The Homeostatic Theory of Obesity: An Empirical Verification of the Circle of Discontent with an Assessment of Its Relationship to Restrained and Uncontrolled Eating among Children and Adolescents


Abstract
:1. Introduction
2. Materials and Methods
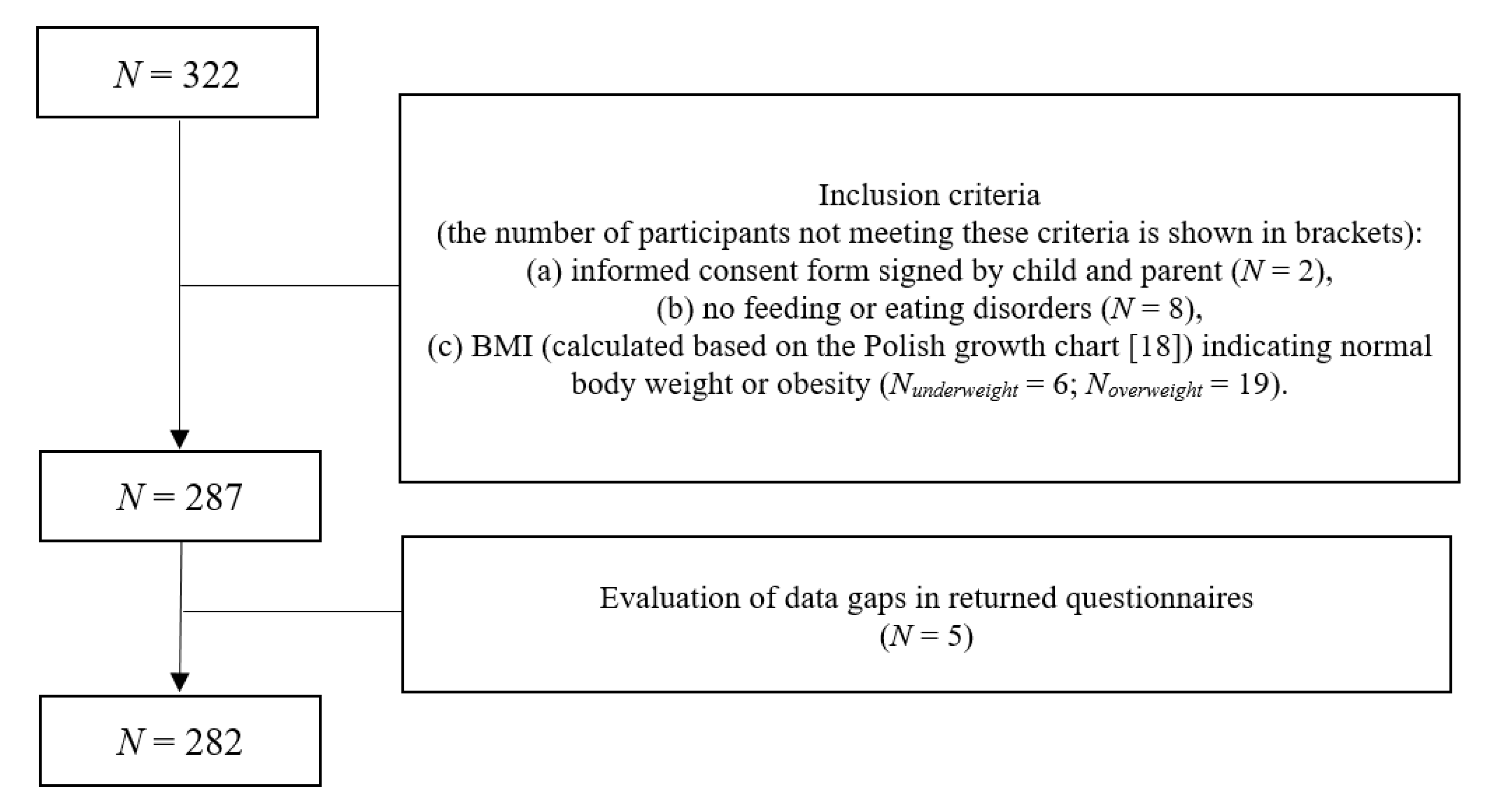
2.1. Participants
2.2. Measures
2.2.1. Negative Affect: Positive and Negative Affect Scale for Children (PANAS-C)
2.2.2. Body Dissatisfaction: Children’s Body Image Scale (Children) and Figure Rating Scale (Adolescents)
2.2.3. Uncontrolled and Restrictive Eating: Three-Factor Eating Questionnaire (TFEQ-R13)
2.2.4. Anthropometrical Status Based on BMI (Normal Body Weight vs. Obesity) and High-Energy Consumption: Sociodemographic Survey and Clinical Diagnosis
2.2.5. Feeding and Eating Disorders: Eating Disorders in Youth—Questionnaire (EDY-Q)
2.3. Procedure
2.4. Data Analysis
3. Results
3.1. Descriptive Statistics and Correlations
3.2. Empirical Verification of the Circle of Discontent and its Relationship to Restrained and Uncontrolled Eating Among Children and Adolescents
4. Discussion
4.1. Strengths
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AIC | Akaike information criterion |
| BIC | Bayesian information criterion |
| BMI | body mass index |
| CFI | comparative fit index |
| COD | Circle of Discontent |
