Associations of Genetic Variations in ABCA1 and Lifestyle Factors with Coronary Artery Disease in a Southern Chinese Population with Dyslipidemia: A Nested Case-Control Study

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Subjects
2.2. Diagnostic Criteria
2.3. Epidemiological Investigation
2.4. SNP Selection and Genotyping
2.5. Statistical Analysis
3. Results
3.1. Basic Characteristics, Lifestyle Factors, and Genotype Distribution in Case and Control Groups
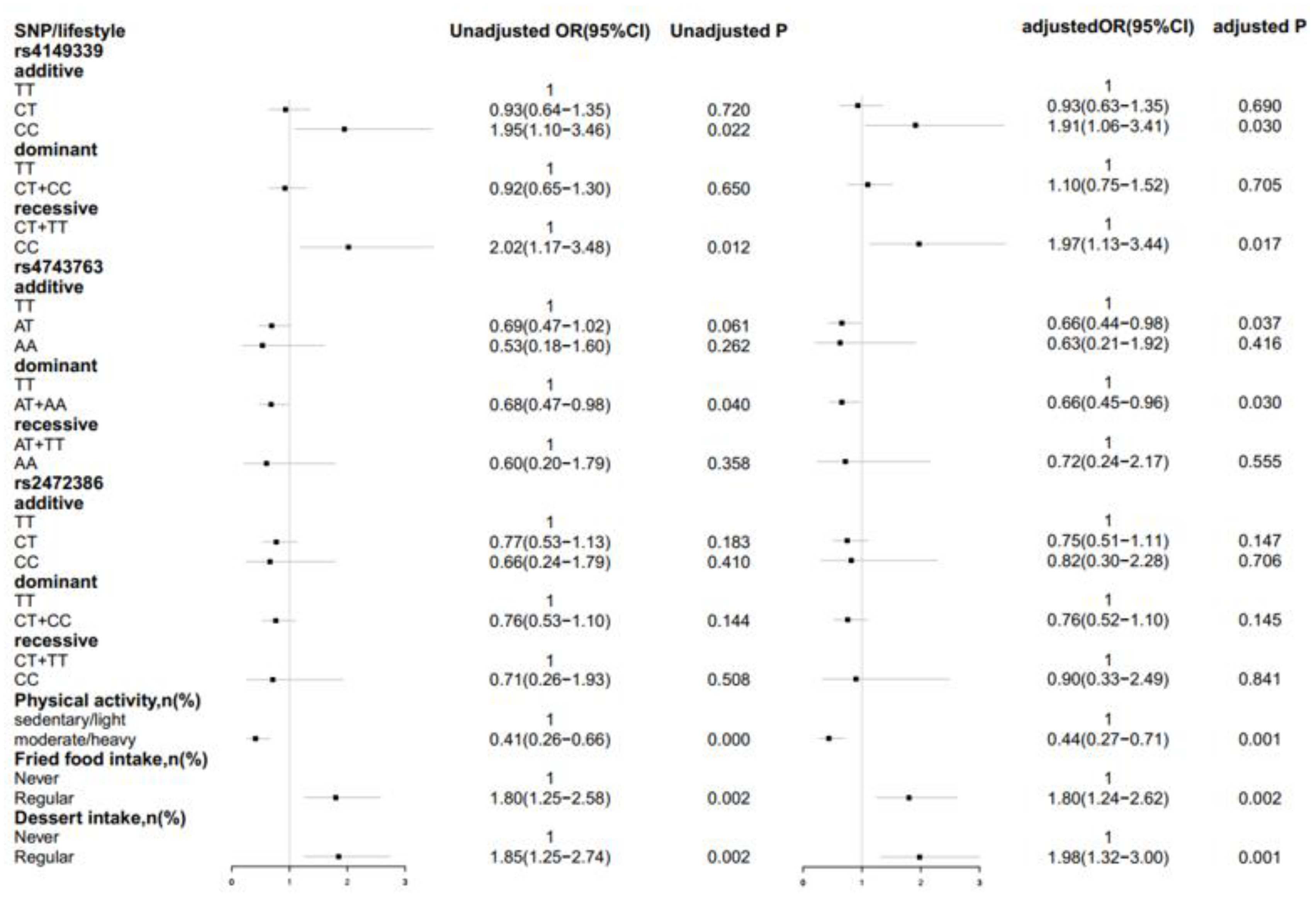
3.2. Associations of Genetic Models and Lifestyle Factors with the Risk of CAD
3.3. Interactions of ABCA1 SNPs and Lifestyle Factors with CAD in Dyslipidemia
3.4. Association of ABCA1 Haplotypes with CAD Risk
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Bibbins-Domingo, K. Aspirin Use for the Primary Prevention of Cardiovascular Disease and Colorectal Cancer: U.S. Preventive Services Task Force Recommendation Statement. Ann. Intern. Med. 2016, 164, 836–845. [Google Scholar] [CrossRef] [PubMed]
- Weiwei, C.; Runlin, G.; LIsheng, L.; Manlu, Z.; Wen, W. Summary of Chinese cardiovascular disease report 2017. Chin. Circ. J. 2018, 33, 1–8. [Google Scholar]
- Wen, Y.; Leake, D.S. Low density lipoprotein undergoes oxidation within lysosomes in cells. Circ. Res. 2007, 100, 1337–1343. [Google Scholar] [CrossRef] [PubMed]
- The Emergency Risk Factors Collaboration. Major lipids, apolipoproteins, and risk of vascular disease. JAMA 2009, 302, 1993–2000. [Google Scholar] [CrossRef]
- Jacobson, T.A.; Ito, M.K.; Maki, K.C.; Orringer, C.E.; Bays, H.E.; Jones, P.H.; McKenney, J.N.; Grundy, S.M.; Gill, E.A.; Wild, R.A.; et al. National lipid association recommendations for patient-centered management of dyslipidemia: Part 1—Full report. J. Clin. Lipidol. 2015, 9, 129–169. [Google Scholar] [CrossRef] [PubMed]
- Lewington, S.; Whitlock, G.; Clarke, R.; Sherliker, P.; Emberson, J.; Halsey, J.; Qizilbash, N.; Peto, R.; Collins, R. Blood cholesterol and vascular mortality by age, sex, and blood pressure: A meta-analysis of individual data from 61 prospective studies with 55,000 vascular deaths. Lancet 2007, 370, 1829–1839. [Google Scholar] [PubMed]
