Biomechanical and Metabolic Effectiveness of an Industrial Exoskeleton for Overhead Work


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
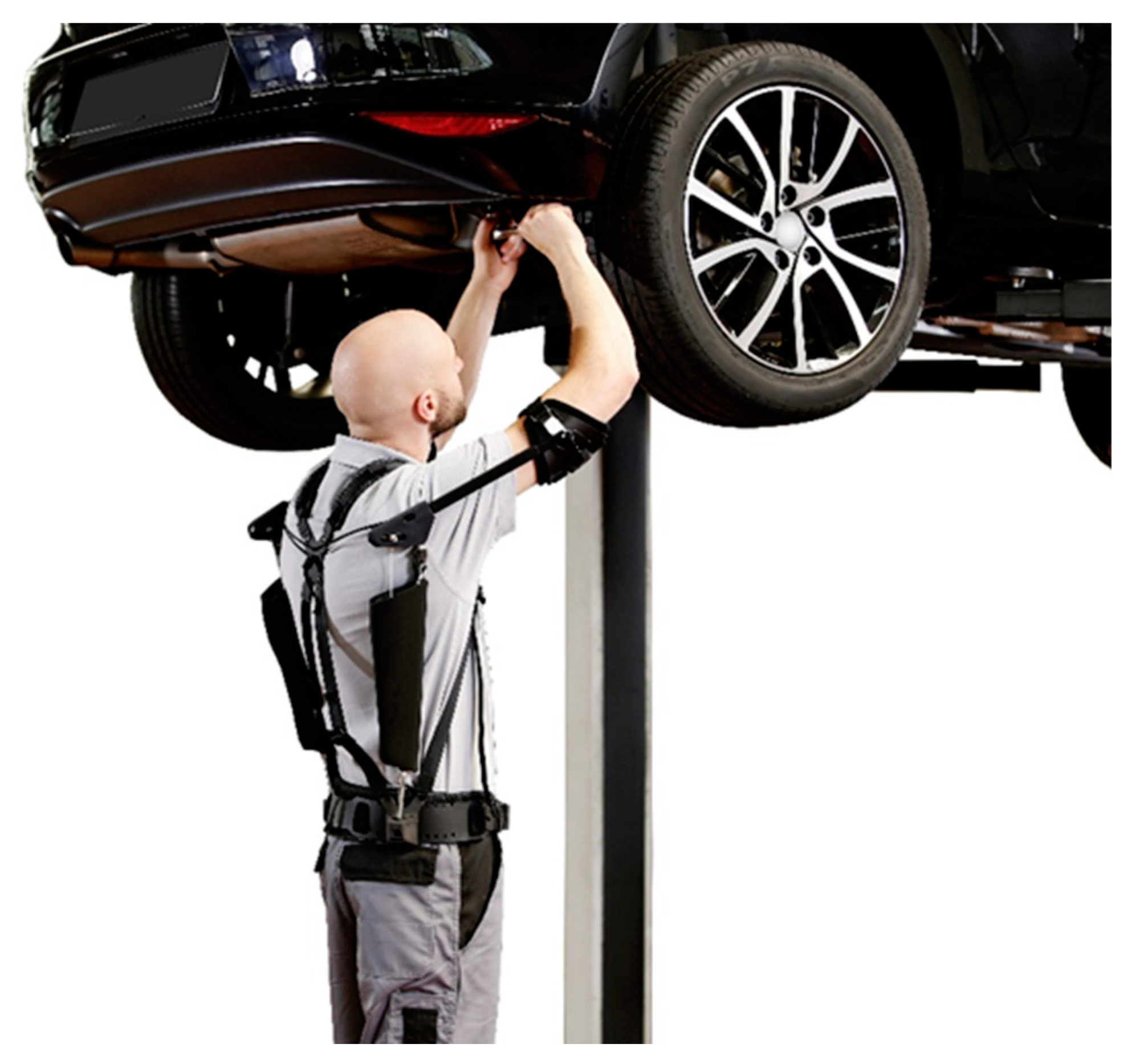
2.1. Exoskeleton
2.2. Participants
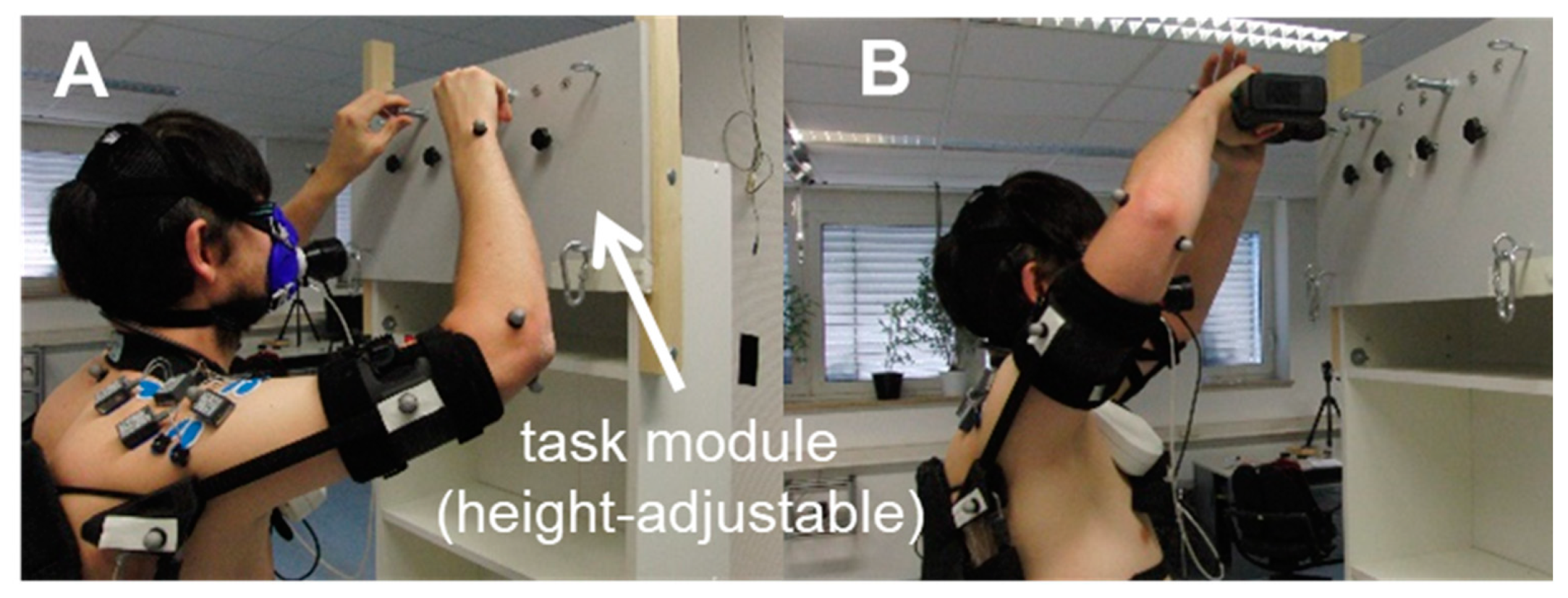
2.3. Simulation of Overhead Work Under Laboratory Conditions
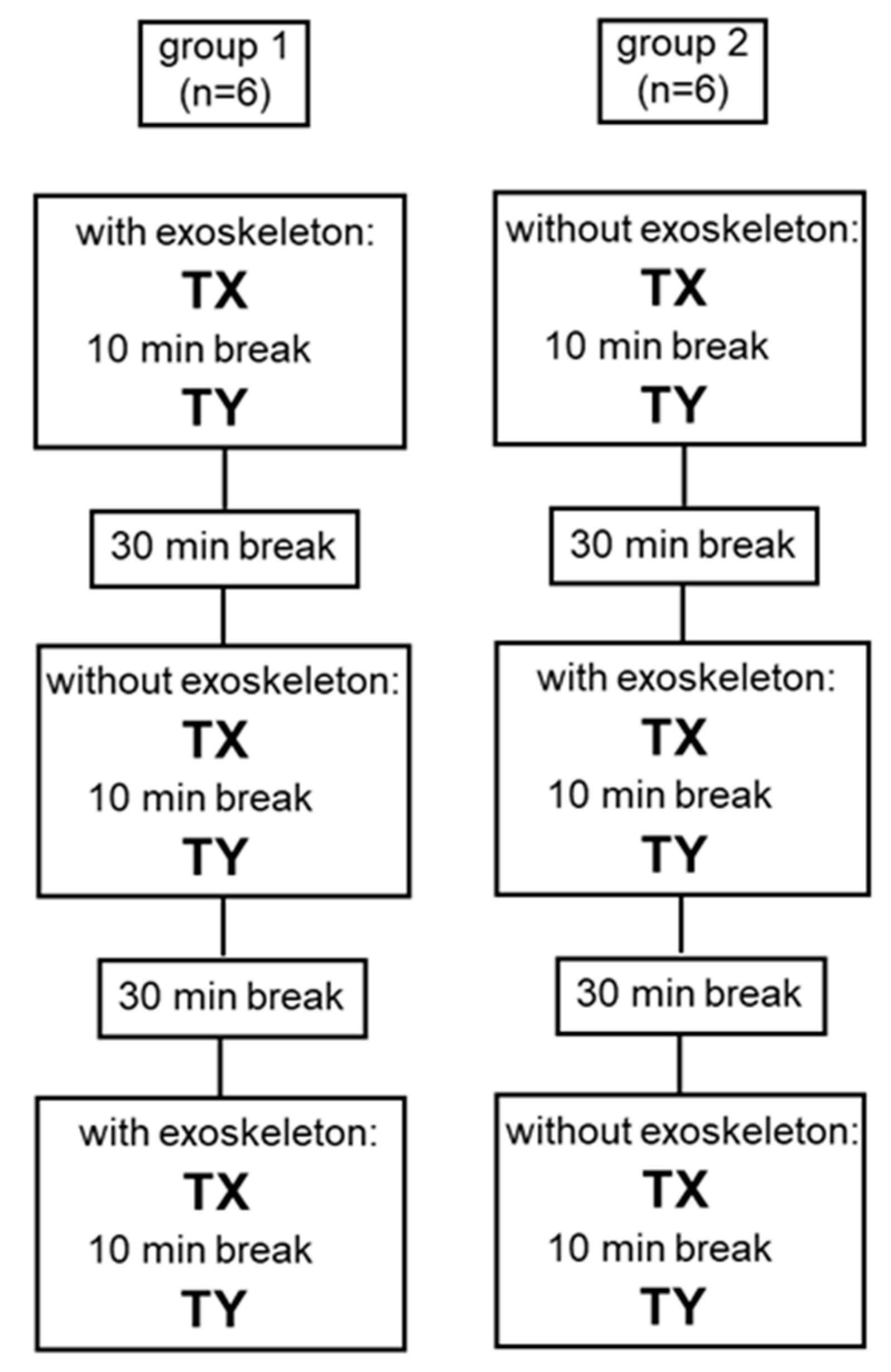
2.4. Test Design
2.5. Measurement Devices
2.5.1. Metabolic Parameters
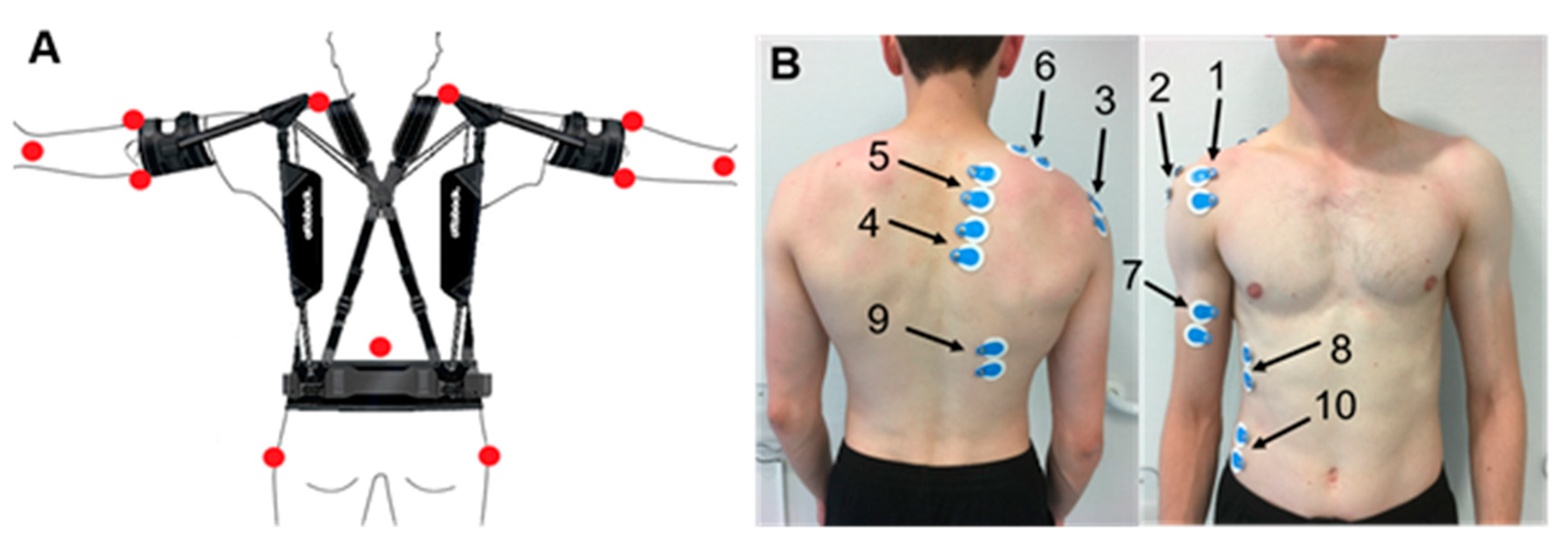
2.5.2. Kinematics
2.5.3. Electromyography
2.6. Data Processing
2.6.1. Metabolic Parameters
2.6.2. Kinematics
2.6.3. Electromyography
2.7. Statistics
3. Results
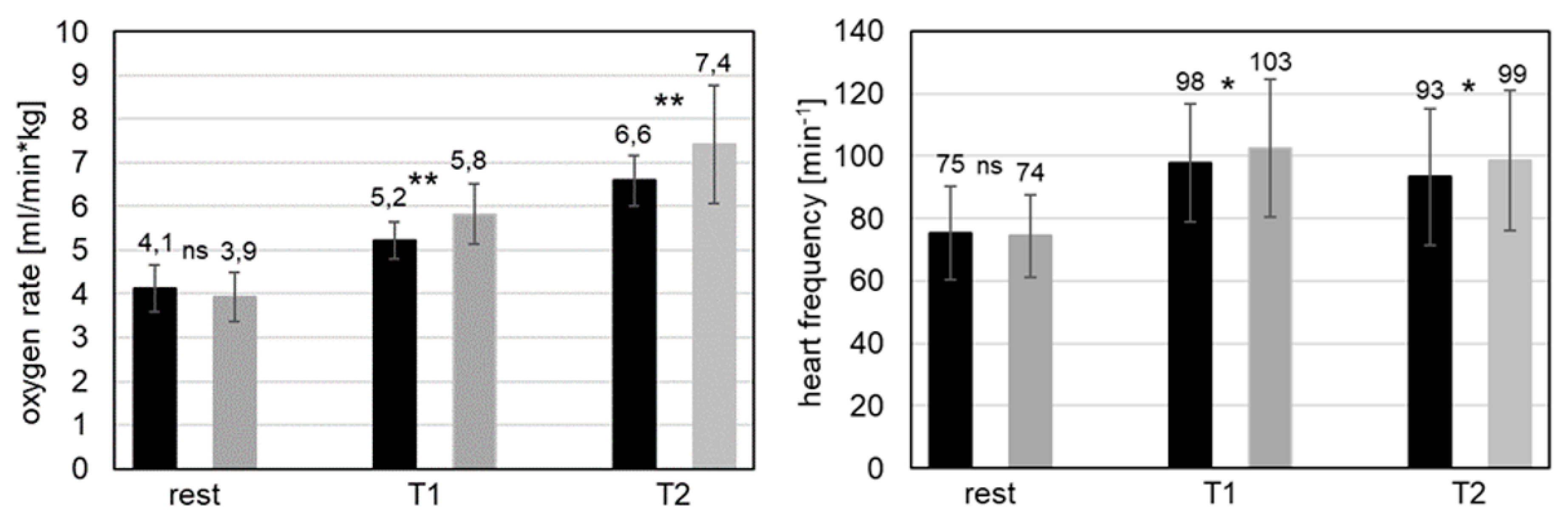
3.1. Metabolic Parameters
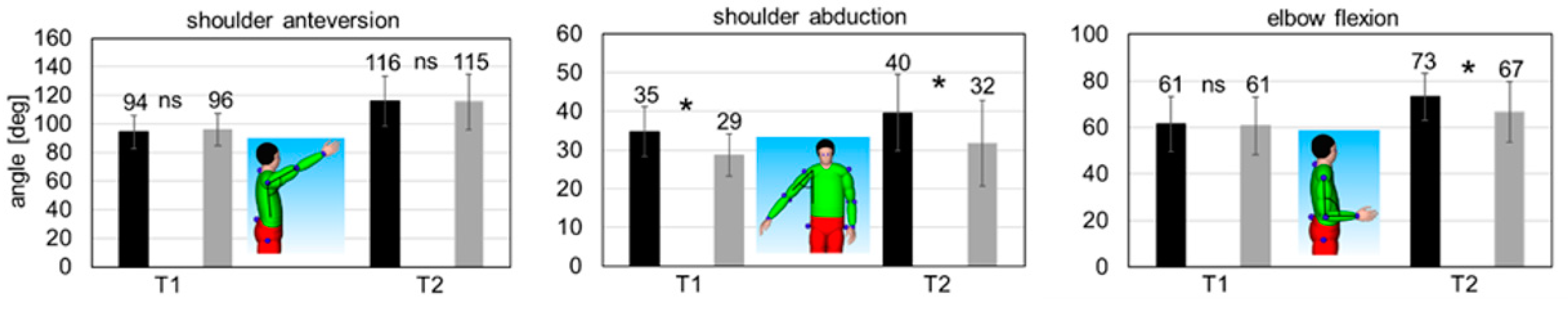
3.2. Kinematics
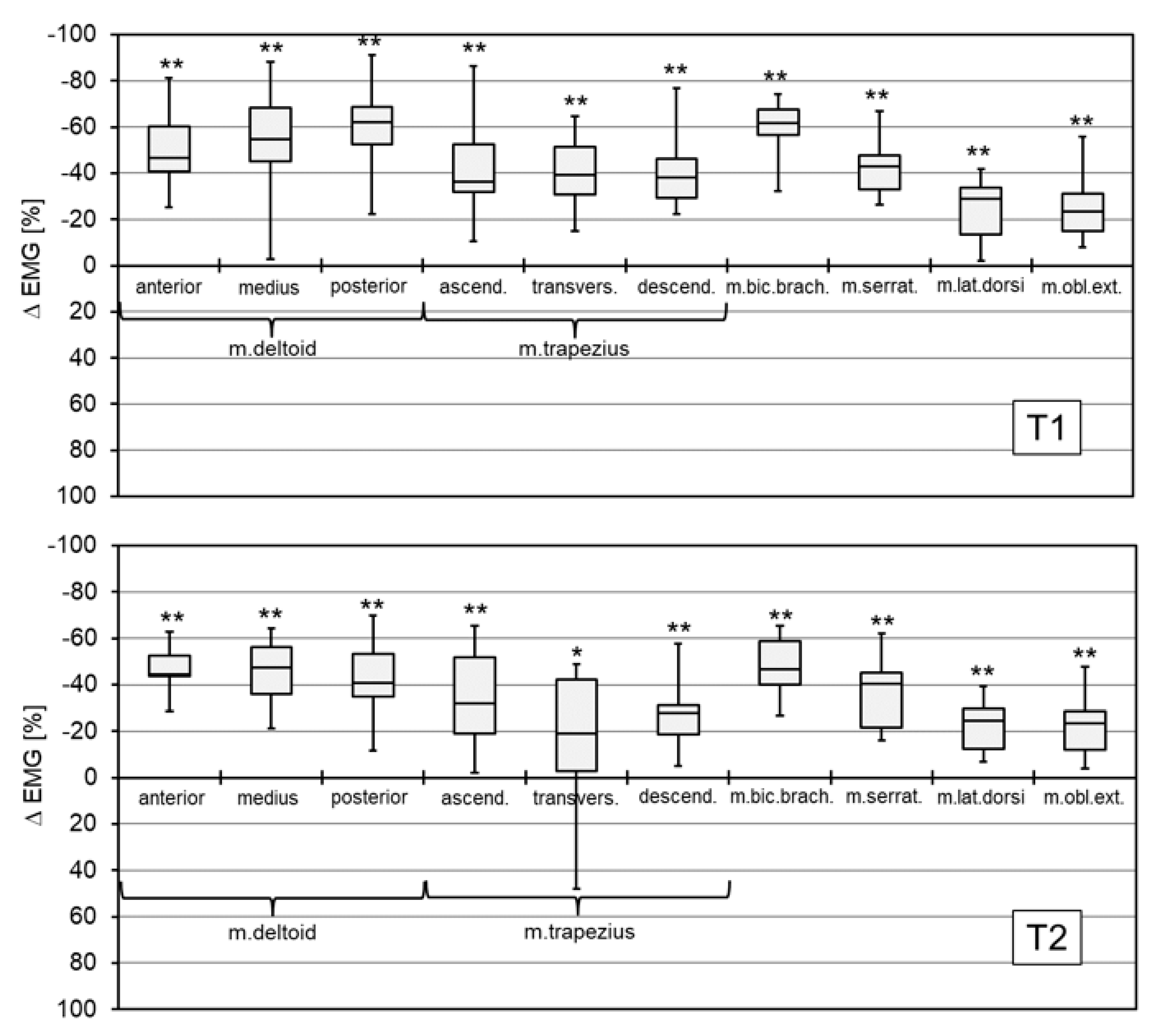
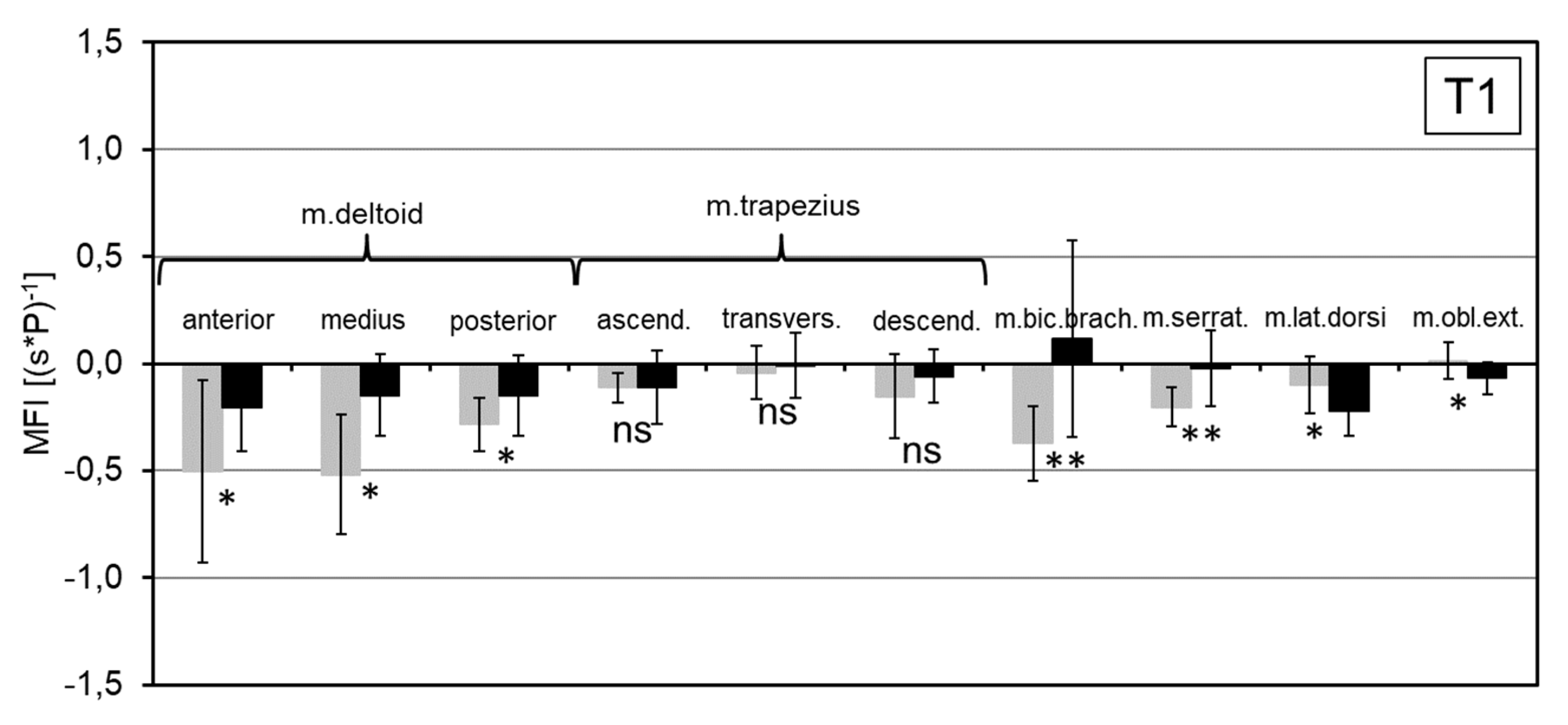
3.3. Electromyography
4. Discussion
4.1. Metabolic Parameters
4.2. Biomechanical Parameters
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Podniece, Z.; van den Heuvel, S.; Blatter, B. Work-Related Musculoskeletal Disorders: Prevention Report; European Agency for Safety and Health at Work: Luxembourg, 2008; ISBN 978-92-9191-162-2. [Google Scholar]
