Balance Tests in Pre-Adolescent Children: Retest Reliability, Construct Validity, and Relative Ability


Abstract
:1. Introduction
- to assess the associations of balance tests with selected motor skills, since the balance is key to all functional movements [28];
- to assess, select, and include the most appropriate balance tests that measure human balance ability into the PF test battery SLOfit, which for more than 30 years has been an obligatory tool used to evaluate the PF level of school-aged children in Slovenia [50]. The more specific aims of the present study were: (1) to examine possible gender differences in balance; and (2) to distinguish the reliability and validity of non-laboratory balance tests.
2. Materials and Methods
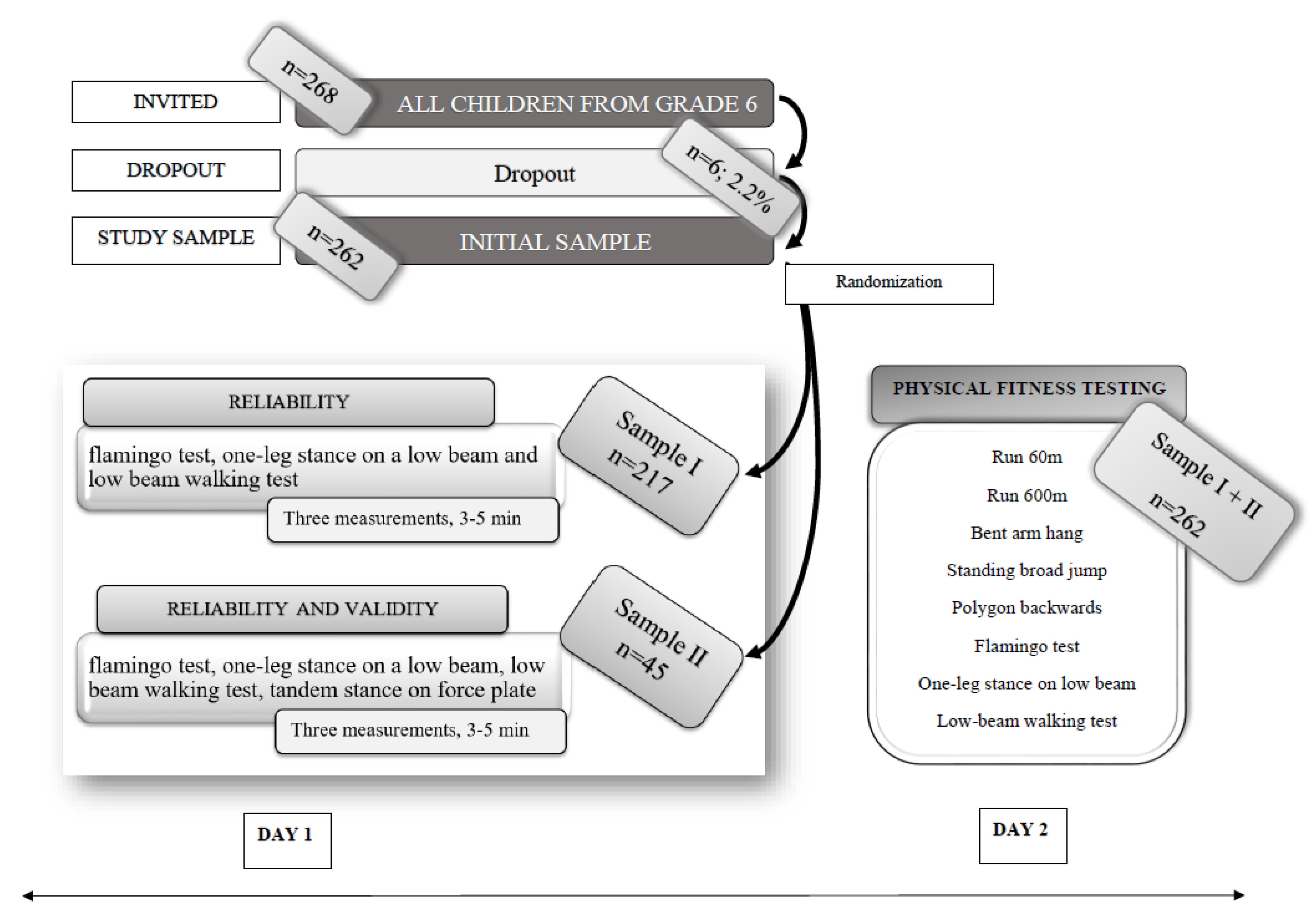
2.1. Participants
2.2. Measurements
2.3. Procedure
2.4. Statistical Analysis
3. Results
4. Discussion
Strengths and Limitations
- (i)
- studying various age groups and patient populations, for instance, a geriatric or population with a neurological handicap, since balance is an essential fundamental movement skill to prevent patients from falling;
- (ii)
- exploring the relationship between balance, attention, and mental abilities or cognition at this age group.
