Evaluation of Quality of Life of Adult Patients with Celiac Disease in Argentina: From Questionnaire Validation to Assessment

 , , , , ,
, , , , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
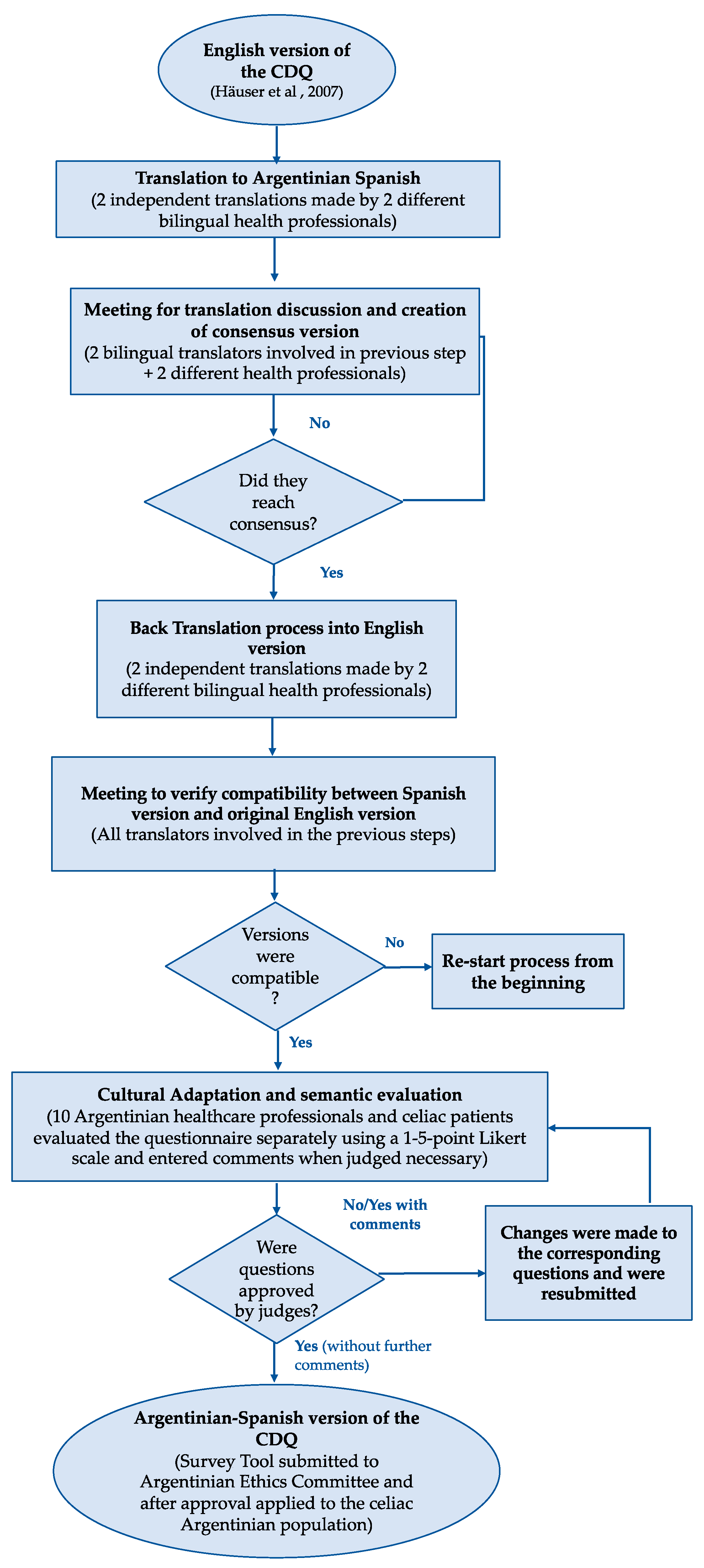
2.1. Translation and Re-Translation of the CDQ to Argentinian-Spanish Language
2.2. Cultural Adaptation and Semantic Evaluation
2.3. Application of the CDQ in Argentina
2.4. Statistical Analysis
3. Results
3.1. Translation and Re-Translation; Cultural Adaptation and Semantic Evaluation
3.2. Internal Consistency and Construct Validity of the Argentinian CDQ
3.3. Application of the CDQ in Argentina
4. Discussion
Potential Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
 |
| Consentimiento Previo, Libre e Informado Cuestionario de calidad de vida asociada a la salud de celíacos argentinos Si sos mayor de 18 años y sos celíaco/a, te invitamos a participar de nuestra investigación respondiendo a las preguntas del siguiente cuestionario. |
| El cuestionario incluye 28 preguntas sobre tu bienestar general, síntomas asociados a tu celiaquía, y tu estado de humor. Lee cada pregunta con mucha atención y seleccioná la opción que mejor describa cómo te has sentido en las últimas 2 semanas. Si no te identificás con alguna de las preguntas realizadas, simplemente, dejala en blanco. ATENCIÓN: Una vez que aceptes participar en este estudio, sólo podrás acceder al cuestionario 1 vez. Por eso, asegurate de disponer de aproximadamente 10 minutos de tu tiempo para poder responderlo hasta el final y así ayudarnos a mejorar la calidad de vida de los celíacos de nuestro país. Tu participación es completamente anónima. Si te interesa saber el resultado de nuestra investigación, lo divulgaremos en la página de la Asociación Argentina de Celíacos una vez concluido el estudio. Cualquier duda podés comunicarte con Nicole Selleski: selleskinicole@gmail.com |
References
- Itzlinger, A.; Branchi, F.; Elli, L.; Schumann, M.; Itzlinger, A.; Branchi, F.; Elli, L.; Schumann, M. Gluten-free diet in celiac disease—Forever and for all? Nutrients 2018, 10, 1796. [Google Scholar] [CrossRef] [Green Version]
- Hauser, W.; Gold, J.; Stallmach, A.; Caspary, W.F.; Stein, J. Development and validation of the Celiac Disease Questionnaire (CDQ), a disease-specific health-related quality of life measure for adult patients with celiac disease. J. Clin. Gastroenterol. 2007, 41, 157–166. [Google Scholar] [PubMed]
- Crocker, H.; College, H.M.; Manchester, H. Coeliac Disease: Health-Related Quality of Life and Patients’ Experiences of Health Care Services Diagnosis and Management of Coeliac Disease: Health-Related Quality of Life and Patients’ Experiences of Health Care Services. Ph.D. Thesis, University of Oxford, Oxford, UK, 2016. [Google Scholar]
- European Medicines Agency. Regulatory Guidance for the Use of Health-Related Quality of Life (HRQL) Measures in the Evaluation of Medicinal Products; European Medicines Agency (EMEA): London, UK, 2005.