| df | degrees of freedom |
| DSM-5 | Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition |
| EDY-Q | Eating Disorders in Youth—Questionnaire |
| GLS | generalized least squares |
| M | mean |
| N | sample size |
| NA | negative affect |
| p | probability value |
| PA | positive affect |
| PANAS-C | Positive and Negative Affect Scale for Children |
| RMSEA | root mean square error of approximation |
| SD | standard deviation |
| SRMR | standardized root mean square residual |
| TFEQ-R13 | Three-Factor Eating Questionnaire |
| χ2 | chi-square statistic |
References
- Sahoo, K.; Sahoo, B.; Choudhury, A.K.; Sofi, N.Y.; Kumar, R.; Bhadoria, A.S. Childhood obesity: Causes and consequences. J. Fam. Med. Prim. Care 2015, 4, 187–192. [Google Scholar] [CrossRef]
- World Health Organization 2020. Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 3 June 2020).
- Kułaga, Z.; Grajda, A.; Gurzkowska, B. The prevalence of overweight and obesity among polish school-aged children and adolescents. Przegl. Epidemiol. 2016, 70, 641–651. [Google Scholar] [PubMed]
- World Health Organization. Reducing Childhood Obesity in Poland by Effective Policies. 2017. Available online: http://www.euro.who.int/__data/assets/pdf_file/0011/350030/Reducing-childhood-obesity-in-Poland_final_WEB.pdf?ua=1 (accessed on 3 June 2020).