- Stone, N.J.; Robinson, J.G.; Lichtenstein, A.H.; Bairey Merz, C.N.; Blum, C.B.; Eckel, R.H.; Goldberg, A.C.; Gordon, D.; Lioyd-Jones, D.M.; et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2014, 63, 2889–2934. [Google Scholar] [CrossRef]
- Katsiki, N.; Al-Rasadi, K.; Mikhailidis, D.P. Lipoprotein (a) and Cardiovascular Risk: The Show Must go on. Curr. Med. Chem. 2017, 24, 989–1006. [Google Scholar] [CrossRef]
- Lee, J.S.; Chang, P.Y.; Zhang, Y.; Kizer, J.R.; Best, L.G.; Howard, B.V. Triglyceride and HDL-C Dyslipidemia and Risks of Coronary Heart Disease and Ischemic Stroke by Glycemic Dysregulation Status: The Strong Heart Study. Diabetes Care 2017, 40, 529–537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berkinbayev, S.; Rysuly, M.; Mussayev, A.; Blum, K.; Baitasova, N.; Mussagaliyeva, A.; Dzhunusbekova, G.; Makhatov, B.; Mussayev, A.A.; Yeshmanova, A.; et al. Apolipoprotein Gene Polymorphisms (APOB, APOC111, APOE) in the Development of Coronary Heart Disease in Ethnic Groups of Kazakhstan. J. Genet. Syndr. Gene Ther. 2014, 5, 216. [Google Scholar] [PubMed]
- Huang, Y.; Ye, H.D.; Gao, X.; Nie, S.; Hong, Q.X.; Ji, H.H.; Sun, J.; Zhou, S.J.; Fei, B.; Li, K.Q.; et al. Significant interaction of APOE rs4420638 polymorphism with HDL-C and APOA-I levels in coronary heart disease in Han Chinese men. Genet. Mol. Res. GMR 2015, 14, 13414–13424. [Google Scholar] [CrossRef] [PubMed]
- Ravnskov, U.; Lorgeril, M.; Diamond, D.M.; Hama, R.; Hamazaki, T.; Hammarskjold, B.; Hynes, N.; Kendrick, M.; Langsjoen, P.H.; Mascitelli, L.; et al. LDL-C does not cause cardiovascular disease: A comprehensive review of the current literature. Expert Rev. Clin. Pharmacol. 2018, 11, 959–970. [Google Scholar] [CrossRef] [PubMed]
- Shahid, S.U.; Cooper, J.A.; Beaney, K.E.; Li, K.; Rehman, A.; Humphries, S.E. Effect of SORT1, APOB and APOE polymorphisms on LDL-C and coronary heart disease in Pakistani subjects and their comparison with Northwick Park Heart Study II. Lipids Health Dis. 2016, 15, 83. [Google Scholar] [CrossRef] [PubMed]
- Ye, H.; Zhao, Q.; Huang, Y.; Wang, L.; Liu, H.; Wang, C.; Dai, D.; Xu, L.; Ye, M.; Duan, S. Meta-analysis of low density lipoprotein receptor (LDLR) rs2228671 polymorphism and coronary heart disease. BioMed Res. Int. 2014. [Google Scholar] [CrossRef] [PubMed]
