Sleep Quality among Police Officers: Implications and Insights from a Systematic Review and Meta-Analysis of the Literature

 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Questionnaire
2.2. Search Strategy
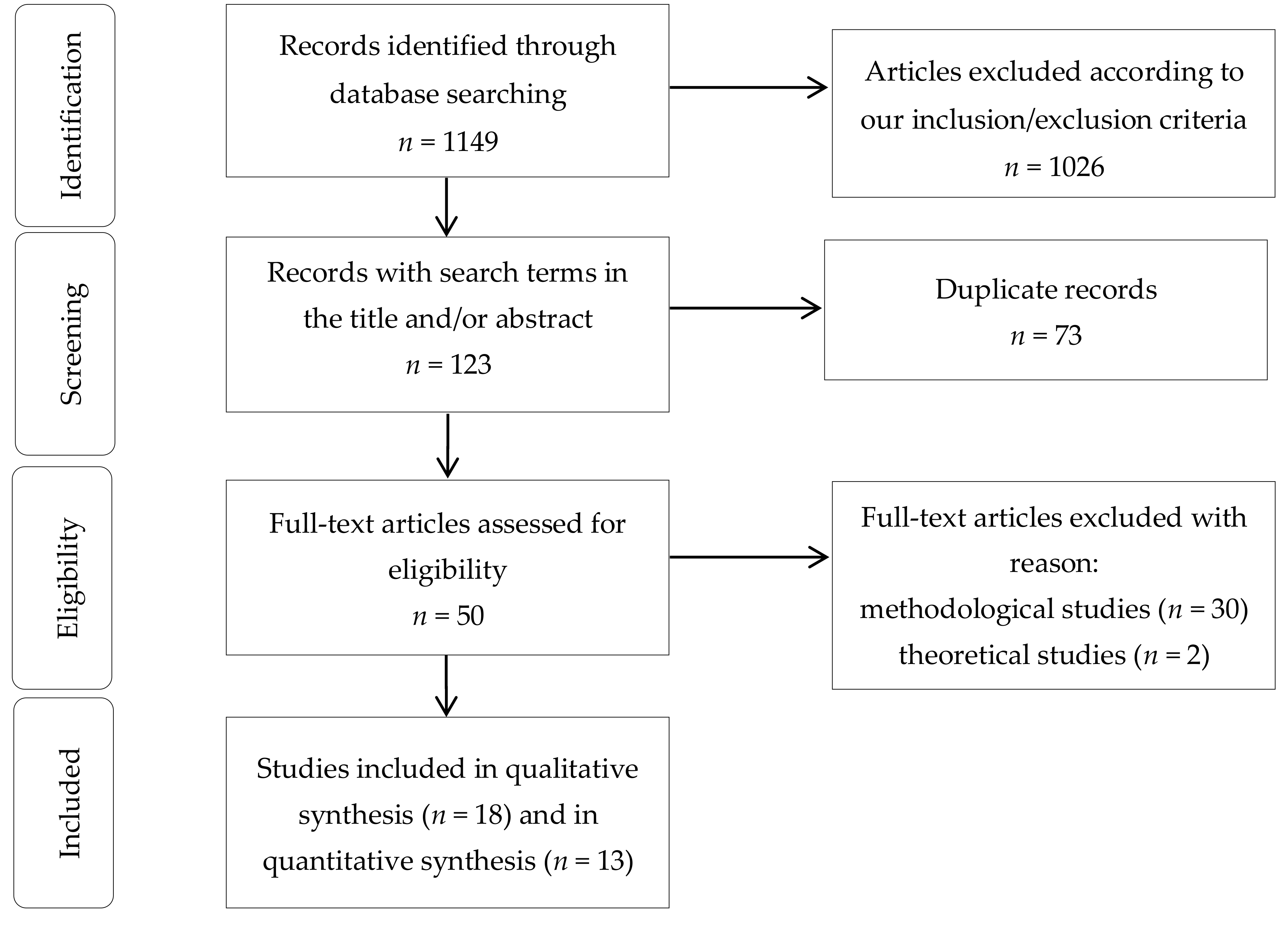
2.3. Selection of Published Studies
2.4. Study Quality Assessment
2.5. Data Extraction and Analysis
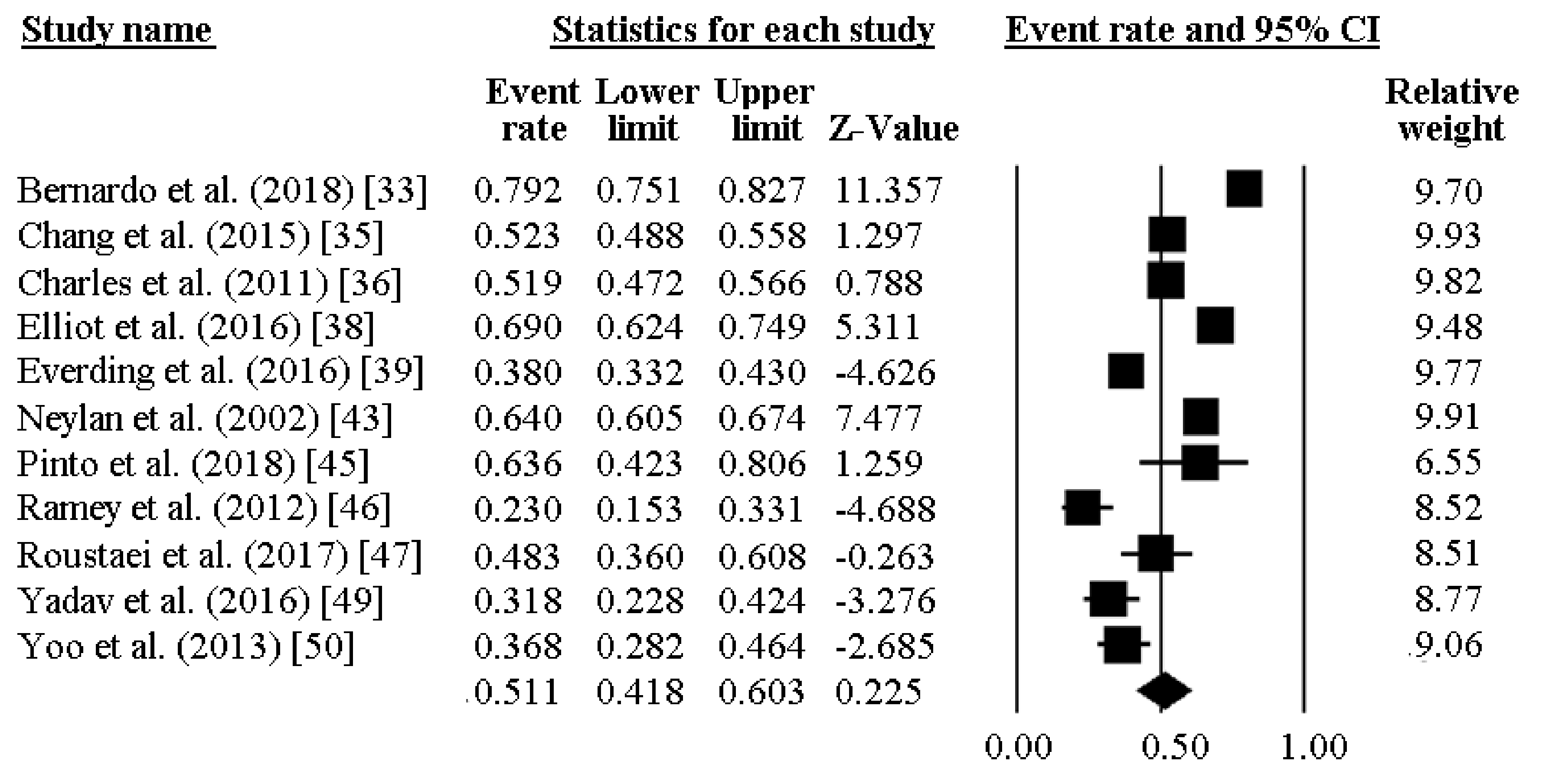
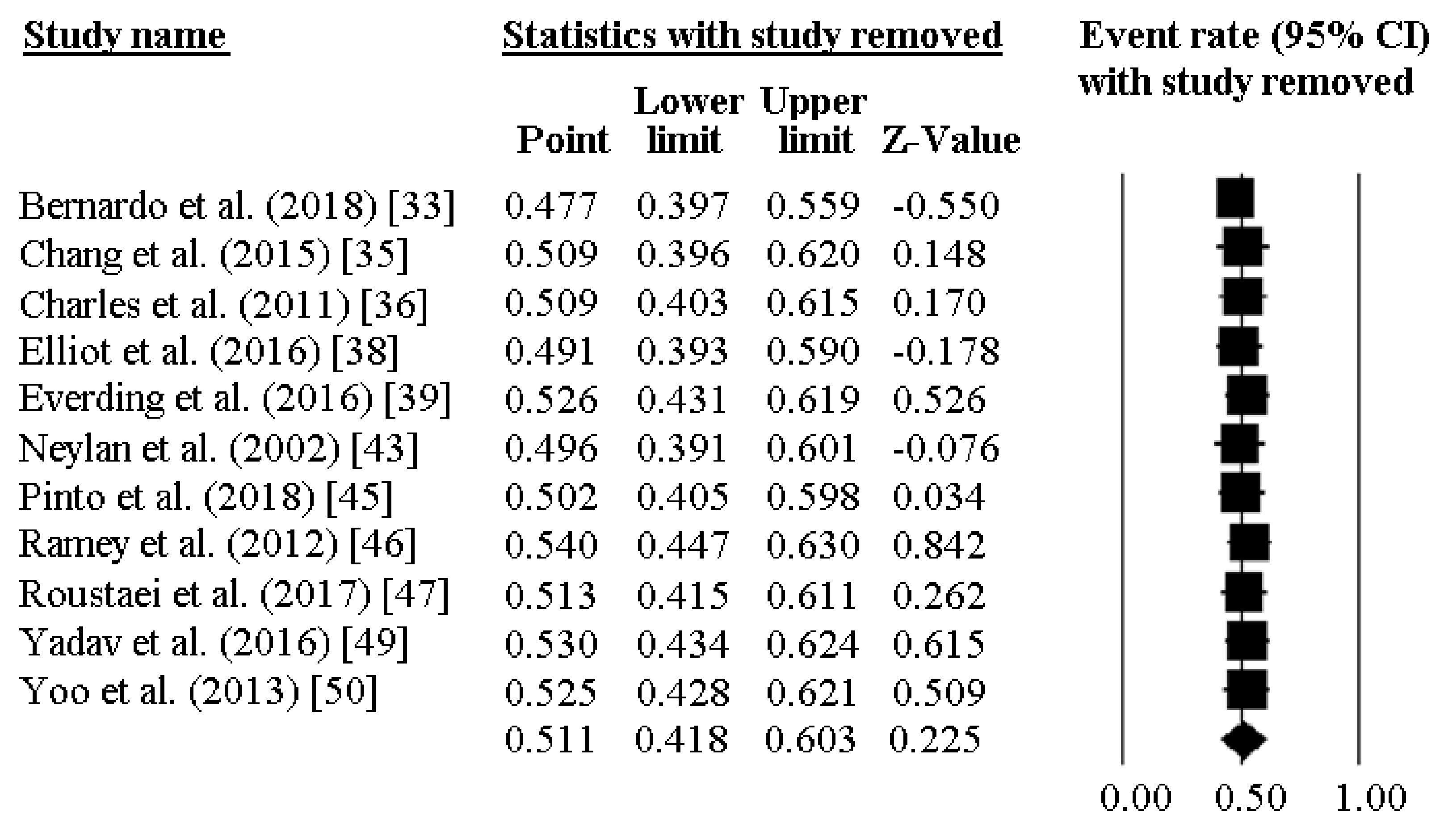
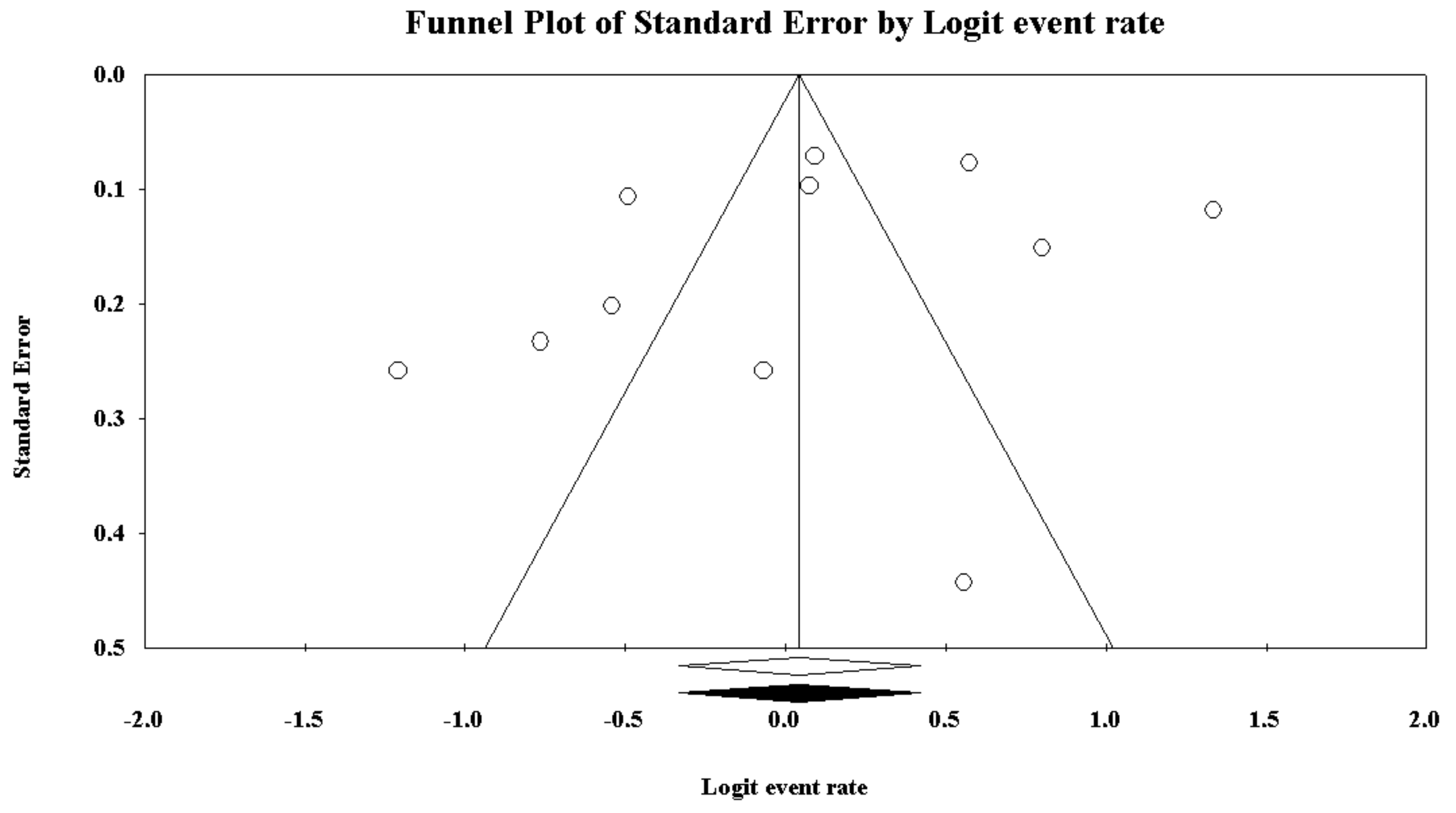
2.6. Quantitative Data Synthesis
2.7. Statistical Software
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Simonelli, G.; Marshall, N.S.; Grillakis, A.; Miller, C.B.; Hoyos, C.M.; Glozier, N. Sleep health epidemiology in low and middle-income countries: A systematic review and meta-analysis of the prevalence of poor sleep quality and sleep duration. Sleep Health 2018, 4, 239–250. [Google Scholar] [CrossRef] [PubMed]
- Min, C.; Kim, H.J.; Park, I.S.; Park, B.; Kim, J.H.; Sim, S.; Choi, H.G. The association between sleep duration, sleep quality, and food consumption in adolescents: A cross-sectional study using the Korea Youth Risk Behavior Web-based Survey. BMJ Open 2018, 8, e022848. [Google Scholar] [CrossRef] [PubMed]
- Rahe, C.; Czira, M.E.; Teismann, H.; Berger, K. Associations between poor sleep quality and different measures of obesity. Sleep Med. 2015, 16, 1225–1228. [Google Scholar] [CrossRef] [PubMed]
- Nixon, J.P.; Mavanji, V.; Butterick, T.A.; Billington, C.J.; Kotz, C.M.; Teske, J.A. Sleep disorders, obesity, and aging: The role of orexin. Ageing Res. Rev. 2015, 20, 63–73. [Google Scholar] [CrossRef] [PubMed]
