Comparison of Two Evacuation Shelter Operating Policies and the Role of Public Health Nurses after the Great East Japan Earthquake: A Qualitative Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection and Analysis
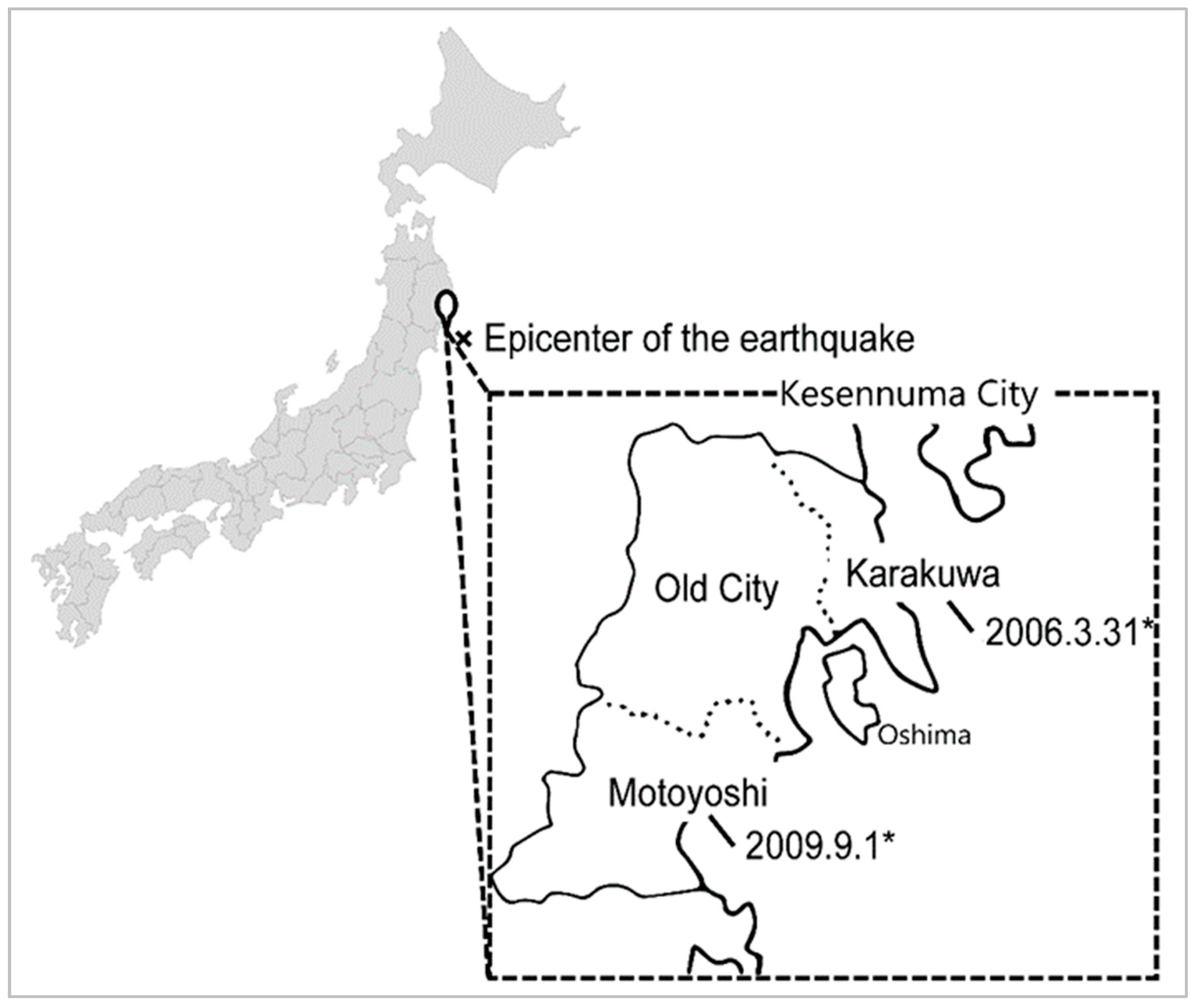
2.2. Damage to Kesennuma Following the Great East Japan Earthquake
3. Results
3.1. Participants and Data Collection
3.2. Analyzed Districts and the Two Shelter Operation Policies
3.3. Description of the Operating Policies Using Four Themes
3.3.1. Theme 1: The Lack of an Operational Preparedness Policy for the Shelters: The Onset of the Disaster
Station Type
- The operating method of each shelter was different. Id 02
- If an operating shelter system had been created, I think, the response to the disaster during March would have been a little better. Id 13
- We were waiting for commands from headquarters without knowing what to do. I don’t remember what time it was, but, at night, the headquarters’ command was for the public health nurses to support the shelters. Id 03
- Everyone gathered in the city office’s large hall... we received a command from headquarters to move to an evacuation shelter. We were told to scatter to each of the evacuation shelters. Id 02
- We wondered, “When we do go out there, what should we do?” Id 01
Patrol Type
- No one can stay in the evacuation shelters. We will move around the shelters with two-person teams,” so I said and we decided. With that, a patrol-type evacuation shelter management style was established. Id 11
- Headquarters was in this large room. The self-defense force, firefighters, the fire brigade, and our desks were gathered on the same floor of this branch. All issues and decision-making procedures were shared with everyone on the floor, helping to understand the priorities in the need for assistance. Id 11
3.3.2. Theme 2: The Provision of Support to the Shelter Residents: Approximately 72 Hours after the Disaster
Station Type
- I couldn’t bring anything for healthcare equipment at all. I managed to contact my parents’ house and bring my parents’ blood pressure monitor. The only medical tool that can be used is the first aid kit provided in the public hall. Id 05