- Marks, D.F. Homeostatic theory of obesity. Health Psychol. Open 2015, 2, 2055102915590692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ames, S.L.; Kisbu-Sakarya, Y.; Reynolds, K.D.; Boyle, S.; Cappelli, C.; Cox, M.G.; Dust, M.; Grenard, J.L.; Mackinnon, D.P.; Stacy, A.W. Inhibitory control effects in adolescent binge eating and consumption of sugar-sweetened beverages and snacks. Appetite 2014, 81, 180–192. [Google Scholar] [CrossRef] [Green Version]
- Czepczor-Bernat, K.; Brytek-Matera, A. Children’s and mothers’ perspectives of problematic eating behaviours in young children and adolescents: An exploratory study. Int. J. Environ. Res. Public Health 2019, 16, 2692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Figueiredo, R.A.O.; Simola-Ström, S.; Isomaa, R.; Weiderpass, E. Body dissatisfaction and disordered eating symptoms in Finnish preadolescents. Eat. Disord. 2019, 27, 34–51. [Google Scholar] [CrossRef]
- Ledoux, T.; Adamus-Leach, H.; O’Connor, D.P.; Mama, S.; Lee, R.E. The association of binge eating and neighbourhood fast-food restaurant availability on diet and weight status. Public Health Nutr. 2015, 18, 352–360. [Google Scholar] [CrossRef]
- Ribeiro-Silva, R.C.; Fiaccone, R.L.; Conceição-Machado, M.E.P.D.; Ruiz, A.S.; Barreto, M.L.; Santana, M.L.P. Body image dissatisfaction and dietary patterns according to nutritional status in adolescents. J. Pediatr. (Rio J.) 2018, 94, 155–161. [Google Scholar] [CrossRef]
- Rodgers, R.F.; McLean, S.A.; Marques, M.; Dunstan, C.J.; Paxton, S.J. Trajectories of body dissatisfaction and dietary restriction in early adolescent girls: A latent class growth analysis. J. Youth Adolesc. 2016, 45, 1664–1677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agras, W.S.; Robinson, A. The Oxford Handbook of Eating Disorders, 2nd ed.; Oxford Univesity Press: New York, NY, USA, 2018; pp. 155–186. [Google Scholar]
- Booth, C.; Spronk, D.; Grol, M.; Fox, E. Uncontrolled eating in adolescents: The role of impulsivity and automatic approach bias for food. Appetite 2018, 120, 636–643. [Google Scholar] [CrossRef] [PubMed]
- Instytut “Pomnik-Centrum Zdrowia Dziecka”. Siatki centylowe dzieci i młodzieży w wieku 3–18 lat [Centile Grids of Children and Adolescents Aged 3–18 Years]. Available online: http://www.czd.pl/index.php?option=com_content&view=article&id=1717&Itemid=538 (accessed on 3 June 2020).
- WHO. AnthroPlus Software. Available online: https://www.who.int/growthref/tools/en/ (accessed on 3 June 2020).
- Laurent, J.; Cantanzaro, S.; Joiner, T.E.J.; Rudolph, K.D.; Potter, K.I.; Lambert, S.; Osborne, S.; Gathright, T. A measure of positive and negative affect for children: Scale development and preliminary validation. Psychol. Assess. 1999, 11, 326–338. [Google Scholar] [CrossRef]
- Wróbel, M.; Finogenow, M.; Szymańska, P.; Laurent, J. Measuring positive and negative affect in a school-based sample: A polish version of the PANAS-C. J. Psychopathol. Behav. Assess. 2019, 41, 598–611. [Google Scholar] [CrossRef] [Green Version]
- Childress, A.C.; Brewerton, T.D.; Hodges, E.L.; Jarrell, P.M. The Kids’ Eating Disorders Survey (KEDS): A study of middle school students. J. Am. Acad. Child. Adolesc. Psychiatry 1993, 32, 843–850. [Google Scholar] [CrossRef] [PubMed]
- Stunkard, A.; Sorensen, T.; Schulsinger, F. Use of the Danish Adoption Register for the study of obesity and thinness. Res. Publ. Assoc. Res. Nerv. Ment. Dis. 1983, 60, 115–120. [Google Scholar] [PubMed]
- Truby, H.; Paxton, S.J. Development of the Children’s body image scale. Br. J. Clin. Psychol. 2002, 41, 185–203. [Google Scholar] [CrossRef] [PubMed]
- Dzielska, A.; Mazur, J.; Małkowska-Szkutnik, A.; Nelcz, H. Adaptacja polskiej wersji kwestionariusza Three-Factor Eating Questionnaire (TFEQ-13) wśród młodzieży szkolnej w badaniach populacyjnych. Probl. Hig. Epidemiol. 2009, 90, 362–369. [Google Scholar]
- Hilbert, A.; van Dyck, Z. Eating Disorders in Youth Questionnaire English Version. Available online: http://ul.qucosa.de/api/qucosa%3A14486/attachment/ATT-0/ (accessed on 3 June 2020).
