Association between Maternal Postpartum Depression, Stress, Optimism, and Breastfeeding Pattern in the First Six Months

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
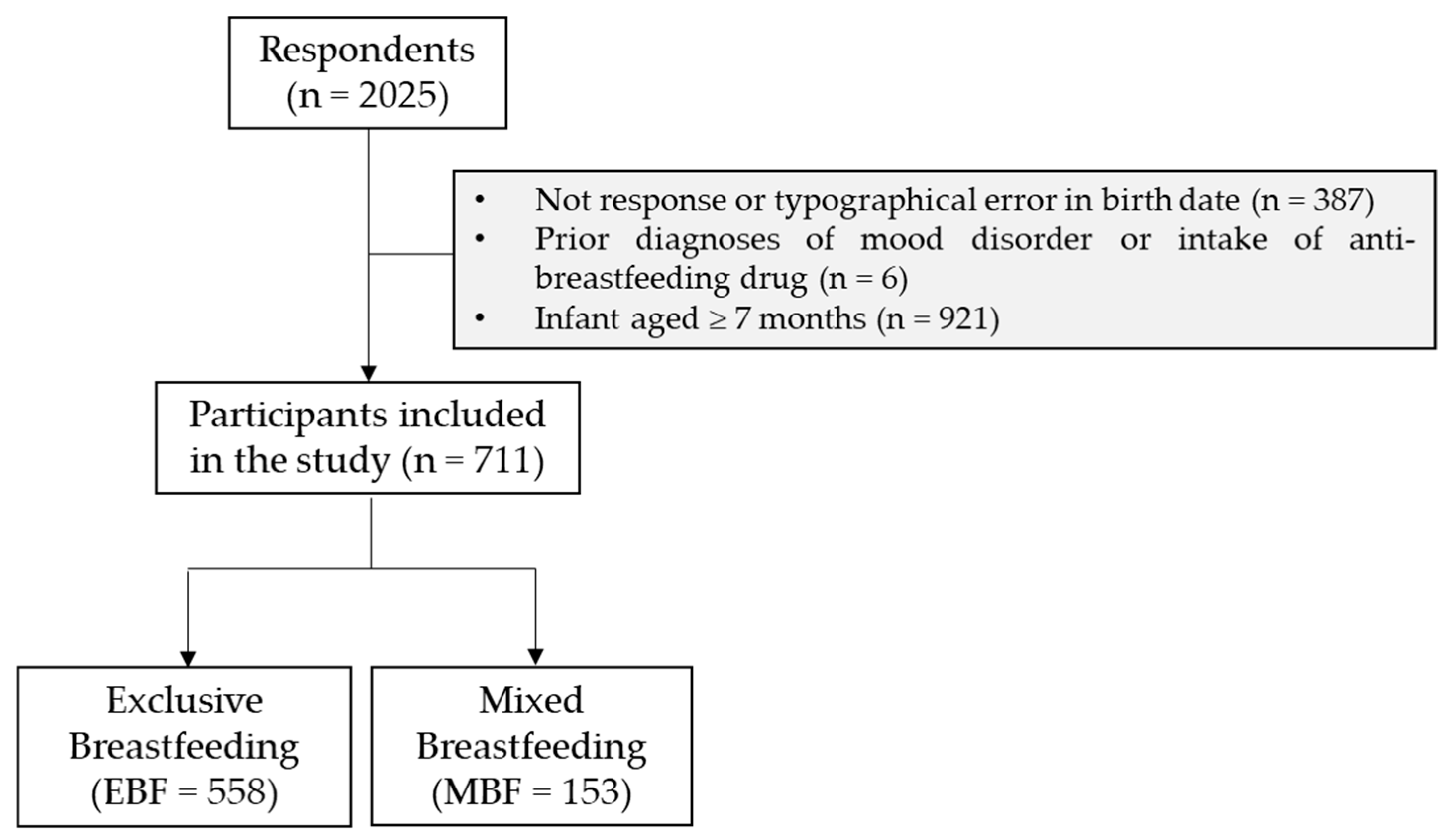
2.1. Study Design and Participants Collection
2.2. Socioeconomical Variables and Breastfeeding Period
2.3. Infant Feeding Practices
