Factors Affecting HIV Testing among Youth in Kenya


Abstract
:1. Introduction
1.1. HIV Testing as An HIV Prevention Strategy
1.2. Facilitators and Barriers to HIV Testing
1.2.1. HIV Knowledge
1.2.2. Stigma
1.2.3. Social Support
1.2.4. Subjective Well-being
1.2.5. Mental Health
1.2.6. Substance Use
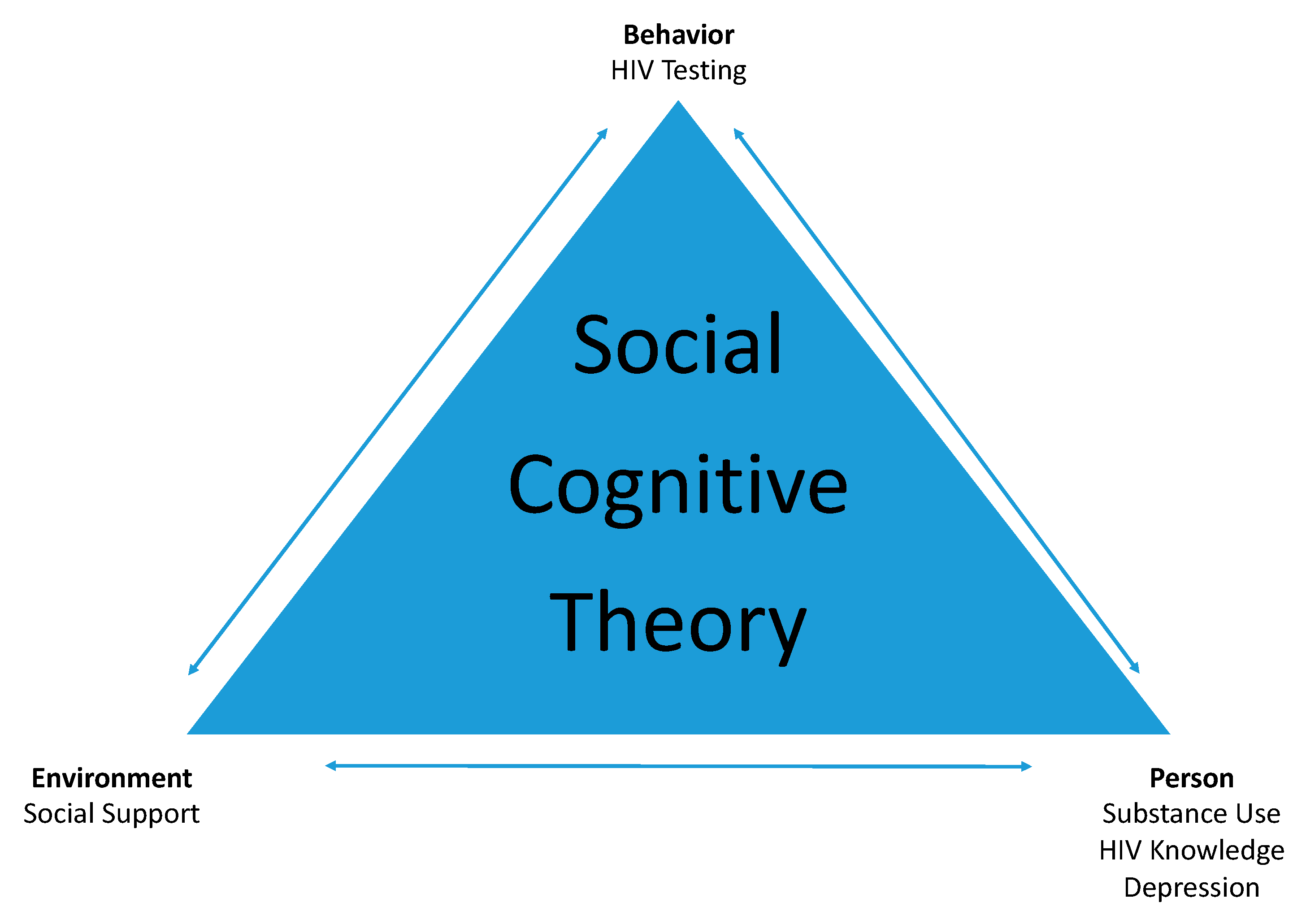
1.3. Social Cognitive Theory Applied to HIV
1.4. Purpose of This Study
2. Materials and Methods
2.1. Study Design
2.2. Research Variables
2.3. Participants and Procedure
2.4. Measures
2.4.1. Behavioral Intentions
2.4.2. Brief HIV Knowledge Questionnaire (HIV KQ-18)
2.4.3. AIDS-Related Stigma Scale (ARSS)
2.4.4. Social Provision Scale
2.4.5. Subjective Well-being Scale
2.4.6. Depression, Anxiety, and Stress Scale (DASS-21)
2.4.7. CRAFFT Screening Tool for Adolescent Substance Abuse
2.5. Date Analysis
3. Results
3.1. Participant Demographics
3.2. Descriptive Statistics
3.2.1. Behavioral Intentions
3.2.2. Brief HIV Knowledge Questionnaire (HIV KQ-18)
3.2.3. AIDS-Related Stigma Scale (ARSS)
3.2.4. Social Provision Scale
3.2.5. Subjective Well-being Scale
3.2.6. Depression, Anxiety, and Stress Scale (DASS-21)
3.2.7. CRAFFT Screening Tool for Adolescent Substance Abuse (CRAFFT)
3.3. Impact of Independent Variables on Intent to Test for HIV
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Joint United Nations Programme on HIV/AIDS; AIDSinfo. People Living with HIV. Available online: http://aidsinfo.unaids.org/ (accessed on 20 March 2019).