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Powell, K.E.; Pratt, M. Physical activity and health. BMJ 1996, 313, 126–127. [Google Scholar] [CrossRef] [PubMed]
- Batty, D.; Thune, I. Does physical activity prevent cancer? BMJ 2000, 321, 1424–1425. [Google Scholar] [CrossRef] [PubMed]
- Swift, D.L.; Lavie, C.J.; Johannsen, N.M.; Arena, R.; Earnest, C.; O'Keefe, J.H.; Milani, R.V.; Blair, S.N.; Church, T.S. Physical activity, cardiorespiratory fitness, and exercise training in primary and secondary coronary prevention. Circ. J. 2013, 77, 281–292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drenowatz, C.; Prasad, V.K.; Hand, G.A.; Shook, R.P.; Blair, S.N. Effects of moderate and vigorous physical activity on fitness and body composition. J. Behav. Med. 2016, 39, 624–632. [Google Scholar] [CrossRef] [PubMed]
- Bull, F.; Bellew, B.; Schöppe, S.; Bauman, A. Developments in national physical activity policy: An international review and recommendations towards better practice. J. Sci. Med. Sport 2004, 7, 93–104. [Google Scholar] [CrossRef]
- Lee, K.Y.; Lee, P.H.; Macfarlane, D. Associations between moderate-to-vigorous physical activity and neighbourhood recreational facilities: The features of the facilities matter. Int. J. Environ. Res. Public Health 2014, 11, 12594–12610. [Google Scholar] [CrossRef] [Green Version]
- Lei, Y.; Lam, C.K.Y.; Huen Sum Lam, M.; Peake, R. Validity and reliability of timed up and go test on dynamic balance in 3–5 years old preschool children. J. Yoga Phys. Ther. 2017, 7, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Freitas, D.L.; Lausen, B.; Maia, J.A.; Gouveia, E.R.; Antunes, A.M.; Thomis, M.; Lefevre, J.; Malina, R.M. Skeletal maturation, fundamental motor skills, and motor performance in preschool children. Scand. J. Med. Sci. Sports 2018, 28, 2358–2368. [Google Scholar] [CrossRef]
- Gallahue, D.L.; Ozmun, J.C.; Goodway, J. Understanding Motor Development: Infants, Children, Adolescents, Adults; McGraw Hill: Boston, MA, USA, 2006. [Google Scholar]
- Clark, J.E.; Metcalfe, J.S. The Mountain of Motor Development: A metaphor. In Motor Development: Research and Reviews; Clark, J.E., Humphre, J.H., Eds.; NASPE Pulications: Reston, VA, USA, 2002; pp. 163–190. [Google Scholar]
- Lubans, D.R.; Morgan, P.; Cliff, D.; Barnett, L.M.; Okely, A.D. Fundamental movement skills in children and adolescents. Sports Med. 2010, 40, 1019–1035. [Google Scholar] [CrossRef] [Green Version]
- Yanci, J.; Arcos, A.L.; Castillo, D.; Cámara, J. Sprinting, change of direction ability and horizontal jump performance in youth runners according to gender. J. Hum. Kinet. 2017, 60, 199–207. [Google Scholar] [CrossRef] [Green Version]
- Baker, J.S.; Grace, F.; Kilgore, L.; Smith, D.J.; Norris, S.R.; Gardner, A.W.; Ringseis, R.; Eder, K.; Shephard, R.J.; Kokkinos, P.; et al. Postural Control. In Encyclopedia of Exercise Medicine in Health and Disease; Springer Science and Business Media LLC: Berlin, Germany, 2012; p. 721. [Google Scholar]
- Shumway-Cook, A.; Woollacott, M.H. Motor Control: Theory and Practical Applications; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2001. [Google Scholar]
