Critical Appraisal of Qualitative Studies of Muslim Females’ Perceptions of Physical Activity Barriers and Facilitators


{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
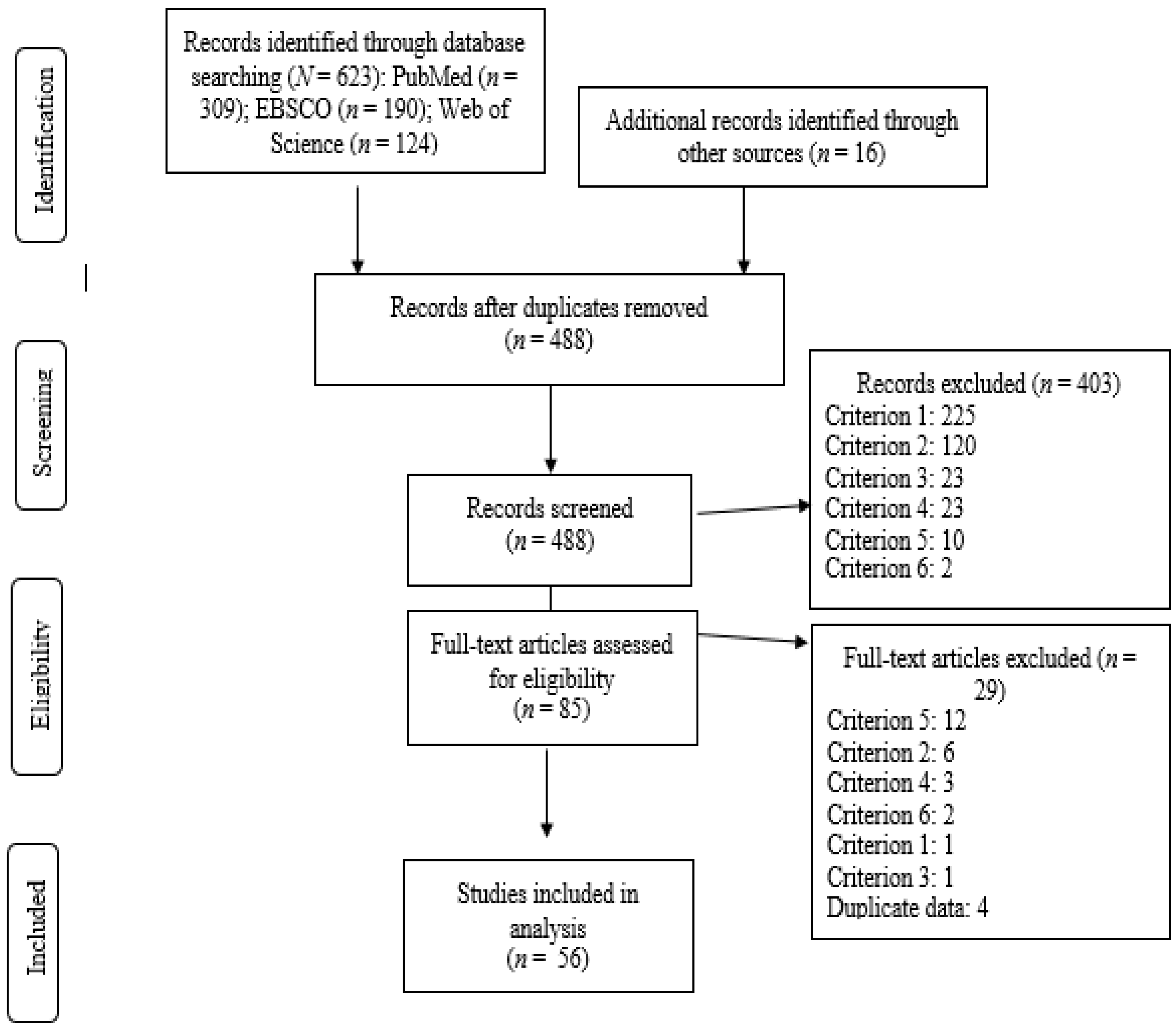
2.1. Data Sources and Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Critical Ratings of Quality of Papers
2.4. Analysis
2.5. Ethical Statements
3. Results
3.1. Study Characteristics
3.2. Descriptive Results
3.3. Crosstabulation Results
4. Discussion
4.1. Descriptive Findings
4.2. Crosstabulation Findings
4.3. Strengths and Limitations
4.4. Implications
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Pew Research Center [PRC]. Table: Muslim Population by Country; PRC: Washington, DC, USA, January 2011; Available online: https://www.pewforum.org/2011/01/27/table-muslim-population-by-country/ (accessed on 5 November 2019).
