Effects of Socioeconomic Status on Physical and Psychological Health: Lifestyle as a Mediator

Abstract
:1. Introduction
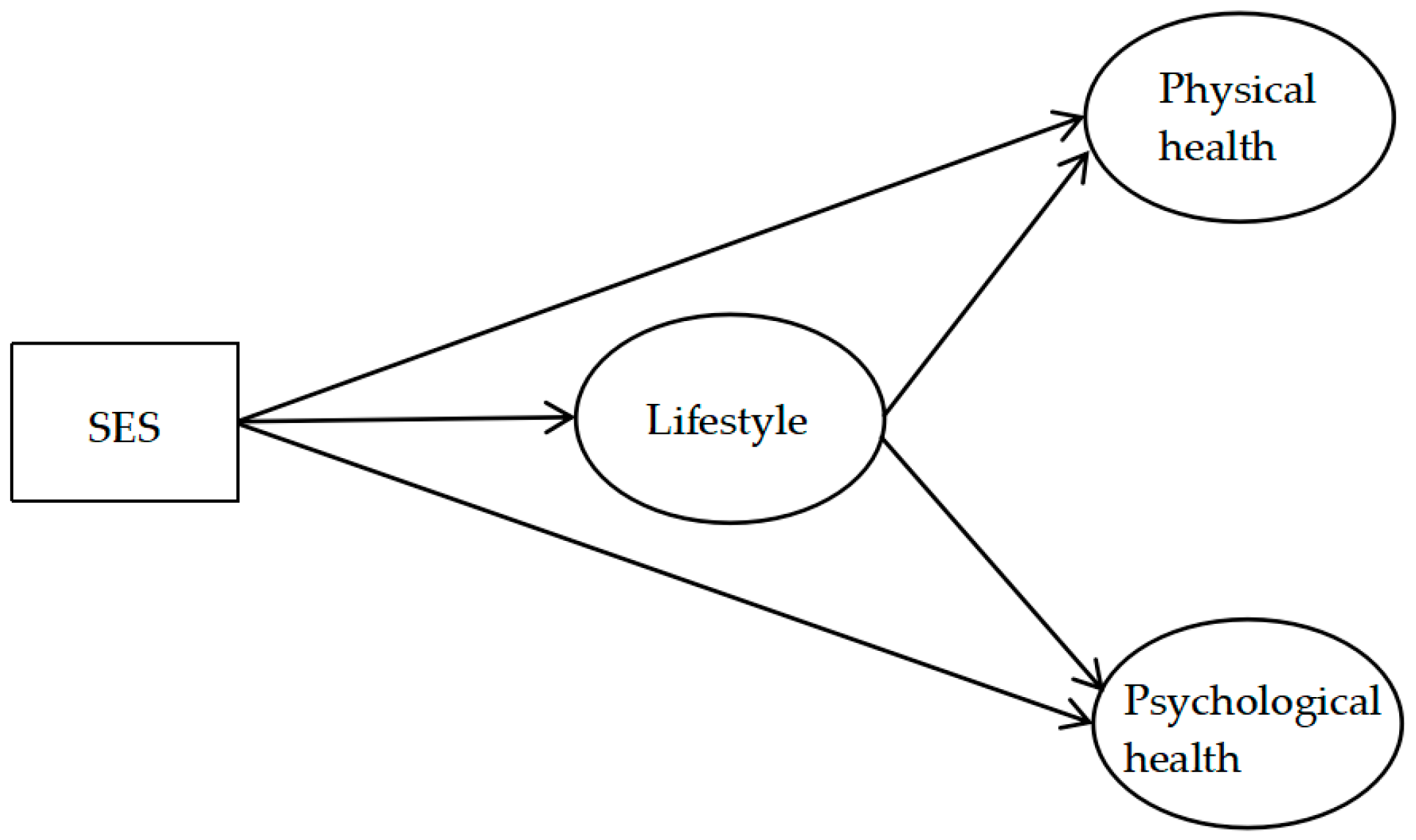
- H1a: People with higher SES are in better physical health.
