Technology Acceptance and Quality of Life among Older People Using a TUI Application


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Ethical Considerations
2.3. The Prototype—Tangible Cup
2.4. Instruments
2.4.1. Technology Acceptance Model (TAM)
2.4.2. Older People’s Quality of Life (OPQOL)
2.4.3. Semi-Structured Interview
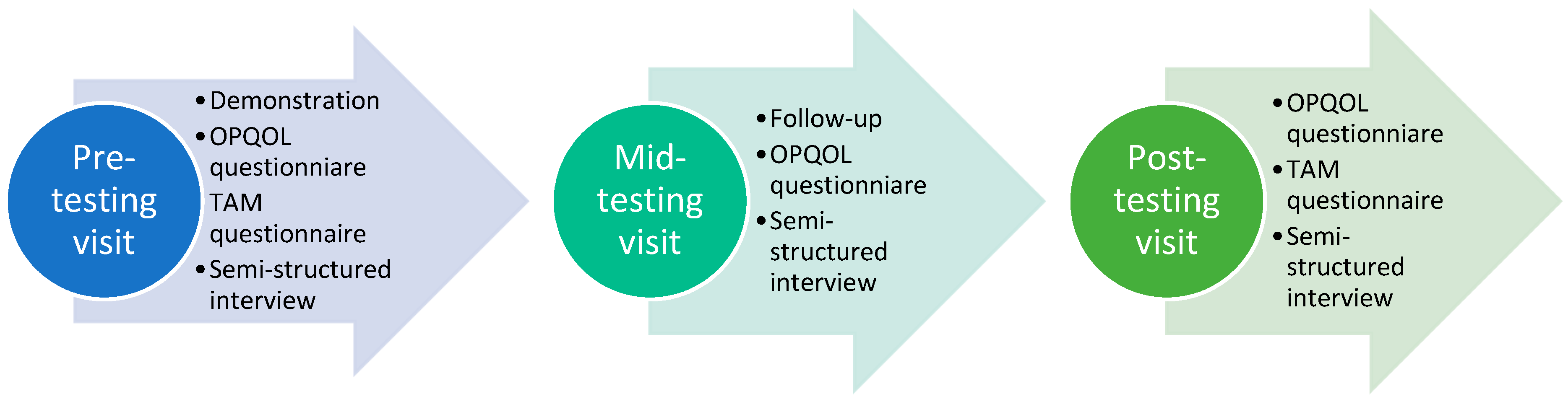
2.5. Data Collection
2.6. Data Analysis
3. Results
3.1. Characteristics of Participants
3.2. OPQOL Questionnaire and TAM Questionnaire
3.3. Semi-Structured Interview
3.3.1. Suitability of the Tangible Cup
“I liked it better when I was informed that I could use the tablet without these cups. I think so. Because then I only had to concentrate on one thing, so it was easier for me.”
“I made a call to one person here, and it rang and rang, and no one picked up the phone. Then I tried two more, the same day! After that I sent a SMS to you (referring to the main author of this paper). I was quite irritated, that I had to sit here and waste my time on this thing!”
“You have to sit down here with this thing and have it in front of you. But a phone is something you can have in your pocket and answer. You don’t need to sit down here to deal with it, you can do it at the kitchen table, or in the bathroom or anywhere. You can even sit on the toilet and talk on the phone, right? You can’t do that with this thing (Tangible Cup) here.”
“I go to the gym, meet friends, take care of the grandchildren….So I’m actually doing something all the time. So I don’t always remember this (referring to the Tangible Cup) is laying there. And since it isn’t ringing, I don’t do anything with it. If it rang then I would pick it up, if you understand? But, that’s how it is…”
3.3.2. Potential of the Tangible Cup
“I do know people who sit alone at home the whole winter, because it’s so slippery right? And they do become very lonely at home by themselves. Because their friends might not be able to go out either. So then it is quite a crisis for them, some people I know.”“I have an uncle who is 95 years old. He is bad with his feet, but his mind is totally fine. So my uncle in Drammen could certainly have enjoyed a system like this.”
“It would certainly be suitable for very lonely people too, but there has to be two people. So one of them could be very lonely, and the other could be relatively healthy and active. It will be a combination where one person doesn’t have much going on and can then call the other one.”
“If you are in a phase where you can easily select someone you know, and you don’t have to think about anything other than that cup and those cup coasters, because the rest sorts itself out, right. So I see the point, I do.”