- Aboul-Enein, B. Health-promoting verses as mentioned in the Holy Quran. J. Relig. Health 2016, 55, 821–829. [Google Scholar] [CrossRef] [PubMed]
- Kizar, O. The place of sports in light of Quran, Hadiths and the opinion of the Muslim scholar in Islam. Univers. J. Educ. Res. 2018, 6, 2663–2668. [Google Scholar] [CrossRef]
- Kahan, D. Adult physical inactivity prevalence in the Muslim world: Analysis of 38 countries. Prev. Med. Rep. 2015, 2, 71–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnes, D.M.; Almasy, N. Refugees’ perceptions of healthy behaviors. J. Immigr. Health 2005, 7, 185–193. [Google Scholar] [CrossRef]
- Kahan, D. Arab-American college students’ physical activity and body composition: Reconciling Middle East-West differences using the socioecological model. Res. Q. Exerc. Sport 2011, 82, 118–128. [Google Scholar] [CrossRef]
- Mohamed, A.A.; Hassan, A.M.; Weis, J.A.; Sia, I.G.; Wieland, M.L. Physical activity among Somali men in Minnesota: Barriers, facilitators, and recommendations. Am. J. Mens Health 2014, 8, 35–44. [Google Scholar] [CrossRef] [Green Version]
- Babakus, W.; Thompson, J.L. Physical activity among South Asian women: A systematic, mixed-methods review. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 150. [Google Scholar] [CrossRef] [Green Version]
- Bhatnagar, P.; Shaw, A.; Foster, C. Generational differences in the physical activity of UK South Asians: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 96. [Google Scholar] [CrossRef] [Green Version]
- Caperchione, C.M.; Kolt, G.S.; Mummery, W.K. Physical activity in culturally and linguistically diverse migrant groups to Western society. Sports Med. 2009, 39, 167–177. [Google Scholar] [CrossRef]
- De Knop, P.; Theeboom, M.; Wittock, H.; De Martelaer, K.; Wittock, H. Implications of Islam on Muslim girls’ sport participation in Western Europe. Literature review and policy recommendations for sport promotion. Sport Educ. Soc. 1996, 1, 147–164. [Google Scholar] [CrossRef]
- Horne, M.; Tierney, S. What are the barriers and facilitators to exercise and physical activity uptake and adherence among South Asian older adults: A systematic review of qualitative studies. Prev. Med. 2012, 55, 276–284. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.R.D. Perceptions of barriers to healthy physical activity among Asian communities. Sport Educ. Soc. 2000, 5, 51–70. [Google Scholar] [CrossRef]
- Koshoedo, S.A.; Paul-Ebhohimhen, V.A.; Jepson, R.G.; Watson, M.C. Understanding the complex interplay of barriers to physical activity amongst black and minority ethnic groups in the United Kingdom: A qualitative synthesis using meta-ethnography. BMC Public Health 2015, 15, 643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Langøien, L.J.; Terragni, L.; Rugseth, G.; Nicolaou, M.; Holdsworth, M.; Stronks, K.; Lien, N.; Roos, G.; DEDIPAC Consortium. Systematic mapping review of the factors influencing physical activity and sedentary behavior in ethnic minority groups in Europe: A DEDIPAC study. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 99. [Google Scholar]
- O’Driscoll, T.; Banting, L.K.; Borkoles, E.; Eime, R.; Polman, R. A systematic literature review of sport and physical activity participation in culturally and linguistically diverse (CALD) migrant populations. J. Immigr. Minor. Health 2014, 16, 515–530. [Google Scholar] [CrossRef] [Green Version]