- Frost, P.; Bonde, J.P.E.; Mikkelsen, S.; Andersen, J.H.; Fallentin, N.; Kaergaard, A.; Thomsen, J.F. Risk of shoulder tendinitis in relation to shoulder loads in monotonous repetitive work. Am. J. Ind. Med. 2002, 41, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Grieve, J.; Dickerson, C. Overhead work: Identification of evidence-based exposure guidelines. Occup. Ergon. 2008, 8, 53–66. [Google Scholar]
- Bjelle, A.; Hagberg, M.; Michaelsson, G. Clinical and ergonomic factors in prolonged shoulder pain among industrial workers. Scand. J. Work Environ. Health 1979, 5, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Reinhart, G.; Prasch, M.; Loy, M.; Schur, S. Ergonomics and efficiency with manipulators—Application criterias for manipulation devices in the serial assembly for medium and low weights. wt Werkstattstech. Online 2006, 8, 569–574. [Google Scholar]
- de Looze, M.P.; Bosch, T.; Krause, F.; Stadler, K.S.; O’Sullivan, L.W. Exoskeletons for industrial application and their potential effects on physical work load. Ergonomics 2016, 59, 671–681. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Nussbaum, M.A.; Mokhlespour Esfahani, M.I.; Alemi, M.M.; Alabdulkarim, S.; Rashedi, E. Assessing the influence of a passive, upper extremity exoskeletal vest for tasks requiring arm elevation: Part I—“Expected” effects on discomfort, shoulder muscle activity, and work task performance. Appl. Ergon. 2018, 70, 315–322. [Google Scholar] [CrossRef]
- van Engelhoven, L.; Poon, N.; Kazerooni, H.; Barr, A.; Rempel, D.; Harris-Adamson, C. Evaluation of an adjustable support shoulder exoskeleton on static and dynamic overhead tasks. Proc. Hum. Fac. Ergon. Soc. Annu. Meet. 2018, 62, 804–808. [Google Scholar] [CrossRef]
- Huysamen, K.; Bosch, T.; de Looze, M.; Stadler, K.S.; Graf, E.; O’Sullivan, L.W. Evaluation of a passive exoskeleton for static upper limb activities. Appl. Ergon. 2018, 70, 148–155. [Google Scholar] [CrossRef]
- Gillette, J.C.; Stephenson, M.L. EMG assessment of a shoulder support exoskeleton during on-site job tasks. Proc. Am. Soc. Biomech. Annu. Meet. Boulder CO USA 2017. [Google Scholar]
