People’s sexual health in every period of life has been arousing great interest among the researchers of many scientific disciplines for years. However, there are few publications discussing the aspect of sexuality during pregnancy. The available studies differ mainly in terms of research methods and instruments used in them, as well as the religious, cultural, social, and ideological aspects. In the study conducted by Aydin et al. [
4], using the Female Sexual Function Index (FSFI), as many as 91% of pregnant women met the criteria for sexual dysfunction compared with 68% of non-pregnant women. Such a large percentage of pregnant women with sexual disorders (including lust, arousal, orgasm, or sexual pain) should be an impulse for modern medicine to meet the expectations of women [
5]. In our study, pregnant women showing a high overall level of sexual satisfaction (7–10 sten) constituted only 42.54% (77) of all participants, while 40 (22.10%) women had a low level of sexual satisfaction (1–4 sten). Different results were reported by Huras et al., who informed that only 13% of women were fully satisfied, and 25% were dissatisfied with their sexual life in pregnancy [
6]. Other authors compared pregnant and non-pregnant women, determining that the levels of satisfaction (91.08% vs. 67.61%,
p = 0.0001) and desire (51.52% vs. 48.48%,
p < 0.001) were higher in the second group of women [
4,
7]. Sexual satisfaction is undoubtedly an important element indicating sexual well-being or the lack of it, as well as the overall quality of life [
8]. In their study of 5582 adults of different sexes and ages, Schmiedeberg et al. observed a relationship between the level of sexual satisfaction and the level of life satisfaction [
9]. We noticed that this tendency also continues during pregnancy. A higher level of satisfaction with life was associated with a higher level of overall sexual satisfaction (
p < 0.001), a higher level of satisfaction with closeness (
p < 0.01), a higher level of satisfaction with caress (
p < 0.05), and a higher level of satisfaction with sex (
p < 0.001). Similar results were reported by Ferreira et al., who found that women with a low quality of life also had a low level of sexual satisfaction [
10]. Physical and emotional changes occurring in this period may result in a decline in the level of life satisfaction and the frequency of sexual activity. The majority of women in our study reported the decreased frequency of intercourse compared to the state before pregnancy (74.59%), however, it affected more often women who were in their first pregnancy (
p < 0.05). Parity had no impact on the level of sexual satisfaction in pregnancy (
p > 0.05). A decrease in sexual activity was also noted by Sossah, who claimed that the most common reason for reducing the frequency of intercourse during pregnancy was the belief that it can lead to miscarriage [
11]. The research conducted in Taiwan has shown that more than half of women thought that pregnancy sex can be dangerous and cause fetal damage [
12]. In our investigation, concern for the baby came second on the list of reasons for reducing the frequency of sexual intercourse (28.15%), while the reason that came first was pregnancy complaints (44.44%). The women also felt less attractive (38; 28.15%) and received less interest from their partners (31; 22.96). The frequency of intercourse before pregnancy was also studied by Yeniel A. O. and Petri E., Makara-Studzińska M. et al., Navidian A. et al., and Beiranvand S. P. et al. All these authors reported a reduction in the amount of sexual activity compared to pre-pregnancy levels [
13,
14,
15,
16]. Both shifting the age limit at which adults decide to have a child, and conscious childlessness ceased to be considered as unusual. However, the problem of infertility among couples and planning offspring can be associated with a sense of pressure from the family or the environment. Many people of reproductive age live in a hurry, strive for self-development, and pursue a professional career. A small percentage of respondents (10.50%) observed an increase in the frequency of intercourse during pregnancy, which was mostly due to mental comfort, understood as the lack of pressure associated with trying to have a baby and less workload. Completely different reasons for undertaking sexual activity in this period are mentioned by Bello F.A. They include maintaining harmony in marriage and accelerating delivery [
17]. It is also interesting that pregnant women showing an increase in sexual activity felt more attractive (63.16%). This suggests that the sense of attractiveness at every stage of life has a huge impact on sexual satisfaction and the frequency of intercourse. Kucharska et al. demonstrated that pregnant women and those who used to be pregnant have a high level of sex appeal and have a positive attitude towards intercourse during this period [
18]. Pauleta et al. asserts that as many as 41.5% of women felt less attractive during pregnancy [
19]. The awareness of physical and emotional changes occurring in this period could have a positive effect on the self-esteem of pregnant women. Isajeva et al. revealed that except for sexual desire, which remains the same, all other parameters are reduced during pregnancy. Available studies prove that sexuality in pregnancy differs not only from that before pregnancy, but also in individual trimesters [
20,
21]. This is associated with the dynamic changes occurring in the subsequent stages of pregnancy. The emotional states in the first and the third trimesters of pregnancy seem to be particularly important. Gałązka et al. observed that the decrease in anxiety in the second trimester contributes to higher sexual activity [