- Abdulwasi, M.; Bhardwaj, M.; Nakamura, Y.; Zawi, M.; Price, J.; Harvey, P.; Banerjee, A.T. An ecological exploration of facilitators to participation in a mosque-based physical activity program for South Asian Muslim women. J. Phys. Act. Health 2018, 15, 671–678. [Google Scholar] [CrossRef]
- Banerjee, A.T.; Landry, M.; Zawi, M.; Childrehose, D.; Stephens, N.; Shafique, A.; Price, J. A pilot examination of a mosque-based physical activity intervention for South Asian Muslim women in Ontario, Canada. J. Immigr. Minor. Health 2017, 19, 349–357. [Google Scholar] [CrossRef]
- Kahan, D.; Amini, H.; Osman, M. Formative evaluation of a pilot study of a university exercise class for female Muslims. J. Phys. Act. Res. 2018, 3, 35–40. [Google Scholar] [CrossRef] [Green Version]
- Pitney, W.A.; Parker, J. Qualitative Research in Physical Activity and the Health Professions; Human Kinetics: Champaign, IL, USA, 2009. [Google Scholar]
- Calderón, J.L.; Baker, R.S.; Wolf, K.E. Focus groups: A qualitative method complementing quantitative research for studying culturally diverse groups. Educ. Health 2000, 13, 91–95. [Google Scholar]
- Akkuş, B.; Postmes, T.; Stroebe, K. Community collectivism: A social dynamic approach to conceptualizing culture. PLoS ONE 2017, 12. [Google Scholar] [CrossRef]
- Vandello, J. Do we need a psychology of women in the Islamic world? Sex Roles 2016, 75, 623–629. [Google Scholar] [CrossRef] [Green Version]
- Kitto, S.C.; Chesters, J.; Grbich, C. Quality in qualitative research: Criteria for authors and assessors in the submission and assessment of qualitative research articles for Medical Journal of Australia. Med. J. Aust. 2008, 188, 243–246. [Google Scholar] [CrossRef] [PubMed]
- Mays, N.; Pope, C. Qualitative research in health care: Assessing quality in qualitative research. Br. Med. J. 2000, 320, 50–52. [Google Scholar] [CrossRef] [PubMed]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [Green Version]
- Hannes, K.; Heyvaert, M.; Slegers, K.; Vandenbrande, S.; Van Nuland, M. Exploring the potential for a consolidated standard for reporting guidelines for qualitative research: An argument Delphi approach. Int. J. Qual. Stud. 2015, 14, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Human Development Report 2015: Work for Human Development. Available online: http://hdr.undp.org/sites/default/files/2015_human_development_report.pdf (accessed on 5 November 2019).
- The Global Changing Religious Landscape. Available online: https://www.pewforum.org/2017/04/05/the-changing-global-religious-landscape/ (accessed on 5 November 2019).
- Shuval, K.; Harker, K.; Roudsari, B.; Groce, N.E.; Mills, B.; Siddiqi, Z.; Shachak, A. Is qualitative research a second class science? A quantitative longitudinal examination of qualitative research in medical journals. PLoS ONE 2011, 6, e16937. [Google Scholar] [CrossRef]
- Galgliardi, A.R.; Dobrow, M.J. Paucity of qualitative research in general medical and health services and policy research journals: Analysis of publication rates. BMC Health Serv. Res. 2011, 11, 268. [Google Scholar]
- McKibbon, K.A.; Gadd, C.S. A quantitative analysis of qualitative studies in clinical journals for the 2000 publishing year. BMC Med. Inform. Decis. Mak. 2004, 4, 11. [Google Scholar] [CrossRef] [Green Version]
- SCImago. SJR—SCImago Journal & Country Rank [Portal]. Available online: http://www.scimagojr.com (accessed on 5 November 2019).