- Okubo, N.; Matsuzaka, M.; Takahashi, I.; Sawada, K.; Sato, S.; Akimoto, N.; Umeda, T.; Nakaji, S. Hirosaki University Graduate School of Medicine. Relationship between self-reported sleep quality and metabolic syndrome in general population. BMC Public Health 2014, 14, 562. [Google Scholar] [CrossRef] [PubMed]
- Hoevenaar-Blom, M.P.; Spijkerman, A.M.; Kromhout, D.; van den Berg, J.F.; Verschuren, W.M. Sleep duration and sleep quality in relation to 12-year cardiovascular disease incidence: The MORGEN study. Sleep 2011, 34, 1487–1492. [Google Scholar] [CrossRef] [PubMed]
- St-Onge, M.P.; Grandner, M.A.; Brown, D.; Conroy, M.B.; Jean-Louis, G.; Coons, M.; Bhatt, D.L. American Heart Association Obesity, Behavior Change, Diabetes, and Nutrition Committees of the Council on Lifestyle and Cardiometabolic Health; Council on Cardiovascular Disease in the Young; Council on Clinical Cardiology; and Stroke Council. Sleep duration and quality: Impact on lifestyle behaviors and cardiometabolic health: A scientific statement from the American Heart Association. Circulation 2016, 134, e367–e386. [Google Scholar] [PubMed]
- Dlugaj, M.; Weinreich, G.; Weimar, C.; Stang, A.; Dragano, N.; Wessendorf, T.E.; Teschler, H.; Winkler, A.; Wege, N.; Moebus, S.; et al. Sleep-disordered breathing, sleep quality, and mild cognitive impairment in the general population. J. Alzheimers Dis. 2014, 41, 479–497. [Google Scholar] [CrossRef] [PubMed]