2.4. Psychological and Breastfeeding Adherence Instruments
2.5. Statistical Analysis
3. Results
3.1. Socioeconomic Factors and Infant Feeding Practices
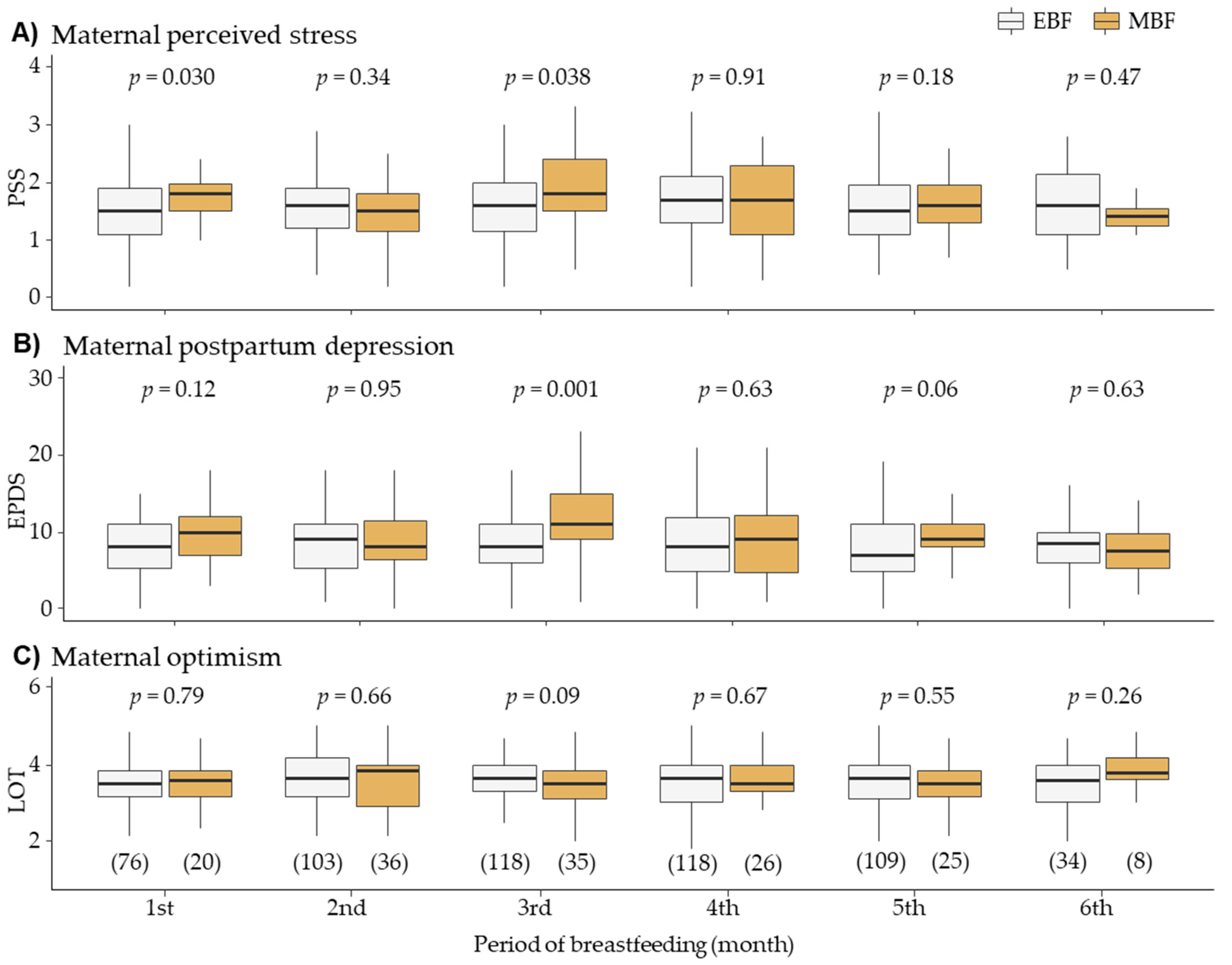
3.2. Maternal Psychological Factors Related to Infant Feeding Practices
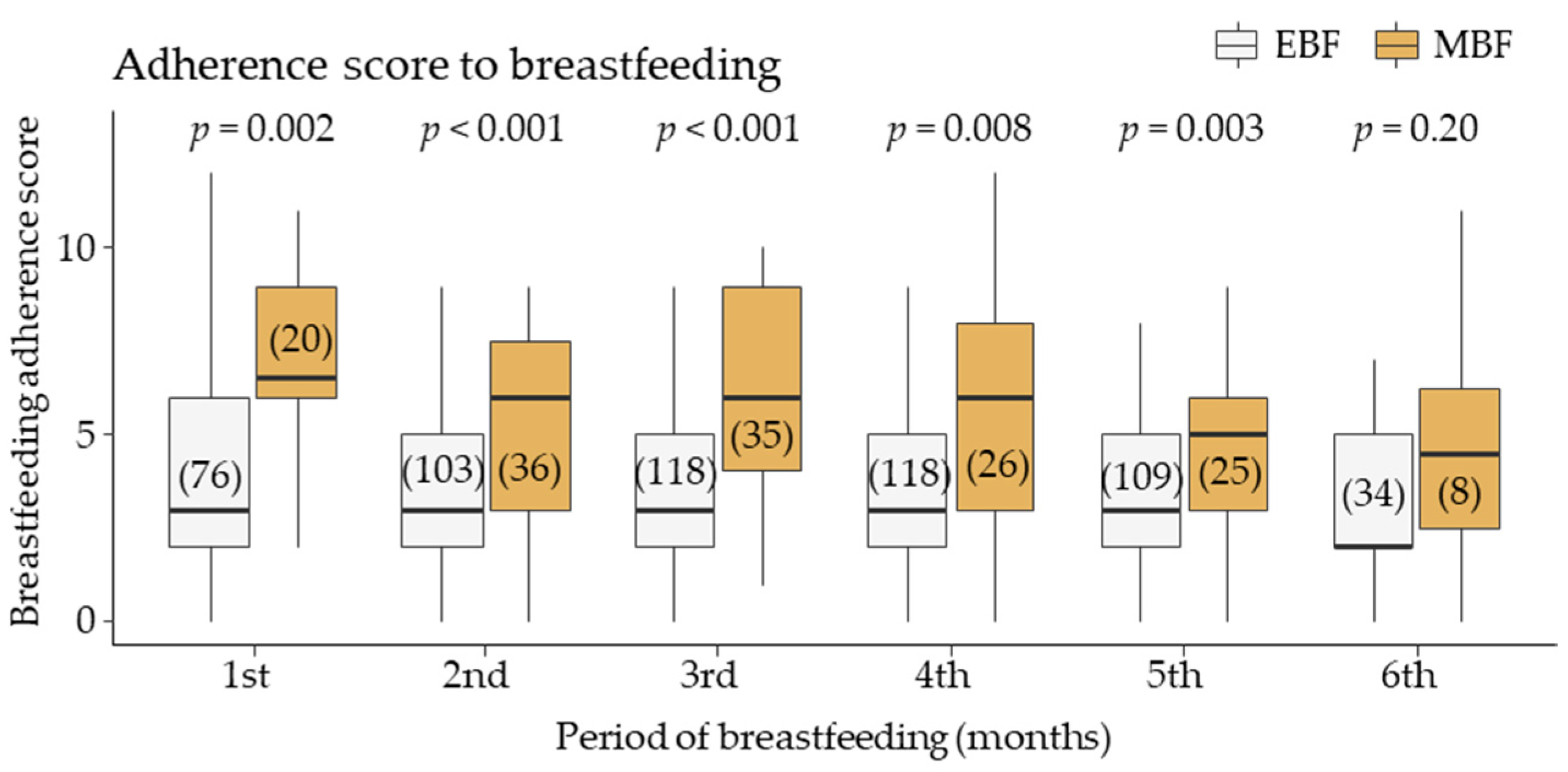
3.3. Breastfeeding Adherence score (BAS) and Psychological Factors
3.4. Breastfeeding Adherence score and Infant Feeding Practices
4. Discussion
Study Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- WHO. Exclusive Breastfeeding for Optimal Growth, Development and Health of Infants. Available online: https://www.who.int/elena/titles/exclusive_breastfeeding/en/ (accessed on 25 August 2020).