- Spodek, B. Handbook of Research on the Education of Young Children; Informa UK Limited: London, UK, 2014. [Google Scholar]
- Brown, L.E.; Weir, J.P. ASEP procedures recommendation I: Accurate assessment of muscular strength and power. J. Exerc. Physiol. Online 2001, 4, 1–2. [Google Scholar]
- Horak, F.B. Postural orientation and equilibrium: What do we need to know about neural control of balance to prevent falls? Age Ageing 2006, 35, 7–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pérennou, D.; Decavel, P.; Manckoundia, P.; Penven, Y.; Mourey, F.; Launay, F.; Pfitzenmeyer, P.; Casillas, J.M. Évaluation de l’équilibre en pathologie neurologique et gériatrique. Evaluation of balance in neurologic and geriatric disorders. Proc. Ann. Réadaptation Médecine Phys. 2005, 48, 317–335. [Google Scholar]
- Yelnik, A.; Bonan, I. Clinical tools for assessing balance disorders. Neurophysiol. Clin. Neurophysiol. 2008, 38, 439–445. [Google Scholar] [CrossRef]
- Pfitzenmeyer, P.; Camus, A.; Pfitzenmeyer, P. Posture and aging. Current fundamental studies and management concepts. Presse Médicale 2000, 29, 340–344. [Google Scholar]
- Kaufman, K.R.; Brey, R.H.; Chou, L.-S.; Rabatin, A.; Brown, A.W.; Basford, J.R. Comparison of subjective and objective measurements of balance disorders following traumatic brain injury. Med Eng. Phys. 2006, 28, 234–239. [Google Scholar] [CrossRef]
- Blum, L.; Korner-Bitensky, N. Usefulness of the berg balance scale in stroke rehabilitation: A systematic review. Phys. Ther. 2008, 88, 559–566. [Google Scholar] [CrossRef]
- Mathias, S.; Nayak, U.S.; Isaacs, B. Balance in elderly patients: The “get-up and go” test. Arch. Phys. Med. Rehabil. 1986, 67, 387–389. [Google Scholar]
- Podsiadlo, D.; Richardson, S. The Timed “Up & Go”: A Test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef]
- Granacher, U.; Gollhofer, A. Is there an association between variables of postural control and strength in prepubertal children? J. Strength Cond. Res. 2012, 26, 210–216. [Google Scholar] [CrossRef]
- Muehlbauer, T.; Besemer, C.; Wehrle, A.; Gollhofer, A.; Granacher, U. Relationship between strength, balance and mobility in children aged 7–10 years. Gait Posture 2013, 37, 108–112. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, A.I.; Muaidi, Q.I.; Abdelsalam, M.S.; Hawamdeh, Z.M.; Alhusaini, A.A. Association of postural balance and isometric muscle strength in early- and middle-school-age boys. J. Manip. Physiol. Ther. 2013, 36, 633–643. [Google Scholar] [CrossRef] [PubMed]
- Groselj, J.; Osredkar, D.; Sember, V.; Pajek, M. Associations between balance and other fundamental motor skills in pre-adolescents. Med. DELLO Sport 2019, 72, 200–215. [Google Scholar]
- Getchell, N.; Pabreja, P.; Neeld, K.; Carrio, V. Comparing Children with and without Dyslexia on the movement assessment battery for children and the test of gross motor development. Percept. Mot. Ski. 2007, 105, 207–214. [Google Scholar] [CrossRef]
- Sjöström, M.; Oja, P.; Hagströmer, M.; Smith, B.J.; Bauman, A. Health-enhancing physical activity across European Union countries: The Eurobarometer study. J. Public Health 2006, 14, 291–300. [Google Scholar] [CrossRef]