- Paunio, T.; Korhonen, T.; Hublin, C.; Partinen, M.; Koskenvuo, K.; Koskenvuo, M.; Kaprio, J. Poor sleep predicts symptoms of depression and disability retirement due to depression. J. Affect. Disord. 2015, 172, 381–389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garbarino, S.; Lanteri, P.; Durando, P.; Magnavita, N.; Sannita, W.G. Co-Morbidity, Mortality, Quality of Life and the Healthcare/Welfare/Social Costs of Disordered Sleep: A Rapid Review. Int. J. Environ. Res. Public Health 2016, 13, 831. [Google Scholar] [CrossRef] [PubMed]
- Garbarino, S.; Guglielmi, O.; Sanna, A.; Mancardi, G.L.; Magnavita, N. Risk of occupational accidents in workers with obstructive sleep apnea: Systematic review and meta-analysis. Sleep 2016, 39, 1211–1218. [Google Scholar] [CrossRef] [PubMed]
- Garbarino, S.; Magnavita, N.; Guglielmi, O.; Maestri, M.; Dini, G.; Bersi, F.M.; Toletone, A.; Chiorri, C.; Durando, P. Insomnia is associated with road accidents. Further evidence from a study on truck drivers. PLoS ONE 2017, 12, e0187256. [Google Scholar] [CrossRef]
- Garbarino, S.; Durando, P.; Guglielmi, O.; Dini, G.; Bersi, F.; Fornarino, S.; Toletone, A.; Chiorri, C.; Magnavita, N. Sleep apnea, sleep debt and daytime sleepiness are independently associated with road accidents. A cross-sectional study on truck drivers. PLoS ONE 2016, 11, e0166262. [Google Scholar] [CrossRef] [PubMed]
- Magnavita, N.; Garbarino, S. Sleep, health and wellness at work: A scoping review. Int. J. Environ. Res. Public Health 2017, 14, 1347. [Google Scholar] [CrossRef] [PubMed]
- Uehli, K.; Mehta, A.J.; Miedinger, D.; Hug, K.; Schindler, C.; Holsboer-Trachsler, E.; Leuppi, J.D.; Künzli, N. Sleep problems and work injuries: A systematic review and meta-analysis. Sleep Med. Rev. 2014, 18, 61–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.C.; Kim, B.K.; Min, K.B.; Min, J.Y.; Hwang, S.H.; Park, S.G. Association between job stress and insomnia in Korean workers. J. Occup. Health 2011, 53, 164–174. [Google Scholar] [PubMed]
