Quality of Life and Work Ability among Healthcare Personnel with Chronic Viral Hepatitis. Evaluation of the Inpatient Rehabilitation Program of the Wartenberg Clinic


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Sample, and Measurements
2.2. Power Estimation
2.3. Statistical Analyses
2.4. Ethical Approval
3. Results
3.1. Description of the Cohort
3.2. Results of the Clinical Survey
3.3. Results of the Survey Based on Self-Assessment Questionnaires
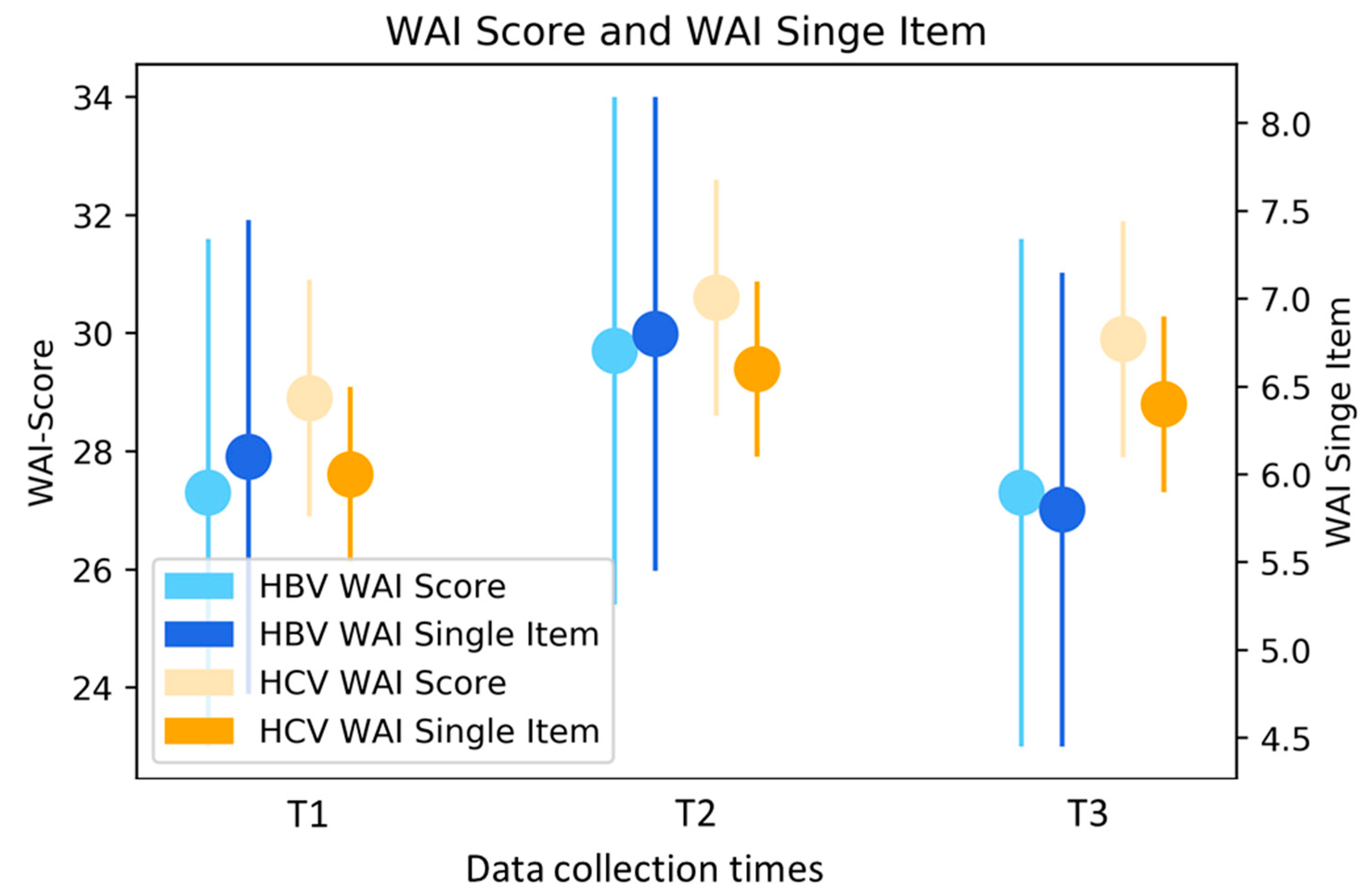
3.3.1. WAI (n = 66)
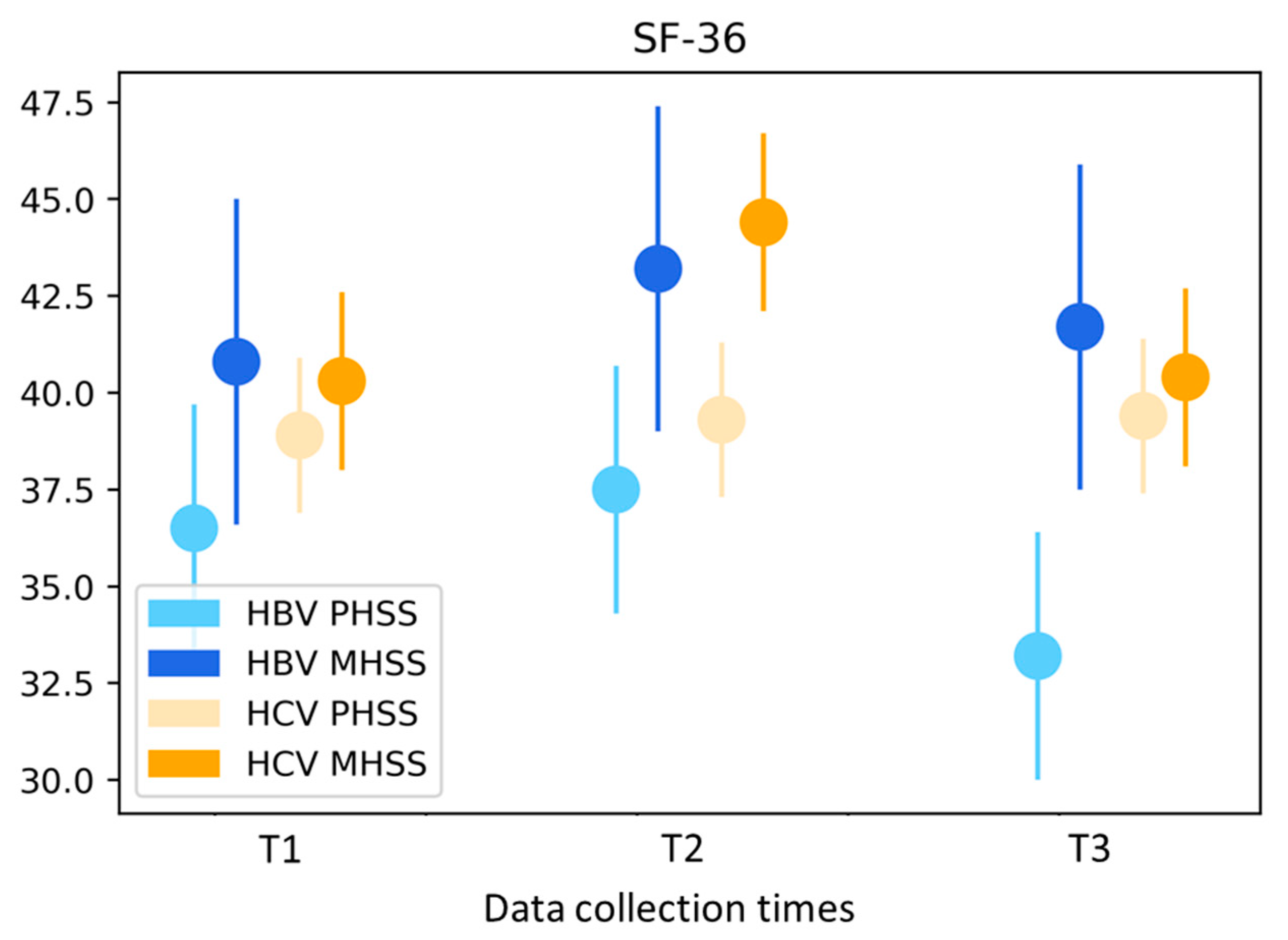
3.3.2. SF-36 (n = 160)
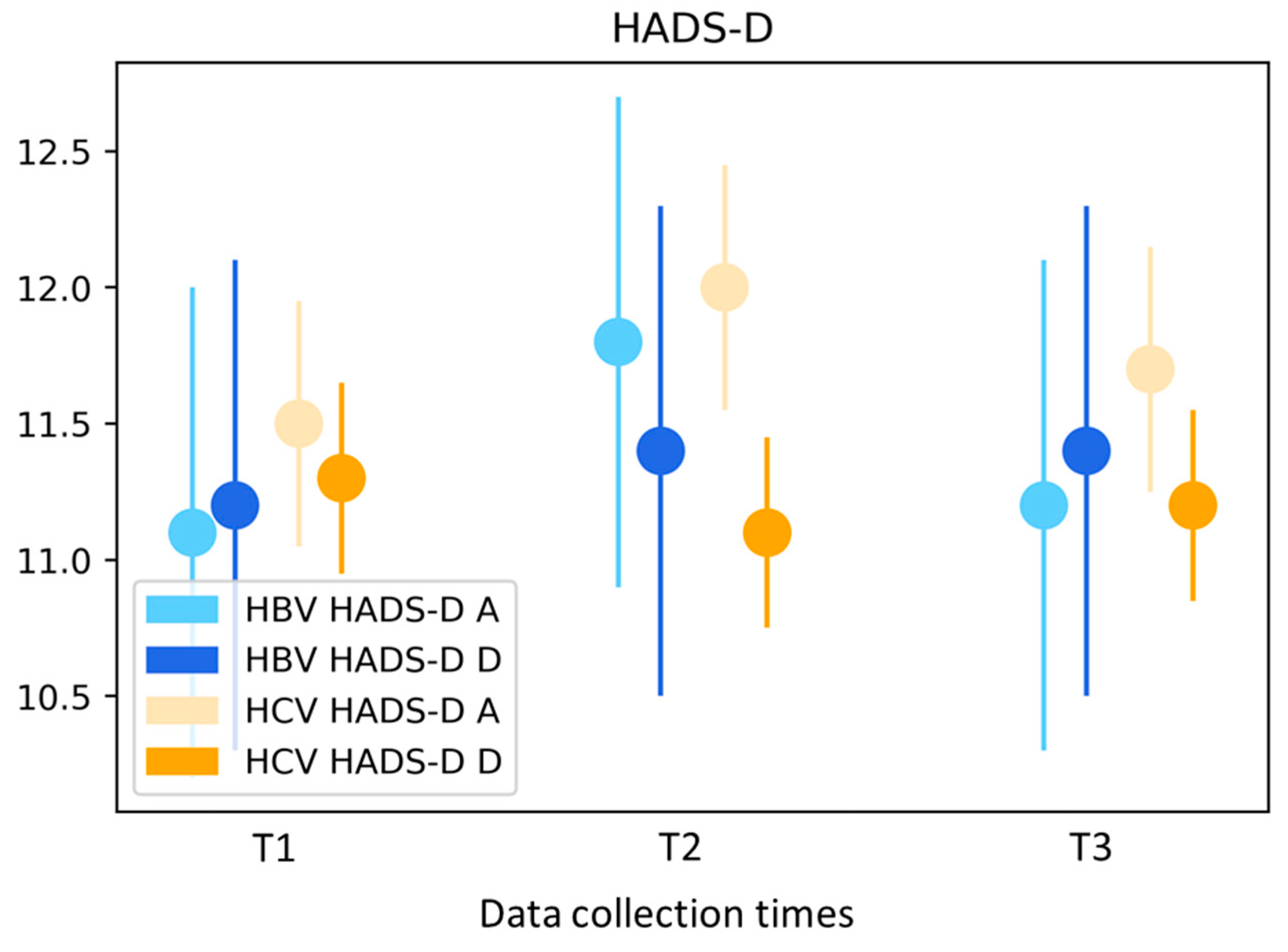
3.3.3. HADS-D (n = 159)
3.4. Satisfaction Survey at T2
4. Discussion
Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Variable * | Total | |
|---|---|---|
| Gender | Female | 12 (86) |
| Male | 2 (14) | |
| Age | Mean (SD) | 59 (8) |
| Working | Yes | 6 (43) |
| Type of Hepatitis | B | 2 (14) |
| C | 12 (86) | |
| Place of birth | Germany | 10 (71) |
| Other | 4 (29) | |
| Household | Single | 7 (50) |
| With Partner and Child(s) | 6 (43) | |
| With Child(s) | 1 (7) | |
| Occupation | Physician | 1 (15) |
| Nurses | 5 (38) | |
| Nursing Home Nurse | 2 (15) | |
| Nurse’s Assistant | 4 (32) | |
| Net household income in € | <2000 | 7 (58) |
| 2000 to <4000 | 3 (25) | |
| ≥4000 | 2 (17) | |
| Chronic Hepatitis for | 10–19 years | 3 (25) |
| 20–29 years | 7 (58) | |
| 30–39 years | 2 (17) | |
| Liver Status | Fibrosis | 8 (66) |
| Cirrhosis | 5 (28) | |
| Without Findings | 1 (6) | |
| RWA | <50 | 7 (50) |
| ≥50 | 7 (50) | |
| Body Mass Index | 19 to <25 Normal | 6 (43) |
| 25 to <30 Overweight | 5 (36) | |
| ≥30 Obesity | 3 (21) | |
| Regular Physical Activity | Yes | 6 (43) |
| Smoking | Yes | 3 (21) |
| Mental Stress | Fatigue | 9 (64) |
| Depression | 4 (29) | |
| Variable 1 | Total | |
|---|---|---|
| n | % | |
| Physician care | 159 | 98 |
| Nursing and assistance staff | 155 | 95 |
| Physiotherapy | 158 | 97 |