- Otten, B.M.; Weidner, R.; Argubi-Wollesen, A. Evaluation of a Novel Active Exoskeleton for Tasks at or Above Head Level: IEEE Robotics and Automation Letters. IEEE Robot. Autom. Lett. 2018, 3, 2408–2415. [Google Scholar] [CrossRef]
- Maurice, P.; Čamernik, J.; Gorjan, D.; Schirrmeister, B.; Bornmann, J.; Tagliapietra, L.; Latella, C.; Pucci, D.; Fritzsche, L.; Ivaldi, S.; et al. Objective and Subjective Effects of a Passive Exoskeleton on Overhead Work. Trans. Neural Syst. Rehabil. Eng. 2019. [Google Scholar] [CrossRef] [PubMed]
- Theurel, J.; Desbrosses, K.; Roux, T.; Savescu, A. Physiological consequences of using an upper limb exoskeleton during manual handling tasks. Appl. Ergon. 2018, 67, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Theurel, J.; Desbrosses, K. Occupational Exoskeletons: Overview of their Benefits and Limitations in Preventing Work-related Musculoskeletal Disorders. IISE Trans. Occup. Ergon. Hum. Factors 2019. [Google Scholar] [CrossRef]
- Steinhilber, B.; Seibt, R.; Luger, T. Exoskeletons in occupational settings—Effects and side effects: Einsatz von Exoskeletten im beruflichen Kontext—Wirkung und Nebenwirkung. ASU Arbeitsmed. Sozialmed. Umweltmed. 2018, 53, 662–664. [Google Scholar]
- Kim, S.; Nussbaum, M.A.; Mokhlespour, E.M.I.; Alemi, M.M.; Jia, B.; Rashedi, E. Assessing the influence of a passive, upper extremity exoskeletal vest for tasks requiring arm elevation: Part II-” Unexpected” effects on shoulder motion, balance, and spine loading. Appl. Ergon. 2018, 70, 323. [Google Scholar] [CrossRef]
- Weston, E.B.; Alizadeh, M.; Knapik, G.G.; Wang, X.; Marras, W.S. Biomechanical evaluation of exoskeleton use on loading of the lumbar spine. Appl. Ergon. 2018, 68, 101–108. [Google Scholar] [CrossRef]
- Schmalz, T.; Bornmann, J.; Schirrmeister, B.; Schändlinger, J.; Schuler, M. Prinzipstudie zur Wirkung eines industriellen Exoskeletts bei Überkopfarbeit. Orthop. Tech. 2019, 70, 36–41. [Google Scholar]
- Huston, R.L. Principles of Biomechanics; CRC Press: Boca Raton, FL, USA, 2009; ISBN 9780849334948. [Google Scholar]