- H1b: People with higher SES are in better psychological health.
- H2a: People with a healthier lifestyle are in better physical health.
- H2b: People with a healthier lifestyle are in better psychological health.
- H3a: Lifestyle mediates the relationship between SES and physical health.
- H3b: Lifestyle mediates the relationship between SES and psychological health.
2. Materials and Methods
2.1. Sample
2.2. Variables and Instruments
2.3. Statistical Analysis
3. Results
3.1. Preliminary Analysis
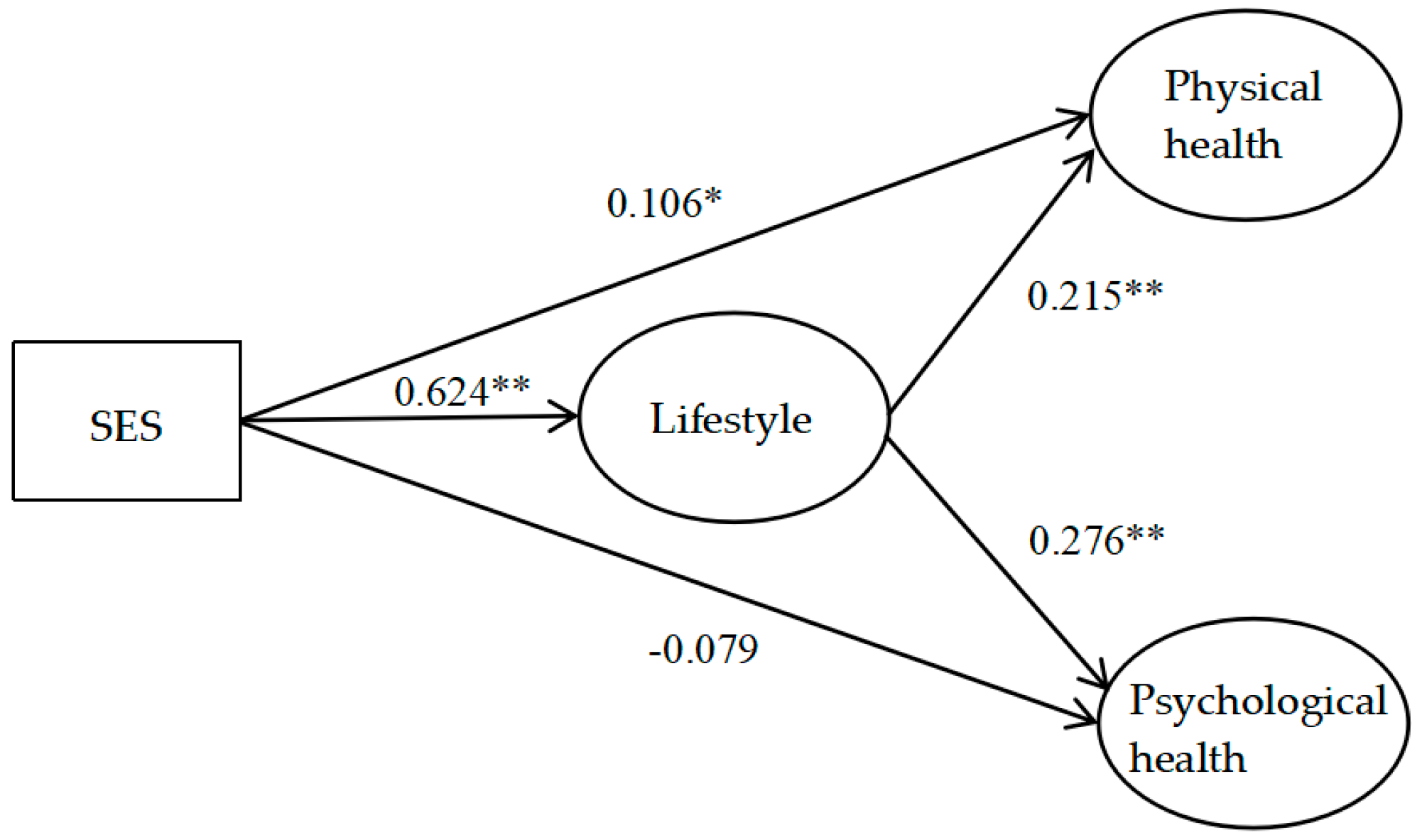
3.2. Testing the Study Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lutfey, K.; Freese, J. Toward some fundamentals of fundamental causality: Socioeconomic status and health in the routine clinic visit for diabetes. Am. J. Sociol. 2005, 110, 1326–1372. [Google Scholar] [CrossRef]
- Smith, G.D.; Bartley, M.; Blane, D. The black report on socioeconomic inequalities in health 10 years on. Br. Med. J. 1990, 301, 373–377. [Google Scholar] [CrossRef]
- Harper, S.; Lynch, J. Trends in socioeconomic inequalities in adult health behaviors among US States, 1990–2004. Public Health Rep. 2007, 122, 177–189. [Google Scholar] [CrossRef] [PubMed]
- Mackenbach, J.P.; Irina, S.; Roskam, A.J.R.; Schaap, M.M.; Gwenn, M.; Mall, L.; Kunst, A.E. Socioeconomic inequalities in health in 22 European countries. N. Engl. J. Med. 2008, 358, 2468–2481. [Google Scholar] [CrossRef] [PubMed]
- Jon Ivar, E.; Steinar, K. Social causation, health-selective mobility, and the reproduction of socioeconomic health inequalities over time: Panel study of adult men. Soc. Sci. Med. 2003, 57, 1475–1489. [Google Scholar] [CrossRef]
- Dahl, E. Social mobility and health: Cause or effect? Br. Med. J. 1996, 313, 435–436. [Google Scholar] [CrossRef]
- West, P. Rethinking the health selection explanation for health inequalities. Soc. Sci. Med. 1991, 32, 373–384. [Google Scholar] [CrossRef]
- Simandan, D. Rethinking the health consequences of social class and social mobility. Soc. Sci. Med. 2018, 200, 258–261. [Google Scholar] [CrossRef]
- Fraser, G.E.; Shavlik, D.J. Ten years of life: Is it a matter of choice? Arch. Intern. Med. 2001, 161, 1645–1652. [Google Scholar] [CrossRef]
- Cockerham, W.C. Health lifestyle theory and the convergence of agency and structure. J. Health Soc. Behav. 2005, 46, 51–67. [Google Scholar] [CrossRef]