| Physical care | 159 | 98 |
| Psychological care | 78 | 96 |
| Catering | 156 | 96 |
| Objectives pursued (multiple nominations) | ||
| Specialist medical care | 91 | 56 |
| Physical stabilisation | 94 | 58 |
| Mental stabilisation | 82 | 50 |
| Other 2 | 14 | 9 |
| Main goals achieved | ||
| Yes | 148 | 91 |
References
- World Health Organization. Global Hepatitis Report 2017; Licence: CC BY-NC-SA 3.0 IGO; World Health Organization: Geneva, Switzerland, 2017; p. 83. Available online: http://www.who.int/hepatitis/publications/global-hepatitis-report2017/en/ (accessed on 6 August 2019).
- World Health Organization. Guidelines for the Prevention, Care and Treatment of Persons with Chronic Hepatitis B Infection; World Health Organization: Geneva, Switzerland, 2015; Available online: https://www.who.int/hiv/pub/hepatitis/hepatitis-b-guidelines/en/ (accessed on 6 August 2019).
- Blachier, M.; Leleu, H.; Peck-Radosavljevic, M.; Valla, D.C.; Roudot-Thoraval, F. The burden of liver disease in Europe: A review of available epidemiological data. J. Hepatol. 2013, 58, 593–608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gomaa, A.I.; Waked, I. Recent advances in multidisciplinary management of hepatocellular carcinoma. World J. Hepatol. 2015, 7, 673–687. [Google Scholar] [CrossRef] [PubMed]
- Deuffic-Burban, S.; Delarocque-Astagneau, E.; Abiteboul, D.; Bouvet, E.; Yazdanpanah, Y. Blood-borne viruses in health care workers: Prevention and management. J. Clin. Virol. 2011, 52, 4–10. [Google Scholar] [CrossRef] [PubMed]
- Quelhas, R.; Lopes, A. Psychiatric problems in patients infected with hepatitis C before and during antiviral treatment with interferon-alpha: A review. J. Psychiatr. Pract. 2009, 15, 262–281. [Google Scholar] [CrossRef] [PubMed]
- Hilsabeck, R.C.; Hassanein, T.I.; Carlson, M.D.; Ziegler, E.A.; Perry, W. Cognitive functioning and psychiatric symptomatology in patients with chronic hepatitis C. J. Int. Neuropsychol. Soc. JINS 2003, 9, 847–854. [Google Scholar] [CrossRef] [PubMed]