- Ip, S.; Chung, M.; Raman, G.; Chew, P.; Magula, N.; DeVine, D.; Trikalinos, T.; Lau, J. Breastfeeding and maternal and infant health outcomes in developed countries. Evid. Rep. Technol. Assess 2007, 153, 1–186. [Google Scholar]
- Hauck, F.R.; Thompson, J.M.; Tanabe, K.O.; Moon, R.Y.; Vennemann, M.M. Breastfeeding and reduced risk of sudden infant death syndrome: A meta-analysis. Pediatrics 2011, 128, 103–110. [Google Scholar] [CrossRef] [Green Version]
- Horta, B.L.; Loret de Mola, C.; Victora, C.G. Long-term consequences of breastfeeding on cholesterol, obesity, systolic blood pressure and type 2 diabetes: A systematic review and meta-analysis. Acta Paediatr. 2015, 104, 30–37. [Google Scholar] [CrossRef]
- Amitay, E.L.; Keinan-Boker, L. Breastfeeding and Childhood Leukemia Incidence: A Meta-analysis and Systematic Review. JAMA Pediatr. 2015, 169, e151025. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kramer, M.S.; Aboud, F.; Mironova, E.; Vanilovich, I.; Platt, R.W.; Matush, L.; Igumnov, S.; Fombonne, E.; Bogdanovich, N.; Ducruet, T.; et al. Breastfeeding and child cognitive development: New evidence from a large randomized trial. Arch Gen. Psychiatry 2008, 65, 578–584. [Google Scholar] [CrossRef]
- Black, R.E.; Allen, L.H.; Bhutta, Z.A.; Caulfield, L.E.; de Onis, M.; Ezzati, M.; Mathers, C.; Rivera, J.; Maternal and Child Undernutrition Study Group. Maternal and child undernutrition: Global and regional exposures and health consequences. Lancet 2008, 371, 243–260. [Google Scholar] [CrossRef]
- Chowdhury, R.; Sinha, B.; Sankar, M.J.; Taneja, S.; Bhandari, N.; Rollins, N.; Bahl, R.; Martines, J. Breastfeeding and maternal health outcomes: A systematic review and meta-analysis. Acta Paediatr 2015, 104, 96–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dias, C.C.; Figueiredo, B. Breastfeeding and depression: A systematic review of the literature. J. Affect Disord 2015, 171, 142–154. [Google Scholar] [CrossRef] [Green Version]
- Binns, C.; Lee, M.; Low, W.Y. The Long-Term Public Health Benefits of Breastfeeding. Asia Pac. J. Public Health 2016, 28, 7–14. [Google Scholar] [CrossRef] [Green Version]
- Gianni, M.L.; Bettinelli, M.E.; Manfra, P.; Sorrentino, G.; Bezze, E.; Plevani, L.; Cavallaro, G.; Raffaeli, G.; Crippa, B.L.; Colombo, L.; et al. Breastfeeding Difficulties and Risk for Early Breastfeeding Cessation. Nutrients 2019, 11, 2266. [Google Scholar] [CrossRef] [Green Version]
- Al-Sahab, B.; Lanes, A.; Feldman, M.; Tamim, H. Prevalence and predictors of 6-month exclusive breastfeeding among Canadian women: A national survey. BMC Pediatr. 2010, 10, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Odar Stough, C.; Khalsa, A.S.; Nabors, L.A.; Merianos, A.L.; Peugh, J. Predictors of Exclusive Breastfeeding for 6 Months in a National Sample of US Children. Am. J. Health Promot. 2019, 33, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Khanal, V.; Lee, A.H.; Scott, J.A.; Karkee, R.; Binns, C.W. Implications of methodological differences in measuring the rates of exclusive breastfeeding in Nepal: Findings from literature review and cohort study. BMC Pregnancy Childbirth 2016, 16, 389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. European Region Has Lowest Global Breastfeeding Rates. Available online: https://www.euro.who.int/en/health-topics/Life-stages/maternal-and-newborn-health/news/news/2015/08/who-european-region-has-lowest-global-breastfeeding-rates (accessed on 25 August 2020).