- [When I was reassigned to the shelter the next day] an officer at the headquarters said, “We heard that 70 elderly people who sustained damage from the tsunami are going to the shelter, and it seems that they are still wet. We order you to take these clothes to the shelter. Anyway, please do what you should do while consulting with the nursing home staff.” After that, I did not receive further instructions from headquarters. Id 02
- The men’s clerks at the local government were continually changing. Until the end of March, we were forced to operate an evacuation center. Id 01
- The situation [of the shelter] did not to allow us to work only on health issues. I could deal with hearing the story of a person who came [to the place where we were], and I was able to handle it. However, I couldn’t really go around to each room in the shelter and listen to and assess each person’s health problem. Id 03
- When asked, “Did you really take your blood pressure medication?” most of the residents gave vague answers. I think everybody has been given their own prescription note, but they never read the contents exactly. Id 01
Patrol Type
- [The day after the earthquake] we asked the nurses at the shelter—including midwives, nurses from city hospitals, and teachers at the school for the disabled—to watch the residents at the shelter and contact us if something happened. Id 11
3.3.3. Theme 3: The Autonomy of the Shelter Residents: The Shelters as Places for Daily Life
Station Type
- Since we had to operate the shelter from the beginning, the residents naturally thought that only the administrative officials should operate the evacuation shelter. Id 02
- I am a public health nurse, so I had received various consults from everyone and decided on my own. However, I was very anxious because I wasn’t sure if these decisions were appreciate. I had been alone. Id 06
- When local residents made rice balls for shelters, they were asked if the city could afford to serve vegetable dishes. But my first concern was whether these budgets could be implemented. I can’t argue with anyone, I don’t have the right to allow it. Having to decide alone was a big worry Id 01.