- United Nations Children’s Fund. Turning the Tide Against AIDS Will Require More Concentrated Focus on Adolescents and Young People. 2017. Available online: https://data.unicef.org/topic/hivaids/adolescents-young-people/# (accessed on 9 February 2019).
- Joint United Nations Programme on HIV/AIDS. UNAIDS Data 2017. Available online: http://www.unaids.org/sites/default/files/media_asset/20170720_Data_book_2017_en.pdf (accessed on 9 February 2019).
- World Health Organization. Global Update on HIV treatment 2013: Results, Impact and Opportunities; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Gardner, E.M.; McLees, M.P.; Steiner, J.F.; del Rio, C.; Burman, W. The spectrum of engagement in HIV care and its relevance to test-and-treat strategies for prevention of HIV infection. Clin. Infect. Dis. 2011, 52, 793–800. [Google Scholar] [CrossRef]
- National AIDS and STI Control Programme, Ministry of Health, Kenya. Guidelines for HIV Testing Services in Kenya; NASCOP: Nairobi, Kenya, 2015. [Google Scholar]
- Kenya National Bureau of Statistics; Ministry of Health/Kenya; National AIDS Control Council/Kenya; Kenya Medical Research Institute; National Council for Population and Development/Kenya; ICF International. Kenya Demographic and Health Survey 2014. 2015. Available online: https://dhsprogram.com/pubs/pdf/fr308/fr308.pdf (accessed on 9 February 2019).
- Rueda, S.; Mitra, S.; Chen, S.; Gogolishvili, D.; Globerman, J.; Chambers, L.; Wilson, M.; Logie, C.H.; Shi, Q.; Morassaei, S.; et al. Examining the associations between HIV-related stigma and health outcomes in people living with HIV/AIDS: A series of meta-analyses. Br. Med. J. Open 2016, 6, e011453. [Google Scholar] [CrossRef]
- Glick, P.; Sahn, D.E. Changes in HIV/AIDS knowledge and testing behavior in Africa: How much and for whom? J. Popul. Econ. 2007, 20, 383–422. [Google Scholar] [CrossRef]
- Okumu, E.; Jolly, D.H.; Alston, L.; Eley, N.T.; Laws, M.; MacQueen, K.M. Relationship between human immunodeficiency virus (HIV) knowledge, HIV-related stigma, and HIV testing among young black adults in a southeastern city. Front. Public Health 2017, 5, 47. [Google Scholar] [CrossRef]
- Evangeli, M.; Pady, K.; Wroe, A.L. Which psychological factors and related to HIV testing? A quantitative systematic review of global studies. AIDS Behav. 2016, 20, 880–918. [Google Scholar] [CrossRef] [PubMed]
- Turan, B.; Hatcher, A.M.; Weiser, S.D.; Johnson, M.O.; Rice, W.S.; Turan, J.M. Framing mechanisms linking HIV-related stigma, adherence to treatment, and health outcomes. Am. J. Public Health 2017, 107, 863–869. [Google Scholar] [CrossRef] [PubMed]
- Knight, R.; Small, W.; Shoveller, J.A. HIV stigma and the experiences of young men with voluntary and routine HIV testing. Sociol. Health Illn. 2016, 38, 153–167. [Google Scholar] [CrossRef]
- Maughan-Brown, B.; Nyblade, L. Different dimensions of HIV-related stigma may have opposite effects on HIV testing: Evidence among young men and women in South Africa. AIDS Behav. 2014, 18, 958–965. [Google Scholar] [CrossRef]
- Smith, R.; Rossetto, K.; Peterson, B.L. A meta-analysis of disclosure of one’s HIV-positive status, stigma and social support. AIDS Care 2008, 20, 1266–1275. [Google Scholar] [CrossRef] [PubMed]
- Drain, P.K.; Losina, E.; Coleman, S.M.; Bogart, L.; Giddy, J.; Ross, D.; Katz, J.N.; Bassett, I.V. Social support and mental health among adults prior to HIV counseling and testing in Durban, South Africa. AIDS Care 2015, 27, 1231–1240. [Google Scholar] [CrossRef] [Green Version]
- Lypen, K.D.; Lockwood, N.M.; Shalabi, F.; Harper, G.W.; Ngugi, E. ‘When we are together I feel at home.’ Types and sources of social support among youth newly diagnosed with HIV in Kenya: Implications for intervention. Afr. J. AIDS Res. 2015, 14, 275–284. [Google Scholar] [CrossRef]