“I think the idea is good, but one has to find a way to use it. I think there’s certainly many people sitting alone (at home), and they would then have someone to call, three, four, five people to call. Seeing the names displayed there (referring to Tangible Cup), when they’re logged in. So I think it can be useful, something like a social service, absolutely… I think.”
“We also do that at the senior center, so there are more people working with it. But most of them are only in one place, not at someone’s home. When one is using it alone (at home), one loses courage quickly, one does that.”
4. Discussion
4.1. Impact of TUI on Older People’s Technology Acceptance
4.2. Impact of TUI on Quality of Life
4.3. Association between Technology Acceptance and Quality of Life Before Testing and Their Changes After Testing
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Iwasa, H.; Kawaai, C.; Gondo, Y.; Inagaki, H.; Suzuki, T. Subjective well-being as a predictor of all-cause mortality among middle-aged and elderly people living in an urban Japanese community: A seven-year prospective cohort study. Geriatr. Gerontol. Int. 2006, 6, 216–222. [Google Scholar] [CrossRef]
- Cohen, R.; Bavishi, C.; Rozanski, A. Purpose in life and its relationship to all-cause mortality and cardiovascular events: A meta-analysis. Psychosom. Med. 2016, 78, 122–133. [Google Scholar] [CrossRef] [PubMed]
- Group, W. Study protocol for the World Health Organization project to develop a Quality of Life assessment instrument (WHOQOL). Qual. Life Res. 1993, 2, 153–159. [Google Scholar] [CrossRef]
- Bowling, A. The most important things in life. Comparisons between older and younger population age groups by gender. Results from a national survey of the public’s judgements. Int. J. Health Sci. 1995, 6, 169–176. [Google Scholar]
- Bowling, A.; Banister, D.; Sutton, S.; Evans, O.; Windsor, J. A multidimensional model of the quality of life in older age. Aging Ment. Health 2002, 6, 355–371. [Google Scholar] [CrossRef]
- Netuveli, G.; Blane, D. Quality of life in older ages. Br. Med. Bull. 2008, 85, 113–126. [Google Scholar] [CrossRef]
- Koceski, S.; Koceska, N. Evaluation of an assistive telepresence robot for elderly healthcare. J. Med. Syst. 2016, 40, 121. [Google Scholar] [CrossRef]
- Gaßner, K.; Conrad, M. ICT enabled independent living for elderly. In A Status-Quo Analysis on Products and the Research Landscape in the Field of Ambient Assisted Living (AAL) in EU-27 (October 2010); Druckerei Feller: Teltow, Germany, 2010. [Google Scholar]
- Gustafson, D.H.; McTavish, F.; Mahoney, J.E.; Johnson, R.A.; Lee, J.D.; Quanbeck, A.; Atwood, A.K.; Isham, A.; Veeramani, R.; Clemson, L. The effect of an information and communication technology (ICT) on older adults’ quality of life: Study protocol for a randomized control trial. Trials 2015, 16, 191. [Google Scholar] [CrossRef]
- Boz, H.; Karatas, S.E. A Review on Internet Use and Quality of Life of the Elderly. Cypriot J. Educ. Sci. 2015, 10, 182–191. [Google Scholar] [CrossRef]
- Miskelly, F.G. Assistive technology in elderly care. Age Ageing 2001, 30, 455–458. [Google Scholar] [CrossRef]
- Dascălu, M.; Rodideal, A.; Popa, L. In Romania, Elderly People Who Most Need ICT Are Those Who Are Less Probable to Use It. Soc. Work Rev. 2018, 17, 81–95. [Google Scholar]
- Chen, K.; Chan, A.H. A review of technology acceptance by older adults. Gerontechnology 2011, 10, 1–12. [Google Scholar] [CrossRef]
- ICT towards elderly independent living. Available online: https://www.researchgate.net/profile/Andrej_Grguric/publication/268177877_ICT_towards_elderly_independent_living/links/54edeb5b0cf25238f9393879/ICT-towards-elderly-independent-living.pdf (accessed on 15 November 2019).
