, 33, 29–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mori, Y.; Downs, J.; Wong, K.; Anderson, B.; Epstein, A.; Leonard, H. Impacts of caring for a child with the CDKL5 disorder on parental wellbeing and family quality of life. Orphanet J. Rare Dis. 2017, 12, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Poley, M.J.; Brouwer, W.B.F.; Job, N.; van Exel, A.; Tibboel, D. Assessing health related quality of life changes in informal caregivers: An evaluation in parents of children with major congenital anomalies. Qual. Life. Res. 2012, 21, 849–861. [Google Scholar] [CrossRef] [Green Version]
- Wittenberg, E.; Prosse, L.A. Disutility of illness for caregivers and families: A systematic review of the literature. Pharmacoeconomics 2013, 31, 489–500. [Google Scholar] [CrossRef] [Green Version]
- The World Health Organization Quality of Life assessment (WHOQOL). Position paper from the World Health Organization. Soc. Sci. Med. 1995, 41, 1403–1409. [Google Scholar] [CrossRef]
- Hoffman, L.; Marquis, J.; Poston, D.; Summers, A.J.; Turnbull, A. Assessing family outcomes: Psychometric evaluation of the beach center family quality of life scale. J. Marriage Fam. 2006, 68, 1069–1083. [Google Scholar] [CrossRef]
- Ha, J.H.; Hong, J.; Seltzer, M.M.; Greenberg, J.S. Age and gender differences in the well-being of midlife and aging parents with children with mental health or developmental problems: Report of a national study. J. Health Soc. Behav. 2008, 49, 301–316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hernández, V.A.; Calixto, B.; Aguilar, E. Aspectos psicológicos de familiares de personas con diagnosticadas con Trastorno del Espectro Autista. Rev. Intercont. de Psicol. y Educ. 2012, 14, 73–90. Available online: https://www.redalyc.org/articulo.oa?id=80224034005 (accessed on 15 December 2019).
- Mugno, D.; Ruta, L.; Genitori, V.; Mazzone, L. Impairment of quality of life in parents of children and adolescents with pervasive developmental disorder. Health Qual. Life Outcomes 2007, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoong, A.; Koritsas, S. The impact of caring for adults with intellectual disability on the quality of life of parents. J. Intellect. Disabil. Res. 2012, 56, 609–619. [Google Scholar] [CrossRef] [PubMed]
- Buys, L.; Boulton-Lewis, G.; Tedman-Jones, J.; Edwards, H.; Knox, M.; Bigby, C. Issues of active ageing: Perceptions of older people with life long intellectual disability. Australas. J. Ageing 2008, 27, 67–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Flick, U. Introducción a la Investigación Cualitativa; Ediciones Morata: Madrid, Spain, 2007. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Publications: Washington, DC, USA, 2014. [Google Scholar]
- The World Health Organization. International Classification of Functioning, Disability and Health; WHO: Geneva, Switzerland, 2001. [Google Scholar]
- Audiotranskription. Software f4 for Transcription. 2019. Available online: https://www.audiotranskription.de/english/f4 (accessed on 12 September 2019).
- Arbeláez, M.; Onrubia, J. Análisis bibliométrico y de contenido. Dos metodologías complementarias para el análisis de la revista colombiana Educación y Cultura. Rev. de Investig. UCM 2014, 14, 14–31. [Google Scholar] [CrossRef] [Green Version]
- Elo, S.; Kaariainen, M.; Kanste, O.; Polkki, T.; Utriainen, K.; Kyngas, H. Qualitative content analysis: A focus on trustworthiness. SAGE Open. 2014, 4. [Google Scholar] [CrossRef]
- Lincoln, Y.S.; Guba, E.G. Naturalistic Inquiry; Sage Publications: Newbury Park, CA, USA, 1985. [Google Scholar]
- Brewer, D. Ethnography, Buckingham; Open University Press: Philadelphia, PA, USA, 2000. [Google Scholar]
- Howitt, D. Introduction to Qualitative Methods in Psychology; Pearson: London, UK, 2013. [Google Scholar]
- Scientific Software Development. Atlas. ti Scientific Software. 2019. Available online: http://www.atlasti.com/es (accessed on 18 September 2019).