- Lindfors, K.; Ciacci, C.; Kurppa, K.; Lundin, K.E.A.; Makharia, G.K.; Mearin, M.L.; Murray, J.A.; Verdu, E.F.; Kaukinen, K. Coeliac disease. Nat. Rev. Dis. Primers 2019, 5. [Google Scholar] [CrossRef]
- Singh, P.; Arora, A.; Strand, T.A.; Leffler, D.A.; Catassi, C.; Green, P.H.; Kelly, C.P.; Ahuja, V.; Makharia, G.K. Global prevalence of celiac disease: Systematic review and meta-analysis. Clin. Gastroenterol. Hepatol. 2018, 16, 823–836. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Araújo, H.M.C.; Araújo, W.M.C. Coeliac disease. Following the diet and eating habits of participating individuals in the Federal District, Brazil. Appetite 2011, 57, 105–109. [Google Scholar] [CrossRef]
- Skjerning, H.; Mahony, R.O.; Husby, S.; DunnGalvin, A. Health-related quality of life in children and adolescents with celiac disease: Patient-driven data from focus group interviews. Qual. Life Res. 2014, 23, 1883–1894. [Google Scholar] [CrossRef] [PubMed]
- Chishty, S.; Singh, N. Impact of nutrition and health counselling on quality of life in celiac children aged 7–12 years as reported by parents. Nutr. Food Sci. 2019, 49, 62–74. [Google Scholar] [CrossRef]
- Zarkadas, M.; Dubois, S.; MacIsaac, K.; Cantin, I.; Rashid, M.; Roberts, K.C.; La Vieille, S.; Godefroy, S.; Pulido, O.M. Living with coeliac disease and a gluten-free diet: A Canadian perspective. J. Hum. Nutr. Diet. 2013, 26, 10–23. [Google Scholar] [CrossRef]
- Casellas, F.; Rodrigo, L.; Molina-Infante, J.; Vivas, S.; Lucendo, A.J.; Rosinach, M.; Dueñas, C.; Fernández-bañares, F.; López-Vivancos, J. Transcultural adaptation and validation of the Celiac Disease Quality of Life Transcultural adaptation and validation of the Celiac Disease Quality of Life ( CD-QOL ) survey, a specific questionnaire to measure quality of life in patients with celiac dis. Rev. Espanõla Enferm. Dig. 2013, 105, 585–593. [Google Scholar] [CrossRef] [Green Version]
- Zingone, F.; Iavarone, A.; Tortora, R.; Imperatore, N.; Pellegrini, L.; Russo, T.; Dorn, S.D.; Ciacci, C. The italian translation of the celiac disease-specific quality of life scale in celiac patients on gluten free diet. Dig. Liver Dis. 2013, 45, 115–118. [Google Scholar] [CrossRef]
- Aksan, A.; Mercanlıgil, S.M.; Häuser, W.; Karaismailoğlu, E. Validation of the Turkish version of the Celiac Disease Questionnaire (CDQ). Health Qual. Life Outcomes 2015, 13, 82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pratesi, C.B.; Häuser, W.; Uenishi, R.H.; Selleski, N.; Nakano, E.Y.; Gandolfi, L.; Pratesi, R.; Zandonadi, R.P. Quality of life of celiac patients in Brazil: Questionnaire translation, cultural adaptation and validation. Nutrients 2018, 10, 1167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, S.; Akbari, M.; Vanga, R.; Kelly, C.P.; Hansen, J.; Theethira, T.; Tariq, S.; Dennis, M.; Leffler, D.A. Patient perception of treatment burden is high in celiac disease compared with other common conditions. Am. J. Gastroenterol. 2014, 109, 1304–1311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Häuser, W.; Gold, J.; Stein, J.; Caspary, W.F.; Stallmach, A. Health-related quality of life in adult coeliac disease in Germany: Results of a national survey. Eur. J. Gastroenterol. Hepatol. 2006, 18, 747–753. [Google Scholar]