- Dulon, M.; Wendeler, D.; Nienhaus, A. Berufsbedingte Infektionskrankheiten bei Beschäftigten im Gesundheitsdienst 2017: Routinedaten der Berufsgenossenschaft für Gesundheitsdienst und Wohlfahrtspflege. Zentralblatt für Arbeitsmedizin Arbeitsschutz und Ergonomie 2019, 69, 16–22. [Google Scholar] [CrossRef]
- Hasselhorn, H.M.; Freude, G. Der Work Ability Index. Ein Leitfaden (Schriftenreihe der Bundesanstalt für Arbeitsschutz und Arbeitsmedizin Sonderschrift, Bd. 87); Fachverlag NW in Carl Ed. Schünemann KG: Bremerhaven, Germany, 2007. [Google Scholar]
- Gould, R.; Ilmarinen, J.; Järvisalo, J.; Koskinen, S. Dimensions of Work Ability—Results of the Health 2000 Survey; Finnish Institute of Occupational Health (FIOH): Helsinki, Finland, 2008. [Google Scholar]
- Morfeld, M.; Kirchberger, I.; Bullinger, M. SF-36 Fragebogen zum Gesundheitszustand: Deutsche Version des Short Form-36 Health Survey; Hofgrefe: Göttingen, Germany, 2011; Volume 2, ergänzte und überarbeitete Auflage. [Google Scholar]
- Hermann-Lingen, C.; Buss, U.; Snaith, R.P. Hospital Anxiety and Depression Scale—Deutsche Version (HADS-D); Verlag Hans Huber: Bern, Switzerland, 2011; Volume 3, aktualisierte und neu normierte Auflage. [Google Scholar]
- Walters, S.J. Sample size and power estimation for studies with health related quality of life outcomes: A comparison of four methods using the SF-36. Health Qual. Life Outcomes 2004, 2, 26. [Google Scholar] [CrossRef] [PubMed]
- Klein, M.; Halsbeck, J. Mit chronischer Krankheit arbeiten (k)ein Problem? ASU Arb. Soz. Umweltmed. 2015, 50, 788–793. [Google Scholar]
- Prümper, J.; Richenhagen, G. Von der Arbeitsunfähigkeit zum Haus der Arbeitsfähigkeit. In Der Work Ability Index und Seine Anwendung; Seyfried, B., Ed.; Bertelsmann: Bielefeld, Germany, 2011. [Google Scholar]