- Park, J.; Hoffman, L.; Marquis, J.; Turnbull, A.P.; Poston, D.; Mannan, H.; Wang, M.; Nelson, L.L. Toward Assessing Family Outcomes of Service Delivery: Validation of a Family Quality of Life Survey. J. Intellect. Disabil Res. 2003, 47, 367–384. [Google Scholar] [CrossRef] [Green Version]
- Beach Center on Disability at the University of Kansas. Family Quality of Life Survey; Beach Center on Disability, University of Kansas: Lawrence, KS, USA, 2001. [Google Scholar]
- Lamb, A.E.; Biesecker, B.B.; Umstead, K.L.; Muratori, M.; Biesecker, L.G.; Erby, L.H. Family Functioning Mediates Adaptation in Caregivers of Individuals with Rett Syndrome. Patient Educ. Couns. 2016, 99, 1873–1879. [Google Scholar] [CrossRef] [Green Version]
- Luijkx, J.; van der Putten, A.A.J.; Vlaskamp, C. “I love my sister, but sometimes I don’t”: A qualitative study into the experiences of siblings of a child with profound intellectual and multiple disabilities. J. Intellect. Dev. Disabil. 2016, 41, 279–288. [Google Scholar] [CrossRef] [Green Version]
- Moyson, T.; Roeyers, H. ‘The overall quality of my life as a sibling is all right, but of course, it could always be better’. Quality of life of siblings of children with intellectual disability: The siblings’ perspectives. J. Appl. Res. Intellect. Disabil. 2011, 56, 87–101. [Google Scholar] [CrossRef] [PubMed]
- Rossetti, Z.; Hall, S. Adult Sibling Relationships with Brothers and Sisters With Severe Disabilities. Res. Pract. Pers. Sev. Disabil. 2015, 40, 120–137. [Google Scholar] [CrossRef]
- Skotko, B.G.; Levine, S.P.; Goldstein, R. Having a brother or sister with Down syndrome: Perspectives from siblings. Am. J. Med. Genet. A 2011, 155, 2348–2359. [Google Scholar] [CrossRef] [Green Version]
- Heiman, T. Parents of children with disabilities: Resilience, coping, and future expectations. J. Dev. Phys. Disabil. 2002, 14, 159–171. [Google Scholar] [CrossRef]
- Marchal, J.P.; Maurice-Stam, H.; van Trotsenburg, P.; Grootenhuis, A. Mothers and fathers of Young Dutch adolescents with Down syndrome: Health related quality of life and family functioning. Res. Dev. Disabil. 2016, 59, 359–369. [Google Scholar] [CrossRef]
- De Graaf, I.; Speetjens, P.; Smit, F.; De Wolff, M.; Tavecchio, L. Effectiveness of the Triple P Positive Parenting Program on Parenting: A Meta-Analysis. Behav. Modif. 2008, 32, 714–735. [Google Scholar] [CrossRef]
- Yamaoka, Y.; Tamiya, N.; Izumida, N.; Kawamura, A.; Takahashi, H.; Noguchi, H. The relationship between raising a child with a disability and the mental health of mothers compared to raising a child without disability in japan. SSM Popul. Health 2016, 2, 542–548. [Google Scholar] [CrossRef] [Green Version]
- Oñate, L.; Calvete, E. Una aproximación cualitativa a los factores de resiliencia en familiares de personas con discapacidad intelectual en España. Interv. Psicosoc. 2017, 26, 93–101. [Google Scholar] [CrossRef] [Green Version]
- Santos, M.A.; Pereira-Martins, M.L. Coping strategies adopted by parents of children with intellectual disabilities. Cien. Saude Colet. 2016, 21, 3233–3244. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.W.; Greenberg, J.S.; Seltzer, M.M.; Krauss, M.W. The role of coping in maintaining the psychological well-being of mothers of adults with intellectual disability and mental illness. J. Intellect. Disabil. Res. 2003, 47, 313–327. [Google Scholar] [CrossRef] [PubMed]
- Piazza, V.E.; Floyd, F.J.; Mailick, M.R.; Greenberg, J.S. Coping and psychological health of aging parents of adult children with developmental disabilities. Am. J. Intellect. Dev. Disabil. 2014, 119, 186–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brehaut, J.C.; Garner, R.E.; Miller, A.R.; Lach, L.M.; Klassen, A.F.; Rosenbaum, P.; Kohen, D.E. Changes Over Time in the Health of Caregivers of Children With Health Problems: Growth-Curve Findings From a 10-Year Canadian Population-Based Study. Am. J. Public Health 2011, 101, 2308–2316. [Google Scholar] [CrossRef] [PubMed]