- American Psychiatric Association. DSM-5: Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Arlington, VA, USA, 2013. [Google Scholar]
- Byrne, B. Structural Equation Modeling with AMOS. Basic Concepts, Applications, and Programming, 2nd ed.; Routledge: New York, NY, USA; London, UK, 2010. [Google Scholar]
- Cruz-Sáez, S.; Pascual, A.; Salaberria, K.; Echeburúa, E. Normal-weight and overweight female adolescents with and without extreme weight-control behaviours: Emotional distress and body image concerns. J. Health Psychol. 2015, 20, 730–740. [Google Scholar] [CrossRef] [Green Version]
- Marcus, M.D.; Wing, R.R.; Lamparski, D.M. Binge eating and dietary restraint in obese patients. Addict. Behav. 1985, 10, 163–168. [Google Scholar] [CrossRef]
- Polivy, J.; Herman, C.P. Distress and eating: Why do dieters overeat? Int. J. Eat. Disord. 1999, 26, 153–164. [Google Scholar] [CrossRef]
- De Lauzon-Guillain, B.; Romon, M.; Musher-Eizenman, D.; Heude, B.; Basdevant, A.; Charles, M.A.; Fleurbaix-Laventie Ville Santé Study Group. Cognitive restraint, uncontrolled eating and emotional eating: Correlations between parent and adolescent. Matern. Child. Nutr. 2009, 5, 171–178. [Google Scholar] [CrossRef] [Green Version]
- Johnson, F.; Wardle, J. Dietary restraint, body dissatisfaction, and psychological distress: A prospective analysis. J. Abnorm. Psychol. 2005, 114, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Rossy, L. The Mindfulness-Based Eating Solution: Proven Strategies to End Overeating, Satisfy Your Hunger, and Savor Your Life; New Harbinger Publications: Oakland, CA, USA, 2016. [Google Scholar]
- Theim, K.R.; Tanofsky-Kraff, M.; Salaita, C.G.; Haynos, A.F.; Mirch, M.C.; Ranzenhofer, L.M.; Yanovski, S.Z.; Wilfley, D.E.; Yanovski, J.A. Children’s descriptions of the foods consumed during loss of control eating episodes. Eat. Behav. 2007, 8, 258–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Emond, J.A.; Longacre, M.R.; Titus, L.J.; Hendricks, K.; Drake, K.M.; Carroll, J.E.; Cleveland, L.P.; Dalton, M.A. Fast food intake and excess weight gain over a 1-year period among preschool-age children. Pediatr. Obes. 2020. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, J.A.; Manson, J.E.; Buijsse, B.; Wang, L.; Allison, M.A.; Neuhouser, M.L.; Tinker, L.; Waring, M.E.; Isasi, C.R.; Martin, L.W.; et al. Chocolate-candy consumption and 3-year weight gain among postmenopausal U.S. women. Obesity (Silver Spring) 2015, 23, 677–683. [Google Scholar] [CrossRef] [PubMed]