- Ijsselsteijn, W.; Nap, H.H.; de Kort, Y.; Poels, K. Digital game design for elderly users. In Proceedings of the 2007 Conference on Future Play, Toronto, ON, Canada, 14–17 November 2007; pp. 17–22. [Google Scholar]
- Sánchez-Rico, A.; Garel, P.; Notarangelo, I.; Quintana, M.; Hernández, G.; Asteriadis, S.; Popa, M.; Vretos, N.; Solachidis, V.; Burgos, M. ICT Services for Life Improvement for the Elderly. Stud. Health Technol. Inform. 2017, 242, 600–605. [Google Scholar] [PubMed]
- Fischer, S.H.; David, D.; Crotty, B.H.; Dierks, M.; Safran, C. Acceptance and use of health information technology by community-dwelling elders. Int. J. Med. Inform. 2014, 83, 624–635. [Google Scholar] [CrossRef]
- Neves, B.B.; Amaro, F. Too old for technology? How the elderly of Lisbon use and perceive ICT. J. Community Inform. 2012, 8, 1–12. [Google Scholar]
- Chou, C.C.; Chang, C.P.; Lee, T.T.; Chou, H.F.; Mills, M.E. Technology acceptance and quality of life of the elderly in a telecare program. Comput. Inform. Nurs. CIN 2013, 31, 335–342. [Google Scholar] [CrossRef]
- Ishii, H.; Ullmer, B. Tangible bits: Towards seamless interfaces between people, bits and atoms. In Proceedings of the ACM SIGCHI Conference on Human Factors in Computing Systems, Atlanta, GA, USA, 22–27 March 1997; pp. 234–241. [Google Scholar]
- Davidoff, S.; Bloomberg, C.; Li, I.A.R.; Mankoff, J.; Fussell, S.R. The book as user interface: Lowering the entry cost to email for elders. In Proceedings of the CHI’05 Extended Abstracts on Human Factors in Computing Systems, Portland, OR, USA, 2–7 April 2005; pp. 1331–1334. [Google Scholar]
- Spreicer, W. Tangible interfaces as a chance for higher technology acceptance by the elderly. In Proceedings of the 12th International Conference on Computer Systems and Technologies, Vienna, Austria, 16–17 June 2011; pp. 311–316. [Google Scholar]
- Marques, T.; Nunes, F.; Silva, P.; Rodrigues, R. Tangible interaction on tabletops for elderly people. In Proceedings of the International Conference on Entertainment Computing, Vancouver, BC, Canada, 5–8 October 2011; pp. 440–443. [Google Scholar]
- Bong, W.K.; Chen, W. Tangible Cup for Elderly Social Interaction: Design TUI for & with Elderly. J. Technol. Pers. Disabil. 2019, 7, 64–78. [Google Scholar]
- Abras, C.; Maloney-Krichmar, D.; Preece, J. User-centered design. In Berkshire Encyclopedia of Human-Computer Interaction; Bainbridge, W., Ed.; Sage Publications: Thousand Oaks, CA, USA, 2004; Volume 37, pp. 445–456. [Google Scholar]
- Steen, M.; Manschot, M.; De Koning, N. Benefits of co-design in service design projects. Int. J. Des. 2011, 5, 53–60. [Google Scholar]
- Mostaghel, R.; Oghazi, P. Elderly and technology tools: A fuzzyset qualitative comparative analysis. Qual. Quant. 2017, 51, 1969–1982. [Google Scholar] [CrossRef]
- Chiu, C.-J.; Hu, Y.-H.; Lin, D.-C.; Chang, F.-Y.; Chang, C.-S.; Lai, C.-F. The attitudes, impact, and learning needs of older adults using apps on touchscreen mobile devices: Results from a pilot study. Comput. Hum. Behav. 2016, 63, 189–197. [Google Scholar] [CrossRef]
- Dogruel, L.; Joeckel, S.; Bowman, N.D. The use and acceptance of new media entertainment technology by elderly users: Development of an expanded technology acceptance model. Behav. Inf. Technol. 2015, 34, 1052–1063. [Google Scholar] [CrossRef]