- Pronk, N.P.; Anderson, L.H.; Crain, A.L.; Martinson, B.C.; O’Connor, P.J.; Sherwood, N.E.; Whitebird, R.R. Meeting recommendations for multiple healthy lifestyle factors: Prevalence, clustering, and predictors among adolescent, adult, and senior health plan members. Am. J. Prev. Med. 2004, 27, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Morawa, E.; Erim, Y. Health-related lifestyle behavior and religiosity among first-generation immigrants of polish origin in Germany. Int. J. Environ. Res. Public Health 2018, 15, 2545. [Google Scholar] [CrossRef] [PubMed]
- Walker, S.N.; Sechrist, K.R.; Pender, N.J. The health-promoting lifestyle profile: Development and psychometric characteristics. Nurs. Res. 1987, 36, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Mokdad, A.H.; Marks, J.S.; Stroup, D.F.; Gerberding, J.L. Actual causes of death in the United States, 2000. JAMA 2004, 291, 1238–1245. [Google Scholar] [CrossRef] [PubMed]
- Ponthiere, G. Mortality, family and lifestyles. J. Fam. Econ. Issue 2011, 32, 175–190. [Google Scholar] [CrossRef]
- Rohrer, J.E.; Pierce Jr, J.R.; Blackburn, C. Lifestyle and mental health. Prev. Med. 2005, 40, 438–443. [Google Scholar] [CrossRef]
- Lawlor, D.A.; Hopker, S.W. The effectiveness of exercise as an intervention in the management of depression: Systematic review and meta-regression analysis of randomised controlled trials. Br. Med. J. 2001, 322, 763–767. [Google Scholar] [CrossRef]
- Prendergast, K.B.; Schofield, G.M.; Mackay, L.M. Associations between lifestyle behaviours and optimal wellbeing in a diverse sample of New Zealand adults. BMC Public Health 2015, 16, 62. [Google Scholar] [CrossRef]
- Cockerham, W.C.; Abel, T.; Lüschen, G. Max Weber, formal rationality, and health lifestyles. Sociol. Q. 1993, 34, 413–428. [Google Scholar] [CrossRef]
- Cockerham, W.C. Health lifestyles: Bringing structure back. In The New Blackwell Companion to Medical Sociology; Cockerham, W.C., Ed.; Blackwell: Oxford, UK, 2010; pp. 159–183. ISBN 9781405188685. [Google Scholar]
- Contoyannis, P.; Jones, A.M. Socio-economic status, health and lifestyle. J. Health Econ. 2004, 23, 965–995. [Google Scholar] [CrossRef]
- Frohlich, K.L.; Corin, E.; Potvin, L. A theoretical proposal for the relationship between context and disease. Sociol. Health Illn. 2001, 23, 776–797. [Google Scholar] [CrossRef] [Green Version]
- Chinese National Survey Data Archive. Available online: http://cnsda.ruc.edu.cn/ (accessed on 6 October 2018).
- Ganzeboom, H.B.G.; Graaf, P.M.D.; Treiman, D.J. A standard international socio-economic index of occupational status. Soc. Sci. Res. 1992, 21, 1–56. [Google Scholar] [CrossRef] [Green Version]
- Ganzeboom, H.B.G.; Treiman, D.J. Internationally comparable measures of occupational status for the 1988 international standard classification of occupations. Soc. Sci. Res. 1996, 25, 201–239. [Google Scholar] [CrossRef]