- Zdravkovic, S.; Wienke, A.; Pedersen, N.L.; de Faire, U. Genetic influences on angina pectoris and its impact on coronary heart disease. Eur. J. Hum. Genet. EJHG 2007, 15, 872–877. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, L.; Yuan, F.; Liu, P.; Fei, L.; Huang, Y.; Xu, L.; Hao, L.; Qiu, X.; Le, Y.; Yang, X.; et al. Association between PCSK9 and LDLR gene polymorphisms with coronary heart disease: Case-control study and meta-analysis. Clin. Biochem. 2013, 46, 727–732. [Google Scholar] [CrossRef] [PubMed]
- Bornaun, H.; Oner, N.; Nisli, K.; Oztarhan, K.; Yavuz, T.; Turkoglu, U.; Dindar, A.; Omeroglu, R.E. Assessment of lipid profile and some risk factors of atherosclerosis in children whose parents had early onset coronary artery disease. Archivos Argentinos Pediatria 2017, 115, 50–54. [Google Scholar]
- Kuang, H.; Zhou, X.; Li, L.; Yi, Q.; Shou, W.; Lu, T. Early severe coronary heart disease and ischemic heart failure in homozygous familial hypercholesterolemia: A case report. Medicine 2018, 97, e12869. [Google Scholar] [CrossRef] [PubMed]
- Soumian, S.; Albrecht, C.; Davies, A.H.; Gibbs, R.G. ABCA1 and atherosclerosis. Vasc. Med. 2005, 10, 109–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; Das, S.R.; de Ferranti, S.; Despres, J.P.; Fullerton, H.J.; et al. Heart Disease and Stroke Statistics-2016 Update: A Report from the American Heart Association. Circulation 2016, 133, e38–e48. [Google Scholar] [CrossRef] [PubMed]
- Mortality rates after 10.5 years for participants in the Multiple Risk Factor Intervention Trial. Findings related to a priori hypotheses of the trial. The Multiple Risk Factor Intervention Trial Research Group. JAMA 1990, 263, 1795–1801. [CrossRef]
- Mozaffarian, D.; Micha, R.; Wallace, S. Effects on coronary heart disease of increasing polyunsaturated fat in place of saturated fat: A systematic review and meta-analysis of randomized controlled trials. PLoS Med. 2010, 7, e1000252. [Google Scholar] [CrossRef] [PubMed]
- Diagnostic Criteria for Coronary AtherscIerotic Heart Disease. Available online: http://www.nhc.gov.cn/zwgkzt/s9494/201007/47956/files/ecbd5f139b58418bb6f6197981e773f2.pdf (accessed on 1 July 2010).