22]. Huras et al. indicated that the libido of pregnant women significantly decreases in the first and the third trimesters of pregnancy compared to the period before pregnancy. This physiological change probably results in a decrease in sexual activity during this period [
6]. In our study, there was no statistically significant relationship between the general sexual satisfaction and the trimester of pregnancy (
p < 0.05). This relationship was noted by Dafna et al., who found that pleasure from sexual activity decreases with increasing pregnancy [
7]. The last trimester of pregnancy is special due to the approaching date of delivery and the resulting fear of pain, previous negative experiences related to delivery, and economic uncertainty. Almost every woman feels the fear of giving birth. Our analysis showed that the level of life satisfaction in pregnant women (
p < 0.05) decreases as pregnancy progresses. The same results were presented by Kang et al., proving that the decrease in life satisfaction in the last trimester has to do with growing antenatal anxiety during this period [
23]. However, there are methods to prevent anxiety growing in the third trimester and its effects, namely proper preparation for childbirth (e.g., at antenatal classes), and social support [
24]. Gebuza et al. emphasize the importance of support received by a pregnant woman in the last trimester of pregnancy, also showing that it positively affects her assessment of life satisfaction [
25]. Taking care of health and physical activity in the periconceptional and perinatal periods are also factors that affect female sexuality. An important part is played by pelvic floor muscles that are responsible for the functioning of the organs within them. Healthy, fit muscles allow a woman to derive satisfaction from intercourse, because well upplied tissue is better innervated, which allows deeper sensations and enhances sexual activity. Unexercised muscles are weakened and slowly degrade. Due to their biological functions, such as pregnancy and childbirth, women are particularly vulnerable to muscle dysfunctions, which substantially worsen the quality of life, as they contribute to limiting sexual intercourse or even giving up sexual contacts, which often causes the weakening of marriage ties. It has been demonstrated that pregnant women who were doing Kegel’s exercises had a higher level of sexual satisfaction in the dimensions of closeness (
p < 0.05) and caress (
p < 0.05). Based on her study of 726 women, Kocur D. concluded that women who regularly exercise these muscle parts more often reach orgasm [
26]. According to this author, 80% of the respondents knew where the pelvic floor muscles were, 73% knew their functions, but only half of the women surveyed had ever exercised them. In addition, Modarres et al. described a positive effect of pelvic floor muscle strengthening on sexual satisfaction. There were significant differences in the levels of sexual satisfaction between the intervention and control groups (
p < 0.001) [
27]. Citak et al. confirmed the positive effect of Kegel’s exercises on female sexual function (
p < 0.0001), and a significant increase in self-esteem in the intervention group (
p < 0.0001) [
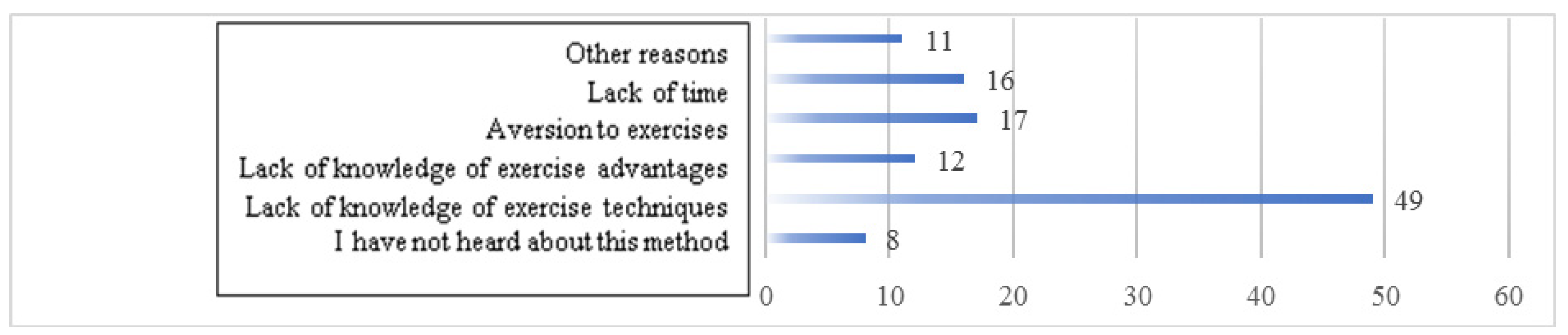
28]. In our research, over half of the study sample did not do pelvic floor muscle exercises (52.49%). The most common reason was the lack of knowledge of the exercise technique (53.26%). Sex education during pregnancy helps to develop the right approach to changes in sexual life, and significantly increases the satisfaction of pregnant women. Shojaa M. et al. showed that the knowledge of Iranian pregnant women is low, which translates into ‘low sexual desire’, ‘fear of harm’, and ‘sexual myths’. Moreover, 73% of women during pregnancy had low libido. None of the women sought advice or information from a doctor or midwife [
29]. Navidian et al. provided evidence that sexual attitudes in the intervention group were significantly better than in the control group (
p < 0.0001) after group sexual counseling. Counseling has changed the traditional perception of sexual activity during pregnancy [
15]. In our research, no statistically significant relationship was observed between sexual satisfaction and seeking information on intercourse during pregnancy (
p > 0.05) [
15]. The respondents most often sought knowledge about intercourse during pregnancy from the Internet (71.92%) and from a gynecologist (68.75%). The quality of the information obtained had not been verified, which may be the reason why this knowledge was not reflected in higher satisfaction with sexual activity. The pregnant women least often used information from midwives (4.86%) and antenatal classes (4.17%), which suggests that in their opinion, a midwife is not a reliable and easily available source of information on sexual problems in this period. This has been confirmed by the research of Liu et al., who noticed that women were much more likely to use unprofessional sources (the Internet, friends, other women having children) than the knowledge of people professionally involved in the care of pregnant women [
12]. In our study, the majority of respondents sought information on sexual activity in pregnancy, but every fifth woman was not interested in getting information on these issues (19.34%). Babazadeh et al. and Shojaa M. et al. believe that the problem is women’s shyness which restrains them from starting a discussion about sexual intercourse during pregnancy with a doctor or a midwife [
29,
30]. Sexual satisfaction is undoubtedly an important element of the overall quality of life. In the light of research, it seems that discussing changes in sexuality during pregnancy with couples expecting a baby, as part of counseling for pregnant women, would be a good practice of obstetricians.




{kind=link}