- Eisenhower, A.S.; Baker, B.L.; Blacher, J. Children’s delayed development and behavior problems: Impact on mothers’ perceived physical health across early childhood. Soc. Sci. Med. 2008, 68, 89–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, A.M.; Grzywacz, J. Health and Well-being in Midlife Parents of Children with Special Health Needs. Fam. Syst. Health 2014, 3, 303–312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuhaneck, H.M.; Burroughs, T.; Wrigth, J.; Lemanczyk, T.; Rowntree, D. A qualitative Study of Coping in Mothers of Children with an Autism Spectrum Disorder. Phys. Occup. Ther. Pediatr. 2010, 30, 340–350. [Google Scholar] [CrossRef]
- Mactavish, J.B.; MacKay, K.J.; Iwasaki, Y.; Betteridge, D. Family caregivers of individuals with intellectual disability: Perspectives on life quality and the role of vacations. J. Leis. Res. 2007, 39, 127–155. [Google Scholar] [CrossRef]
- Taanila, A.; Syrjälä, L.; Kokkonen, J.; Järvelin, M.R. Coping of parents with physically and/or intellectually disabled children. Child Care Health Dev. 2002, 28, 73–86. [Google Scholar] [CrossRef]
- Coughlin, M.B.; Sethares, K.A. Chronic sorrow in parents of children with a chronic illness or disability: An integrative literature review. J. Pediatr. Nurs. 2017, 37, 108–116. [Google Scholar] [CrossRef]
- Sheehan, P.; Guerin, S. Exploring the range of emotional response experienced when parenting a child with an intellectual disability: The role of dual process. Br. J. Learn. Disabil. 2018, 46, 109–117. [Google Scholar] [CrossRef]
- Stroebe, M.; Schut, H. Overload: A missing link in the dual process model? OMEGA 2016, 74, 96–109. [Google Scholar] [CrossRef]
- Stroebe, M.; Schut, H.; Boerner, K. Models of coping with bereavement: An updated overview. Stud. Psychol. 2017, 38, 582–607. [Google Scholar] [CrossRef]
- Fernández-Alcántara, M.; García-Caro, M.P.; Berrocal-Castellano, M.; Benítez, A.; Robles-Vizcaíno, C.; Laynez-Rubio, C. Experiences and changes in parents of children with infant cerebral palsy: A qualitative study. An. Sist. Sanit. Navar. 2013, 36, 9–20. [Google Scholar] [CrossRef] [Green Version]
- Griffith, G.M.; Totsika, V.; Nash, S.; Jones, R.S.P.; Hastings, R.P. “We are all there silently coping”. The hidden experiences of parents of adults with Asperger syndrome. J. Intellect. Dev. Disabil. 2012, 37, 237–247. [Google Scholar] [CrossRef]
- Heiman, T.; Berger, O. Parents of children with Asperger syndrome or with learning disabilities: Family environment and social support. Res. Dev. Disabil. 2008, 29, 289–300. [Google Scholar] [CrossRef]
- Taggart, L.; Truesdale-Kennedy, M.; Ryan, A.; McConkey, R. Examining the support needs of ageing family careers in developing future plans for a relative with an intellectual disability. J. Intellect. Disabil. 2012, 16. [Google Scholar] [CrossRef] [PubMed]
- Beighton, C.; Wills, J. Are parents identifying positive aspects to parenting their child with an intellectual disability or are they just coping? A qualitative exploration. J. Intellect. Disabil. 2017, 21, 325–345. [Google Scholar] [CrossRef] [Green Version]
- Beighton, C.; Wills, J. How parents describe the positive aspects of parenting their child who has intellectual disabilities: A systematic review and narrative synthesis. J. Appl. Res. Intellect. Disabil. 2019. [Google Scholar] [CrossRef] [Green Version]
- Blackledge, J.T.; Hayes, S.C. Using acceptance and commitment training in the support of parents of children diagnosed with autism. Child Fam. Behav. Ther. 2006, 28, 1–18. [Google Scholar] [CrossRef]