- Hsiao, C.-H.; Tang, K.-Y. Examining a model of mobile healthcare technology acceptance by the elderly in Taiwan. J. Glob. Inf. Technol. Manag. 2015, 18, 292–311. [Google Scholar] [CrossRef]
- Lekjaroen, K.; Ponganantayotin, R.; Charoenrat, A.; Funilkul, S.; Supasitthimethee, U.; Triyason, T. IoT Planting: Watering system using mobile application for the elderly. In Proceedings of the 2016 International Computer Science and Engineering Conference (ICSEC), Chiangmai, Thailand, 14–17 December 2016; pp. 1–6. [Google Scholar]
- Bowling, A. The psychometric properties of the older people’s quality of life questionnaire, compared with the CASP-19 and the WHOQOL-OLD. Curr. Gerontol. Geriatr. Res. 2009, 2009, 298950. [Google Scholar] [CrossRef] [PubMed]
- Beaton, D.E.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Guidelines for the Process of Cross-Cultural Adaptation of Self-Report Measures. Spine 2000, 25, 3186–3191. [Google Scholar] [CrossRef]
- Pallant, J.; Manual, S.S. A Step by Step Guide to Data Analysis Using SPSS; McGraw-Hill Education: Berkshire, UK, 2010. [Google Scholar]
- Elo, S.; Kyngäs, H. The qualitative content analysis process. J. Adv. Nurs. 2008, 62, 107–115. [Google Scholar] [CrossRef]
- White, M.D.; Marsh, E.E. Content analysis: A flexible methodology. Libr. Trends 2006, 55, 22–45. [Google Scholar] [CrossRef]
- Cavanagh, S. Content analysis: Concepts, methods and applications. Nurse Res. 1997, 4, 5–16. [Google Scholar] [CrossRef]
- Craik, F.I. Memory changes in normal aging. Curr. Dir. Psychol. Sci. 1994, 3, 155–158. [Google Scholar] [CrossRef]
- Collie, A.; Maruff, P.; Shafiq-Antonacci, R.; Smith, M.; Hallup, M.; Schofield, P.; Masters, C.; Currie, J. Memory decline in healthy older people: Implications for identifying mild cognitive impairment. Neurology 2001, 56, 1533–1538. [Google Scholar] [CrossRef]
- Chen, Y.-R.R.; Schulz, P.J. The effect of information communication technology interventions on reducing social isolation in the elderly: A systematic review. J. Med. Internet Res. 2016, 18, e18. [Google Scholar] [CrossRef]
- Dickinson, A.; Gregor, P. Computer use has no demonstrated impact on the well-being of older adults. Int. J. Hum. Comput. Stud. 2006, 64, 744–753. [Google Scholar] [CrossRef]
- Mitzner, T.L.; Boron, J.B.; Fausset, C.B.; Adams, A.E.; Charness, N.; Czaja, S.J.; Dijkstra, K.; Fisk, A.D.; Rogers, W.A.; Sharit, J. Older adults talk technology: Technology usage and attitudes. Comput. Hum. Behav. 2010, 26, 1710–1721. [Google Scholar] [CrossRef] [PubMed]
- Tung, F.-C.; Chang, S.-C.; Chou, C.-M. An extension of trust and TAM model with IDT in the adoption of the electronic logistics information system in HIS in the medical industry. Int. J. Med. Inform. 2008, 77, 324–335. [Google Scholar] [CrossRef] [PubMed]
- Ryu, M.-H.; Kim, S.; Lee, E. Understanding the factors affecting online elderly user’s participation in video UCC services. Comput. Hum. Behav. 2009, 25, 619–632. [Google Scholar] [CrossRef]
- Blažun, H.; Saranto, K.; Kokol, P.; Vošner, J. Information and communication technology as a tool for improving physical and social activity of the elderly. In Proceedings of the NI 2012: 11th International Congress on Nursing Informatics, Montreal, QC, Canada, 23–27 June 2012. [Google Scholar]