- Van Laethem, M.; Beckers, D.G.; Kompier, M.A.; Kecklund, G.; van den Bossche, S.N.; Geurts, S.A. Bidirectional relations between work-related stress, sleep quality and perseverative cognition. J. Psychosom. Res. 2015, 79, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Åkersted, T.; Kecklund, G.; Gillberg, M. Sleep and sleepiness in relation to stress and displaced work hours. Physiol Behav 2007, 92, 250–255. [Google Scholar] [CrossRef] [PubMed]
- Ekstedt, M.; Södeström, M.; Åkerstedt, T.; Nilsson, J.; Søndergaard, H.P.; Aleksander, P. Disturbed sleep and fatigue in occupational burnout. Scand. J. Work Environ. Health 2006, 32, 121–131. [Google Scholar] [PubMed]
- Habersaat, S.A.; Geiger, A.M.; Abdellaoui, S.; Wolf, J.M. Health in police officers: Role of risk factor clusters and police divisions. Soc. Sci. Med. 2015, 143, 213–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santana, A.M.; Gomes, J.K.; De Marchi, D.; Girondoli, Y.M.; Rosado, L.E.; Rosado, G.P.; de Andrade, I.M. Occupational stress, working condition and nutritional status of military police officers. Work 2012, 41, 2908–2914. [Google Scholar] [CrossRef] [PubMed]
- Dubrow, R.; Burnett, C.A.; Gute, D.M.; Brockert, J.E. Ischemic heart disease and acute myocardial infarction mortality among police officers. J. Occup. Med. 1998, 30, 650–654. [Google Scholar]