- Plisky, P.J.; Rauh, M.J.; Kaminski, T.W.; Underwood, F.B. Star excursion balance test as a predictor of lower extremity injury in high school basketball players. J. Orthop. Sports Phys. Ther. 2006, 36, 911–919. [Google Scholar] [CrossRef]
- De Kegel, A.; Dhooge, I.; Peersman, W.; Rijckaert, J.; Baetens, T.; Cambier, D.; Van Waelvelde, H. Construct validity of the assessment of balance in children who are developing typically and in children with hearing impairments. Phys. Ther. 2010, 90, 1783–1794. [Google Scholar] [CrossRef] [Green Version]
- Villamonte, R.; Vehrs, P.; Feland, J.B.; Johnson, A.W.; Seeley, M.K.; Eggett, D. Reliability of 16 balance tests in Individuals with down syndrome. Percept. Mot. Ski. 2010, 111, 530–542. [Google Scholar] [CrossRef]
- Blomqvist, S.; Olsson, J.; Wallin, L.; Wester, A.; Rehn, B. Adolescents with intellectual disability have reduced postural balance and muscle performance in trunk and lower limbs compared to peers without intellectual disability. Res. Dev. Disabil. 2013, 34, 198–206. [Google Scholar] [CrossRef]
- Fleishman, E.A.; Hempel, W.E.J. The relation between abilities and improvement with practice in a visual discrimination reaction task. J. Exp. Psychol. 1955, 49, 301–312. [Google Scholar] [CrossRef]
- Westcott, S.L.; Lowes, L.P.; Richardson, P.K.; Crowe, T.K.; Deitz, J. Difference in the use of sensory information for maintenance of standing balance in children with different motor disabilities. Dev. Med. Child Neurol. 1997, 39, 32–33. [Google Scholar]
- Clark, J.E.; Watkins, D.L. Static balance in young children. Child Dev. 1984, 55, 854–857. [Google Scholar] [CrossRef]
- Cattaneo, D.; Regola, A.; Meotti, M. Validity of six balance disorders scales in persons with multiple sclerosis. Disabil. Rehabil. 2006, 28, 789–795. [Google Scholar] [CrossRef] [PubMed]
- Tsigilis, N.; Douda, H.; Tokmakidis, S.P. Test-retest reliability of the Eurofit test battery administered to university students. Percept. Mot. Ski. 2002, 95, 1295–1300. [Google Scholar] [CrossRef]
- Atwater, S.W.; Crowe, T.K.; Deitz, J.C.; Richardson, P.K. Interrater and test-retest reliability of two pediatric balance tests. Phys. Ther. 1990, 70, 79–87. [Google Scholar] [CrossRef]
- Venetsanou, F.; Kambas, A. The effects of age and gender on balance skills in preschool children. Facta Univ. Phys. Educ. Sport 2011, 9, 81–90. [Google Scholar]
- Holm, I.; Vøllestad, N.K. Significant effect of gender on hamstring-to-quadriceps strength ratio and static balance in prepubescent children from 7 to 12 years of age. Am. J. Sports Med. 2008, 36, 2007–2013. [Google Scholar] [CrossRef]
- Milanese, C.; Sandri, M.; Cavedon, V.; Zancanaro, C. The role of age, sex, anthropometry, and body composition as determinants of physical fitness in nonobese children aged 6–12. PeerJ 2020, 8, e8657. [Google Scholar] [CrossRef]
- Venetsanou, F.; Kambas, A.; Ellinoudis, T.; Fatouros, I.; Giannakidou, D.; Kourtessis, T. Can the movement assessment battery for children-test be the “gold standard” for the motor assessment of children with developmental coordination disorder? Res. Dev. Disabil. 2011, 32, 1–10. [Google Scholar] [CrossRef]
- De Miguel-Etayo, P.; Gracia-Marco, L.; Ortega, F.B.; Intemann, T.; Foraita, R.; Lissner, L.; Oja, L.; Barba, G.; Michels, N. Physical fitness reference standards in European children: The IDEFICS study. Int. J. Obes. 2014, 38, S57–S66. [Google Scholar] [CrossRef] [Green Version]