- Whipp, B.J.; Wasserman, K. Oxygen uptake kinetics for various intensities of constant-load work. J. Appl. Physiol. 1972, 33, 351–356. [Google Scholar] [CrossRef]
- Hermens, H.J. European Recommendations for Surface ElectroMyoGraphy. Results of the SENIAM Project; Roessingh Research and Development: Enschede, The Netherlands, 1999; ISBN 9075452152. [Google Scholar]
- Kluth, K.; Göbel, M.; Bopp, V.; Strasser, H. Anwendung der Oberflächen-Elektromyographie zur Beanspruchungsermittlung bei der arbeitsphysiologischen Beurteilung von Arbeitsplätzen und Arbeitsmitteln. Zentralblatt Arbeitsmedizin 2013, 63, 286–292. [Google Scholar] [CrossRef]
- Hof, A.L. A simple method to remove ECG artifacts from trunk muscle EMG signals. J. Electromyogr. Kinesiol. 2009, 19, 554–555. [Google Scholar] [CrossRef]
- De Luca, C.; Knaflitz, M. Surface Electromyography: What’s New? CLUT: Torino, Italy, 1992; ASIN B0010N33MY. [Google Scholar]
- Schmidt, R.F.; Thews, G. (Eds.) Physiologie des Menschen; Fünfundzwanzigste, korrigierte Auflage; Springer: Berlin/Heidelberg, Germany, 1993; ISBN 978-3-662-09337-5. [Google Scholar]