- Masulani-Mwalea, C.; Mathanga, D.; Kauye, F.; Gladstone, M. Psychosocial interventions for parents of children with intellectual disabilities–A narrative review and implications for low income settings. Ment. Health Prev. 2018, 11, 24–32. [Google Scholar] [CrossRef]
- Alsem, M.W.; Ausems, F.; Verhoef, M.; Jongmans, M.J.; Meily-Visser, J.M.A.; Ketelaar, M. Information seeking by parents of children with physical disabilities: An exploratory qualitative study. Res. Dev. Disabil. 2017, 60, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Dzamonja-Ignjatovica, T.; Milanovicb, M.; Zegaraca, N. How services for children with disabilities in Serbia affect the quality of life of their families. Res. Dev. Disabil. 2017, 68, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kuhlthau, K.; Hill, K.S.; Yucel, R.; Perris, J. Financial Burden for Families of Children with Special Health Care Needs. Matern. Child Health J. 2005, 9, 207–218. [Google Scholar] [CrossRef]
- Emerson, E.; Hatton, C. The socio-economic circumstances of children at risk of disability in Britain. Disabil. Soc. 2007, 22, 563–580. [Google Scholar] [CrossRef]
- Mohan, R.; Kulkarni, M. Resilience in Parents of Children with Intellectual Disabilities. Psychol. Dev. Soc. J. 2018, 30, 19–43. [Google Scholar] [CrossRef]
- Lawoko, S.; Soares, J. Quality of life among parents of children with congenital heart disease, parents of children with other diseases and parents of healthy children. Qual. Life Res. 2003, 12, 655–666. [Google Scholar] [CrossRef]
- Park, J.; Turnbull, A.P.; Turnbull, H.R. Impacts of Poverty on Quality of Life in Families of Children with Disabilities. Except. Child. 2002, 68. [Google Scholar] [CrossRef]
- Boehm, T.L.; Carter, E.W.; Taylor, J.L. Family Quality of Life during the Transition to Adulthood for Individuals with Intellectual Disability and/or Autism Spectrum Disorders. Am. J. Intellect. Dev. Disabil. 2015, 120, 395–411. [Google Scholar] [CrossRef]
- Chadwick, D.D.; Mannan, H.; Garcia-Iriarte, E.; McConkey, R.; O’brien, P.; Finlay, F.; Lawlor, A.; Harrington, G. Family voices: Life for family careers of people with intellectual disabilities in Ireland. J. Appl. Res. Intellect. Disabil. 2013, 26, 119–132. [Google Scholar] [CrossRef]
- Ekas, N.V.; Lickenbrock, D.M.; Whitman, T.L. Optimism, social support, and well-being in mothers of children with autism spectrum disorder. J. Autism Dev. Disord. 2010, 40, 1274–1284. [Google Scholar] [CrossRef]
- Perera, B.D.; Standen, P.J. Exploring coping strategies of careers looking after people with intellectual disabilities and dementia. Adv. Ment. Health Intellect. Disabil. 2014, 8, 292–301. [Google Scholar] [CrossRef]
- Slattery, E.; McMahon, J.; Gallagher, S. Optimism and benefit finding in parents of children with developmental disabilities: The role of positive reappraisal and social support. Res. Dev. Disabil. 2017, 65, 12–22. [Google Scholar] [CrossRef]
- Daly, L.; Sharek, D.; DeVries, J.; Griffiths, C. The impact of four family support programs for people with a disability in Ireland. J. Intellect. Disabil. 2015, 19, 34–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dew, A.; Collings, S.; Dowse, L.; Meltzer, A.; Smith, L. ‘I don’t feel like I’m in this on my own’: Peer support for mothers of children with intellectual disability and challenging behaviour. J. Intellect. Disabil. 2019, 23, 344–358. [Google Scholar] [CrossRef] [PubMed]
- Bray, L.; Carter, B.; Sanders, C.; Blake, L.; Keegan, K. Parent-to-parent peer support for parents of children with a disability: A mixed method study. Patient Educ. Couns. 2017, 100, 1537–1543. [Google Scholar] [CrossRef] [PubMed]
- García-Iriarte, E.; McConkey, R.; Vilda, D. Family experiences of personalised accommodation and support for people with intellectual disability. J. Intellect. Disabil. 2020. [Google Scholar] [CrossRef]


{kind=link}