- Garbarino, S.; Magnavita, N. Work Stress and metabolic syndrome in police officers. A prospective study. PLoS ONE 2015, 10, e0144318. [Google Scholar] [CrossRef] [PubMed]
- Garbarino, S.; Cuomo, G.; Chiorri, C.; Magnavita, N. Association of work-related stress with mental health problems in a special police force unit. BMJ Open 2013, 3, e002791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajaratnam, S.M.; Barger, L.K.; Lockley, S.W.; Shea, S.A.; Wang, W.; Landrigan, C.P.; O’ Brien, C.S.; Qadri, S.; Sullivan, J.P.; Cade, B.E.; et al. Sleep disorders, health, and safety in police officers. JAMA 2011, 306, 2567–2578. [Google Scholar] [CrossRef] [PubMed]
- Garbarino, S.; De Carli, F.; Nobili, L.; Mascialino, B.; Squarcia, S.; Penco, M.A.; Beelke, M.; Ferrillo, F. Sleepiness and sleep disorders in shift workers: A study on a group of Italian police officers. Sleep 2002, 25, 648–653. [Google Scholar] [PubMed]
- Garbarino, S. 24-Hour work: The interaction of stress and changes in the sleep-wake cycle in the police force. G. Ital. Med. Lav. Ergon. 2014, 36, 392–396. [Google Scholar] [PubMed]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [PubMed]
- Mollayeva, T.; Thurairajah, P.; Burton, K.; Mollayeva, S.; Shapiro, C.M.; Colantonio, A. The Pittsburgh sleep quality index as a screening tool for sleep dysfunction in clinical and non-clinical samples: A systematic review and meta-analysis. Sleep Med. Rev. 2016, 25, 52–73. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.A.; Shea, B.; O’Connel, D.; Petersen, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analyses. 2012. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 5 September 2018).