- Broadhead, G.D.; Bruininks, R.H. Childhood motor performance traits on the short form Bruininks-Oseretsky Test (Special Populations). Phys. Educ. 1982, 39, 149. [Google Scholar]
- Fjørtoft, I.; Sageie, J. The natural environment as a playground for children. Landsc. Urban Plan. 2000, 48, 83–97. [Google Scholar] [CrossRef]
- Kourtessis, T.; Tsougou, E.; Maheridou, M.; Tsigilis, N.; Psalti, M.; Kioumourtzoglou, E. Developmental coordination disorder in early childhood-A preliminary epidemiological study in greek schools. Int. J. Med. 2008, 1, 95–99. [Google Scholar]
- Panjan, A.; Sarabon, N. Methods for the evaluation of human balance body. Sport Sci. Rev. 2010, 19, 5–6. [Google Scholar] [CrossRef] [Green Version]
- Jurak, G.; Kovac, M.; Sember, V.; Starc, G. 30 Years of SLOfit: Its Legacy and Perspective. Turk. J. Sports Med. 2019, 54, 23–27. [Google Scholar] [CrossRef]
- Barabas, A.; Bretz, K.; Kaske, R.J. Stabilometry of the Flamingo Balance Test. In Proceedings of the ISBS-Conference Proceedings Archive, Funchal, Madeira, Portugal, 25–29 June 1996; Volume 1. [Google Scholar]
- Kovač, M.; Jurak, G.; Starc, G.; Leskošek, B.; Strel, J. Športnovzgojni Harton: Diagnostika in Ovrednotenje Telesnega in Gibalnega Razvoja Otrok in Mladine v Sloveniji; Fakulteta za šport: Ljubljana, Slovenia, 2011. [Google Scholar]
- Šarabon, N.; Rosker, J.; Loefler, S.; Kern, H.; Loefler, S. The effect of vision elimination during quiet stance tasks with different feet positions. Gait Posture 2013, 38, 708–711. [Google Scholar] [CrossRef]
- Webber, C.L.; Zbilut, J.P. Dynamical assessment of physiological systems and states using recurrence plot strategies. J. Appl. Physiol. 1994, 76, 965–973. [Google Scholar] [CrossRef]
- Riley, M.A.; Balasubramaniam, R.; Turvey, M. Recurrence quantification analysis of postural fluctuations. Gait Posture 1999, 9, 65–78. [Google Scholar] [CrossRef]
- Bruhn, S.; Kullmann, N.; Gollhofer, A. The Effects of a sensorimotor training and a strength training on postural stabilisation, maximum isometric contraction and jump performance. Int. J. Sports Med. 2004, 25, 56–60. [Google Scholar] [CrossRef]
- Rugelj, D.; Tomšič, M.; Ovca, A.; Sevšek, F. Za ravnotežje specifična vadba in zmanjševanje ogroženosti za padce. Raziskovalni dan Zdr. Fakulteta 2009, 4, 29–40. [Google Scholar]
- Buderath, P.; Gärtner, K.; Frings, M.; Christiansen, H.; Schoch, B.; Konczak, J.; Gizewski, E.R.; Hebebrand, J.; Timmann, D.; Konczak, J. Postural and gait performance in children with attention deficit/hyperactivity disorder. Gait Posture 2009, 29, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Johnson-Kramer, C.; Sherwood, D.; French, R.; Canabal, M.Y. Performance and learning of a dynamic balance task by visually impaired children. Clin. Kinesiol. 1992, 31, 3–6. [Google Scholar]
- Goulding, A.; Jones, I.E.; Taylor, R.W.; Piggot, J.M.; Taylor, D. Dynamic and static tests of balance and postural sway in boys: Effects of previous wrist bone fractures and high adiposity. Gait Posture 2003, 17, 136–141. [Google Scholar] [CrossRef]