- Bilotta, C.; Bowling, A.; Nicolini, P.; Casè, A.; Pina, G.; Rossi, S.V.; Vergani, C. Older People’s Quality of Life (OPQOL) scores and adverse health outcomes at a one-year follow-up. A prospective cohort study on older outpatients living in the community in Italy. Health Qual. Life Outcomes 2011, 9, 72. [Google Scholar] [CrossRef]
- Kojima, G.; Iliffe, S.; Morris, R.W.; Taniguchi, Y.; Kendrick, D.; Skelton, D.A.; Masud, T.; Bowling, A. Frailty predicts trajectories of quality of life over time among British community-dwelling older people. Qual. Life Res. 2016, 25, 1743–1750. [Google Scholar] [CrossRef] [Green Version]
- Dattilo, J.; Lorek, A.E.; Mogle, J.; Sliwinski, M.; Freed, S.; Frysinger, M.; Schuckers, S. Perceptions of leisure by older adults who attend senior centers. Leis. Sci. 2015, 37, 373–390. [Google Scholar] [CrossRef]
- Cohen, P.; West, S.G.; Aiken, L.S. Applied Multiple Regression/Correlation Analysis for the Behavioral Sciences; Psychology Press: New York, NY, USA, 2014. [Google Scholar]
- Christophorou, C.; Kleanthous, S.; Georgiadis, D.; Cereghetti, D.M.; Andreou, P.; Wings, C.; Christodoulou, E.; Samaras, G. ICT services for active ageing and independent living: Identification and assessment. Healthc. Technol. Lett. 2016, 3, 159–164. [Google Scholar] [CrossRef] [Green Version]
- Bowling, A.; Stenner, P. Which measure of quality of life performs best in older age? A comparison of the OPQOL, CASP-19 and WHOQOL-OLD. J. Epidemiol. Community Health 2011, 65, 273–280. [Google Scholar] [CrossRef]
- Button, K.S.; Ioannidis, J.P.A.; Mokrysz, C.; Nosek, B.A.; Flint, J.; Robinson, E.S.J.; Munafò, M.R. Power failure: Why small sample size undermines the reliability of neuroscience. Nat. Rev. Neurosci. 2013, 14, 365. [Google Scholar] [CrossRef] [Green Version]
- Zickuhr, K.; Madden, M. Older Adults and Internet Use: For the First Time, Half of Adults Ages 65 and Older Are Online; Pew Research Center’s Internet & American Life Project; Pew Research Center: Washington, DC, USA, 2012. [Google Scholar]
- González, A.; Ramírez, M.P.; Viadel, V. Attitudes of the Elderly Toward Information and Communications Technologies. Educ. Gerontol. 2012, 38, 585–594. [Google Scholar] [CrossRef]
- Framtidens eldre i by og bygd. Befolkningsframskrivinger, sosiodemografiske mønstre og helse. Available online: https://ssb.brage.unit.no/ssb-xmlui/bitstream/handle/11250/2490230/RAPP2017-32_web.pdf?sequence=1&isAllowed=y (accessed on 10 September 2019).
- Mayo, A.M. Psychometric instrumentation: Reliability and validity of instruments used for clinical practice, evidence-based practice projects and research studies. Clin. Nurse Spec. 2015, 29, 134–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hak, T.; van der Veer, K.; Jansen, H. The Three-Step Test-Interview (TSTI): An observational instrument for pretesting self-completion questionnaires. Surv. Res. Methods 2008, 2, 143–150. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dimension | Items | Reference |
|---|---|---|
| D1. Perceived usefulness | Q1. By using digital communication tools, I can have better social interactions with my friends. | [27,28,29,30,31] |
| Q2. By using digital communication tools, I can have a better social life. | ||
| Q3. By using digital communication tools, I can make new friends. | ||
| D2. Perceived ease of use | Q4. Interaction with digital communication tools is clear and understandable. | [27,28,29,30,31] |
| Q5. Interaction with digital communication tools does not require a lot of mental effort. | ||