- Spriet, L.L. New insights into the interaction of carbohydrate and fat metabolism during exercise. Sports Med. 2014, 44, 87–96. [Google Scholar] [CrossRef] [PubMed]
- Robertson, D.G.E.; Caldwell, G.E.; Hamill, J.; Kamen, G.; Whittlesey, S.N. Research Methods in Biomechanics, 2nd ed.; Human Kinetics: Champaign, IL, USA, 2014; ISBN 0736093400. [Google Scholar]
- Paulsen, F.; Böckers, T.M.; Waschke, J.; Winkler, S.; Dalkowski, K.; Mair, J.; Klebe, S. Sobotta Anatomy Textbook: English Edition with Latin Nomenclature; Elsevier Health Sciences: Munich, Germany, 2018; ISBN 0720676177. [Google Scholar]
- Poppen, N.K.; Walker, P.S. Forces at the glenohumeral joint in abduction. Clin. Orthop. Relat. Res. 1978, 135, 165–170. [Google Scholar] [CrossRef]
- Page, P. Shoulder muscle imbalance and subacromial impingement syndrome in overhead athletes. Int. J. Sports Phys. Ther. 2011, 6, 51–58. [Google Scholar] [PubMed]
- Rashedi, E.; Kim, S.; Nussbaum, M.A.; Agnew, M.J. Ergonomic evaluation of a wearable assistive device for overhead work. Ergonomics 2014, 57, 1864–1874. [Google Scholar] [CrossRef]








© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schmalz, T.; Schändlinger, J.; Schuler, M.; Bornmann, J.; Schirrmeister, B.; Kannenberg, A.; Ernst, M. Biomechanical and Metabolic Effectiveness of an Industrial Exoskeleton for Overhead Work. Int. J. Environ. Res. Public Health 2019, 16, 4792. https://doi.org/10.3390/ijerph16234792
Schmalz T, Schändlinger J, Schuler M, Bornmann J, Schirrmeister B, Kannenberg A, Ernst M. Biomechanical and Metabolic Effectiveness of an Industrial Exoskeleton for Overhead Work. International Journal of Environmental Research and Public Health. 2019; 16(23):4792. https://doi.org/10.3390/ijerph16234792
Chicago/Turabian StyleSchmalz, Thomas, Jasmin Schändlinger, Marvin Schuler, Jonas Bornmann, Benjamin Schirrmeister, Andreas Kannenberg, and Michael Ernst. 2019. "Biomechanical and Metabolic Effectiveness of an Industrial Exoskeleton for Overhead Work" International Journal of Environmental Research and Public Health 16, no. 23: 4792. https://doi.org/10.3390/ijerph16234792