- Sarki, M.; Parlesak, A.; Robertson, A. Comparison of national cross-sectional breast-feeding surveys by maternal education in Europe (2006–2016). Public Health Nutr. 2019, 22, 848–861. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pediatría, C.d.L.M.d.l.A.E.d. Lactancia Materna en Cifras: Tasas de Inicio y Duración de la Lactancia en España y en Otros Países. Available online: https://www.aeped.es/sites/default/files/documentos/201602-lactancia-materna-cifras.pdf (accessed on 25 August 2020).
- Theurich, M.A.; Davanzo, R.; Busck-Rasmussen, M.; Diaz-Gomez, N.M.; Brennan, C.; Kylberg, E.; Baerug, A.; McHugh, L.; Weikert, C.; Abraham, K.; et al. Breastfeeding Rates and Programs in Europe: A Survey of 11 National Breastfeeding Committees and Representatives. J. Pediatr. Gastroenterol Nutr. 2019, 68, 400–407. [Google Scholar] [CrossRef]
- Kronborg, H.; Vaeth, M. Validation of the Breastfeeding Score-A Simple Screening Tool to Predict Breastfeeding Duration. Nutrients 2019, 11, 2852. [Google Scholar] [CrossRef] [Green Version]
- Sheehan, D.; Krueger, P.; Watt, S.; Sword, W.; Bridle, B. The Ontario Mother and Infant Survey: Breastfeeding outcomes. J. Hum. Lact. 2001, 17, 211–219. [Google Scholar] [CrossRef]
- Jones, J.R.; Kogan, M.D.; Singh, G.K.; Dee, D.L.; Grummer-Strawn, L.M. Factors associated with exclusive breastfeeding in the United States. Pediatrics 2011, 128, 1117–1125. [Google Scholar] [CrossRef] [Green Version]
- Victora, C.G.; Bahl, R.; Barros, A.J.; Franca, G.V.; Horton, S.; Krasevec, J.; Murch, S.; Sankar, M.J.; Walker, N.; Rollins, N.C.; et al. Breastfeeding in the 21st century: Epidemiology, mechanisms, and lifelong effect. Lancet 2016, 387, 475–490. [Google Scholar] [CrossRef] [Green Version]
- Nishioka, E.; Haruna, M.; Ota, E.; Matsuzaki, M.; Murayama, R.; Yoshimura, K.; Murashima, S. A prospective study of the relationship between breastfeeding and postpartum depressive symptoms appearing at 1-5 months after delivery. J. Affect. Disord 2011, 133, 553–559. [Google Scholar] [CrossRef]
- Field, T.; Diego, M.A.; Hernandez-Reif, M.; Figueiredo, B.; Ascencio, A.; Schanberg, S.; Kuhn, C. Prenatal dysthymia versus major depression effects on maternal cortisol and fetal growth. Depress. Anxiety 2008, 25, E11–E16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mezzacappa, E.S.; Katlin, E.S. Breast-feeding is associated with reduced perceived stress and negative mood in mothers. Health Psychol. 2002, 21, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Pope, C.J.; Mazmanian, D. Breastfeeding and Postpartum Depression: An Overview and Methodological Recommendations for Future Research. Depress. Res. Treat. 2016, 2016, 4765310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sisk, P.M.; Lovelady, C.A.; Dillard, R.G.; Gruber, K.J. Lactation counseling for mothers of very low birth weight infants: Effect on maternal anxiety and infant intake of human milk. Pediatrics 2006, 117, e67–e75. [Google Scholar] [CrossRef] [Green Version]
- Ystrom, E. Breastfeeding cessation and symptoms of anxiety and depression: A longitudinal cohort study. BMC Pregnancy Childbirth 2012, 12, 36. [Google Scholar] [CrossRef] [Green Version]
- Islam, M.J.; Broidy, L.; Baird, K.; Mazerolle, P. Intimate partner violence around the time of pregnancy and postpartum depression: The experience of women of Bangladesh. PLoS ONE 2017, 12, e0176211. [Google Scholar] [CrossRef] [Green Version]
- INE. Hogares y Personas. Available online: https://www.ine.es/jaxiT3/Datos.htm?t=10694#!tabs-tabla (accessed on 25 August 2020).