- Larson, N.; Story, M. A review of snacking patterns among children and adolescents: What are the implications of snacking for weight status? Child. Obes. 2013, 9, 104–115. [Google Scholar] [CrossRef] [PubMed]
- Honicky, M.; Cardoso, S.M.; de Lima, L.R.A.; Ozcariz, S.; Vieira, F.; de Carlos Back, I.; Moreno, Y. Added sugar and trans fatty acid intake and sedentary behavior were associated with excess total-body and central adiposity in children and adolescents with congenital heart disease. Pediatr. Obes. 2020, 15, e12623. [Google Scholar] [CrossRef]
- Kivimäki, M.; Head, J.; Ferrie, J.E.; Shipley, M.J.; Brunner, E.; Vahtera, J.; Marmot, M.G. Work stress, weight gain and weight loss: Evidence for bidirectional effects of job strain on body mass index in the Whitehall II study. Int. J. Obes. (Lond.) 2006, 30, 982–987. [Google Scholar] [CrossRef] [Green Version]
- Shroff, M.R.; Perng, W.; Baylin, A.; Mora-Plazas, M.; Marin, C.; Villamor, E. Adherence to a snacking dietary pattern and soda intake are related to the development of adiposity: A prospective study in school-age children. Public Health Nutr. 2014, 17, 1507–1513. [Google Scholar] [CrossRef] [Green Version]
- Njike, V.Y.; Smith, T.M.; Shuval, O.; Edshteyn, I.; Kalantari, V.; Yaroch, A.L. Snack food, satiety, and weight. Adv. Nutr. 2016, 7, 866–878. [Google Scholar] [CrossRef] [Green Version]
- Zhu, Z.; He, Y.; Wang, Z.; He, X.; Zang, J.; Guo, C.; Jia, X.; Ren, Y.; Shan, C.; Sun, J.; et al. The associations between sugar-sweetened beverage intake and cardiometabolic risks in Chinese children and adolescents. Pediatr. Obes. 2020, e12634. [Google Scholar] [CrossRef]
- McGale, L.S.; Smits, T.; Halford, J.C.G.; Harrold, J.A.; Boyland, E.J. The influence of front-of-pack portion size images on children’s serving and intake of cereal. Pediatr. Obes. 2020, 15, e12583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wouters, S.; Jacobs, N.; Duif, M.; Lechner, L.; Thewissen, V. Negative affective stress reactivity: The dampening effect of snacking. Stress. Health 2018, 34, 286–295. [Google Scholar] [CrossRef] [PubMed]