- Guerrero-Botea, V.P.; Moya-Anegón, F. A further step forward in measuring journals’ scientific prestige: The SJR2 indicator. J. Informetr. 2012, 6, 674–688. [Google Scholar] [CrossRef] [Green Version]
- Agergaard, S. Religious culture as a barrier? A counter-narrative of Danish Muslim girls’ participation in sports. Qual. Res. Sport Exerc. Health 2015, 8, 213–224. [Google Scholar] [CrossRef]
- Ahmad, A. British football: Where are the Muslim female footballers? Exploring the connection between gender, ethnicity and Islam. Soccer Soc. 2011, 12, 443–456. [Google Scholar] [CrossRef]
- Alamri, A.A. How Australian female Muslim students interpret challenges in high school sports. J. Muslim Minor. Aff. 2015, 35, 215–229. [Google Scholar] [CrossRef]
- Arar, K.; Rigbi, A. ‘To participate or not to participate?’—Status and perception of physical education among Muslim Arab-Israeli secondary school pupils. Sport Educ. Soc. 2009, 12, 183–202. [Google Scholar] [CrossRef]
- Benn, T. Muslim women and physical education in initial teacher training. Sport Educ. Soc. 1996, 1, 5–21. [Google Scholar] [CrossRef]
- Benn, T.; Dagkas, S.; Jawad, H. Embodied faith, Islam, religious freedom and educational practices in physical education. Sport Educ. Soc. 2011, 16, 17–34. [Google Scholar] [CrossRef]
- Brophy, S.; Crowley, A.; Mistry, R.; Hill, R.; Chowdhury, S.; Thomas, N.E.; Rapport, F. Recommendations to improve physical activity among teenagers—A qualitative study with ethnic minority and European teenagers. BMC Public Health 2011, 11, 412. [Google Scholar] [CrossRef] [Green Version]
- Caperchione, C.M.; Kolt, G.S.; Tennent, R.; Mummery, W.K. Physical activity behaviours of culturally and linguistically diverse (CALD) women living in Australia: A qualitative study of socio-cultural influences. BMC Public Health 2011, 11, 26. [Google Scholar] [CrossRef] [Green Version]
- Carroll, R.; Ali, N.; Azam, N. Promoting physical activity in South Asian Muslim women through “exercise on prescription”. Health Technol. Assess. 2002, 6, 1–101. [Google Scholar] [CrossRef] [Green Version]
- Carroll, B.; Hollinshead, G. Ethnicity and conflict in physical education. Br. Educ. Res. J. 1993, 19, 59–76. [Google Scholar] [CrossRef]
- Cross-Bardell, L.; George, T.; Bhoday, M.; Tuomainen, H.; Qureshi, N.; Kai, J. Perspectives on enhancing physical activity and diet for health promotion among at-risk urban UK South Asian communities: A qualitative study. BMJ Open 2015, 5. [Google Scholar] [CrossRef] [Green Version]
- Curry, W.B.; Duda, J.L.; Thompson, J.L. Perceived and Objectively Measured Physical Activity and Sedentary Time among South Asian Women in the UK. Int. J. Environ. Res. Public Health 2015, 12, 3152–3173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dagkas, S.; Benn, T.; Jawad, H. Multiple voices: Improving participation of Muslim girls in physical education and school sport. Sport Educ. Soc. 2011, 16, 223–239. [Google Scholar] [CrossRef]
- Dagkas, S.; Hunter, L. ‘Racialised’ pedagogic practice influencing young Muslims’ physical culture. Phys. Educ. Sport Pedagogy 2015, 20, 547–558. [Google Scholar] [CrossRef]
- Dave, S.D.; Craft, L.L.; Mehta, P.; Naval, S.; Kumar, S.; Kandula, N.R. Life stage influences on U.S. South Asian women’s physical activity. Am. J. Health Promot 2015, 29, 100–108. [Google Scholar] [CrossRef]
- De Knop, P.; Theeboom, M.; Van Engeland, E.; Van Puymbroeck, L.; De Martelaer, K.; Wittock, H. Sport and ethnic minority youth. J. Comp. Phys. Educ. Sport 1995, 17, 12–23. [Google Scholar]