- Converso, D.; Sottimano, I.; Guidetti, G.; Loera, B.; Cortini, M.; Viotti, S. Aging and Work Ability: The Moderating Role of Job and Personal Resources. Front. Psychol. 2017, 8, 2262. [Google Scholar] [CrossRef] [PubMed]
- Koolhaas, W.; van der Klink, J.J.; de Boer, M.R.; Groothoff, J.W.; Brouwer, S. Chronic health conditions and work ability in the ageing workforce: The impact of work conditions, psychosocial factors and perceived health. Int. Arch. Occup. Environ. Health 2014, 87, 433–443. [Google Scholar] [CrossRef] [PubMed]
- Van den Berg, T.I.; Elders, L.A.; de Zwart, B.C.; Burdorf, A. The effects of work-related and individual factors on the Work Ability Index: A systematic review. Occup. Environ. Med. 2009, 66, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Dirks, M.; Pflugrad, H.; Haag, K.; Tillmann, H.L.; Wedemeyer, H.; Arvanitis, D.; Hecker, H.; Tountopoulou, A.; Goldbecker, A.; Worthmann, H.; et al. Persistent neuropsychiatric impairment in HCV patients despite clearance of the virus? J. Viral Hepat. 2017, 24, 541–550. [Google Scholar] [CrossRef] [PubMed]
- Ashrafi, M.; Modabbernia, A.; Dalir, M.; Taslimi, S.; Karami, M.; Ostovaneh, M.R.; Malekzadeh, R.; Poustchi, H. Predictors of mental and physical health in non-cirrhotic patients with viral hepatitis: A case control study. J. Psychosom. Res. 2012, 73, 218–224. [Google Scholar] [CrossRef] [PubMed]
- Erim, Y.; Tagay, S.; Beckmann, M.; Bein, S.; Cicinnati, V.; Beckebaum, S.; Senf, W.; Schlaak, J.F. Depression and protective factors of mental health in people with hepatitis C: A questionnaire survey. Int. J. Nurs. Stud. 2010, 47, 342–349. [Google Scholar] [CrossRef] [PubMed]
- Amodio, P.; Salari, L.; Montagnese, S.; Schiff, S.; Neri, D.; Bianco, T.; Minazzato, L. Hepatitis C virus infection and health-related quality of life. World J. Gastroenterol. WJG 2012, 18, 2295–2299. [Google Scholar] [CrossRef] [PubMed]
- Heintges, T.; Erhardt, A.; Sagir, A.; Häussinger, D. Kombinationstherapie der chronischen Hepatitis C: Pegyliertes (PEG)-Interferon und Ribavirin. Dtsch. Arztebl.-Arztl. Mitt.-Ausg. A 2002, 99, 1239–1241. [Google Scholar]