- I had no idea where a colleague in the same department was assigned to the shelter. I didn’t even know that there were 100 shelters in the city until April. Id 03
- I now think that what we had to do was more than manage the evacuation shelters. Certainly, we should have been able to leave the shelter a bit when the medical team arrived. Id 01
- I now think that we should have not felt that a PHN was a member of the shelter as well. The more I stayed in the shelter, the more work I had to do. But we should have acted as members of the local government. Id 01
Patrol Type
- The teams did not act without notifying the chief clerk of the PHNs in the branch office. This did not mean that the branch office approved these teams; they provided systems for sharing information and behaved in a cohesive manner. Id 08
3.3.4. Theme 4: The Relationship with the External PHN Support Teams: The Disaster Recovery Phase
Station Type
- From the day when the teams came, the evacuation shelter changed completely. First, I was not able to talk to each resident individually, so I asked them to conduct health interviews for each resident. Id 07
- Since the supporters were replaced in a week, I had to hear the information from the previous teams and convey it to the new team each time. I had to endlessly repeat this information sharing. Id 14
- With the arrival of support public health nurses from non-disaster areas, we were finally able to return home. Id 02
- Until then, my heart was full dealing with the problems at the shelter. When I returned to being an administrative official temporarily, I became aware that what I had to do was turn from the management of the evacuation shelter to solving the community’s health problems. Id 07
Patrol Type
- Once I explained to the residents about the beginning of the continuous activities of the external support team, I left the shelter and entrusted the management to them. I was able to integrate the information that the branch government had with the new information captured by the support teams; therefore, together, we could discuss what to do next. Id 08
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
| Please Share in Detail What Happened Immediately after the Disaster. |
|---|
| What did you do for the first 72 h after the disaster? |
| What changes occurred after 72 h? |
| Please tell us about your dilemma as a victim and your professional responsibilities. |
| Please share any lessons concerning disaster recovery. |
References
- United States Department of the Interior; United States Geological Survey. 20 Largest Earthquakes in the World. Available online: https://www.usgs.gov/natural-hazards/earthquake-hazards/science/20-largest-earthquakes-world?qt-science_center_objects=0#qt-science_center_objects (accessed on 9 September 2020).
- Emergency Agency Security Headquarters, National Police Agency. Police Measures and Damage Situation of the 2011 of the Pacific Coast of Tohoku Earthquake (In Japanese). Available online: https://www.npa.go.jp/news/other/earthquake2011/pdf/higaijokyo.pdf (accessed on 9 September 2020).
- Klein, K.R.; Pepe, P.E.; Burkle, F.M., Jr.; Nagel, N.E.; Swienton, R.E. Evolving need for alternative triage management in public health emergencies: A Hurricane Katrina case study. Disaster Med. Public Health Prep. 2008, 2 (Suppl. 1), S40–S44. [Google Scholar] [CrossRef] [PubMed]
- Bradly, N.; Meara, J.; Murray, V. Principles of public health emergency response for acute environmental, chemical, and rediation incidents. In Oxford Textbook of Global Public Health, 6th ed.; Detels, R., Gulliford, M., Karim, Q.A., Tan, C.C., Eds.; Oxford University Press: Oxford, UK, 2017; pp. 1608–1620. ISBN 978-0198810131. [Google Scholar]
- Burkle, F.M. Complex Public Health Emergencies. In Koenig and Schultz’s Disaster Medicine: Comprehensive Principles and Practices; Koenig, K.L.S.C., Ed.; Cambridge University Press: Cambridge, UK, 2009; pp. 361–376. ISBN 978-1107040755. [Google Scholar]
- FEMA. We Are FEMA. Available online: https://www.fema.gov/about/we-are-fema (accessed on 9 September 2020).
- Civil Contingencies Secretariat. The Lead Government Department and Its Role—Guidance and Best Practice. 2004. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/207227/the_lead_Government_department_and_its_role_-_guidance_and_best_practice.pdf (accessed on 9 September 2020).
- Swedish Civil Contingencies Agency. Swedish Civil Contingencies Agency. Available online: https://www.msb.se/en/ (accessed on 9 September 2020).
- European Commission. European Civil Protection and Humanitarian AID Operations: Resceu. Available online: https://ec.europa.eu/echo/what/civil-protection/resceu_en (accessed on 30 October 2020).