- Pouchot, J.; Despujol, C.; Malamut, G.; Ecosse, E.; Coste, J.; Cellier, C. Validation of a French version of the quality of life “celiac disease questionnaire”. PLoS ONE 2014, 9, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Marchese, A.; Klersy, C.; Biagi, F.; Balduzzi, D.; Bianchi, P.I.; Trotta, L.; Vattiato, C.; Zilli, A.; Rademacher, J.; Andrealli, A.; et al. Quality of life in coeliac patients: Italian validation of a coeliac questionnaire. Eur. J. Intern. Med. 2013, 24, 87–91. [Google Scholar] [CrossRef]
- Nachman, F.; del Campo, M.P.; González, A.; Corzo, L.; Vázquez, H.; Sfoggia, C.; Smecuol, E.; Sánchez, M.I.P.; Niveloni, S.; Sugai, E.; et al. Long-term deterioration of quality of life in adult patients with celiac disease is associated with treatment noncompliance. Dig. Liver Dis. 2010, 42, 685–691. [Google Scholar] [CrossRef]
- Nachman, F.; Mauriño, E.; Vázquez, H.; Sfoggia, C.; Gonzalez, A.; Gonzalez, V.; del Campo, M.P.; Smecuol, E.; Niveloni, S.; Sugai, E.; et al. Quality of life in celiac disease patients. Prospective analysis on the importance of clinical severity at diagnosis and the impact of treatment. Dig. Liver Dis. 2009, 41, 15–25. [Google Scholar] [CrossRef]
- Rodríguez Almagro, J.; Hernández Martínez, A.; Lucendo, A.J.; Casellas, F.; Solano Ruiz, M.C.; Siles González, J. Health-related quality of life and determinant factors in celiac disease. A population-based analysis of adult patients in Spain. Rev. Española Enferm. Dig. 2016, 108, 181–189. [Google Scholar] [CrossRef] [Green Version]
- Guillemin, F.; Bombardier, C.; Beaton, D. Cross-cultural adaptation of health-related quality of life measures: Literature review and proposed guidelines. J. Clin. Epidemiol. 1993, 46, 1417–1432. [Google Scholar] [CrossRef]
- Okoli, C.; Pawlowski, S.D. The delphi method as a research tool: An example, design considerations and applications. Inf. Manag. 2004, 42, 15–29. [Google Scholar] [CrossRef] [Green Version]
- Skulmoski, G.J.; Hartman, F.T. The delphi method for graduate research. J. Inf. Technol. Educ. 2007, 6, 1–21. [Google Scholar] [CrossRef]
- de Lima, T.C.; Gallani, M.C.B.J.; de Freitas, M.I.P. Content validation of an instrument to characterize people over 50 years of age living with human immunodeficiency virus/acquired immunodeficiency syndrome. Acta Paul. Enferm. 2012, 25, 4–10. [Google Scholar] [CrossRef] [Green Version]
- Farage, P.; Zandonadi, R.P.; Ginani, V.C.; Gandolfi, L.; Pratesi, R.; Nobrega, Y.K.M. Content validation and semantic evaluation of a check-list elaborated for the prevention of gluten cross-contamination in food services. Nutrients 2017, 9, 36. [Google Scholar] [CrossRef]
- Norman, G.R.; Sloan, J.A.; Wyrwich, K.W. Interpretation of changes in health-related quality of life. Med. Care 2003, 41, 582–592. [Google Scholar] [CrossRef]