- Devlin, J.T.; Dhalac, D.; Suldan, A.A.; Jacobs, A.; Guled, K.; Bankole, K.A. Determinants of physical activity among Somali women living in Maine. J Immigr Minor. Health 2012, 14, 300–306. [Google Scholar] [CrossRef]
- Eyre, E.L.; Duncan, M.J.; Birch, S.L.; Cox, V. Environmental and school influences on physical activity in South Asian children from low socio-economic backgrounds: A qualitative study. J. Child Health Care 2015, 19, 345–358. [Google Scholar] [CrossRef]
- Guerin, P.B.; Diiriye, R.O.; Corrigan, C.; Guerin, B. Physical activity programs for refugee Somali women: Working out in a new country. Women Health 2003, 38, 83–99. [Google Scholar] [CrossRef]
- Hamzeh, M.; Oliver, K.L. “Because I am Muslim, I cannot wear a swimsit:” Muslim girls negotiate participation opportunities for physical activity. Res. Q. Exerc. Sport 2012, 83, 330–339. [Google Scholar]
- Horne, M.; Skelton, D.A.; Speed, S.; Todd, C. Attitudes and beliefs to the uptake and maintenance of physical activity among community-dwelling South Asians aged 60–70 years: A qualitative study. Public Health 2012, 126, 417–423. [Google Scholar] [CrossRef]
- Horne, M.; Skelton, D.A.; Speed, S.; Todd, C. Perceived barriers to initiating and maintaining physical activity among South Asian and White British adults in their 60s living in the United Kingdom. Ethn. Health 2013, 18, 626–645. [Google Scholar] [CrossRef] [PubMed]
- Jepson, R.; Harris, F.M.; Bowes, A.; Robertson, R.; Avan, G.; Sheikh, A. Physical activity in South Asians: An in-depth qualitative study to explore motivators and facilitators. PLoS ONE 2012, 7, e45333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiwani, N.; Rail, G. Islam, hijab and young Shia Muslim Canadian women’s discursive constructions of physical activity. Sociol. Sport, J. 2010, 27, 250–267. [Google Scholar] [CrossRef]
- Kay, T. Daughters of Islam: Family influences on Muslim young women’s participation in sport. Int. Rev. Sociol. Sport 2006, 41, 357–373. [Google Scholar] [CrossRef]
- Khanam, S.; Costarelli, V. Attitudes towards health and exercise of overweight women. J. R. Soc. Promot. Health 2008, 128, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Knez, K.; Macdonald, D.; Abbott, R. Challenging stereotypes: Muslim girls talk about physical activity, physical education and sport. Asia-Pacific J. Health Sport Phys. Educ. 2012, 3, 109–122. [Google Scholar] [CrossRef]
- Lindsay, K.; McEwen, S.; Knight, J. Islamic principles and physical education. Unicorn 1987, 13, 75–78. [Google Scholar]
- Macdonald, D.; Abbott, R.; Knez, K.; Nelson, A. Taking exercise: Cultural diversity and physically active lifestyles. Sport Educ. Soc. 2009, 14, 1–19. [Google Scholar] [CrossRef]
- Marinescu, L.G.; Sharify, D.; Krieger, J.; Saelens, B.E.; Calleja, J.; Aden, A. Be active together: Supporting physical activity in public housing communities through women-only programs. Prog. Community Health Partnersh. 2013, 7, 57–66. [Google Scholar] [CrossRef]
- McGee, J.E.; Hardman, K. Muslim schoolgirls’ identity and participation in school-based physical education in England. SportLogia 2012, 8, 49–71. [Google Scholar] [CrossRef]
- Miles, C.; Benn, T. A case study on the experiences of university-based Muslim women in physical activity during their studies at one UK higher education institution. Sport Educ. Soc. 2016, 21, 723–740. [Google Scholar] [CrossRef]