- Wouters, S.; Jacobs, N.; Duif, M.; Lechner, L.; Thewissen, V. Affect and between-meal snacking in daily life: The moderating role of gender and age. Psychol. Health 2018, 33, 555–572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malik, V.; Willett, W.; Hu, F. Global obesity: Trends, risk factors and policy implications. Nat. Rev. Endocrinol. 2013, 9, 13–27. [Google Scholar] [CrossRef] [PubMed]
- Dobbs, R.; Sawers, C.; Thompson, F.; Manyika, J.; Woetzel, J.; Child, P.; McKenna, S.; Spatharo, A. Overcoming Obesity: An Initial Economic Analysis. Available online: https://www.mckinsey.com/~/media/McKinsey/Business%20Functions/Economic%20Studies%20TEMP/Our%20Insights/How%20the%20world%20could%20better%20fight%20obesity/MGI_Overcoming_obesity_Full_report.ashx (accessed on 3 June 2020).
- Skrypnik, D.; Bogdański, P.; Zawiejska, A.; Wender-Ożegowska, E. Role of gestational weight gain, gestational diabetes, breastfeeding, and hypertension in mother-to-child obesity transmission. Pol. Arch. Intern. Med. 2019, 129, 267–275. [Google Scholar] [CrossRef] [Green Version]
- Skrypnik, D.; Bogdański, P.; Skrypnik, K.; Mądry, E.; Karolkiewicz, J.; Szulińska, M.; Suliburska, J.; Walkowiak, J. Influence of endurance and endurance–strength training on mineral status in women with abdominal obesity. Medicine 2019, 98, e14909. [Google Scholar] [CrossRef]
- Szulińska, M.; Skrypnik, D.; Ratajczak, M.; Karolkiewicz, J.; Madry, E.; Musialik, K.; Walkowiak, J.; Jakubowski, H.; Bogdański, P. Effects of endurance and endurance-strength exercise on renal function in abdominally obese women with Renal Hyperfiltration: A prospective randomized trial. Biomed. Environ. Sci. 2016, 29, 706–712. [Google Scholar] [CrossRef]
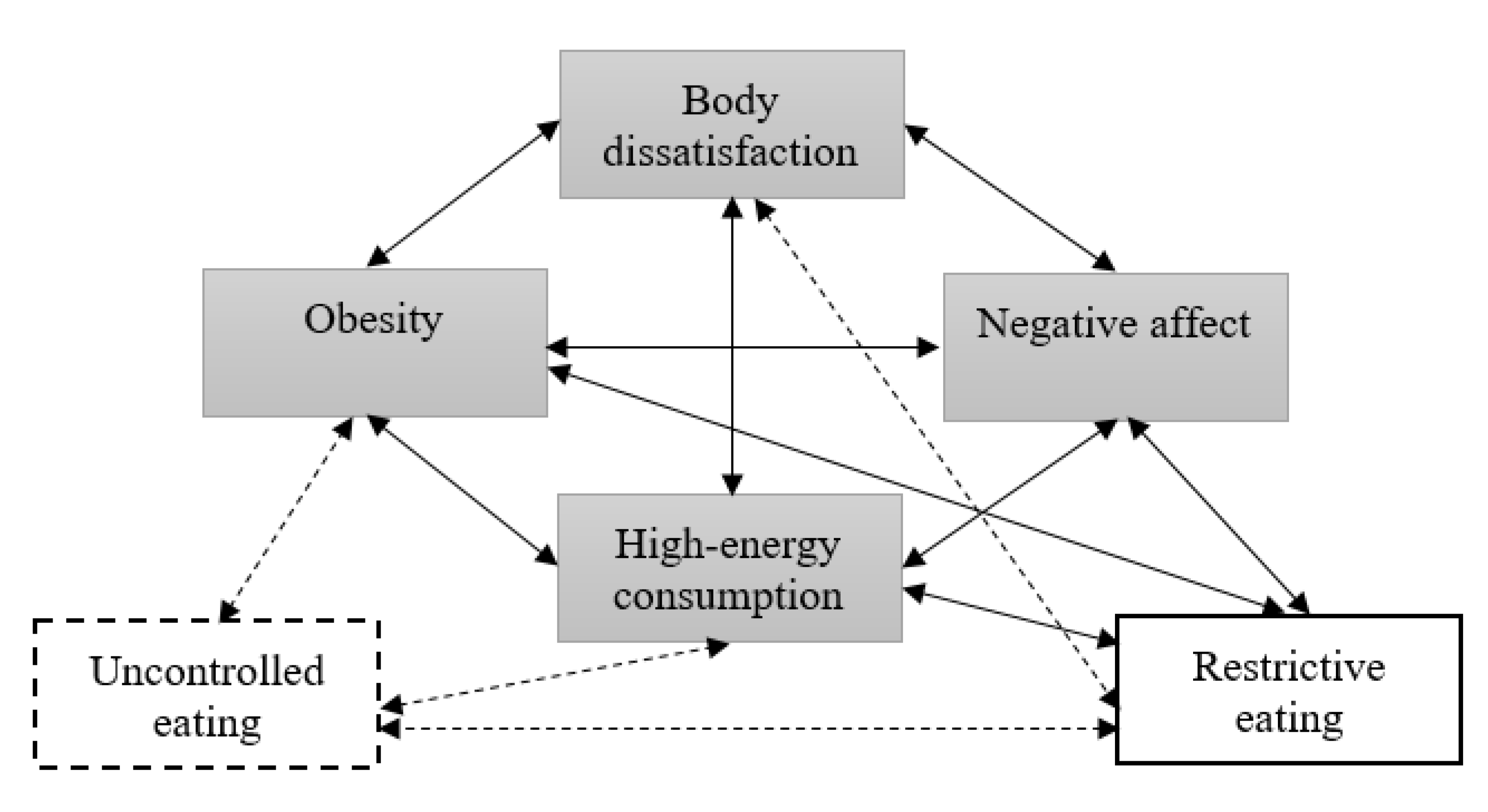
 the variables from the Circle of Discontent;
the variables from the Circle of Discontent;  a variable from Homeostatic Theory of Obesity whose relationship with COD was described by Marks;
a variable from Homeostatic Theory of Obesity whose relationship with COD was described by Marks;  a new variable (proposed to be tested by the authors);
a new variable (proposed to be tested by the authors);  relationships described by Marks;
relationships described by Marks;  new relationships (proposed to be tested by the authors).