| Q6. I find digital communication tools easy to use. | ||
| Q7. I find it easy to learn to use digital communication tools. | ||
| D3. Perceived enjoyment | Q8. I find it enjoyable to use digital communications tools. | [29] |
| Q9. I find it exciting to use digital communications tools. | ||
| Q10. I find it pleasant to use digital communications tools. | ||
| Q11. I find it interesting to use digital communications tools. | ||
| D4. Intention to use | Q12. I would use digital communication tools. | [30,31] |
| D5. Actual use | Q13. I use digital communication tools very often. | [29] |
| D6. Compatibility | Q14. Using digital communication tools is compatible with most aspects of my social life. | [28] |
| Q15. Using digital communication tools fits my lifestyle. | ||
| Q16. Using digital communication tools fits well with the way I socialize with others. | ||
| D7. Attitude | Q17. Using digital communication tools is a good idea. | [28,30,31] |
| Q18. I am positive towards digital communication tools. | ||
| D8. Self-efficacy | Q19. I feel confident about learning to use digital communication tools. | [29] |
| Q20. I feel confident about using digital communication tools. | ||
| Q21. I have the necessary skills in using digital communication tools. |
| Age | Gender | Education (Years) | ICT Skills | |
|---|---|---|---|---|
| P1 | 79 | Female | 12 | Basic |
| P2 | 74 | Female | 11 | Basic |
| P3 | 82 | Female | 21 | Basic |
| P4 | 77 | Female | 10 | Basic |
| P5 | 76 | Female | 14 | Very advanced |
| P6 | 81 | Female | 15 | Basic |
| P7 | 82 | Female | 10 | Advanced |
| P8 | 72 | Female | 12 | Advanced |
| P9 | 82 | Female | 13 | Basic |
| P10 | 81 | Female | 14 | Basic |
| P11 | 81 | Female | 19 | Advanced |
| P12 | 89 | Male | 17 | Advanced |
| P13 | 77 | Female | 11 | Advanced |
| P14 | 83 | Male | 14 | Advanced |
| P15 | 83 | Female | 12 | Advanced |
| P16 | 79 | Female | 12 | Advanced |
| P17 | 77 | Female | 11 | Advanced |
| P18 | 81 | Female | 8 | Basic |
| P19 | 76 | Female | 13 | Very advanced |
| P20 | 79 | Female | 10 | Basic |
| Correlations | ||
|---|---|---|
| Spearman’s Rho | ||
| TAM (Total Score) | ||
| Correlation Coefficient | p-Value | |
| OPQOL (total score) | −0.03 | 0.92 |
| OPQOL _D1 (life overall) | −0.34 | 0.19 |
| OPQOL _D2 (health) | 0.20 | 0.46 |
| OPQOL _D3 (social relationships and participation) | −0.41 | 0.12 |
| OPQOL _D4 (independence, control over life, freedom) | 0.05 | 0.86 |
| OPQOL _D5 (home and neighborhood) | 0.19 | 0.48 |
| OPQOL _D6 (psychological and emotion well-being) | 0.05 | 0.85 |
| OPQOL _D7 (financial circumstances) | 0.03 | 0.90 |
| OPQOL _D8 (leisure and activities) | 0.20 | 0.47 |
| OPQOL _Q (First question evaluating quality of life as a whole) | −0.30 | 0.27 |
| 1 Strongly Disagree | 2 Disagree | 3 Somewhat Disagree | 4 Neither Disagree nor Agree | 5 Somewhat Agree | 6 Agree | 7 Strongly Agree | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Pre | Post | Pre | Post | Pre | Post | Pre | Post | Pre | Post | |
| D1. Perceived usefulness | 12.50 | 14.58 | 6.25 | 4.17 | 12.5 | 8.33 | 18.75 | 10.42 | 20.83 | 31.25 | 14.58 | 22.92 | 14.58 | 8.33 |
| D2. Perceived ease of use | 3.13 | 1.56 | 9.38 | 3.13 | 12.5 | 21.88 | 34.38 | 10.94 | 12.50 | 31.25 | 23.44 | 31.25 | 4.69 | 0 |
| D3. Perceived enjoyment | 4.69 | 0 | 3.13 | 3.13 | 4.69 | 12.5 | 37.50 | 14.06 | 12.50 | 25.00 | 6.25 | 10.94 | 31.25 | 34.38 |