- Murray, K.; Sheik Mohamed, A.; Dawson, D.B.; Syme, M.; Abdi, S.; Barnack-Tavlaris, J. Somali perspectives on physical activity: Photovoice to address barriers and resources in San Diego. Prog. Community Health Partnersh. 2015, 9, 83–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakamura, Y. Beyond the hijab: Female Muslims and physical activity. Women Sport Phys. Act. J. 2002, 11, 21–48. [Google Scholar] [CrossRef]
- Palmer, C. Soccer and the politics of identity for young Muslim refugee women in South Australia. Soccer Soc. 2009, 10, 27–38. [Google Scholar] [CrossRef] [Green Version]
- Persson, G.; Mahmud, A.J.; Hansson, E.E.; Strandberg, E.L. Somali women’s view of physical activity—A focus group study. BMC Womens Health 2014, 14, 129. [Google Scholar] [CrossRef] [Green Version]
- Riley, L.; Mili, S.; Trinh-Shevrin, C.; Islam, N. Using qualitative methods to understand physical activity and weight management among Bangladeshis in New York City, 2013. Prev. Chronic Dis. 2016, 13, E87. [Google Scholar] [CrossRef] [Green Version]
- Rothe, E.; Holt, C.; Kuhn, C.; McAteer, T.; Askari, I.; O’Meara, M.; Sharif, A.; Dexter, W. Barriers to outdoor physical activity in wintertime among Somali youth. J. Immigr. Minor. Health 2010, 12, 726–736. [Google Scholar] [CrossRef]
- Samie, S.F. Hetero-sexy self/body work and basketball: The invisible sporting women of British Pakistani Muslim heritage. South Asian Pop. Cult. 2013, 11, 257–270. [Google Scholar] [CrossRef]
- Shuval, K.; Weissblueth, E.; Araida, A.; Brezis, M.; Faridi, Z.; Ali, A.; Katz, D.L. The role of culture, environment, and religion in the promotion of physical activity among Arab Israelis. Prev. Chronic Dis. 2008, 5, A88. [Google Scholar]
- Södergren, M.; Hylander, I.; Törnkvist, L.; Sundquist, J.; Sundquist, K. Arranging appropriate activities: Immigrant women’s ideas of enabling exercises. Womens Health Issues 2008, 18, 413–422. [Google Scholar] [CrossRef]
- Strandbu, A. Identity, embodied culture and physical exercise: Stories from Muslim girls in Oslo with immigrant backgrounds. Young 2005, 13, 27–45. [Google Scholar] [CrossRef]
- Stride, A. Centralising space: The physical education and physical activity experiences of South Asian, Muslim girls. Sport Educ. Soc. 2016, 21, 677–697. [Google Scholar] [CrossRef]
- Stride, A. Let US tell YOU! South Asian, Muslim girls tell tales about physical education. Phys. Educ. Sport Pedagogy 2014, 19, 398–417. [Google Scholar] [CrossRef]
- Sulaiman, N.D.; Furler, J.S.; Hadj, E.J.; Corbett, H.M.; Young, D.Y. Stress, culture and ‘home’: Social context in Turkish and Arabic-speaking Australians’ views of diabetes prevention. Health Promot. J. Austr. 2007, 18, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Tami, S.H.; Reed, D.B.; Boylan, M.; Zvonkovic, A. Assessment of the effect of acculturation on dietary and physical activity behaviors of Arab mothers in Lubbock, Texas. Ethn. Dis. 2012, 22, 192–197. [Google Scholar] [PubMed]
- Taylor, T.; Doherty, A. Adolescent sport, recreation and physical education: Experiences of recent arrivals to Canada. Sport Educ. Soc. 2005, 10, 211–238. [Google Scholar] [CrossRef]
- Taylor, T.; Toohey, K. Behind the veil: Exploring the recreation needs of Muslim women. Leisure 2001, 26, 85–105. [Google Scholar] [CrossRef]
- Walseth, K. Young Muslim women and sport: The impact of identity work. Leisure Studies 2006, 25, 75–94. [Google Scholar] [CrossRef]
- Walseth, K. Sport and belonging. Int. Rev. Sociol. Sport 2006, 41, 447–464. [Google Scholar] [CrossRef]