- Yourkavitch, J.; Chetwynd, E.M. Toward Consistency: Updating Lactation and Breastfeeding Terminology for Population Health Research. J. Hum. Lact. 2019, 35, 418–423. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Remor, E. Psychometric properties of a European Spanish version of the Perceived Stress Scale (PSS). Span. J. Psychol. 2006, 9, 86–93. [Google Scholar] [CrossRef] [Green Version]
- White, R.S.; Jiang, J.; Hall, C.B.; Katz, M.J.; Zimmerman, M.E.; Sliwinski, M.; Lipton, R.B. Higher Perceived Stress Scale scores are associated with higher pain intensity and pain interference levels in older adults. J. Am. Geriatr. Soc. 2014, 62, 2350–2356. [Google Scholar] [CrossRef] [Green Version]
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. Br. J. Psychiatry 1987, 150, 782–786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia-Esteve, L.; Ascaso, C.; Ojuel, J.; Navarro, P. Validation of the Edinburgh Postnatal Depression Scale (EPDS) in Spanish mothers. J. Affect. Disord. 2003, 75, 71–76. [Google Scholar] [CrossRef]
- Vazquez, M.B.; Miguez, M.C. Validation of the Edinburgh postnatal depression scale as a screening tool for depression in Spanish pregnant women. J. Affect. Disord. 2019, 246, 515–521. [Google Scholar] [CrossRef]
- Smith-Nielsen, J.; Matthey, S.; Lange, T.; Vaever, M.S. Validation of the Edinburgh Postnatal Depression Scale against both DSM-5 and ICD-10 diagnostic criteria for depression. BMC Psychiatry 2018, 18, 393. [Google Scholar] [CrossRef] [Green Version]
- Scheier, M.F.; Carver, C.S.; Bridges, M.W. Distinguishing optimism from neuroticism (and trait anxiety, self-mastery, and self-esteem): A reevaluation of the Life Orientation Test. J. Pers Soc. Psychol. 1994, 67, 1063–1078. [Google Scholar] [CrossRef] [PubMed]
- Ferrando, P.J.; Chico, E.; Tous, J.M. Propiedades psicométricas del test de optimismo Life Orientation Test. Psicotherma 2002, 14, 673–680. [Google Scholar]
- Pan, T.M.; Mills, S.D.; Fox, R.S.; Baik, S.H.; Harry, K.M.; Roesch, S.C.; Sadler, G.R.; Malcarne, V.L. The Psychometric Properties of English and Spanish Versions of the Life Orientation Test-Revised in Hispanic Americans. J. Psychopathol. Behav. Assess. 2017, 39, 657–668. [Google Scholar] [CrossRef] [PubMed]
- Glaesmer, H.; Rief, W.; Martin, A.; Mewes, R.; Brahler, E.; Zenger, M.; Hinz, A. Psychometric properties and population-based norms of the Life Orientation Test Revised (LOT-R). Br. J. Health Psychol. 2012, 17, 432–445. [Google Scholar] [CrossRef]
- Section on Breastfeeding. Breastfeeding and the use of human milk. Pediatrics 2012, 129, e827–e841. [Google Scholar] [CrossRef] [Green Version]
- School of Public Health, Yale University. Becoming Breastfeeding Friendly: A Guide to Global Scale Up. Available online: https://publichealth.yale.edu/bfci/countries/mexico/ (accessed on 23 September 2020).