- Dipartimento Della Protezione Civile. Civil Protection Department. Available online: http://www.protezionecivile.gov.it/home (accessed on 9 September 2020).
- Federal Office of Civil Protection and Disaster Assistance. Federal Office of Civil Protection and Disaster Assistance (BBK). Available online: https://www.bbk.bund.de/EN/Home/home_node.html (accessed on 30 October 2020).
- Cabinet Office Japan. Disaster Management in Japan. Available online: http://www.bousai.go.jp/taisaku/soshiki2/soshiki2.html (accessed on 9 September 2020).
- Los Angeles County Department of Public Health. Collaborative Effort. Prepare, Respond and Recover. Available online: http://www.laresilience.org/#:~:text=The%20Los%20Angeles%20County%20Community,such%20as%20pandemics%20and%20disasters (accessed on 9 September 2020).
- OECD. Italian System for the Mobilisation of Volunteers in Civil Protection. Available online: https://www.oecd.org/governance/toolkit-on-risk-governance/goodpractices/page/italiansystemforthemobilisationofvolunteersincivilprotection.htm#tab_description (accessed on 9 September 2020).
- UNDRR. What Is the Sendai Framework for Disaster Risk Reduction? Available online: https://www.undrr.org/implementing-sendai-framework/what-sf (accessed on 9 September 2020).
- Tiepolo, M.; Braccio, S. Mainstreaming Disaster Risk Reduction into Local Development Plans for Rural Tropical Africa: A Systematic Assessment. Sustainability 2020, 12, 2196. [Google Scholar] [CrossRef] [Green Version]
- González-Riancho, P.; Gerkensmeier, B.; Ratter, B.M.W. Storm surge resilience and the Sendai Framework: Risk perception, intention to prepare and enhanced collaboration along the German North Sea coast. Ocean Coast. Manag. 2017, 141, 118–131. [Google Scholar] [CrossRef]
- Godsoe, M.; Ladd, M.; Cox, R. Assessing Canada’s disaster baselines and projections under the Sendai Framework for Disaster Risk Reduction: A modeling tool to track progress. Nat. Hazards 2019, 98, 293–317. [Google Scholar] [CrossRef]
- Chan, E.Y.Y.; Murray, V. What are the health research needs for the Sendai Framework? Lancet 2017, 390, e35–e36. [Google Scholar] [CrossRef]
- Kayano, R.; Chan, E.Y.; Murray, V.; Abrahams, J.; Barber, S.L. WHO Thematic Platform for Health Emergency and Disaster Risk Management Research Network (TPRN): Report of the Kobe Expert Meeting. Int. J. Environ. Res. Public Health 2019, 16, 1232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jensen, J.; Thompson, S. The Incident Command System: A literature review. Disasters 2016, 40, 158–182. [Google Scholar] [CrossRef]
- Australian Institute for Disaster Resilience. Handbook 4—Evacuation Planning. In Austrarian Disaster Resilience Handbook Collection; Australian Institute for Disaster Resilience: Melbourne, Australia, 2017. [Google Scholar]
- Cabinet Office. Evacuation and Shelter Guidance-Non-Statutory Guidance to Complement Emergency Preparedness and Emergency Response and Recovery. 2013. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/274615/Evacuation_and_Shelter_Guidance_2014.pdf (accessed on 3 September 2020).
- Goniewicz, K.; Burkle, F.M. Disaster Early Warning Systems: The Potential Role and Limitations of Emerging Text and Data Messaging Mitigation Capabilities. Disaster Med. Public Health Prep. 2019, 13, 709–712. [Google Scholar] [CrossRef]
- Goniewicz, K.; Burkle, F.M., Jr. Challenges in Implementing Sendai Framework for Disaster Risk Reduction in Poland. Int. J. Environ. Res. Public Health 2019, 16, 2574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veenema, T.G.; Rains, A.B.; Casey-Lockyer, M.; Springer, J.; Kowal, M. Quality of healthcare services provided in disaster shelters: An integrative literature review. Int. Emerg. Nurs. 2015, 23, 225–231. [Google Scholar] [CrossRef] [PubMed]
- The Sphere Project. The Sphere Handbook 2018. Available online: https://handbook.spherestandards.org/en/sphere/#ch001 (accessed on 9 September 2020).