- Kooistra, L.; Ramage, B.; Crawford, S.; Cantell, M.; Wormsbecker, S.; Gibbard, B.; Kaplan, B.J. Can attention deficit hyperactivity disorder and fetal alcohol spectrum disorder be differentiated by motor and balance deficits? Hum. Mov. Sci. 2009, 28, 529–542. [Google Scholar] [CrossRef] [PubMed]
- Hsue, B.-J.; Miller, F.; Su, F.-C. The dynamic balance of the children with cerebral palsy and typical developing during gait. Part I: Spatial relationship between COM and COP trajectories. Gait Posture 2009, 29, 465–470. [Google Scholar] [CrossRef]
- Collings, R.; Paton, J.; Glasser, S.; Marsden, J. The effect of vision impairment on dynamic balance. J. Foot Ankle Res. 2015, 8, A6. [Google Scholar] [CrossRef] [Green Version]
- Goetz, M.; Schwabova, J.P.; Hlavka, Z.; Ptacek, R.; Surman, C.B. Dynamic balance in children with attention-deficit hyperactivity disorder and its relationship with cognitive functions and cerebellum. Neuropsychiatr. Dis. Treat. 2017, 13, 873–880. [Google Scholar] [CrossRef] [Green Version]
- Libardoni, T.D.C.; Da Silveira, C.B.; Sinhorim, L.M.B.; De Oliveira, A.S.; Dos Santos, M.J.; Santos, G. Reference values and equations reference of balance for children of 8 to 12 years. Gait Posture 2018, 60, 122–127. [Google Scholar] [CrossRef]
- Schwiertz, G.; Brueckner, D.; Schedler, S.; Kiss, R.; Muehlbauer, T. Performance and reliability of the lower quarter Y balance test in healthy adolescents from grade 6 to 11. Gait Posture 2019, 67, 142–146. [Google Scholar] [CrossRef]
- Kranti Panta, B.P.T. A study to associate the Flamingo Test and the Stork Test in measuring static balance on healthy adults. Foot Ankle Online J. 2015, 8. [Google Scholar] [CrossRef]
- Helbostad, J.L.; Sturnieks, D.L.; Menant, J.C.; Delbaere, K.; Lord, S.R.; Pijnappels, M. Consequences of lower extremity and trunk muscle fatigue on balance and functional tasks in older people: A systematic literature review. BMC Geriatr. 2010, 10, 56. [Google Scholar] [CrossRef] [Green Version]
- Barati, A.; Safarcherati, A.; Aghayari, A.; Azizi, F.; Abbasi, H. Evaluation of Relationship between Trunk muscle endurance and static balance in male students. Asian J. Sports Med. 2013, 4, 289–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vancampfort, D.; Hallgren, M.; Vandael, H.; Probst, M.; Stubbs, B.; Raymaekers, S.; Van Damme, T. Test-retest reliability and clinical correlates of the Eurofit test battery in people with alcohol use disorders. Psychiatry Res. 2019, 271, 208–213. [Google Scholar] [CrossRef] [Green Version]
- Tomkinson, G.R.; Carver, K.D.; Atkinson, F.; Daniell, N.D.; Lewis, L.K.; Fitzgerald, J.S.; Lang, J.J.; Ortega, F.B. European normative values for physical fitness in children and adolescents aged 9–17 years: Results from 2 779 165 Eurofit performances representing 30 countries. Br. J. Sports Med. 2017, 52, 1445–1456. [Google Scholar] [CrossRef] [Green Version]
- Strel, J.; Šturm, J.; Pistotnik, B.; Lenarčič, M. Zanesljivost in Struktura Nekaterih Motoričnih Sposobnosti in Morfoloških Značilnosti Šest in Pol Letnih Učencev in Učenk; Visoka Šola za Telesno Kulturo, Inštitut Za Kineziologijo: Playa Del Rey, CA, USA, 1981. [Google Scholar]