- de Lauzon-Guillain, B.; Thierry, X.; Bois, C.; Bournez, M.; Davisse-Paturet, C.; Dufourg, M.N.; Kersuzan, C.; Ksiazek, E.; Nicklaus, S.; Vicaire, H.; et al. Maternity or parental leave and breastfeeding duration: Results from the ELFE cohort. Matern. Child. Nutr. 2019, 15, e12872. [Google Scholar] [CrossRef] [PubMed]
- Avendano, M.; Berkman, L.F.; Brugiavini, A.; Pasini, G. The long-run effect of maternity leave benefits on mental health: Evidence from European countries. Soc. Sci Med. 2015, 132, 45–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aguilar-Ortega, J.M.; Gonzalez-Pascual, J.L.; Cardenete-Reyes, C.; Perez-de-Algaba-Cuenca, C.; Perez-Garcia, S.; Esteban-Gonzalo, L. Adherence to initial exclusive breastfeeding among Chinese born and native Spanish mothers. BMC Pregnancy Childbirth 2019, 19, 44. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Pascual, J.L.; Aguilar-Ortega, J.M.; Esteban-Gonzalo, L.; Mesa-Leiva, C.; Perez-Garcia, S.; Cardenete-Reyes, C. Comparison of attitudes to breastfeeding among Spanish-born and Chinese-born postpartum women in Madrid. Int. Breastfeed. J. 2018, 13, 45. [Google Scholar] [CrossRef] [PubMed]
- Social, S.-S. Periodo de Descanso en Relacion al Estatuto de los Trabajadores. Available online: http://www.seg-social.es/wps/portal/wss/internet/Trabajadores/PrestacionesPensionesTrabajadores/6b96a085-4dc0-47af-b2cb-97e00716791e/0b5879ed-1156-4676-b38c-7229dcba9c49/descansoet#DescansoET (accessed on 25 August 2020).
- Brandao, T.; Brites, R.; Hipolito, J.; Pires, M.; Nunes, O. Dyadic coping, marital adjustment and quality of life in couples during pregnancy: An actor-partner approach. J. Reprod. Infant Psychol. 2020, 38, 49–59. [Google Scholar] [CrossRef] [Green Version]
- Rusu, P.P.; Nussbeck, F.W.; Leuchtmann, L.; Bodenmann, G. Stress, dyadic coping, and relationship satisfaction: A longitudinal study disentangling timely stable from yearly fluctuations. PLoS ONE 2020, 15, e0231133. [Google Scholar] [CrossRef] [Green Version]
- Palmer, L.; Carlsson, G.; Mollberg, M.; Nystrom, M. Severe breastfeeding difficulties: Existential lostness as a mother-Women’s lived experiences of initiating breastfeeding under severe difficulties. Int. J. Qual. Stud. Health Well Being 2012, 7, 10846. [Google Scholar] [CrossRef]
- Cunningham, E.M.; Doyle, E.I.; Bowden, R.G. Maternity Nurses’ Perceptions of Implementation of the Ten Steps to Successful Breastfeeding. MCN Am. J. Matern. Child. Nurs. 2018, 43, 38–43. [Google Scholar] [CrossRef]
- Madrid Munoz, R.; Cano, C.C.; Cortes Rojas, R. The impact of the extension of the post-natal in the adherence to breastfeeding Cohort study. Rev. Chil. Pediatr. 2018, 89, 484–490. [Google Scholar] [CrossRef] [Green Version]
- Li, R.; Fein, S.B.; Chen, J.; Grummer-Strawn, L.M. Why mothers stop breastfeeding: Mothers’ self-reported reasons for stopping during the first year. Pediatrics 2008, 122 (Suppl. 2), S69–S76. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| EBF (n = 558) | MBF (n = 153) | p-Value | |
|---|---|---|---|
| Maternal age (years) | 33.0 [30.0; 36.0] | 33.0 [29.0; 36.0] | 0.93 |