| D4. Intention to use | 0 | 0 | 0 | 0 | 0 | 6.25 | 31.25 | 12.50 | 12.50 | 0 | 31.25 | 43.75 | 25.00 | 37.50 |
| D5. Actual use | 0 | 0 | 0 | 0 | 6.25 | 0 | 6.25 | 6.25 | 25.00 | 12.50 | 37.50 | 37.50 | 25.00 | 43.75 |
| D6. Compatibility | 12.50 | 2.08 | 4.17 | 0 | 16.67 | 12.50 | 20.83 | 20.83 | 8.33 | 16.67 | 25.00 | 35.42 | 12.50 | 12.50 |
| D7. Attitude | 0 | 0 | 3.13 | 0 | 6.25 | 0 | 18.75 | 6.25 | 15.63 | 25.00 | 40.63 | 37.50 | 15,63 | 31.25 |
| D8. Self-efficacy | 0 | 0 | 2.08 | 0 | 8.33 | 2.08 | 0 | 2.08 | 25.00 | 27.08 | 45.83 | 50.00 | 18,75 | 18.75 |
| OPQOL | OPQOL_D1 | OPQOL_D2 | OPQOL_D3 | OPQOL_D4 | OPQOL_D5 | OPQOL_D6 | OPQOL_D7 | OPQOL_D8 | OPQOL_Q | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Spearman’s rho | TAM | Correlation Coefficient | 0.21 | −0.17 | 0.07 | −0.31 | −0.11 | 0.62 ** | 0.21 | 0.06 | 0.29 | −0.02 |
| p -value | 0.44 | 0.53 | 0.79 | 0.24 | 0.70 | 0.01 | 0.44 | 0.82 | 0.28 | 0.95 | ||
| TAM_D1 | Correlation Coefficient | 0.05 | −0.11 | 0.02 | −0.44 | 0.01 | 0.35 | 0.11 | −0.04 | 0.22 | −0.23 | |
| p -value | 0.86 | 0.69 | 0.93 | 0.09 | 0.98 | 0.18 | 0.68 | 0.88 | 0.42 | 0.40 | ||
| TAM_D2 | Correlation Coefficient | 0.29 | −0.17 | 0.19 | −0.04 | −0.14 | 0.59 * | 0.34 | 0.16 | 0.14 | −0.17 | |
| p -value | 0.27 | 0.54 | 0.49 | 0.89 | 0.61 | 0.02 | 0.20 | 0.55 | 0.60 | 0.52 | ||
| TAM_D3 | Correlation Coefficient | 0.19 | 0.19 | −0.07 | −0.20 | 0.29 | 0.14 | −0.15 | 0.20 | 0.26 | 0.42 | |
| p -value | 0.48 | 0.48 | 0.80 | 0.45 | 0.28 | 0.61 | 0.57 | 0.45 | 0.33 | 0.10 | ||
| TAM_D4 | Correlation Coefficient | 0.64 ** | −0.07 | 0.36 | 0.33 | 0.25 | 0.29 | −0.07 | 0.60 * | 0.06 | 0.21 | |
| p -value | 0.01 | 0.80 | 0.17 | 0.22 | 0.35 | 0.28 | 0.80 | 0.02 | 0.84 | 0.43 | ||
| TAM_D5 | Correlation Coefficient | 0.36 | −0.03 | 0.32 | 0.08 | −0.03 | 0.27 | 0.50 | 0.27 | 0.07 | −0.51 * | |
| p -value | 0.18 | 0.91 | 0.23 | 0.76 | 0.91 | 0.32 | 0.05 | 0.31 | 0.79 | 0.04 | ||
| TAM_D6 | Correlation Coefficient | 0.20 | 0.08 | 0.11 | −0.07 | −0.05 | 0.24 | 0.44 | 0.11 | 0.27 | −0.37 | |
| p -value | 0.46 | 0.76 | 0.68 | 0.79 | 0.85 | 0.37 | 0.09 | 0.69 | 0.32 | 0.16 | ||
| TAM_D7 | Correlation Coefficient | 0.29 | 0.11 | −0.01 | 0.01 | 0.02 | 0.39 | 0.11 | 0.06 | 0.17 | 0.70 ** | |
| p -value | 0.27 | 0.68 | 0.98 | 0.98 | 0.94 | 0.14 | 0.70 | 0.83 | 0.54 | 0.00 | ||
| TAM_D8 | Correlation Coefficient | 0.23 | −0.47 | 0.19 | −0.01 | −0.25 | 0.54 * | 0.24 | 0.20 | 0.05 | 0.07 | |
| p-value | 0.40 | 0.07 | 0.48 | 0.96 | 0.36 | 0.03 | 0.38 | 0.45 | 0.90 | 0.80 | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bong, W.K.; Bergland, A.; Chen, W. Technology Acceptance and Quality of Life among Older People Using a TUI Application. Int. J. Environ. Res. Public Health 2019, 16, 4706. https://doi.org/10.3390/ijerph16234706
Bong WK, Bergland A, Chen W. Technology Acceptance and Quality of Life among Older People Using a TUI Application. International Journal of Environmental Research and Public Health. 2019; 16(23):4706. https://doi.org/10.3390/ijerph16234706
Chicago/Turabian StyleBong, Way Kiat, Astrid Bergland, and Weiqin Chen. 2019. "Technology Acceptance and Quality of Life among Older People Using a TUI Application" International Journal of Environmental Research and Public Health 16, no. 23: 4706. https://doi.org/10.3390/ijerph16234706