- Boydell, N.; Buston, K.; McDaid, L.M. Patterns of HIV testing practices among young gay and bisexual men living in Scotland: A qualitative study. BMC Public Health 2017, 17, 660–670. [Google Scholar] [CrossRef]
- Mashburn, A.J.; Peterson, J.L.; Bakeman, R.; Miller, R.L.; Cork, L.F. Influences on HIV testing among young African-American men who have sex with men and the moderating effect of the geographic setting. J. Community Psychol. 2004, 32, 45–60. [Google Scholar] [CrossRef]
- Gronlie, A.A.; Dageid, W. Subjective well-being among HIV-positive South Africans: The influence of resilience and social capital. Soc. Indic. Res. 2017, 131, 1251–1268. [Google Scholar] [CrossRef]
- Hutton, V.E.; Misajon, R.; Collins, F.E. Subjective wellbeing and felt stigma when living with HIV. Qual. Life Res. 2013, 22, 65–73. [Google Scholar] [CrossRef]
- Reis, A.S.; Guerra, M.P.; Lencastre, L.E. Treatment adherence and subjective well-being in HIV/AIDS infection. AIDS Care 2013, 25, 1604–1611. [Google Scholar] [CrossRef]
- Kiene, S.M.; Lule, H.; Sileo, K.M.; Slimi, K.P.; Wahyenze, R.K. Depression, alcohol use, and intimate partner violence among outpatients in rural Uganda: Vulnerabilities for HIV, STIs and high risk sexual behavior. Biomed Cent. Infect. Dis. 2017, 17, 88. [Google Scholar] [CrossRef]
- Kagee, A.; Saal, W.; De Villiers, L.; Sefatsa, M.; Bantjes, J. The prevalence of common mental disorders among South Africans seeking HIV testing. AIDS Behav. 2017, 21, 1511–1517. [Google Scholar] [CrossRef]
- Sahay, S.; Phadke, M.; Brahme, R.; Paralikar, V.; Joshi, V.; Sane, S.; Risbud, A.; Mate, S.; Mehendale, S. Correlates of anxiety and depression among HIV test-seekers at a voluntary counseling and testing facility in Pune, India. Qual. Life Res. 2007, 16, 41–52. [Google Scholar] [CrossRef]
- Lin, C.; Lee, Y.; Yang, H. Risky sexual behaviors as correlates of depression and suicidal ideation among male HIV test-seekers at a voluntary counseling and testing facility in Taiwan. Asia-Pac. J. Public Health 2017, 29, 219–228. [Google Scholar] [CrossRef]
- Worthington, C.; Meyers, T. Factors underlying anxiety in HIV testing: Risk perceptions, stigma, and the patient-provider power dynamic. Qual. Health Res. 2003, 13, 636–655. [Google Scholar] [CrossRef] [PubMed]
- Kohler, P.K.; Ondenge, K.; Mills, L.A.; Okanda, J.; Kinuthia, J.; Olilo, G.; Odhiambo, F.; Laserson, K.F.; Zierler, B.; Voss, J.; et al. Shame, guilt, and stress: Community perceptions of barriers to engaging in prevention of mother to child transmission (PMTCT) programs in western Kenya. AIDS Patient Care STDs 2014, 28, 643–651. [Google Scholar] [CrossRef]
- Yehia, B.R.; Cui, W.; Thompson, W.W.; Zack, M.M.; McKnight-Eily, L.; DiNenno, E.; Rose, C.E.; Blank, M.B. HIV testing among adults with mental illness in the United States. AIDS Patient Care STDs 2014, 28, 628–634. [Google Scholar] [CrossRef]
- Strathdee, S.A.; Patrick, D.M.; Currie, S.L.; Cornelisse, P.G.; Rekart, M.L.; Montaner, J.S.; Schechter, M.T.; O’shaughnessy, M.V. Needle exchange is not enough: Lessons from the Vancouver injecting drug use study. AIDS 1997, 11, F59–F65. [Google Scholar] [CrossRef] [PubMed]
- Walter, A.W.; Cheng, D.M.; Lloyd-Travaglini, C.A.; Samet, J.H.; Bernstein, J.; Saitz, R. Are decreases in drug use risk associated with reductions in HIV sex risk behaviors among adults in an urban hospital primary care setting? Prev. Med. Rep. 2016, 4, 410–416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joint United Nations Programme on HIV/AIDS. Harm Reduction Saves Lives; Joint United Nations Programme on HIV/AIDS: Geneva, Switzerland, 2017; Available online: http://www.unaids.org/sites/default/files/media_asset/harm-reduction-saves-lives_en.pdf (accessed on 9 February 2019).