- Schilderman, T. Adapting traditional shelter for disaster mitigation and reconstruction: Experiences with community-based approaches. Build. Res. Inf. 2004, 32, 414–426. [Google Scholar] [CrossRef]
- Phillips, B.D.; Wikle, T.A.; Hakim, A.H.; Pike, L. Establishing and operating shelter after Hurricane Katrina. Int. J. Emerg. Manag. 2012, 8, 153–167. [Google Scholar] [CrossRef]
- North, C.S.; King, R.V.; Fowler, R.L.; Kucmierz, R.; Wade, J.D.; Hogan, D.; Carlo, J.T. Delivery of Mental Health Care in a Large Disaster Shelter. Disaster Med. Public Health Prep. 2015, 9, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labour and Welfare; Ministry of Education, Culture, Sports, Science and Technology. Calling Attention to Surveys and Research Conducted in the Disaster Area (Office Work Communication) (In Japanese). 2011. Available online: https://www.mhlw.go.jp/seisakunitsuite/bunya/hokabunya/kenkyujigyou/hisaichi/jimurenraku.html (accessed on 30 October 2020).
- Charmaz, K. The Power of Constructivist Grounded Theory for Critical Inquiry. Qual. Inq. 2016, 23, 34–45; [Google Scholar] [CrossRef]
- Kesennuma City. Kesennuma City Report—About the damage situation of Kesennuma City Related to the Great Earthquake (In Japanese). Available online: https://www.kesennuma.miyagi.jp/sec/s019/010/010/040/001/shimin1shiryo7.pdf (accessed on 9 September 2020).
- Kesennuma City. Statistics Report on Kesennuma City (In Japanese). Available online: http://www.kesennuma.miyagi.jp/sec/s021/010/020/060/1355201655254.html (accessed on 9 September 2020).
- The United Nations Statistics Division. Demographic and Social Statistics Population Size and Density. Available online: https://unstats.un.org/unsd/demographic-social/products/dyb/documents/DYB2018/table08.pdf (accessed on 9 September 2020).
- Glaser, B.G.; Strauss, A.L.; Strutzel, E. The Discovery of Grounded Theory: Strategies for Qualitative Research: Strategies for Qualitative Research; Aldine Publishing Company: Chicago, IL, USA, 1967; ISBN 0-202-30260-1. [Google Scholar]
- Patton, M.Q. Qualitative Research & Evaluation Methods: Integrating Theory and Practice, 4th ed.; AGE: Los Angeles, CA, USA, 2014; ISBN 978-1412972123. [Google Scholar]
- Ministry of Health, Labour and Welfare. Number of Full-Time Public Health Nurses by Municipality, Public Health Nurse Activity Area Survey. 2011. Available online: https://www.e-stat.go.jp/stat-search/files?page=1&layout=datalist&toukei=00450471&tstat=000001035128&cycle=7&tclass1=000001038881&tclass2=000001049571&stat_infid=000012886178 (accessed on 30 October 2020).
- FEMA. The Revised FEMA Incident Action Planning Guide. Security, U.S. Department of Homeland Security: U.S. Washington. 2015. Available online: https://www.fema.gov/sites/default/files/2020-07/Incident_Action_Planning_Guide_Revision1_august2015.pdf (accessed on 9 September 2020).