- Subramanian, S.V.; Subramanyam, M.A.; Selvaraj, S.; Kawachi, I. Are self-reports of health and morbidities in developing countries misleading? Evidence from India. Soc. Sci. Med. 2009, 68, 260–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Mackenbach, J.P. Socioeconomic inequalities in health in the Netherlands: Impact of a five year research programme. Br. Med. J. 1994, 309, 1487–1491. [Google Scholar] [CrossRef]
- Winkleby, M.A.; Jatulis, D.E.; Frank, E.; Fortmann, S.P. Socioeconomic status and health: How education, income, and occupation contribute to risk factors for cardiovascular disease. Am. J. Public Health 1992, 82, 816–820. [Google Scholar] [CrossRef]
- Adler, N.E.; Boyce, T.; Chesney, M.A.; Cohen, S.; Folkman, S.; Kahn, R.L.; Syme, S.L. Socioeconomic status and health. The challenge of the gradient. Am. Psychol. 1994, 49, 15–24. [Google Scholar] [CrossRef]
- Lorant, V.; Deliège, D.; Eaton, W.; Robert, A.; Philippot, P.; Ansseau, M. Socioeconomic inequalities in depression: A meta-analysis. Am. J. Epidemiol. 2003, 157, 98–112. [Google Scholar] [CrossRef]
- Lorant, V.; Croux, C.S.; Deliege, D.; Mackenbach, J.; Ansseau, M. Depression and socio-economic risk factors: 7-year longitudinal population study. Br. J. Psychiatry 2007, 190, 293–298. [Google Scholar] [CrossRef] [Green Version]
- Martin, L.M.; Ali, S.M.; Maria, R. Socioeconomic status, labour market connection, and self-rated psychological health: The role of social capital and economic stress. Scand. J. Public Health 2012, 40, 51–60. [Google Scholar] [CrossRef]
- Kosidou, K.; Dalman, C.; Lundberg, M.; Hallqvist, J.; Isacsson, G.; Magnusson, C. Socioeconomic status and risk of psychological distress and depression in the Stockholm public health cohort: A population-based study. J. Affect. Disord. 2011, 134, 160–167. [Google Scholar] [CrossRef]
- Johnson, J.G.; Cohen, P.; Dohrenwend, B.P.; Link, B.G.; Brook, J.S. A longitudinal investigation of social causation and social selection processes involved in the association between socioeconomic status and psychiatric disorders. J. Abnorm. Psychol. 1999, 108, 490–499. [Google Scholar] [CrossRef]
- Grzywacz, J.G.; Almeida, D.M.; Neupert, S.D.; Ettner, S.L. Socioeconomic status and health: A micro-level analysis of exposure and vulnerability to daily stressors. J. Health Soc. Behav. 2004, 45, 1–16. [Google Scholar] [CrossRef]