- Greenland, S. Variance estimators for attributable fraction estimates consistent in both large strata and sparse data. Stat. Med. 1987, 6, 701–708. [Google Scholar] [PubMed]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. Introduction to Meta-Analysis; Wiley: Chichester, UK, 2011. [Google Scholar]
- Bernardo, V.M.; Cascaes da Silva, F.; Goncalves Ferreira, E.; Bento, G.G.; Zilch, M.C.; Andrade de Sousa, B.; da Silva, R. Actividade fisica e qualidade do sono em policiais militares. Physical activity and sleep quality in military police officers. Rev. Bras. Cienc. Esporte 2018, 408, 131–137. [Google Scholar] [CrossRef]
- Bond, J.; Hartley, T.A.; Sarkisian, K.; Andrew, M.E.; Charles, L.E.; Violanti, J.M.; Burchfiel, C.M. Association of traumatic police event exposure with sleep quality and quantity in the BCOPS Study cohort. Int. J. Emerg. Ment. Health 2013, 15, 255–265. [Google Scholar] [PubMed]
- Chang, J.H.; Huang, P.T.; Lin, Y.K.; Lin, C.E.; Lin, C.M.; Shieh, Y.H.; Lin, Y.C. Association between sleep duration and sleep quality, and metabolic syndrome in Taiwanese police officers. Int. J. Occup. Med. Environ. Health 2015, 28, 1011–1023. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charles, L.E.; Slaven, J.E.; Mnatsakanova, A.; Ma, C.; Violanti, J.M.; Fekedulegn, D.; Andrew, M.E.; Vila, B.J.; Burchfiel, C.M. Association of perceived stress with sleep duration and sleep quality in police officers. Int. J. Emerg. Ment. Health 2011, 13, 229–241. [Google Scholar] [PubMed]
- Chopko, B.A.; Palmieri, P.A.; Adams, R.E. Trauma-related sleep problems and associated health outcomes in police officers: A path analysis. J. Interpers. Violence 2018. [Google Scholar] [CrossRef]
- Elliott, J.L.; Lal, S. Blood pressure, sleep quality and fatigue in shift working police officers: Effects of a twelve hour roster system on cardiovascular and sleep health. Int. J. Environ. Res. Public Health 2016, 13, 172. [Google Scholar] [CrossRef] [PubMed]
- Everding, B.; Hallam, J.E.; Kohut, M.L.; Lee, D.C.; Anderson, A.A.; Franke, W.D. Association of sleep quality with cardiovascular disease risk and mental health in law enforcement officers. J. Occup. Environ. Med. 2016, 58, e281–e286. [Google Scholar] [CrossRef] [PubMed]
- Fekedulegn, D.; Burchfiel, C.M.; Charles, L.E.; Hartley, T.A.; Andrew, M.E.; Violanti, J.M. Shift Work and Sleep Quality Among Urban Police Officers: The BCOPS Study. J. Occup. Environ. Med. 2016, 58, e66–e71. [Google Scholar] [CrossRef] [PubMed]
- Hartley, T.A.; Violanti, J.M.; Sarkisian, K.; Fekedulegn, D.; Mnatsakanova, A.; Andrew, M.E.; Burchfiel, C.M. Association between police-specific stressors and sleep quality: Influence of coping and depressive symptoms. J. Law Enforc. Leadersh. Ethics 2014, 1, 31–48. [Google Scholar] [PubMed]
- McCanlies, E.C.; Slaven, J.E.; Smith, L.M.; Andrew, M.E.; Charles, L.E.; Burchfiel, C.M.; Violanti, J.M. Metabolic syndrome and sleep duration in police officers. Work 2012, 43, 133–139. [Google Scholar] [PubMed]
- Neylan, T.C.; Metzler, T.J.; Best, S.R.; Weiss, D.S.; Fagan, J.A.; Liberman, A.; Rogers, C.; Vedantham, K.; Brunet, A.; Lipsey, T.L.; et al. Critical incident exposure and sleep quality in police officers. Psychosom. Med. 2002, 64, 345–352. [Google Scholar] [CrossRef] [PubMed]
- Neylan, T.C.; Metzler, T.J.; Henn-Haase, C.; Blank, Y.; Tarasovsky, G.; McCaslin, S.E.; Lenoci, M.; Marmar, C.R. Prior night sleep duration is associated with psychomotor vigilance in a healthy sample of police academy recruits. Chronobiol. Int. 2010, 27, 1493–1508. [Google Scholar] [CrossRef] [PubMed]
- Pinto, J.N.; Perin, C.; Dick, N.R.; Lazzarotto, A.R. Avaliação do sono em um grupo de policiais militares de elite. Acta Paul. Enferm. 2018, 31, 153–161. [Google Scholar] [CrossRef]
- Ramey, S.L.; Perkhounkova, Y.; Moon, M.; Budde, L.; Tseng, H.C.; Clark, M.K. The effect of work shift and sleep duration on various aspects of police officers’ health. Workplace Health Saf. 2012, 60, 215–222. [Google Scholar] [CrossRef] [PubMed]
- Roustaei, N.; Jamali, H.; Jamali, M.R.; Nourshargh, P.; Jamali, J. The association between quality of sleep and health-related quality of life in military and non-military women in Tehran, Iran. Oman Med. J. 2017, 32, 134-130. [Google Scholar] [CrossRef] [PubMed]
- Slaven, J.E.; Mnatsakanova, A.; Burchfiel, C.M.; Smith, L.M.; Charles, L.E.; Andrew, M.E.; Gu, J.K.; Ma, C.; Fekedulegn, D.; Violanti, J.M. Association of sleep quality with depression in police officers. Int. J. Emerg. Ment. Health 2011, 13, 267–277. [Google Scholar] [PubMed]