- Jakeway, C.C.; LaRosa, G.; Cary, A.; Schoenfisch, S. The role of public health nurses in emergency preparedness and response: A position paper of the Association of State and Territorial Directors of Nursing. Public Health Nurs. 2008, 25, 353–361. [Google Scholar] [CrossRef] [PubMed]
- Charmaz, K. Constructing Grounded Theory: A Practical Guide through Qualitative Analysis; Saga: London, UK, 2006; ISBN 978-0761973539. [Google Scholar]
- Communuty-Care Policy Network. Dementia Supporter Program (In Japanese). Available online: http://www.caravanmate.com/aboutus/ (accessed on 9 September 2020).
- Fire and Disaster Management Agency. Self Fire Defense Groups (In Japanese). Available online: https://www.fdma.go.jp/relocation/syobodan/ (accessed on 9 September 2020).

| District | Old City * | Karakuwa | Motoyoshi |
|---|---|---|---|
| Area (km2) | 130.03 | 42.31 | 106.7 |
| Population ** | 52,089 | 7420 | 10,855 |
| Percentage of population over 65 years old ** | 29.7% | 34.2% | 30.8% |
| Population density (person/km2) ** | 145.3 | 175.4 | 101.7 |
| Damage Status | |||
| Houses | |||
| Fully destroyed | 11,391 | 1867 | 2417 |
| Destroyed, difficult to live in | 1689 | 80 | 289 |
| Partly destroyed | 2666 | 186 | 558 |
| Percentage of all houses | 38.40% | 28.20% | 28.50% |
| Evacuation shelters | |||
| Maximum number of shelters | 65 | 16 | 17 |
| Maximum number of residents in the shelters | 2000 | 230 | 530 |
| Total number of residents in the shelters | 14,491 | 1250 | 3005 |
| Operational Policy of the Evacuation Shelter | |
|---|---|
| Station Type (in the Old City) | Patrol Type (in Motoyoshi District) |
| Theme 1: The lack of an operational preparedness policy for the shelters | |
| Everyone gathered in the city office’s large hall, and, while still not knowing anything at all about the disaster conditions, we received a command from Headquarters to move to an evacuation shelter. We were told to scatter to each of the evacuation shelters. Id 02 | For my title, I was a leader. Since the section manager happened to be there, I said, “Section manager, no one can stay in the evacuation shelters. We must move between the shelters in two-person teams,” and with that, a patrol-focused evacuation shelter management style was established. Id 11 |
| So then, we wondered, “When we do go out there, what should we do?” Id 01 | With administrative nurses, there are two persons, and with public health nurses, there are four persons. I thought this could not cover all of the evacuation shelters. I recommended the following to the community health policy leader: “Divide into groups of two nurses and rotate around the evacuation shelters to check the situation.” Id 09 |
| Since we did not know who would be coming to the evacuation shelter, the management varied completely, depending on the evacuation shelter. Id 01 | I thought that fixed placement was impossible because there were few public health nurses. It’s been like that from the first day of the disaster. Id 09 |
| Theme 2: The provision of support to the shelter residents | |
| At the large evacuation shelters, with everyone coming together without territorial connections or links, since the shelters had the presence of an administrative staff, everything that has to do with sheltering is done by the administrative staff. Id 13 | There were the municipal hospital nurses and nurses who were working independently, among whom leadership was just naturally generated. Id 04 |
| The evacuation shelter administrative operations involved the delivery of meals, the creation of name lists, and the carry-in of resources, and it ended with that. Since I was a medical technician, I could not, of course, say that I couldn’t handle it. Id 02 | The day after the earthquake, we asked the nurses at the shelter—including midwives, nurses from city hospitals, and teachers at the school for the disabled—to watch the residents at the shelter and contact us if anything happened. Id 11 |
| I couldn’t do it (nurse work), because there was no other person. The situation did not allow us to work only on health issues. Id 03 | Of course, it was not possible for health professionals to be stationed at all of the places where the shelters were established, so I checked the situation by walking around the places that became shelters in order, with one pair of two health professionals. Id 09 |
| I remained at that evacuation shelter all the way until around April. With the arrival of the support public health nurses from non-disaster areas, we staff were finally able to return home. Id 02 | |