- Knol, M.J.; VanderWeele, T.J. Recommendations for presenting analyses of effect modification and interaction. Int. J. Epidemiol. 2012, 41, 514–520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolovou, V.; Kolovou, G.; Marvaki, A.; Karakosta, A.; Vasilopoulos, G.; Kalogiani, A.; Degiannis, D.; Marvaki, C.; Demopoulos, C.A. ATP-binding cassette transporter A1 gene polymorphisms and serum lipid levels in young Greek nurses. Lipids Health Dis. 2011, 10, 56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolovou, V.; Marvaki, A.; Karakosta, A.; Vasilopoulos, G.; Kalogiani, A.; Mavrogeni, S.; Degiannis, D.; Marvaki, C.; Kolovou, G. Association of gender, ABCA1 gene polymorphisms and lipid profile in Greek young nurses. Lipids Health Dis. 2012, 11, 62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dean, M.; Hamon, Y.; Chimini, G. The human ATP-binding cassette (ABC) transporter superfamily. J. Lipid Res. 2001, 42, 1007–1017. [Google Scholar] [CrossRef] [PubMed]
- Oram, J.F. HDL apolipoproteins and ABCA1: Partners in the removal of excess cellular cholesterol. Arterioscler. Thromb. Vasc. Biol. 2003, 23, 720–727. [Google Scholar] [CrossRef] [PubMed]
- Von, E.A.; Nofer, J.R.; Assmann, G. High density lipoproteins and arteriosclerosis. Role of cholesterol efflux and reverse cholesterol transport. Arterioscler. Thromb. Vasc. Biol. 2001, 21, 13–27. [Google Scholar]
- Lee, J.Y.; Parks, J.S. ATP-binding cassette transporter AI and its role in HDL formation. Curr. Opin. Lipidol. 2005, 16, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Liu, Y.; Li, Y.; Zhang, H.; Yu, M.; Kanu, J.S.; Qiao, Y.; Tang, Y.; Zhen, Q.; Cheng, Y. Association of ATP-binding cassette transporter A1 gene polymorphisms with plasma lipid variability and coronary heart disease risk. Int. J. Clin. Exp. Pathol. 2015, 8, 13441–13449. [Google Scholar] [PubMed]
- Evenson, K.R.; Rosamond, W.D.; Cai, J.; Diez-Roux, A.V.; Brancati, F.L. Influence of retirement on leisure-time physical activity: The atherosclerosis risk in communities study. Am. J. Epidemiol. 2002, 155, 692–699. [Google Scholar] [CrossRef] [PubMed]
- Kohl, H.W. Physical activity and cardiovascular disease: Evidence for a dose response. Med. Sci. Sports Exerc. 2001, 33, S472–S483. [Google Scholar] [CrossRef] [PubMed]
- Leischik, R.; Foshag, P.; Strauss, M.; Garg, P.; Dworrak, B.; Littwitz, H.; Lazic, J.S.; Horlitz, M. Physical activity, cardiorespiratory fitness and carotid intima thickness: Sedentary occupation as risk factor for atherosclerosis and obesity. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 3157–3168. [Google Scholar] [PubMed]
- Stamler, J.; Neaton, J.D.; Cohen, J.D.; Cutler, J.; Eberly, L.; Grandits, G.; Kuller, L.H.; Ockene, J.; Prineas, R.; the MRFIT Research Group. Multiple risk factor intervention trial revisited: A new perspective based on nonfatal and fatal composite endpoints, coronary and cardiovascular, during the trial. J. Am. Heart Assoc. 2012, 1, e003640. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.S.; Lay, S.; Yu, H.N.; Shen, S.R. Dietary Guidelines for Chinese Residents (2016): Comments and comparisons. J. Zhejiang Univ. Sci. B 2016, 17, 649–656. [Google Scholar] [CrossRef] [PubMed]