- Spilker, B. Quality of Life and Pharmacoeconomics in Clinical Trials, 2nd ed.; Lippincott-Raven Publishers: Philadelphia, PA, USA, 1996; Volume 1. [Google Scholar]
- Streiner, D.L. Starting at the beginning: An introduction to coefficient alpha and internal consistency starting at the beginning: An introduction to coefficient alpha and internal consistency. J. Personal. Assess. 2003, 80, 99–103. [Google Scholar] [CrossRef]
- World Health Organization. The Third Ten Years of the World Health Organization, 1st ed.; WHO: Geneva, Switzerland, 2008; ISBN 9789241563666. [Google Scholar]
- Zarkadas, M.; Cranney, A.; Case, S.; Molloy, M.; Switzer, C.; Graham, I.D.; Butzner, J.D.; Rashid, M.; Warren, R.E.; Burrows, V. The impact of a gluten-free diet on adults with coeliac disease: Results of a national survey. J. Hum. Nutr. Diet. 2006, 19, 41–49. [Google Scholar] [CrossRef]
- Lee, A.; Newman, J.M. Celiac diet: Its impact on quality of life. J. Am. Diet. Assoc. 2003, 103, 1533–1535. [Google Scholar] [CrossRef]
- Gadelha de Mattos, Y.; Puppin Zandonadi, R.; Gandolfi, L.; Pratesi, R.; Yoshio Nakano, E.; Pratesi, C. Self-reported non-celiac gluten sensitivity in Brazil: Translation, cultural adaptation, and validation of italian questionnaire. Nutrients 2019, 11, 781. [Google Scholar] [CrossRef] [Green Version]
- Sverker, A.; Hensing, G.; Hallert, C. ‘Controlled by food’ lived experiences of coeliac disease. J. Hum. Nutr. Diet. 2005, 18, 171–180. [Google Scholar] [CrossRef]
- Hallert, C.; Grännö, C.; Hultén, S.; Midhagen, G.; Ström, M.; Svensson, H.; Valdimarsson, T. Living with coeliac disease: Controlled study of the burden of illness. Scand. J. Gastroenterol. 2002, 37, 39–42. [Google Scholar] [CrossRef] [PubMed]
- Hallert, C.; Sandlund, O.; Broqvist, M. Perceptions of health-related quality of life of men and women living with coeliac disease. Scand. J. Caring Sci. 2003, 17, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Tovoli, F. Clinical and diagnostic aspects of gluten related disorders. World J. Clin. Cases 2015, 3, 275. [Google Scholar] [CrossRef] [PubMed]
- Barker, J.M.; Liu, E. Celiac disease: Pathophysiology, clinical manifestations, and associated autoimmune conditions. Adv. Pediatrics 2008, 55, 349–365. [Google Scholar] [CrossRef] [Green Version]
- Jacobsson, L.R.; Friedrichsen, M.; Göransson, A.; Hallert, C. Impact of an active patient education program on gastrointestinal symptoms in women with celiac disease following a gluten-free diet. Gastroenterol. Nurs. 2012, 35, 200–206. [Google Scholar] [CrossRef]
- Cabrera-Chávez, F.; Dezar, G.V.; Islas-Zamorano, A.P.; Espinoza-Alderete, J.G.; Vergara-Jiménez, M.J.; Magaña-Ordorica, D.; Ontiveros, N. Prevalence of Self-Reported Gluten Sensitivity and Adherence to a Gluten-Free Diet in Argentinian Adult Population. Nutrients 2017, 9, 81. [Google Scholar] [CrossRef]
- Congreso de la Nacion Argentina. Ley 26588/2009; Boletín Nacional: Buenos Aires, Argetina, 2009; pp. 1–2.