| Primiparous | 36.7% (205) | 43.3% (65) | 0.009 |
| Gestational age (weeks) | 39.3 [38.3; 40.4] | 39.0 [38.0; 39.8] | <0.001 |
| Origin | <0.001 | ||
| European | 74.0% (413) | 57.3% (86) | |
| North American | 16.3% (91) | 27.3% (41) | |
| South American | 8.2% (46) | 12.7% (19) | |
| Asian | 0.2% (1) | 0.7% (1) | |
| Educational level | 0.65 | ||
| Middle school | 9.9% (55) | 11.3% (17) | |
| High school | 17.2% (96) | 19.3% (29) | |
| University degree | 72.9% (407) | 68.0% (102) | |
| Work situation | 0.69 | ||
| Studying | 1.6% (9) | 1.3% (2) | |
| Working | 74.9% (418) | 72.0% (108) | |
| Unemployment | 23.3% (130) | 26.7% (40) | |
| Family core | 0.33 | ||
| Single-parent | 12.5% (70) | 16.0% (24) | |
| Two-parents | 87.5% (488) | 84.0% (126) | |
| Number of family members | 4 [3; 4] | 3 [3; 4] | 0.11 |
| Economic status | 0.96 | ||
| No-income | 2.3% (13) | 2.7% (4) | |
| < 1000 € | 8.4% (47) | 9.3% (14) | |
| 1000–2500 € | 45.5% (254) | 42.7% (64) | |
| 2501–4000 € | 33.3% (186) | 35.3% (53) | |
| > 4000 € | 9.0% (50) | 9.3% (14) |
| Period of Breastfeeding | PSS | EPDS | LOT | |||
|---|---|---|---|---|---|---|
| ρ | p-Value | ρ | p-Value | ρ | p-Value | |
| First month (n = 96) | 0.27 | 0.018 | 0.21 | 0.05 | −0.09 | 0.43 |
| Second month (n = 139) | 0.07 | 0.54 | 0.02 | 0.82 | −0.20 | 0.028 |
| Third month (153) | 0.13 | 0.13 | 0.30 | <0.001 | −0.15 | 0.07 |
| Fourth month (n = 144) | 0.06 | 0.51 | 0.10 | 0.28 | 0.02 | 0.81 |
| Fifth month (n = 134) | 0.14 | 0.14 | 0.11 | 0.31 | −0.01 | 0.97 |
| Sixth month (n = 42) | 0.09 | 0.61 | 0.00 | 0.81 | −0.08 | 0.70 |
| Model 1 | Model 2 | Model 3 | Model 4 | |||||
|---|---|---|---|---|---|---|---|---|
| OR 95% [CI] | p-Value | OR 95% [CI] | p-Value | OR 95% [CI] | p-Value | OR 95% [CI] | p-Value | |
| BAS | 1.4 [1.2; 1.6] | <0.001 | - | - | - | - | 1.3 [1.1; 1.6] | 0.001 |
| PSS | - | - | 1.5 [0.9; 2.3] | 0.09 | - | - | 1.0 [0.5; 2.0] | 0.95 |
| EPDS | - | - | - | - | 1.1 [1.0; 1.1] | 0.020 | 1.1 [1.0; 1.2] | 0.19 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gila-Díaz, A.; Carrillo, G.H.; López de Pablo, Á.L.; Arribas, S.M.; Ramiro-Cortijo, D. Association between Maternal Postpartum Depression, Stress, Optimism, and Breastfeeding Pattern in the First Six Months. Int. J. Environ. Res. Public Health 2020, 17, 7153. https://doi.org/10.3390/ijerph17197153
Gila-Díaz A, Carrillo GH, López de Pablo ÁL, Arribas SM, Ramiro-Cortijo D. Association between Maternal Postpartum Depression, Stress, Optimism, and Breastfeeding Pattern in the First Six Months. International Journal of Environmental Research and Public Health. 2020; 17(19):7153. https://doi.org/10.3390/ijerph17197153
Chicago/Turabian StyleGila-Díaz, Andrea, Gloria Herranz Carrillo, Ángel Luis López de Pablo, Silvia M. Arribas, and David Ramiro-Cortijo. 2020. "Association between Maternal Postpartum Depression, Stress, Optimism, and Breastfeeding Pattern in the First Six Months" International Journal of Environmental Research and Public Health 17, no. 19: 7153. https://doi.org/10.3390/ijerph17197153