UK Research Priorities for Electronic Cigarettes: A James Lind Alliance Priority Setting Partnership


Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Considerations
2.2. Initiation
2.3. Consultation
2.4. Collation
2.5. Prioritisation
3. Results
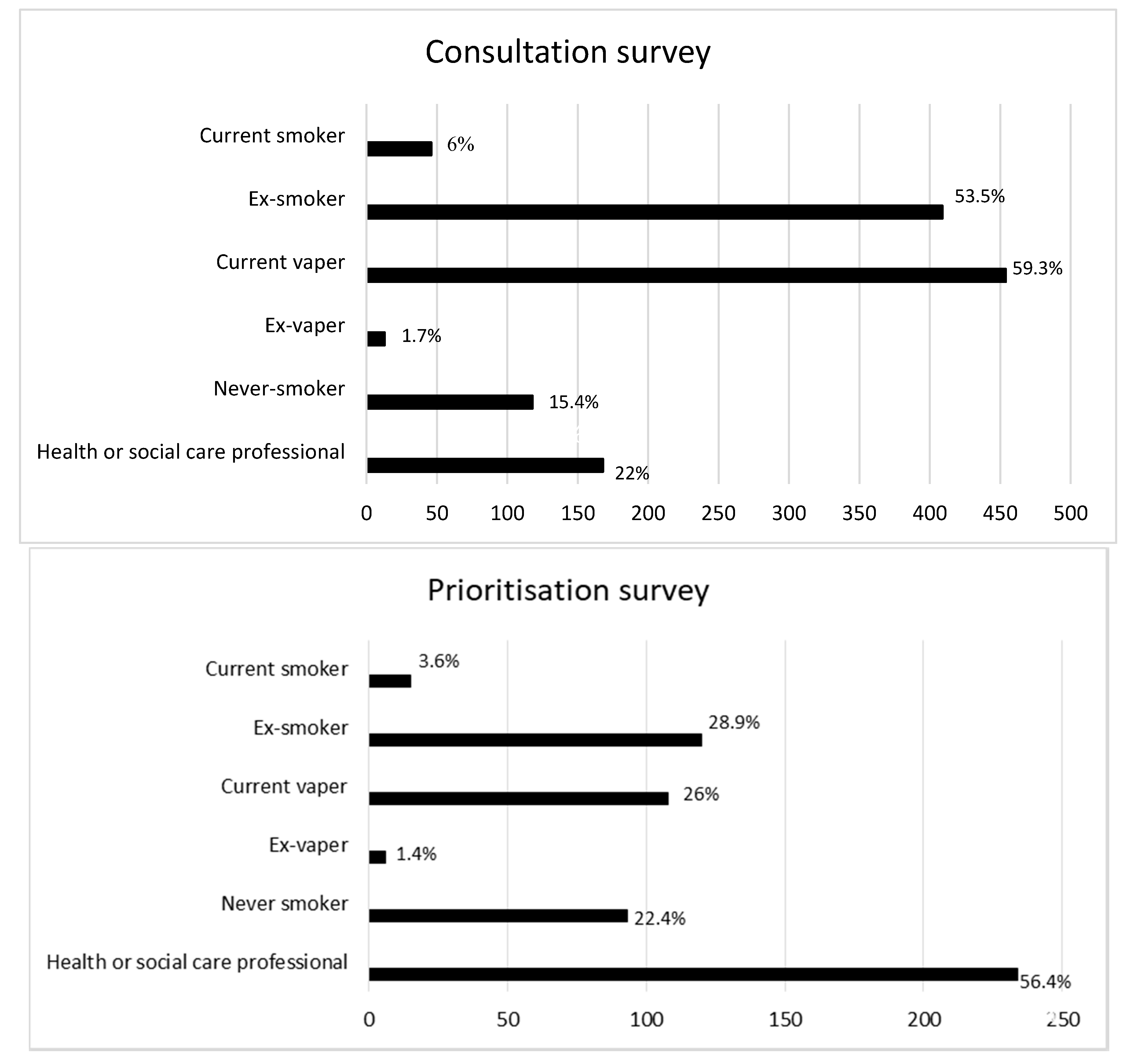
3.1. Consultation and Collation Stage
3.2. Prioritisation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Office for National Statistics. Adult Smoking Habits in the UK: 2019. 2020. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/healthandlifeexpectancies/bulletins/adultsmokinghabitsingreatbritain/2019 (accessed on 8 September 2020).
- West, R.; Bear, E.; Brown, J. Trends in Electronic Cigarette Use in England; University College London, Smoking Toolkit Study: London, UK, 2006. [Google Scholar]
- Action on Smoking and Health (ASH). Use of e-Cigarettes (Vaporisers) Among Adults in Great Britain. 2019. Available online: https://ash.org.uk/wp-content/uploads/2019/09/Use-of-e-cigarettes-among-adults-2019.pdf (accessed on 8 September 2020).