- Kohli, A.; Shaffer, A.; Sherman, A.; Kottilil, S. Treatment of hepatitis C: A systematic review. JAMA 2014, 312, 631–640. [Google Scholar] [CrossRef] [PubMed]
- Kraus, M.R.; Wilms, K. Interferon-αWirkung, Indikationen, Therapieüberwachung und Nebenwirkungen. Der Internist 2000, 41, 1399–1406. [Google Scholar] [CrossRef] [PubMed]
- Vabo, I.L.; Ferreira, L.E.; Pace, F.H. Depressive Episode Incidence in Patients with Chronic Hepatitis C Treated with Pegylated Interferon and Ribavirin. Arq. Gastroenterol. 2016, 53, 20–24. [Google Scholar] [CrossRef] [PubMed]
- Carrat, F.; Fontaine, H.; Dorival, C.; Simony, M.; Diallo, A.; Hezode, C.; De Ledinghen, V.; Larrey, D.; Haour, G.; Bronowicki, J.P.; et al. Clinical outcomes in patients with chronic hepatitis C after direct-acting antiviral treatment: A prospective cohort study. Lancet 2019, 393, 1453–1464. [Google Scholar] [CrossRef]



| Variable * | Total | Working | HCV | HBV | p Value | |
|---|---|---|---|---|---|---|
| HP | 163 (%) | 66 (%) | 132 (%) | (31 %) | ||
| Gender | Female | 123 (75) | 56 (85) | 104 (79) | 19 (61) | p = 0.32 |
| Male | 40 (25) | 10 (15) | 28 (21) | 12 (39) | ||
| Age | Mean (SD) | 63 (9) | 56 (6) | 62 (9) | 66 (9) | p = 0.03 |
| Nationality | German | 151 (95) | 60 (94) | 124 (96) | 27 (90) | p = 0.34 |
| Other | 8 (5) | 4 (6) | 5 (4) | 3 (10) | ||
| Place of birth | Germany | 129 (79) | 55 (83) | 108 (82) | 21 (68) | p = 0.10 |
| Other | 34 (21) | 11 (17) | 24 (18) | 10 (32) | ||
| Marital status | Single | 17 (10) | 10 (15) | 17 (13) | - | p = 0.59 |
| Married | 96 (59) | 38 (57) | 74 (56) | 22 (71) | ||
| Divorced | 32 (20) | 13 (20) | 28 (21) | 4 (13) | ||
| Widowed | 18 (11) | 5 (8) | 13 (10) | 5 (16) | ||
| Household | Single | 51 (31) | 18 (27) | 42 (32) | 9 (29) | p = 0.19 |
| With Partner | 84 (51) | 29 (43) | 63 (48) | 21 (68) | ||