- Congreso de la Nacion Argentina. Ley 27196/2015; Boletín Nacional: Buenos Aires, Argetina, 2015; pp. 1–2.
- Landau, E. In therapy? In Argentina, it’s the norm. Available online: http://edition.cnn.com/2013/04/28/health/argentina-psychology-therapists/index.html (accessed on 19 May 2020).
- Davidson, D.J.; Freudenburg, W.R. Gender and environmental risk concerns: A review and analysis of available research. Environ. Behav. 1996, 28, 302–339. [Google Scholar] [CrossRef]
- Internet World Stats. Argentina Internet Usage Stats and Telecommunications Reports. Available online: https://www.internetworldstats.com/sa/ar.htm (accessed on 19 May 2020).
- Argentina.gob.ar WiFi País Digital. Available online: https://www.argentina.gob.ar/jefatura/innovacion-publica/gobierno-abierto-y-pais-digital/wifi (accessed on 19 May 2020).


{kind=link}
| Mean (SD) | Median (IQR) | Range | Floor Effect (%) | Ceiling Effect (%) | Internal Consistency (Alpha Cronbach) | |
|---|---|---|---|---|---|---|
| Emotional | 26.07 (10.38) | 24 (18–34) | 7–49 | 0% | 1% | 0.922 |
| Social | 35.8 (9.25) | 37 (28–44) | 10–49 | 0% | 6% | 0.832 |
| Worries | 28.82 (10.11) | 28 (31–37) | 7–49 | 0% | 1% | 0.771 |
| Gastrointestinal | 33.77 (9.24) | 34 (27–41) | 9–49 | 0% | 3% | 0.849 |
| Total Score | 124.14 (32.44) | 123 (99–149) | 34–96 | 0% | 0% | 0.934 |
| Emotion | Social | Worries | Gastrointestinal | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean (SD) | p | Mean (SD) | p | Mean (SD) | p | Mean (SD) | p | Mean (SD) | p | |
| Gender * | ||||||||||
| Female (n = 149) | 25.12 (10.16) | <0.001 | 35.26 (3.38) | 0.079 | 28.48 (10.16) | 0.298 | 33.02 (9.32) | 0.001 | 121.73 (32.44) | 0.006 |
| Male (n = 18) | 34.11 (9.49) | 39.33 (7.84) | 31.25 (9.38) | 40.56 (5.36) | 145.19 (26.45) | |||||
| Present Age * | ||||||||||
| ≤39 years (n = 112) | 25.67 (10.47) | 0.423 | 35.45 (9.12) | 0.568 | 28.24 (10.22) | 0.293 | 33.05 (9.34) | 0.134 | 121.82 (32.11) | 0.197 |
| ≥40 years (n = 58) | 27.02 (10.23) | 36.31 (9.53) | 29.98 (9.97) | 35.29 (8.95) | 128.70 (33.12) | |||||
| Age at diagnosis * | ||||||||||
| ≤30 years (n = 93) | 27.15 (10.84) | 0.103 | 36.06 (8.91) | 0.532 | 29.03 (10.67) | 0.750 | 33.51 (9.92) | 0.698 | 124.90 (33.96) | 0.645 |
| ≥31 years (n = 72) | 24.49 (9.68) | 35.14 (9.58) | 28.54 (9.17) | 34.06 (8.05) | 122.51 (30.44) | |||||
| Symptoms at diagnosis * | ||||||||||
| No (n = 40) | 24.02 (8.53) | 0.109 | 35.15 (9.34) | 0.607 | 28.22 (10.35) | 0.674 | 34.68 (7.60) | 0.480 | 122.08 (28.45) | 0.646 |
| Yes (n = 130) | 26.70 (10.84) | 36.02 (9.26) | 29.00 (10.07) | 33.49 (9.69) | 124.79 (33.69) | |||||
| College education * | ||||||||||
| No (n = 83) | 25.01 (10.83) | 0.228 | 34.99 (9.73) | 0.352 | 27.61 (10.35) | 0.124 | 32.57 (9.22) | 0.093 | 119.85 (33.40) | 0.118 |
| Yes (n = 82) | 26.98 (9.91) | 36.34 (8.61) | 30.03 (9.57) | 34.96 (8.92) | 127.86 (31.04) | |||||
| Marital status *,° | ||||||||||
| Stable relationship (n = 63) | 25.02 (10.84) | 0.395 | 34.97 (9.71) | 0.478 | 28.95 (10.38) | 0.894 | 33.33 (9.20) | 0.647 | 121.63 (34.29) | 0.516 |