- Ford, K.; Wirawan, D.N.; Sumantera, G.M.; Sawitri, A.A.S.; Stahre, M. Voluntary HIV testing, disclosure, and stigma among injection drug users in Bali, Indonesia. AIDS Educ. Prev. 2004, 16, 487–498. [Google Scholar] [CrossRef]
- Bandura, A. Social Foundations of thought and Action: A Social Cognitive Theory; Prentice-Hall: Englewood Cliffs, NJ, USA, 1986. [Google Scholar]
- Bandura, A. Social cognitive theory and exercise of control over HIV infection. In Preventing AIDS: Theories and Methods of Behavioral Interventions; DiClemente, R.J., Peterson, J.L., Eds.; Plenum: New York, NY, USA, 1994; pp. 25–59. [Google Scholar]
- Li, X.; Zhang, L.; Mao, R.; Zhao, Q.; Stanton, B. Effect of social cognitive theory-based HIV education prevention program among high school students in Nanjing, China. Health Educ. Res. 2011, 26, 419–431. [Google Scholar] [CrossRef] [Green Version]
- Chenneville, T. Formative HIV research among youth in Kenya: Findings from a psychosocial needs assessment. J. Assoc. Nurses AIDS Care 2017, 28, 443–449. [Google Scholar] [CrossRef]
- Chenneville, T.; Gabbidon, K.; Drake, H. The HIV SEERs project: A qualitative analysis of program facilitators’ experience. J. Int. Assoc. Provid. AIDS Care 2019, 18, 1–10. [Google Scholar] [CrossRef]
- Chenneville, T.; Gabbidon, K.; Drake, H.; Rodriguez, L. Preliminary findings from the HIV SEERs Project: A community-based participatory research project to reduce HIV stigma among youth in Kenya. J. Assoc. Nurses AIDS Care 2019. [Google Scholar] [CrossRef]
- Roy-Campbell, Z.M. Teaching English as a “second language” in Kenya and the United States: Convergences and divergences. Glob. Educ. Rev. 2015, 2, 84–97. [Google Scholar]
- Carey, M.P.; Schroder, K.E. Development and psychometric evaluation of the brief HIV Knowledge Questionnaire. AIDS Educ. Prev. 2002, 14, 172–182. [Google Scholar] [CrossRef]
- Kalichman, S.C.; Simbayi, L.C.; Jooste, S.; Toefy, Y.; Cain, D.; Cherry, C.; Kagee, A. Development of a brief scale to measure AIDS-related stigma in South Africa. AIDS Behav. 2005, 9, 135–143. [Google Scholar] [CrossRef]
- Weiss, R. The provisions of social relationships. In Doing Unto Others; Rubin, Z., Ed.; Prentice Hall: Englewood Cliffs, NJ, USA, 1974; pp. 17–26. [Google Scholar]
- Cutrona, C.E.; Russell, D.W. The provisions of social relationships and adaptation to stress. Adv. Pers. Relatsh. 1987, 1, 37–67. [Google Scholar]
- Layard, R. Measuring subjective well-being. Science 2010, 327, 534–535. [Google Scholar] [CrossRef]
- Lovibond, S.H.; Lovibond, P.F. Manual for the Depression Anxiety Stress Scales, 2nd ed.; Psychology Foundation: Sydney, Australia, 1995. [Google Scholar]
- Antony, M.M.; Bieling, P.J.; Cox, B.J.; Enns, M.W.; Swinson, R.P. Psychometric properties of the 42-item and 21-item versions of the Depression Anxiety Stress Scales in clinical groups and a community sample. Psychol. Assess. 1998, 10, 176. [Google Scholar] [CrossRef]
- Knight, J.R.; Shrier, L.A.; Bravender, T.D.; Farrell, M.; Vander Bilt, J.; Shaffer, H.J. A new brief screen for adolescent substance abuse. Arch. Pediatr. Adolesc. Med. 1999, 153, 591–596. [Google Scholar] [CrossRef]
- Lee, K.; Koval, J.J. Determination of the best significance level in forward stepwise logistic regression. Commun. Stat.-Simul. Comput. 1997, 26, 559–575. [Google Scholar] [CrossRef]