| With Partner and Child(s) | 22 (14) | 15 (23) | 21 (16) | 1 (3) | ||
| With Child(s) | 2 (1) | 1 (2) | 2 (1) | - | ||
| With Relatives or Friends | 4 (3) | 3 (5) | 4 (3) | - | ||
| Highest Level of Education | Secondary School | 32 (20) | 9 (14) | 25 (19) | 7 (24) | p = 0.29 |
| Polytechnic Secondary School | 78 (48) | 35 (53) | 66 (51) | 12 (41) | ||
| Higher Education | 46 (28) | 21 (32) | 37 (28) | 9 (32) | ||
| Other | 4 (4) | 1 (1) | 3 (2) | 1 (3) | ||
| Occupation | Physician | 15 (9) | 5 (8) | 11 (9) | 4 (13) | p = 0.98 |
| Nurses | 69 (44) | 27 (41) | 57 (44) | 12 (40) | ||
| Nursing Home Nurse | 8 (5) | 3 (5) | 5 (4) | 3 (10) | ||
| Nurse’s Assistant | 13 (8) | 3 (5) | 8 (6) | 5 (17) | ||
| Medical-Technical Assistant | 54 (34) | 27 (41) | 48 (37) | 6 (20) | ||
| Net household income in € | <2000 | 82 (50) | 28 (47) | 65 (55) | 17 (61) | p = 0.84 |
| 2000 to <4000 | 54 (33) | 27 (45) | 45 (38) | 9 (32) | ||
| ≥4000 | 10 (7) | 5 (8) | 8 (7) | 2 (7) | ||
| grouped | <2000 | 82 (56) | 28 (47) | 65 (55) | 17 (60) | |
| ≥2000 | 64 (44) | 32 (53) | 53 (45) | 11 (40) | ||
| Variable * | Total | Working | HCV | HBV | |
|---|---|---|---|---|---|
| Healthcare Personnel | 163 (%) | 66 (%) | 132 (%) | 31 (%) | |
| Chronic Hepatitis for | <10 years | 2 (1) | 2 (3) | 5 (4) | - |
| 10–19 years | 32 (22) | 11 (18) | 26 (21) | 3 (12) | |
| 20–29 years | 59 (40) | 25 (42) | 47 (39) | 12 (46) | |
| 30–39 years | 43 (29) | 19 (32) | 34 (28) | 8 (30) | |
| 40–49 years | 12 (8) | 3 (5) | 10 (8) | 3 (12) | |
| Liver Status | Fibrosis | 107 (66) | 52 (80) | 93 (70) | 14 (47) |
| Cirrhosis | 46 (28) | 8 (12) | 33 (25) | 13 (43) | |
| Without Findings | 10 (6) | 6 (8) | 5 (5) | 4 (10) | |
| p = 0.04 * | |||||
| HCC | 8 (5) | 4 (6) | 5 (4) | 3 (10) | |
| LTX | 6 (4) | 2 (3) | 5 (4) | 1 (3) | |
| RWA | <50 | 101 (64) | 56 (86) | 82 (62) | 19 (61) |
| ≥50 | 57 (36) | 9 (14) | 45 (38) | 12 (39) | |
| Interferon Experience | Yes | 98 (64) | 34 (55) | 91 (31) | 7 (39) |