| Not in a stable relationship (n = 101) | 26.44 (10.07) | 36.03 (8.91) | 28.74 (9.87) | 34.01 (9.16) | 125.07 (31.33) | |||||
| Gluten-free diet *, ± | ||||||||||
| No (n = 27) | 22.74 (9.32) | 0.067 | 33.59 (9.39) | 0.173 | 27.30 (10.20) | 0.352 | 28.33 (9.66) | <0.001 | 111.96 (32.71) | 0.029 |
| Yes (n = 141) | 26.75 (10.53) | 36.26 (9.23) | 29.27 (10.05) | 34.96 (8.71) | 126.91 (32.03) | |||||
| Celiac legislation: Aware of Legislation * | ||||||||||
| No (n = 41) | 21.46 (8.58) | <0.001 | 30.49 (7.94) | <0.001 | 23.70 (9.97) | <0.001 | 29.68 (8.82) | 0.001 | 103.87 (25.63) | <0.001 |
| Yes (n = 128) | 27.53 (10.54) | 37.39 (9.07) | 30.57 (9.53) | 35.23 (8.87) | 130.43 (31.86) | |||||
| Celiac legislation: Aware of benefits * | ||||||||||
| No (n = 111) | 24.51 (9.85) | 0.007 | 34.71 (9.13) | 0.040 | 27.62 (10.13) | 0.021 | 32.79 (9.26) | 0.032 | 118.98 (30.88) | 0.004 |
| Yes (n = 58) | 29.02 (10.88) | 37.79 (9.29) | 31.38 (9.49) | 35.97 (8.62) | 134.16 (33.26) | |||||
| Celiac legislation: uses of benefit? * | ||||||||||
| No (n = 136) | 25.67 (10.16) | 0.324 | 34.89 (9.39) | 0.012 | 28.46 (10.26) | 0.222 | 33.46 (9.43) | 0.220 | 122.34 (32.94) | 0.111 |
| Yes (n = 33) | 27.67 (11.40) | 39.39 (7.92) | 30.88 (9.00) | 35.64 (7.76) | 132.53 (29.46) | |||||
| Other chronic diseases * | ||||||||||
| No (n = 98) | 26.78 (10.80) | 0.303 | 36.28 (8.64) | 0.444 | 27.67 (9.52) | 0.086 | 34.05 (8.98) | 0.464 | 123.97 (31.07) | 0.937 |
| Yes (n = 72) | 25.11 (9.76) | 35.1 (10.06) | 30.38 (10.74) | 33.39 (9.63) | 124.37 (34.47) | |||||
| Use of antidepressants * | ||||||||||
| No (n = 158) | 26.39 (10.56) | 0.028 | 36.01 (9.36) | 0.361 | 28.71 (10.27) | 0.622 | 33.91 (9.33) | 0.470 | 124.66 (32.97) | 0.435 |
| Yes (n = 12) | 21.27 (6.33) | 33.36 (8.00) | 30.27 (7.81) | 31.82 (8.38) | 116.73 (23.68) | |||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Selleski, N.; Zandonadi, R.P.; Milde, L.B.; Gandolfi, L.; Pratesi, R.; Häuser, W.; Uenishi, R.H.; Nakano, E.Y.; Pratesi, C.B. Evaluation of Quality of Life of Adult Patients with Celiac Disease in Argentina: From Questionnaire Validation to Assessment. Int. J. Environ. Res. Public Health 2020, 17, 7051. https://doi.org/10.3390/ijerph17197051
Selleski N, Zandonadi RP, Milde LB, Gandolfi L, Pratesi R, Häuser W, Uenishi RH, Nakano EY, Pratesi CB. Evaluation of Quality of Life of Adult Patients with Celiac Disease in Argentina: From Questionnaire Validation to Assessment. International Journal of Environmental Research and Public Health. 2020; 17(19):7051. https://doi.org/10.3390/ijerph17197051
Chicago/Turabian StyleSelleski, Nicole, Renata Puppin Zandonadi, Laura B. Milde, Lenora Gandolfi, Riccardo Pratesi, Winfred Häuser, Rosa Harumi Uenishi, Eduardo Yoshio Nakano, and Claudia B. Pratesi. 2020. "Evaluation of Quality of Life of Adult Patients with Celiac Disease in Argentina: From Questionnaire Validation to Assessment" International Journal of Environmental Research and Public Health 17, no. 19: 7051. https://doi.org/10.3390/ijerph17197051