- Yadav, A.; Rani, S.; Singh, S. Working “out-of-phase” with reference to chronotype compromises sleep quality in police officers. Chronobiol. Int. 2016, 33, 151–160. [Google Scholar] [CrossRef] [PubMed]
- Yoo, H.; Franke, W.D. Sleep habits, mental health, and the metabolic syndrome in law enforcement officers. J. Occup. Environ. Med. 2013, 55, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Garbarino, S.; Magnavita, N.; Elovainio, M.; Heponiemi, T.; Ciprani, F.; Cuomo, G.; Bergamaschi, A. Police job strain during routine activities and a major event. Occup. Med. 2011, 61, 395–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeitlhofer, J.; Schmeiser-Rieder, A.; Tribl, G.; Rosenberger, A.; Bolitschek, J.; Kapfhammer, G.; Saletu, B.; Katschnig, H.; Holzinger, B.; Popovic, R.; et al. Sleep and quality of life in the Austrian population. Acta Neurol. Scand. 2000, 102, 249–257. [Google Scholar] [CrossRef] [PubMed]
- Wong, W.S.; Fielding, R. Prevalence of insomnia among Chinese adults in Hong Kong: A population-based study. J Sleep Res 2011, 20, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Hinz, A.; Glaesmer, H.; Brähler, E.; Löffler, M.; Engel, C.; Enzenbach, C.; Hegerl, U.; Sander, C. Sleep quality in the general population: Psychometric properties of the Pittsburgh Sleep Quality Index, derived from a German community sample of 9284 people. Sleep Med. 2017, 30, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Guglielmi, O.; Magnavita, N.; Garbarino, S. Sleep quality, obstructive sleep apnea, and psychological distress in truck drivers: A cross-sectional study. Soc. Psychiatry Psychiatr. Epidemiol. 2018, 53, 531–536. [Google Scholar] [CrossRef] [PubMed]
- Vargas de Barros, V.; Martins, L.F.; Saitz, R.; Bastos, R.R.; Ronzani, T.M. Mental health conditions, individual and job characteristics and sleep disturbances among firefighters. J. Health Psychol. 2013, 18, 350–358. [Google Scholar] [CrossRef] [PubMed]
- Cho, H.S.; Kim, Y.W.; Park, H.W.; Lee, K.H.; Jeong, B.G.; Kang, Y.S.; Park, K.S. The relationship between depressive symptoms among female workers and job stress and sleep quality. Ann. Occup. Environ. Med. 2013, 25, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kara, N. Effect of sleep quality on psychiatric symptoms and life quality in newspaper couriers. Noro Psikiyatr. Ars. 2016, 53, 102–107. [Google Scholar] [CrossRef] [PubMed]
- Monk, T.H.; Buysse, D.J.; Billy, B.D.; Fletcher, M.E.; Kennedy, K.S. Polysomnographic sleep and circadian temperature rhythms as a function of prior shift work exposure in retired seniors. Healthy Aging Clin. Care Elder 2013, 2013, 9–19. [Google Scholar] [PubMed]
- Garbarino, S.; Guglielmi, O.; Sannita, W.G.; Magnavita, N.; Lanteri, P. Sleep and mental health in truck drivers: Descriptive review of the current evidence and proposal of strategies for primary prevention. Int. J. Environ. Res. Public Health 2018, 15, 1852. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Year) | Type of Study, Quality | Sample Country) | Mean Age (% fem) | BMI Mean (SD) | Smoking Status (%) | Alcohol Intake | Married (%) | Caucasians and Hispanics (%) | Education (High–School %) | Years of Service (Work Hours per Day) | Hierarchical Role (%) | Administrative Role (%) | Military/Previous Military Experience | Evening and Night–Shift (%) | Prevalence of Poor Sleep Quality | PSQI Global Score (Number of Hours of Sleep) | Main Factor Related |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Bernardo et al., (2018) [33] | Cross sec * | 438 (Brazil) | 33.2 ± 7.6 [20–53] (10.5%) | No data | No data | No data | No data | No data | No data | No data (no data) | 4.6% | 26.3% | Military police | 73.7% | 79.2% | No data (no data) | Physical activity (low, 20.5%) |
| Bond et al., (2013) [34] | Cross sec ** | 372 (USA) | 41.3 ± 6.7 (27.7%) | 29.1 ± 4.7 | 39.7% | 5.6 ± 9.4 | 72.9% | 79.3% | 10.5% | 14.6 ± 7.0 (high 63.8%) | 16.6% | No data | 22.3% | 59.3% | 54.8% | 6.5 (6.1 ± 1.2) | Traumatic event exposure |
| Chang et al., (2015) [35] | Cross sec ** | 796 (China) | 37.4 ± 7.7 [20–60] (0%) | 25.2 ± 3.6 | 43.1% | 1.8% | No data | No data | No data | No data | No data | No data | No data | 52.5% | 52.3% | 6.1 ± 3.1 (6.1 ± 1.1) | Met S, shift work |
| Charles et al., (2011) [36] | Cross sec ** | 430 (USA) | 42.1 ± 8.4 (25.8%) | 29.2 ± 4.8 | 41.4% | 5.6 ± 9.5 | No data | 80% | 11% | No data (high 36.0%) | 15.7% | No data | 25.4% | 57.6% | 51.9% | No data (6.1 ± 1.2) | Perceived stress |