- Naylor, L.H.; George, K.; O’Driscoll, G.; Green, D.J. The athlete’s heart: A contemporary appraisal of the ‘Morganroth hypothesis’. Sports Med.e 2008, 38, 69–90. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Folsom, A.R.; Shahar, E.; Eckfeldt, J.H. Plasma fatty acid composition as an indicator of habitual dietary fat intake in middle-aged adults. The Atherosclerosis Risk in Communities (ARIC) Study Investigators. Am. J. Clin. Nutr. 1995, 62, 564–571. [Google Scholar] [CrossRef] [PubMed]
- Mensink, R.P.; Zock, P.L.; Kester, A.D.; Katan, M.B. Effects of dietary fatty acids and carbohydrates on the ratio of serum total to HDL cholesterol and on serum lipids and apolipoproteins: A meta-analysis of 60 controlled trials. Am. J. Clin. Nutr. 2003, 77, 1146–1155. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Case | Control | t/z/χ2 | p |
|---|---|---|---|---|
| (n = 173) | (n = 500) | |||
| Age, Median (IQR), y | 65 (15) | 65 (15) | −0.394 | 0.693 |
| sex, n (%) | 0.002 | 0.963 | ||
| Male | 73 (42.2) | 212 (42.4) | ||
| Female | 100 (57.8) | 288 (57.6) | ||
| Waist circumference, Median (IQR), cm | 84 (12) | 80 (10.1) | −4.515 | <0.001 |
| BMI, Mean (SD), kg/m2 | 24.23 ± 3.23 | 23.11 ± 2.93 | −4.210 | <0.001 |
| SBP, Median (IQR), mmHg | 145 (20) | 140 (28) | −1.613 | 0.107 |
| DBP, Median (IQR), mmHg | 86 (14) | 81 (16) | −3.418 | 0.001 |
| TC, Median (IQR), mmol/L | 5.14 (1.31) | 5.05 (1.22) | −0.662 | 0.508 |
| TG, Median (IQR), mmol/L | 1.37 (0.88) | 1.34 (0.92) | −0.004 | 0.997 |
| HDL-C, Median (IQR), mmo/L | 1.22 (0.4) | 1.265 (0.35) | −0.700 | 0.484 |
| LDL-C, Median (IQR), mmol/L | 3.42 (1.06) | 3.025 (1.21) | −4.483 | <0.001 |
| Current smoking, n (%) | 35 (20.2) | 106 (21.2) | 0.073 | 0.787 |
| Current alcohol intake, n (%) | 43 (24.9) | 148 (29.6) | 1.423 | 0.233 |
| Physical activity, n (%) | ||||
| Sedentary/light | 149 (86.1) | 360 (72) | 13.918 | <0.001 |
| Moderate/heavy | 24 (13.9) | 140 (28) | ||
| Fried food intake, n (%) | ||||
| Never | 57 (33.1) | 235 (47.1) | 10.134 | 0.001 |
| Regular | 115 (66.9) | 264 (52.9) | ||
| Dessert intake, n (%) | ||||
| Never | 41 (23.7) | 182 (36.5) | 9.453 | 0.002 |
| Regular | 132 (76.3) | 317 (63.5) | ||
| rs4149339 | ||||
| CC | 24 (13.90) | 37 (7.40) | 6.658 | 0.036 |
| CT | 67 (38.70) | 216 (43.20) | ||
| TT | 82 (47.40) | 247 (49.40) | ||
| rs4743763 | ||||
| AA | 4 (2.3) | 19 (3.8) | 4.425 | 0.109 |
| AT | 47 (27.2) | 172 (34.4) | ||
| TT | 122 (70.5) | 309 (61.8) | ||
| rs2472386 | ||||
| CC | 5 (2.9) | 20 (4) | 2.23 | 0.328 |
| CT | 51 (29.5) | 173 (34.6) | ||
| TT | 117 (67.3) | 307 (61.4) |
| Lifestyles | Non-Risk Allele Carriers (CT + TT) | Risk Allele Carriers (CC) | OR (95% CI) for CC Within Strata of Lifestyles | RERI (95% CI) | p | ||