the variables from the Circle of Discontent; a variable from Homeostatic Theory of Obesity whose relationship with COD was described by Marks; a new variable (proposed to be tested by the authors); relationships described by Marks; new relationships (proposed to be tested by the authors).
new relationships (proposed to be tested by the authors).
the variables from the Circle of Discontent; a variable from Homeostatic Theory of Obesity whose relationship with COD was described by Marks; a new variable (proposed to be tested by the authors); relationships described by Marks; new relationships (proposed to be tested by the authors).

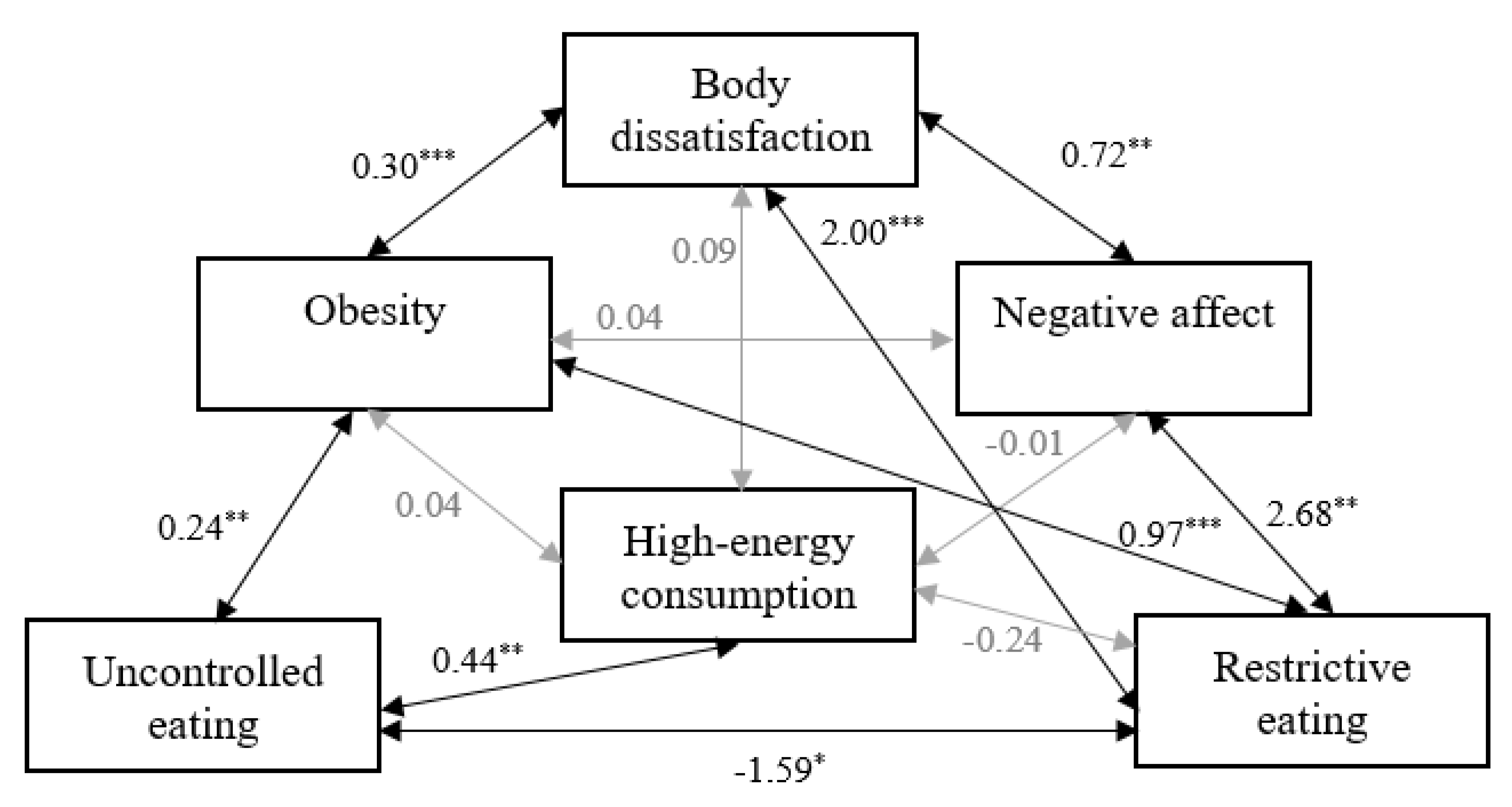
 a significant relationship;
a significant relationship;  a non-significant relationship.