- Nguyen, U.-S.D.T.; Kiel, D.P.; Li, W.; Galica, A.M.; Kang, H.G.; Casey, V.A.; Hannan, M.T. Correlations of clinical and laboratory measures of balance in older men and women. Arthritis Rheum. 2012, 64, 1895–1902. [Google Scholar] [CrossRef]
- Sawacha, Z.; Carraro, E.; Contessa, P.; Guiotto, A.; Masiero, S.; Cobelli, C. Relationship between clinical and instrumental balance assessments in chronic post-stroke hemiparesis subjects. J. Neuroeng. Rehabil. 2013, 10, 95. [Google Scholar] [CrossRef] [Green Version]
- Sember, V. Impact of Physical Activity and Physical Fitness on Academic Performance in Selected Slovenian Schoolchildren. Ph.D. Thesis, Primorska University, Capodistria, Slovenia, March 2017. [Google Scholar]
- Araújo, F.; Simões, D.; Silva, P.; Alegrete, N.; Lucas, R. Sagittal standing posture and relationships with anthropometrics and body composition during childhood. Gait Posture 2019, 73, 45–51. [Google Scholar] [CrossRef]
- Smith, A.W.; Ulmer, F.F.; Wong, D.P. Gender differences in postural stability among children. J. Hum. Kinet. 2012, 33, 25–32. [Google Scholar] [CrossRef]
- Shumway-Cook, A.; Woollacott, M.H. Motor Control: Translating Research Into Clinical Practice; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2007. [Google Scholar]


{kind=link}
| Gender | n | Physical Fitness Test | Mean + (SD) | Physical Fitness Test | Mean ± (SD) |
|---|---|---|---|---|---|
| M F ALL | 139 123 262 | Standing broad jump (cm) | 160.04 ± 18.6 156.8 ± 21.5 158.34 ± 20.2 | Run 60 m (s) | 10.6 ± 8.9 10.9 ± 8.7 10.8 ± 8.9 |
| M F ALL | 139 123 262 | Bent arm hang (s) | 43.4 ± 31.9 39.0 ± 29.4 41.06 ± 30.7 | Flamingo test (rep.) | 12.6 + 7.0 12.0 + 6.1 12.4 + 6.6 |
| M F ALL | 139 123 262 | Polygon backwards (s) | 13.9 ± 4.0 13.8 ± 3.8 13.8 ± 3.4 | One-leg stance on low beam (s) | 31.4 + 26.6 35.7 + 36.6 33.7 + 18.4 |
| M F ALL | 139 123 262 | Run 600 m (s) | 162.6 ± 27.3 174.0 ± 28.7 168.7 ± 28.5 | Low-beam walking test (s) | 5.8 + 1.2 6.0 + 1.5 5.9 + 1.4 |
| Balance/PF Test | Gender | n | OLSB | LBWT | SBJ | PB | BAH | R60 | R600 |
|---|---|---|---|---|---|---|---|---|---|
| FLA | M F ALL | 139 123 262 | −0.376 ** −0.392 ** −0.372 ** | 0.410 0.363 0.392 | −0.304 ** −0.481 ** −.0372 ** | 0.234 ** 0.586 ** 0.384 ** | −0.297 ** −0.429 ** −0.349 ** | 0.366 ** 0.531 ** 0.430 ** | 0.320 ** 0.662 ** 0.411 ** |
| OLSB | M F ALL | 139 123 262 | −0.226 −0.271 −0.238 | 0.291 ** 0.370 ** 0.299 ** | −0.350 ** −0.390 ** −0.362 ** | 0.447 ** 0.535 ** 0.475 ** | −0.201 * −0.337 ** −0.194 ** | −0.208 * −0.493 ** −0.411 ** | |
| LBWT | M F ALL | 118 99 217 | −0.360 ** −0.463 ** −0.400 ** | 0.283 ** 0.427 ** 0.336 ** | −0.211 * −0.257 * −0.226 ** | 0.359 ** 0.208 * 0.301 * | 0.268 ** 0.433 * 0.320 ** |
| Balance Tests/Motor Test | Sample | Gender | n | Mean + (SD) | ICC | 95 % ICC | Cronbach |
|---|---|---|---|---|---|---|---|
| Flamingo test (rep.)* | I | M F ALL | 118 99 217 | 11.70 ± 6.31 12.99 ± 7.09 12.29 ± 6.69 | 0.902 0.919 0.910 | 0.868–0.929 0.887–0.943 0.888–0.929 | 0.917 0.903 0.910 |
| II | M F ALL | 21 24 45 | 14.25 ± 6.47 11.63 ± 5.03 12.85 ± 5.83 | 0.938 0.901 0.925 | 0.873–0.973 0.806–0.954 0.877–0.956 | 0.938 0.901 0.925 | |
| One-leg stance on low beam (s) | I | M F ALL | 118 99 217 | 28.32 ± 17.63 32.53 ± 16.81 30.24 ± 17.35 | 0.827 0.785 0.810 | 0.765–0.856 0.700–0.849 0.762–0.850 | 0.769 0.838 0.810 |