- Luseno, W.K.; Wechsberg, W.M. Correlates of HIV testing among South African women with high sexual and substance-use risk behaviours. AIDS Care 2009, 21, 178–184. [Google Scholar] [CrossRef] [Green Version]
- Altice, F.L.; Kamarulzaman, A.; Soriano, V.V.; Schechter, M.; Friedland, G.H. Series: Treatment of medical, psychiatric, and substance-use comorbidities in people infected with HIV who use drugs. Lancet 2010, 376, 367–387. [Google Scholar] [CrossRef]
- Simeone, C.A.; Seal, S.M.; Savage, C. Feature: Implementing HIV Testing in Substance Use Treatment Programs: A Systematic Review. J. Assoc. Nurses AIDS Care 2017, 28, 199–215. [Google Scholar] [CrossRef]
- Hamra, M.; Ross, M.W.; Orrs, M.; D’Agostino, A. Relationship between expressed HIV/AIDS-related stigma and HIV-beliefs/knowledge and behaviour in families of HIV infected children in Kenya. Trop. Med. Int. Health 2006, 11, 513–527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tavakol, A.; Dennick, R. Making sense of cronbach’s alpha. Int. J. Med. Educ. 2011, 2, 53–55. [Google Scholar] [CrossRef] [PubMed]
- Spiliotopoulou, G. Reliability reconsidered: Cronbach’s alpha and paediatric assessment in occupational therapy. Aust. Occup. Ther. J. 2009, 56, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Montano, D.E.; Kaspryzyk, D. Theory of reasoned action, theory of planned behavior, and the integrated behavioral model. In Health Behavior: Theory, Research, and Practice, 5th ed.; Glanz, K., Rimer, B.K., Viswanath, K., Eds.; Wiley: San Francisco, CA, USA, 2015; pp. 67–96. [Google Scholar]
- Fernandez, M.I.; Collazo, J.B.; Bowen, G.S.; Varga, L.M.; Hernandez, N.; Perrino, T. Predictors of HIV testing and intention to test among Hispanic farmworkers in south Florida. J. Rural Health 2005, 21, 56–64. [Google Scholar] [CrossRef] [PubMed]
- MacKeller, D.; Hou, S.; Whalen, C.C.; Samuelsen, K.; Sanchez, T.; Smith, A.; Denson, D.; Lansky, A.; Sullivan, P. Reasons for not HIV testing, testing intentions, and potential use of an over-the-counter rapid HIV test in an internet sample of men who have sex with men who have never tested for HIV. Sex. Transm. Dis. 2011, 38, 419–428. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Exp(B) | b | S.E.(b) | χ2 | p |
|---|---|---|---|---|---|
| HIV knowledge | 1.091 | 0.087 | 0.035 | 6.186 | 0.013 |
| Substance use | 1.413 | 0.346 | 0.128 | 7.334 | 0.007 |
| Depression | 0.981 | −0.019 | 0.010 | 3.716 | 0.054 |
| Social support | 0.976 | −0.024 | 0.012 | 3.682 | 0.055 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nall, A.; Chenneville, T.; Rodriguez, L.M.; O’Brien, J.L. Factors Affecting HIV Testing among Youth in Kenya. Int. J. Environ. Res. Public Health 2019, 16, 1450. https://doi.org/10.3390/ijerph16081450
Nall A, Chenneville T, Rodriguez LM, O’Brien JL. Factors Affecting HIV Testing among Youth in Kenya. International Journal of Environmental Research and Public Health. 2019; 16(8):1450. https://doi.org/10.3390/ijerph16081450
Chicago/Turabian StyleNall, Allison, Tiffany Chenneville, Lindsey M. Rodriguez, and Jennifer L. O’Brien. 2019. "Factors Affecting HIV Testing among Youth in Kenya" International Journal of Environmental Research and Public Health 16, no. 8: 1450. https://doi.org/10.3390/ijerph16081450