| Chopko et al. (2018) [37] | Cross sec * | 193 (USA) | 41.6 ± 9.2 [23–63] (6.7%) | No data | No data | No data | 82.4% | 93.3% | 14.7 ± 1.9 years [12–22] | 16.4 ± 8.9 [1–42] | 15% | No data | No data | No data | No data | 4.8 ± 3.1 (no data) | PTSD, general health |
| Elliot et al., (2016) [38] | Cross sec * | 206 (Australia) | 31.6 ± 8.5 (32%) | No data | No data | No data | No data | No data | No data | 6.4 ± 7.5 | 17.5% | No data | No data | 44.7% | 69% | 6.8 ± 3.6(no data) | Blood pres., fatigue, card. diseases |
| Everding et al., (2016) [39] | Cross sec * | 379 (USA) | 41.5 ± 8.6 (6%) | 28.8 ± 3.9 | No data | No data | No data | No data | No data | No data | No data | No data | No data | No data | 38% | 5.4 ± 3.1 (no data) | Card. disease and mental health, inflammatory markers |
| Fekedulegn et al., (2016) [40] | Cross sec ** | 363 (USA) | 41.2 ± 6.6 [27–66] (28%) | 29.2 ± 4.7 (BMI>25 81%) | 39.3% | 5.5 ± 9.4 | 72.2% | 76.5% | 10.5% | 14.4 ± 6.8 (high 64%) | 28.1% | No data | No data | 50.4% | 54% | No data (no data) | Shift work |
| Hartley et al., (2014) [41] | Cross sec ** | 356 (USA) | 41.3 ± 6.7 (28%) | 29.2 ± 4.7 | 40.4% | 5.6 ± 9.4 | 73.9% | 79.5% | 10.7% | 49% ≥15 years (no data) | 28.1% | No data | 21.4% | 59.9% | 54.2% | 6.5 ± 3.4 (6.1 ± 1.2) | Stress |
| McCanlies et al., (2012) [42] | Cross sec ** | 98 (USA) | 39.6 (39.8%) | No data | 53.1% | No data | 65.3% | 81.6% | 18.4% | No data | 34.7% | No data | No data | No data | No data | No data (6.4) | Met S |
| Neylan et al., (2002) [43] | Cross sec ** | 733 (USA) | 37.0 (29%) | No data | No data | No data | 68.8& | 69% | 28% | 12.6 (no data) | No data | No data | No data | No data | 64% | 6.1 ± 3.2 * | Critical incidents |
| Neylan et al., (2010) [44] | Cross sec * | 189 (USA) | 26.4 ± 4.2 [21–43] (12%) | No data | No data | No data | No data | No data | No data | No data | No data | No data | No data | 0% | No data | 3.5 ± 2.1 (6.25 ± 1.70) | Psychomotor performance |
| Pinto et al., (2018) [45] | Cross sec * | 22 (Brazil) | 34.6 ± 6.1 (0%) | 25.2 [23–31] | No data | No data | No data | No data | 22.7% | 9 [6–25] (No data) | 27.2% | No data | Military | No data | 63.6% | 5.5 ± 3.0 *(6.5 ± 0.8) | QoL, work accidents |
| Ramey et al., (2012) [46] | Cross sec * | 85 (USA) | 39.6 ± 9.0 [22.4–63.3] (0%) | 80%> 25 | No data | No data | No data | No data | No data | No data (45.9 ± 7.5 [8–70]) | No data | No data | No data | 41/85 (48.2%) | 23% | 5.9 ± 2.9 [2–13] (6.8 ± 1.3 [3.5–9.5]) | Shift work |
| Roustaei et al., (2017) [47] | Cross sec * | 60 (Iran) | No data (100%) | No data | No data | No data | No data | No data | No data | No data | No data | 50% | No data | No data | 48.3% | 6.1 (no data) | QoL |
| Slaven et al., (2011) [48] | Cross sec ** | 391 (USA) | 40.7 ± 7.1 (27.4%) | No data | 40% | 5.4 ± 9.2 | 73% | 80% | 10% | No data | No data | No data | No data | No data | 66.2% | 6.5 ± 3.4 (no data) | Depression |
| Yadav et al., (2016) [49] | Cross sec * | 85 (India) | 26.6 ± 0.6 (60%) | 22.9 ± 0.2 | No data | No data | No data | No data | No data | No data | No data | No data | No data | No data | 31.8% | No data (no data) | Chronotype and duty schedule |
| Yoo et al., (2013) [50] | Cross sec * | 106 (USA) | 42.3 ± 8.4 (0%) | 29.7 ± 4.1 | No data | No data | No data | No data | No data | No data | No data | No data | No data | No data | 36.8% | 5.4 ± 3.4 (no data) | Met S, mental health |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garbarino, S.; Guglielmi, O.; Puntoni, M.; Bragazzi, N.L.; Magnavita, N. Sleep Quality among Police Officers: Implications and Insights from a Systematic Review and Meta-Analysis of the Literature. Int. J. Environ. Res. Public Health 2019, 16, 885. https://doi.org/10.3390/ijerph16050885
Garbarino S, Guglielmi O, Puntoni M, Bragazzi NL, Magnavita N. Sleep Quality among Police Officers: Implications and Insights from a Systematic Review and Meta-Analysis of the Literature. International Journal of Environmental Research and Public Health. 2019; 16(5):885. https://doi.org/10.3390/ijerph16050885
Chicago/Turabian StyleGarbarino, Sergio, Ottavia Guglielmi, Matteo Puntoni, Nicola Luigi Bragazzi, and Nicola Magnavita. 2019. "Sleep Quality among Police Officers: Implications and Insights from a Systematic Review and Meta-Analysis of the Literature" International Journal of Environmental Research and Public Health 16, no. 5: 885. https://doi.org/10.3390/ijerph16050885