| Therapy | Current | 23 (14) | 13 (20) | 6 (5) | 17 (55) |
| Interferon-free | 21 (13) | 13 (20) | 6 (5) | 16 (48) | |
| completed | 28 (17) | 7 (11) | 28 (21) | - | |
| compatibility | |||||
| good | 43 (88) | 16 (94) | 29 (83) | 16 (100) | |
| moderate | 5 (10) | 1 (6) | 5 (14) | - | |
| bad | 1 (2) | - | 1 (3) | - | |
| Laboratory values | AST a increased | 72 (44) | 28 (42) | 69 (53) | 3 (10) |
| ALT a increased | 73 (45) | 32 (48) | 70 (53) | 3 (10) | |
| GGT b increased | 60 (37) | 22 (33) | 53 (40) | 7 (23) | |
| ALP c increased | 23 (14) | 6 (9) | 20 (15) | 3 (10) | |
| ChE d decreased | 16 (10) | 4 (6) | 15 (11) | 1 (3) | |
| Viremia e | 86 (53) | 21 (32) | 61 (46) | 25 (81) | |
| Body Mass Index | <19 Underweight | 4 (3) | 3 (6) | 4 (3) | - |
| 19 to < 25 Normal | 68 (49) | 31 (56) | 53 (47) | 15 (55) | |
| 25 to < 30 Overweight | 37 (26) | 11 (20) | 30 (27) | 7 (26) | |
| ≥30 Obesity | 31 (22) | 10 (18) | 26 (23) | 5 (19) | |
| Regular Physical Activity | Yes | 52 (32) | 21 (32) | 40 (46) | 12 (40) |
| Smoking | Yes | 26 (16) | 16 (24) | 24 (18) | 2 (7) |
| Mental Stress | Fatigue | 121(74) | 47 (71) | 100 (76) | 21 (68) |
| Depression | 60 (35) | 21 (32) | 50 (39) | 10 (34) | |
| Variable | Total | HCV | HBV | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean ⱡ (95%-CI) | Mean ⱡ (95%-CI) | Mean ⱡ (95%-CI) | ||||||||||
| N | T1 | T2 | T3 | N | T1 | T2 | T3 | N | T1 | T2 | T3 | |
| SF-36 | ||||||||||||
| PHSS #,§ | 160 | 38.4 | 38.8 | 38.2 | 129 | 38.9 | 39.3 | 39.4 | 29 | 36.5 | 37.5 * | 33.2 |
| (36.7–40.1) | (37.2–40.5) | (36.5–39.9) | (36.9–40.9) | (37.3–41.3) | (37.4–41.4) | (33.3–39.6) | (34.3–40.7) | (30.1–36.4) | ||||
| MHSS # | 160 | 40.2 | 44.0 * | 40.4 | 129 | 40.3 | 44.4 * | 40.4 | 29 | 40.8 | 43.2 | 41.7 |
| (38.2–42.2) | (42.0–46.0) | (38.4–42.4) | (38.0–42.6) | (42.1–46.7) | (38.0–42.7) | (36.6–45.0) | (38.9–47.4) | (37.5-45.8) | ||||
| HADS-D | ||||||||||||