a significant relationship; a non-significant relationship.
a non-significant relationship.
a significant relationship; a non-significant relationship.

{kind=link}
{kind=link}
{kind=link}
| Normal Body Weight N = 141 | Obesity N = 141 | ||
|---|---|---|---|
| N (%) | p | ||
| Sex 1 | >0.05 | ||
| Female | 76 (53.90) | 72 (51.06) | |
| Male | 65 (46.10) | 69 (48.94) | |
| M (SD) | |||
| Age | 11.72 (2.74) | 12.73 (2.77) | >0.05 |
| Weight | 46.80 (17.84) | 71.06 (22.47) | <0.001 |
| Height | 153.24 (17.15) | 159.44 (15.34) | <0.01 |
| BMI 2 | 19.26 (4.31) | 27.32 (5.26) | <0.001 |
| BMI z-score 3 | 0.25 (1.38) | 2.34 (0.96) | <0.001 |
| 2 | 3 | 4 | 5 | 6 | |
|---|---|---|---|---|---|
| 1. Negative affect | 0.177 ** | 0.075 | 0.172 ** | 0.032 | 0.009 |
| 2. Body dissatisfaction | 0.008 | 0.487 *** | 0.559 *** | 0.102 | |
| 3. Uncontrolled eating | −0.125 * | 0.154 ** | 0.168 ** | ||
| 4. Restrictive eating | 0.505 *** | −0.073 | |||
| 5. Obesity 1 | 0.087 | ||||
| 6. High-energy consumption 2 |
| χ2 | df | p | χ2/df | RMSEA 1 | pclose | SRMR | CFI | AIC 2 | BIC 3 |
|---|---|---|---|---|---|---|---|---|---|
| 1.60 | 2 | 0.449 | 0.80 | 0.00 | 0.655 | 0.02 | 0.99 | 39.60 | 40.57 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Czepczor-Bernat, K.; Brytek-Matera, A.; Matusik, P. The Homeostatic Theory of Obesity: An Empirical Verification of the Circle of Discontent with an Assessment of Its Relationship to Restrained and Uncontrolled Eating among Children and Adolescents. Int. J. Environ. Res. Public Health 2020, 17, 6028. https://doi.org/10.3390/ijerph17176028
Czepczor-Bernat K, Brytek-Matera A, Matusik P. The Homeostatic Theory of Obesity: An Empirical Verification of the Circle of Discontent with an Assessment of Its Relationship to Restrained and Uncontrolled Eating among Children and Adolescents. International Journal of Environmental Research and Public Health. 2020; 17(17):6028. https://doi.org/10.3390/ijerph17176028
Chicago/Turabian StyleCzepczor-Bernat, Kamila, Anna Brytek-Matera, and Paweł Matusik. 2020. "The Homeostatic Theory of Obesity: An Empirical Verification of the Circle of Discontent with an Assessment of Its Relationship to Restrained and Uncontrolled Eating among Children and Adolescents" International Journal of Environmental Research and Public Health 17, no. 17: 6028. https://doi.org/10.3390/ijerph17176028