- Chalmers, I.; Glasziou, P. Avoidable waste in the production and reporting of research evidence. Lancet 2009, 374, 86–89. [Google Scholar] [CrossRef]
- Cowan, K. The James Lind alliance: Tackling treatment uncertainties together. J. Ambul. Care Manag. 2010, 33, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Lindson, N.; Richards-Doran, D.; Heath, L.; Hartmann-Boyce, J. Setting research priorities in tobacco control: A stakeholder engagement project. Addiction 2017, 112, 2257–2271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- James Lind Alliance Guidebook (Version 8); James Lind Alliance: Southampton, UK, 2018; Available online: http://www.JLAguidebook.org (accessed on 8 September 2020).
- James Lind Alliance. Electronic Cigarettes. Available online: http://www.jla.nihr.ac.uk/priority-setting-partnerships/Electronic-cigarettes/ (accessed on 8 September 2020).
- Kanchustambham, V.; Saladi, S.; Rodrigues, J.; Fernandes, H.; Patolia, S.; Santosh, S. The knowledge, concerns and healthcare practices among physicians regarding electronic cigarettes. J. Community Hosp. 2017, 7, 144–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stepney, M.; Aveyard, P.; Begh, R. GPs’ and Nurses’ Perceptions of Electronic Cigarettes in England: A qualitative interview study. Br. J. Gen. Pract. 2019, 69, e8–e14. [Google Scholar] [CrossRef] [PubMed]
- Van Gucht, D.; Baeyens, F. Health professionals in Flanders perceive the potential health risks of vaping as lower than those of smoking but do not recommend using e-cigarettes to their smoking patients. Harm Reduct. 2016, 13, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mann, R.; Faflik, F. Survey of smoking cessation services and pregnant women’s views on use of electronic cigarettes in pregnancy. J. Health Visit 2018, 6, 32–39. [Google Scholar] [CrossRef]
- Ahmed, Z.; Preshaw, P.M.; Bauld, L.; Holliday, R. Dental professionals’ opinions and knowledge of smoking cessation and electronic cigarettes: A cross-sectional survey in the north of England. Br. Dent. J. 2018, 225, 947. [Google Scholar] [CrossRef] [PubMed]
- Cancer Research UK: E-cigarettes–Answering the Burning Questions. 2015. Available online: https://scienceblog.cancerresearchuk.org/2015/08/11/e-cigarettes-answering-the-burning-questions/?_ga=2.49956774.144173359.1576682219-1468954628.1576682219 (accessed on 8 September 2020).
- Kaisar, M.A.; Prasad, S.; Liles, T.; Cucullo, L. A decade of e-cigarettes: Limited research & unresolved safety concerns. Toxicology 2016, 365, 67–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cancer Research UK. Does Vaping Cause Popcorn Lung. Available online: https://www.cancerresearchuk.org/about-cancer/causes-of-cancer/cancer-controversies/does-vaping-cause-popcorn-lung (accessed on 8 September 2020).
- Greener, M. E-Cigarettes: Making Healthcare Professionals Myth Busters. Prescriber 2018, 29, 20–24. [Google Scholar] [CrossRef] [Green Version]
- Staley, K.; Crowe, S. More Than a Top 10: How James Lind Alliance Priority Setting Partnerships Transform Research, People and Organisations; NIHR Oxford Biomedical Research Centre: Oxford, UK, 2019. [Google Scholar]


{kind=link}
| Question | Both | HCP | Non-HCP | |
|---|---|---|---|---|
| 1 | What are the long-term effects of vaping? Compared to smoking, ex-smokers, never-smokers and NRT use? | ✓ | ||
| 2 | What are the short-term effects of vaping? Compared to smoking, ex-smokers, never-smokers and NRT use? | ✓ | ||
| 3 | How do e-cigarettes compare to other treatments for stopping smoking, in terms of effectiveness, cost-effectiveness, long-term abstinence, and relapse to smoking? | ✓ | ||
| 4 | How effective are e-cigarettes for smoking cessation in patients with mental health problems? And what effect do they have on mental health? | ✓ | ||
| 5 | How safe are e-cigarettes in pregnancy, compared to smoking and NRT use? | ✓ | ||
| 6 | What effect does vaping in pregnancy (and when breastfeeding) have on the health outcomes of the fetus and baby, compared to smoking? Including any long-term effects. | ✓ | ||
| 7 | How effective are e-cigarettes in pregnancy for smoking cessation? And compared to other treatments? | ✓ | ||
| 8 | Will prescribing e-cigarettes to pregnant smokers encourage smoking cessation, and reduce risk of relapse? | ✓ | ||
| 9 | What effect does second hand vape have on adults (including pregnant women), children and animals, and how does this compare to second hand smoke? | ✓ | ||
| 10 | What are the impacts of vaping on indoor and outdoor air quality, and how does this compare to other air pollutants? | ✓ | ||