| A § | 159 | 11.4 | 12.0 * | 11.6 | 129 | 11.5 | 12.0 * | 11.7 | 30 | 11.1 | 11.8 | 11.2 |
| (11.0–11.8) | (11.6–12.4) | (11.2–12.1) | (11,0–11,9) | (11.6–12.5) | (11.2–12.2) | (10.2–12.0) | (11.0–12.7) | (10.3–12.1) | ||||
| D | 159 | 11.3 | 11.2 | 11.3 | 129 | 11.3 | 11.1 | 11.2 | 29 | 11.2 | 11.4 | 11.4 |
| (11.0–11.6) | (10.9–11.5) | (10.9–11.6) | (10.9–11.6) | (10.7–11.5) | (10.8–11.6) | (10.3–12.1) | (10.5–12.3) | (10.5–12.2) | ||||
| Working | ||||||||||||
| WAI | ||||||||||||
| Score | 66 | 28.7 | 30.5 * | 29.6 | 56 | 28.9 | 30.6 | 29.9 | 10 | 27.3 | 29.7 | 27.3 |
| (26.9–30.5) | (28.7–32.3) | (27.8–31.4) | (26.9–30.9) | (28.6–32.6) | (27.9–32.0) | (23.2–31.4) | (25.3–34.1) | (22.8–31.8) | ||||
| Single Item | 66 | 6.0 | 6.6 * | 6.3 | 56 | 6.0 | 6.6 * | 6.4 | 10 | 6.1 | 6.8 | 5.8 |
| (5.5–6.4) | (6.2–7.1) | (5.8–6.7) | (5.5–6.5) | (6.1–7.1) | (5.8–6.9) | (4.9–7.3) | (5.5–8.2) | (4.4–7.2) | ||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Westermann, C.; Nienhaus, A.; Treszl, A. Quality of Life and Work Ability among Healthcare Personnel with Chronic Viral Hepatitis. Evaluation of the Inpatient Rehabilitation Program of the Wartenberg Clinic. Int. J. Environ. Res. Public Health 2019, 16, 3874. https://doi.org/10.3390/ijerph16203874
Westermann C, Nienhaus A, Treszl A. Quality of Life and Work Ability among Healthcare Personnel with Chronic Viral Hepatitis. Evaluation of the Inpatient Rehabilitation Program of the Wartenberg Clinic. International Journal of Environmental Research and Public Health. 2019; 16(20):3874. https://doi.org/10.3390/ijerph16203874
Chicago/Turabian StyleWestermann, Claudia, Albert Nienhaus, and András Treszl. 2019. "Quality of Life and Work Ability among Healthcare Personnel with Chronic Viral Hepatitis. Evaluation of the Inpatient Rehabilitation Program of the Wartenberg Clinic" International Journal of Environmental Research and Public Health 16, no. 20: 3874. https://doi.org/10.3390/ijerph16203874