| Theme 3: The autonomy of the shelter residents | |
| There were some small evacuation shelters where such residents’ associations moved. A large evacuation shelter where everyone gathered from various places was managed by the administration. There are administrative staff here as well, so the administrative staff must act in the core role of evacuation shelter management. Id 10 | Self-nursing teams had been created. These team members were nurses who couldn’t go to work, and they checked on the residents’ health in the shelters while we were patrolling. Id 04 |
| We talked about our shelter several times (about self-government management). A problem has arisen among us that said, “If possible, people who are evacuating should be able to operate independently.” Was it about a week? Id 01 | From the next day, an independent nursing team consisting of midwives, municipal hospital nurses, and elderly home nurses cared for and evaluated the health problems [of the residents] at the evacuation shelters. Therefore, I requested health management at the shelter. I asked them. “Please contact me immediately when any accidents occur.” Id 11 |
| Every morning a staff member holds a meeting and says, “Let’s do this today.” Since we had to operate the shelter from the start, the residents naturally though that only administrative officials should operate the evacuation shelter. Id 02 | The teams did not act without notifying the chief clerk of public health. This did not mean that the branch office approved these teams; they provided systems for sharing information and behaved in a cohesive manner. Id 08 |
| I now think that what we had to do was more than managing the evacuation shelters. Certainly, we should have been able to leave the shelter for a bit when the medical team arrived. Id 01 | |
| Theme 4: The relationship with the external PHN support teams | |
| Since the supporters will be replaced in a week, I have to hear the information from the previous teams and convey it to the new team each time. I have to endlessly repeat this information sharing. It’s a new support form for the shelter. I stayed in the shelter for half a day (even in April). I only handed over the information and then worked in the area as a public health nurse. Id 14 | Once I explained to the residents about the beginning of the continuous activities of the external support team, I left the shelter and entrusted the management to them. I was able to integrate the information that the branch government had and the new information captured by the support teams; therefore, together, we could discuss what to do next. Id 08 |
| If I knew that support was coming at that time, I might have left the shelter early. But by staying (we are in the shelter) for a long time, it was rather hard to leave the shelter. Id 01 | Since information was collected in only one building (the branch office), it was easy for the public health nurses to have external support. After that, we were able to make allocation plans for support with other members. Id 11 |
| At that time, I first noticed that my original work had stopped. I got back to my heart. It’s April, and I have to do a lot of things, but it’s all stopped. Id 02 | We were able to integrate the information held in the city office with the new situation captured by the external supporters. So I was able to think together with the support team about what to do next. Id 04 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mori, H.; Obuchi, S.P.; Sugawara, Y.; Nakayama, T.; Takahashi, R. Comparison of Two Evacuation Shelter Operating Policies and the Role of Public Health Nurses after the Great East Japan Earthquake: A Qualitative Study. Int. J. Environ. Res. Public Health 2020, 17, 8310. https://doi.org/10.3390/ijerph17228310
Mori H, Obuchi SP, Sugawara Y, Nakayama T, Takahashi R. Comparison of Two Evacuation Shelter Operating Policies and the Role of Public Health Nurses after the Great East Japan Earthquake: A Qualitative Study. International Journal of Environmental Research and Public Health. 2020; 17(22):8310. https://doi.org/10.3390/ijerph17228310
Chicago/Turabian StyleMori, Hiroko, Shuichi P. Obuchi, Yasuhiro Sugawara, Takeo Nakayama, and Ryutaro Takahashi. 2020. "Comparison of Two Evacuation Shelter Operating Policies and the Role of Public Health Nurses after the Great East Japan Earthquake: A Qualitative Study" International Journal of Environmental Research and Public Health 17, no. 22: 8310. https://doi.org/10.3390/ijerph17228310