|---|---|---|---|---|---|---|---|
| Case/Control (n) | OR (95% CI) | Case/Control (n) | OR (95% CI) | ||||
| physical activity | |||||||
| Moderately/heavy physical activity | 20/134 | 4/6 | |||||
| 1 | 3.83 (0.97–15.06) | 3.83 (0.97–15.06) | |||||
| p = 0.055 | p = 0.055 | ||||||
| Sedentary/light physical activity | 129/329 | 20/31 | −1.17 (−6.78–4.42) | 0.699 | |||
| 2.45 (1.46–4.13) | 4.10 (1.94–8.67) | 1.71 (0.93–3.16) | |||||
| p= 0.001 | p< 0.001 | p = 0.0860 | |||||
| OR (95% CI) for Sedentary/light physical activity intensity within strata of genotype | 2.45 (1.46–4.13) | 1.16 (0.22–6.10) | |||||
| p= 0.001 | p = 0.865 | ||||||
| fried food intake | |||||||
| No fried food intake | 50/224 | 7/11 | |||||
| 1 | 2.58 (0.94–7.09) | 2.58 (0.94–7.09) | |||||
| p = 0.067 | p = 0.067 | ||||||
| Regular fried food intake | 98/238 | 17/26 | −0.44 (−3.61–2.73) | 0.780 | |||
| 1.88 (1.26–2.79) | 2.98 (1.47–6.02) | 1.62 (0.83–3.18) | |||||
| p= 0.003 | p= 0.002 | p = 0.161 | |||||
| OR (95% CI) for regular fried food intake within strata of genotype | 1.88 (1.26–2.79) | 1.22(0.35–4.20) | |||||
| p= 0.003 | p = 0.753 | ||||||
| Dessert intake | |||||||
| No dessert intake | 33/74 | 8/8 | |||||
| 1 | 5.26 (1.81–15.25) | 5.26 (1.81–15.25) | |||||
| p= 0.002 | p= 0.002 | ||||||
| Regular dessert intake | 116/288 | 16/29 | −3.51(−9.35–2.34) | 0.240 | |||
| 2.29 (1.47–3.56) | 3.04 (1.46–6.34) | 1.35 (0.69–2.63) | |||||
| p< 0.001 | p= 0.003 | p = 0.380 | |||||
| OR (95% CI) for regular dessert food | 2.29 (1.47–3.56) | 0.51 (0.14–1.79) | |||||
| intake within strata of genotype | p< 0.001 | p = 0.290 | |||||
| Lifestyles | Non-Risk Allele Carriers (AT + AA) | Risk Allele Carriers (TT) | OR (95% CI) for TT within Strata of Lifestyles | RERI (95% CI) | p | ||
|---|---|---|---|---|---|---|---|
| Case/Control (n) | OR (95%CI) | Case/Control (n) | OR (95%CI) | ||||
| Physical activity | |||||||
| Moderately/heavy physical activity | 7/61 | 17/79 | |||||
| 1 | 1.96 (0.76–5.08) | 1.96 (0.76–5.08) | |||||
| p = 0.167 | p = 0.167 | ||||||
| Sedentary/light physical activity | 44/130 | 105/230 | 0.12 (−6.21–6.46) | 0.969 | |||
| 2.80 (1.18–6.64) | 3.88 (1.70–8.86) | 1.38 (0.91–2.11) | |||||
| p= 0.020 | p= 0.001 | p = 0.133 | |||||
| OR (95% CI) for Sedentary/light physical activity intensity within strata of genotype | 2.80 (1.18–6.64) | 2.07 (1.14–3.74) | |||||
| p= 0.020 | p= 0.016 | ||||||
| fried food intake | |||||||
| No fried food intake | 13/94 | 44/141 | |||||
| 1 | 2.38 (1.20–4.74) | 2.38 (1.20–4.74) | |||||
| p= 0.013 | p= 0.013 | ||||||
| Regular fried food intake | 38/97 | 77/167 | −0.80 (−2.81–1.20) | 0.432 | |||
| 2.92 (1.44–5.91) | 3.50 (1.82–6.73) | 1.19 (0.74–1.91) | |||||
| p= 0.003 | p< 0.001 | p = 0.477 | |||||
| OR (95% CI) for regular fried food intake within strata of genotype | 2.92 (1.44–5.91) | 1.42 (0.91–2.24) | |||||