| 11 | What impact do restrictions on vaping (e.g., including vaping in smoke free policies; age limits; tank size) have on smoking behaviour and smoking cessation? as well as perceptions of harm from vaping? | ✓ | ||
| 12 | What testing should be done on the flavourings, ingredients and devices to ensure they are safe? | ✓ | ||
| 13 | How addictive are e-cigarettes compared with regular cigarettes? | ✓ | ||
| 14 | What impact do flavourings have on e-cigarette usage, smoking behaviour and health, in adults and children, and smokers and non-smokers? | ✓ | ||
| 15 | What effect do the ingredients, chemicals and flavourings have on health, and how does this differ from cigarettes? | ✓ | ||
| 16 | What are the views of healthcare professionals of e-cigarettes for smoking cessation (including in pregnancy)? And how can we improve knowledge? | ✓ | ||
| 17 | How are e-cigarettes represented in the media? And what impact does this have on public perceptions, attitudes and behaviours? | ✓ | ||
| 18 | How can e-cigarettes be incorporated into a smoking cessation programme or treatment guidelines? How will this differ for different populations? | ✓ | ||
| 19 | Can advice from healthcare professionals lead to better outcomes for smoking cessation if accurate information is provided about e-cigarettes? | ✓ | ||
| 20 | How can hospitals better support patients to stop or reduce their smoking with the use of e-cigarettes? | ✓ | ||
| 21 | What are the barriers and facilitators for e-cigarette use for smoking cessation? What different barriers may exist for those with mental health problems or heavily dependent smokers? | ✓ | ||
| The Top 5 Voted for by the Steering Group from the Next 10 Most Frequent Responses | ||||
| 22 | What are the health effects of vaping for never-smokers and ex-smokers? | |||
| 23 | What is the best way to educate adults and children about vaping, and to provide information about vaping products and device safety (including battery safety)? | |||
| 24 | How can we motivate smokers to try e-cigarettes for smoking cessation? | |||
| 25 | What effect does vaping have on mental health, including any risks and benefits? In adults, children and young people. | |||
| 26 | What are the risks and benefits of nicotine consumption, and/or nicotine cessation? | |||
| Rank | Question |
|---|---|
| 1 | What are the long-term effects of vaping? Compared to smoking, ex-smokers, never-smokers and NRT use? |
| 2 | What effect do the ingredients, chemicals and flavourings have on health, and how does this differ from cigarettes? |
| 3 | What effect does vaping in pregnancy (and when breastfeeding) have on the health outcomes of the foetus and baby, compared to smoking? Including any long-term effects. |
| 4 | How effective are e-cigarettes for smoking cessation in patients with mental health problems? And what effect do they have on mental health? |
| 5 | What are the barriers and facilitators for e-cigarette use for smoking cessation? What different barriers may exist for those with mental health problems or heavily dependent smokers? |
| 6 | How do e-cigarettes compare to other treatments for stopping smoking, in terms of effectiveness, cost-effectiveness, long-term abstinence, and relapse to smoking? |
| 7 | What impact do restrictions on vaping (e.g., including vaping in smoke free policies; age limits; tank size) have on smoking behaviour and smoking cessation? as well as perceptions of harm from vaping? |
| 8 | What testing should be done on the flavourings, ingredients and devices to ensure they are safe? |
| 9 | Will prescribing/providing e-cigarettes to pregnant smokers encourage smoking cessation, and reduce risk of relapse? |
| 10 | What effect does second hand vape have on adults (including pregnant women), children and animals, and how does this compare to second hand smoke? |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hunter, A.; Ross, L.; Gronlund, T.; Cooper, S. UK Research Priorities for Electronic Cigarettes: A James Lind Alliance Priority Setting Partnership. Int. J. Environ. Res. Public Health 2020, 17, 8500. https://doi.org/10.3390/ijerph17228500
Hunter A, Ross L, Gronlund T, Cooper S. UK Research Priorities for Electronic Cigarettes: A James Lind Alliance Priority Setting Partnership. International Journal of Environmental Research and Public Health. 2020; 17(22):8500. https://doi.org/10.3390/ijerph17228500
Chicago/Turabian StyleHunter, Abby, Louise Ross, Toto Gronlund, and Sue Cooper. 2020. "UK Research Priorities for Electronic Cigarettes: A James Lind Alliance Priority Setting Partnership" International Journal of Environmental Research and Public Health 17, no. 22: 8500. https://doi.org/10.3390/ijerph17228500