| Participant | Sex | Age | Kinship | Educational Level | Occupation | Marital Status | Offspring Sex-Age | Timing of Diagnosis | Degree of ID | Number of Additional Children | Residence |
|---|---|---|---|---|---|---|---|---|---|---|---|
| I 01 | Female | 71 | Mother | Primary | Homemaker | Married | F-39 | Post-Birth (2 years) | 86% | 1 | Family |
| I 02 | Female | 59 | Mother | Primary | Homemaker | Married | F-27 | Post-Birth (2 years) | 84% | 0 | Residence |
| I 03 | Male | 69 | Father | Primary | Retired | Married | M-37 | Birth | 99% | 0 | Family |
| I 04 | Female | 83 | Mother | Primary | Homemaker | Married | M-40 | Birth | 79% | 0 | Residence |
| I 05 | Female | 71 | Mother | Primary | Homemaker | Widow | F-31 | Post-Birth (3 years) | 65% | 0 | Family |
| I 06 | Female | 63 | Mother | Primary | Homemaker | Married | F-36 | Post-Birth (10 years) | 70% | 1 | Family |
| I 07 | Female | 66 | Mother | Primary | Retired | Married | F-32 | Post-Birth (10 years) | 75% | 0 | Family |
| I 08 | Female | 54 | Mother | University | Homemaker | Married | M-18 | Post-Birth (4 years) | 48% | 0 | Family |
| I 09 | Male | 53 | Father | Secondary | Unemployed | Married | M-18 | Post-Birth (5 years) | 48% | 0 | Family |
| I 10 | Female | 56 | Mother | Primary | Employed | Married | M-31 | Birth | 75% | 1 | Family |
| I 11 | Male | 67 | Father | Secondary | Retired | Married | M-39 | Birth | 98% | 0 | Residence |
| I 12 | Female | 62 | Mother | University | Homemaker | Married | M-39 | Birth | 98% | 0 | Residence |
| I 13 | Male | 72 | Father | Secondary | Retired | Married | F-39 | Post-Birth (3 years) | 86% | 1 | Family |
| I 14 | Female | 65 | Mother | Secondary | Freelance | Married | F-36 | Post-Birth (2 years) | 33% | 0 | Family |
| I 15 | Male | 64 | Father | University | Retired | Married | M-27 | Post-Birth (13 years) | 75% | 1 | Family |
| I 16 | Female | 56 | Mother | University | Unemployed | Married | M-28 | Post-Birth (11 years) | 36% | 1 | Family |
| When did you or another family member begin to notice that something was happening to your child? What did you perceive as different in your child’s development? Why? |
| How did you feel at the time of the diagnosis? What thoughts did you have as you tried to understand that diagnosis? What did you do about it? |
| Where did you encounter the most difficulty in raising your child? Why? |
| Do you feel that your general health and well-being has worsened in recent years compared to the time of diagnosis? Why? |
| Which changes occurred in your family dynamics in the moment of diagnosis on a social, economic/work, and leisure level and as a couple or with the child’s other siblings or relatives? Have these changes been maintained in the adult stage of your children? |
| What is your child’s relationship with his/her other siblings like? |
| How much time do you spend on yourself every week? What do you do in that free time? |
| Do you have family or close people (neighbors and friends) who currently help you? Did you have this support at the time of the diagnosis? |
| What do you think about the care your child receives from the health system? |
| What support have the different care associations provided you? |
| What are your main concerns about your child? |
| What did you previously think about your child’s future and how do you imagine it now? |
| What aspects of your life and that of your child do you think could be improved? |
| Changes Produced after the Diagnosis | Interpersonal Relationships | Physical and Emotional Well-Being as a Caregiver | Concerns about the Future |
|---|---|---|---|
| Changing residence/home | Little family support | Poorer physical health | Child’s place of residence |
| Adequacy of the home for the child with ID | Social distancing | Anxiety/worry | Economic expenses and employment |
| Abandonment of the carer’s job | Problems with partner | Lack of self-care and enjoyment | Physical health status of the child |