| II | M F ALL | 21 24 45 | 46.98 ± 15.28 53.44 ± 12.23 50.42 + 13.96 | 0.759 0.821 0.791 | 0.501–0.894 0.646 –0.917 0.658–0.878 | 0.759 0.821 0.791 | |
| Low-beam walking test (s) | I | M F ALL | 118 99 217 | 5.76 ± 1.22 6.81 ± 1.59 5.91 ± 1.41 | 0.881 0.880 0.882 | 0.838–0.914 0.832–0.916 0.852–0.907 | 0.873 0.896 0.882 |
| II | M F ALL | 21 24 45 | 5.80 ± 1.16 6.27 ± 1.10 6.05 ± 1.14 | 0.937 0.906 0.925 | 0.870–0.973 0.815–0.956 0.876–0.956 | 0.937 0.906 0.925 | |
| BSEO (mm) | II | M F ALL | 21 24 45 | 1185.45 ± 71.56 1020.97 ± 26.79 1097.73 ± 59.40 | 0.897 0.931 0.916 | 0.787–0.955 0.863–0.968 0.862 –0.951 | 0.897 0.931 0.916 |
| BSEC (mm) | II | M F ALL | 21 24 45 | 1924.95 ± 456.95 1588.06 ± 388.91 1745.27 ± 450.40 | 0.780 0.901 0.858 | 0.545 - 0.904 0.804–0.954 0.767–0.917 | 0.780 0.901 0.858 |
| BSapEO (mm) | II | M F ALL | 21 24 45 | 881.30 ± 226.91 741.79 ± 201.99 806.89 ± 222.90 | 0.910 0.941 0.926 | 0.814–0.961 0.884–0.973 0.878–0.957 | 0.910 0.941 0.926 |
| BSmlEO (mm) | II | M F ALL | 21 24 45 | 615.68 ± 123.76 558.00 ± 108.09 584.92 ± 117.97 | 0.843 0.869 0.859 | 0.675–0.931 0.741–0.939 0.769–0.918 | 0.843 0.869 0.859 |
| VEO (mm/s) | II | M F ALL | 21 24 45 | 39.51 ± 9.06 34.03 ± 7.56 36.59 ± 8.65 | 0.896 0.931 0.915 | 0.786–0.955 0.863–0.968 0.861–0.951 | 0.896 0.931 0.915 |
| AapEO (mm) | II | M F ALL | 21 24 45 | 5.51 ± 1.98 3.98 ± 1.46 4.69 ± 1.87 | 0.922 0.920 0.926 | 0.838–0.966 0.842–0.963 0.879–0.957 | 0.922 0.920 0.926 |
| AmlEO (mm) | II | M F ALL | 21 24 45 | 4.53 + 1.25 3.39 ± 0.95 3.93 ± 1.23 | 0.777 0.819 0.827 | 0.538–0.902 0.642–0.916 0.717–0.899 | 0.777 0.819 0.827 |
| Component | ||
|---|---|---|
| Balance Variable | 1 | 2 |
| Total sway path with eyes open (BSEO) | 0.990 | −0.041 |
| Total body sway with EC of CoP displacement in all directions (BSEC) | 0.845 | −0.097 |
| Body sway of CoP displacements in the a-p direction (BSapEO) | 0.972 | −0.035 |
| Body sway of CoP displacements in the m-l direction (BSmlEO) | 0.891 | −0.014 |
| Mean velocity of CoP displacements (VEO) | 0.990 | −0.040 |
| Mean amplitude of COP displacements in the a-p direction (AapEO) | 0.927 | 0.093 |
| Mean amplitude of COP displacements in the m-l direction (AmlEO) | 0.865 | 0.173 |
| Flamingo test | 0.106 | 0.852 |
| Low-beam walking test | −0.150 | 0.787 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sember, V.; Grošelj, J.; Pajek, M. Balance Tests in Pre-Adolescent Children: Retest Reliability, Construct Validity, and Relative Ability. Int. J. Environ. Res. Public Health 2020, 17, 5474. https://doi.org/10.3390/ijerph17155474
Sember V, Grošelj J, Pajek M. Balance Tests in Pre-Adolescent Children: Retest Reliability, Construct Validity, and Relative Ability. International Journal of Environmental Research and Public Health. 2020; 17(15):5474. https://doi.org/10.3390/ijerph17155474
Chicago/Turabian StyleSember, Vedrana, Janja Grošelj, and Maja Pajek. 2020. "Balance Tests in Pre-Adolescent Children: Retest Reliability, Construct Validity, and Relative Ability" International Journal of Environmental Research and Public Health 17, no. 15: 5474. https://doi.org/10.3390/ijerph17155474