| p= 0.003 | p = 0.126 | ||||||
| Dessert intake | |||||||
| No dessert intake | 14/80 | 27/102 | |||||
| 1 | 1.59 (0.77–3.27) | 1.59 (0.77–3.27) | |||||
| p = 0.210 | p = 0.210 | ||||||
| Regular dessert intake | 37/111 | 95/206 | 0.25 (−1.09–1.59) | 0.711 | |||
| 2.07 (1.04–4.16) | 2.92 (1.55–5.50) | 1.41 (0.89–2.22) | |||||
| p= 0.039 | p= 0.001 | p = 0.140 | |||||
| OR (95% CI) for regular dessert | 2.07 (1.04–4.16) | 1.85 (1.11–3.07) | |||||
| intake within strata of genotype | p= 0.039 | p= 0.018 | |||||
| Gene | Non-Risk Allele Carriers (CT + TT) | Risk Allele Carriers (CC) | OR (95% CI) for rs4149339 CC within Strata of rs4743763 Genotype | ||
|---|---|---|---|---|---|
| Case/Control (n) | OR (95%CI) | Case/Control (n) | OR (95%CI) | ||
| Non-risk allele carriers AT + AA | 46/172 | 5/19 | |||
| 1 | 0.83 (0.29–2.38) | 0.83 (0.29–2.38) | |||
| p = 0.725 | p = 0.725 | ||||
| Risk allele carriers TT | 103/291 | 19/18 | |||
| 1.34 (0.90–2.00) | 4.35 (2.07–9.15) | 3.48 (1.71–7.10) | |||
| p = 0.161 | p< 0.001 | p= 0.001 | |||
| OR (95% CI) for rs4743763 TT within strata of rs4149339 genotype | 1.34 (0.90–2.00) | 4.66 (1.29–16.79) | |||
| p = 0.161 | p= 0.019 | ||||
| Haplotypes a | Frequency | Cases n (%) | Controls n (%) | OR (95% CI) | p |
|---|---|---|---|---|---|
| T T T | 0.56 | 188 (54.2) | 563 (56.3) | 1 | |
| C A C | 0.07 | 16 (4.6) | 69 (6.9) | 0.51 (0.23–1.10) | 0.086 |
| C T T | 0.23 | 94 (27.3) | 212 (21.2) | 1.49 (1.07–2.08) | 0.019 |
| T A C | 0.12 | 36 (10.4) | 129 (12.9) | 0.99 (0.62–1.60) | 0.990 |
| T T C | 0.01 | 7 (1.9) | 11 (1.1) | 2.17 (0.81–5.80) | 0.121 |
| rare group b | 0.02 | 6 (1.6) | 16 (1.6) | 0.81 (0.28–2.32) | 0.689 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, T.-Y.; Lei, S.; Huang, L.; Wang, Y.-N.; Wang, X.-N.; Zhou, P.-P.; Xu, X.-J.; Zhang, L.; Xu, L.-W.; Yang, L. Associations of Genetic Variations in ABCA1 and Lifestyle Factors with Coronary Artery Disease in a Southern Chinese Population with Dyslipidemia: A Nested Case-Control Study. Int. J. Environ. Res. Public Health 2019, 16, 786. https://doi.org/10.3390/ijerph16050786
Zhao T-Y, Lei S, Huang L, Wang Y-N, Wang X-N, Zhou P-P, Xu X-J, Zhang L, Xu L-W, Yang L. Associations of Genetic Variations in ABCA1 and Lifestyle Factors with Coronary Artery Disease in a Southern Chinese Population with Dyslipidemia: A Nested Case-Control Study. International Journal of Environmental Research and Public Health. 2019; 16(5):786. https://doi.org/10.3390/ijerph16050786
Chicago/Turabian StyleZhao, Tian-Yu, Song Lei, Liu Huang, Yi-Nan Wang, Xiao-Ni Wang, Ping-Pu Zhou, Xiao-Jun Xu, Long Zhang, Liang-Wen Xu, and Lei Yang. 2019. "Associations of Genetic Variations in ABCA1 and Lifestyle Factors with Coronary Artery Disease in a Southern Chinese Population with Dyslipidemia: A Nested Case-Control Study" International Journal of Environmental Research and Public Health 16, no. 5: 786. https://doi.org/10.3390/ijerph16050786