| Economic difficulties | Feeling of sorrow/grief | Having family and social support | |
| Relationship with the siblings of the child with ID | Positive aspects | Happiness of the child |
| Codes | Quotes |
|---|---|
| Worse physical health | “In the middle of the night I have to get up 3 or 4 times to change him. Nights where I don’t sleep, nights where I sleep for the first 3 or 4 h and that’s it, or he/she starts to make noise, I can’t get back to sleep” (I03 Father). |
| Anxiety | “It’s a huge suffering when he gets sick, I tremble when he gets sick. I don’t want anything to hurt him, so he doesn’t get worse, he doesn’t suffer, and that worries me a lot…” (I12 Mother). “For some time now I’ve had anxiety attacks, in fact, they were affecting my heart, I have heart problems, I take drugs for that. The anxiety is because of the fear that something will happen to him, that his health will deteriorate, that he will not have any friends…” (I16 Mother). |
| Lack of self-care and enjoyment | “Before we had friends, but not anymore. It’s not the same to have one child to having three, and to have a child with difficulties… because that means that you can’t do the same as you did before. Also, if nobody helps you... I couldn’t go out much before, nor now...” (I06 Mother). “When you go with these children to places where families with children who are okay go, they don’t accept them. So, because they are not accepted, you pull back and make your own life, you end up alone without having any time for yourself or the marriage...” (I04 Mother). |
| Feeling of sorrow/grief | “Well, the truth is that the mood is sadder because of the care, yes... We’re not going to say no... [But,] physically, no, because the truth is that she’s truly autonomous... on a physical level it hasn’t affected me...” (I02 Mother). “They’re never entirely accepted. There you have your thorn... The thorn that could’ve been more independent, more autonomous. Within a normality, I would like it to be like that, but it’s not. What can I do? It’s not like that. I feel sorrow and sadness because I’m not like I used to be, as I remember being, or how I remember my brother or my friend were” (I09 Father). |
| Positive aspects | “My sisters say that I’m getting better with her every day, they say ‘she’s helped you to live’, and I believe it might be true because I don’t stop, I’m more active” (I05 Mother). “My son, within the limits of his disability, has changed everything for the better, the experience has been hard, but his love is very enriching without a doubt” (I11 Father), |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-Ávalos, M.I.; Pérez-Marfil, M.N.; Ferrer-Cascales, R.; Cruz-Quintana, F.; Clement-Carbonell, V.; Fernández-Alcántara, M. Quality of Life and Concerns in Parent Caregivers of Adult Children Diagnosed with Intellectual Disability: A Qualitative Study. Int. J. Environ. Res. Public Health 2020, 17, 8690. https://doi.org/10.3390/ijerph17228690
Fernández-Ávalos MI, Pérez-Marfil MN, Ferrer-Cascales R, Cruz-Quintana F, Clement-Carbonell V, Fernández-Alcántara M. Quality of Life and Concerns in Parent Caregivers of Adult Children Diagnosed with Intellectual Disability: A Qualitative Study. International Journal of Environmental Research and Public Health. 2020; 17(22):8690. https://doi.org/10.3390/ijerph17228690
Chicago/Turabian StyleFernández-Ávalos, María Inmaculada, María Nieves Pérez-Marfil, Rosario Ferrer-Cascales, Francisco Cruz-Quintana, Violeta Clement-Carbonell, and Manuel Fernández-Alcántara. 2020. "Quality of Life and Concerns in Parent Caregivers of Adult Children Diagnosed with Intellectual Disability: A Qualitative Study" International Journal of Environmental Research and Public Health 17, no. 22: 8690. https://doi.org/10.3390/ijerph17228690