- Walseth, K. Muslim girls’ experiences in physical education in Norway: What role does religiosity play? Sport Educ. Soc. 2015, 20, 304–322. [Google Scholar] [CrossRef] [Green Version]
- Walseth, K.; Strandbu, A. Young Norwegian-Pakistani women and sport: How does culture and religiosity matter? European Phys. Educ. Rev. 2014, 20, 489–507. [Google Scholar] [CrossRef]
- Wieland, M.L.; Weis, J.A.; Palmer, T.; Goodson, M.; Loth, S.; Omer, F.; Abbenyi, A.; Krucker, K.; Edens, K.; Sia, I.G. Physical activity and nutrition among immigrant women: A community-based participatory research approach. Womens Health Issues 2012, 22, e225–e232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, A.; Renzaho, A. Intergenerational differences in acculturation experiences, food beliefs and perceived health risks among refugees from the Horn of Africa in Melbourne, Australia. Public Health Nutr. 2015, 18, 176–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- With-Nielsen, N.; Pfister, G. Gender constructions and negotiations in physical education: Case studies. Sport Educ. Soc. 2011, 16, 645–664. [Google Scholar] [CrossRef]
- Green, J.; Thorogood, N. Qualitative Methods for Health Research, 4th ed.; Sage Publications: London, UK, 2018. [Google Scholar]
- Buus, N.; Agdal, R. Can the use of reporting guidelines in peer-review damage the quality and contribution of qualitative health care research? Int. J. Nurs. Stud. 2013, 50, 1289–1291. [Google Scholar] [CrossRef]
- Peditto, K. Reporting qualitative research: Standards, challenges, and implications for health design. HERD 2018, 11, 16–19. [Google Scholar] [CrossRef]
- Richardson, J.C.; Liddle, J. Where does good quality qualitative health care research get published? Prim. Health Care Res. Dev. 2017, 18, 515–521. [Google Scholar] [CrossRef] [Green Version]
- McKosker, L.K.; Sendall, M.C. Undergraduate public health students and perceptions of qualitative research: A trajectory of understanding from Airy Fairy to valuable tool. Teach. Learn. 2015, 8, 19–36. [Google Scholar] [CrossRef]
- Slade, S.C.; Patel, S.; Underwood, M.; Keating, J.L. Rigorous qualitative research in sports, exercise and musculoskeletal medicine journals is important and relevant. Br. J. Sports Med. 2018, 52, 1409–1410. [Google Scholar] [CrossRef]
- Thomas, J.R.; Nelson, J.K.; Silverman, S.J. Research Methods in Physical Activity, 6th ed.; Human Kinetics: Champaign, IL, USA, 2011. [Google Scholar]
- Rai, K.K.; Dogra, S.A.; Barber, S.; Adab, P.; Summerbell, C. A scoping review and systematic mapping of health promotion interventions associated with obesity in Islamic religious settings in the UK. Obes. Rev. 2019, 20, 1231–1261. [Google Scholar] [CrossRef] [Green Version]



© 2019 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kahan, D. Critical Appraisal of Qualitative Studies of Muslim Females’ Perceptions of Physical Activity Barriers and Facilitators. Int. J. Environ. Res. Public Health 2019, 16, 5040. https://doi.org/10.3390/ijerph16245040
Kahan D. Critical Appraisal of Qualitative Studies of Muslim Females’ Perceptions of Physical Activity Barriers and Facilitators. International Journal of Environmental Research and Public Health. 2019; 16(24):5040. https://doi.org/10.3390/ijerph16245040
Chicago/Turabian StyleKahan, David. 2019. "Critical Appraisal of Qualitative Studies of Muslim Females’ Perceptions of Physical Activity Barriers and Facilitators" International Journal of Environmental Research and Public Health 16, no. 24: 5040. https://doi.org/10.3390/ijerph16245040