- Galan-Lopez, P.; Ries, F.; Gisladottir, T.; Domínguez, R.; Sánchez-Oliver, A. Healthy lifestyle: Relationship between Mediterranean diet, body composition and physical fitness in 13 to 16-years old Icelandic students. Int. J. Environ. Res. Public Health 2018, 15, 2632. [Google Scholar] [CrossRef]
- Kushner, R.F. Weight loss strategies for treatment of obesity: Lifestyle management and pharmacotherapy. Prog. Cardiovasc. Dis. 2018, 61, 246–252. [Google Scholar] [CrossRef]
- Kurth, T.; Moore, S.C.; Gaziano, J.M.; Kase, C.S.; Stampfer, M.J.; Berger, K.; Buring, J.E. Healthy lifestyle and the risk of stroke in women. Arch. Intern. Med. 2006, 166, 1403–1409. [Google Scholar] [CrossRef]
- Joseph, J.J.; Echouffo-Tcheugui, J.B.; Talegawkar, S.A.; Effoe, V.S.; Okhomina, V.; Carnethon, M.R.; Hsueh, W.A.; Golden, S.H. Modifiable lifestyle risk factors and incident diabetes in African Americans. Am. J. Prev. Med. 2017, 53, e165–e174. [Google Scholar] [CrossRef]
- Ronksley, P.E.; Brien, S.E.; Turner, B.J.; Mukamal, K.J.; Ghali, W.A. Association of alcohol consumption with selected cardiovascular disease outcomes: A systematic review and meta-analysis. Br. Med. J. 2011, 342, d671. [Google Scholar] [CrossRef]
- Martin, L.; Harald, W. The combined effects of healthy lifestyle behaviors on all cause mortality: A systematic review and meta-analysis. Prev. Med. 2012, 55, 163–170. [Google Scholar] [CrossRef]
- Hamer, M.; Stamatakis, E.; Steptoe, A. Dose-response relationship between physical activity and mental health: The Scottish health survey. Br. J. Sports Med. 2009, 43, 1111–1114. [Google Scholar] [CrossRef]
- Teychenne, M.; Ball, K.; Salmon, J. Physical activity and likelihood of depression in adults: A review. Prev. Med. 2008, 46, 397–411. [Google Scholar] [CrossRef]
- Son, Y.J.; Park, C.; Won, M. Impact of physical activity and sleep duration on depressive symptoms in hypertensive patients: Results from a nationally representative Korean sample. Int. J. Environ. Res. Public Health 2018, 15, 2611. [Google Scholar] [CrossRef]
- Boschloo, L.; Reeuwijk, K.G.; Schoevers, R.A.; Penninx, B.W. The impact of lifestyle factors on the 2-year course of depressive and/or anxiety disorders. J. Affect. Disord. 2014, 159, 73–79. [Google Scholar] [CrossRef]
- Haapasalo, V.; de Vries, H.; Vandelanotte, C.; Rosenkranz, R.R.; Duncan, M.J. Cross-sectional associations between multiple lifestyle behaviours and excellent well-being in Australian adults. Prev. Med. 2018, 116, 119–125. [Google Scholar] [CrossRef]
- Lahelma, E. Health and social stratification. In The Blackwell Companion to Medical Sociology; Cockerham, W.C., Ed.; Blackwell: Oxford, UK, 2007; pp. 64–93. ISBN 9780631217039. [Google Scholar]
- Puolakka, E.; Pahkala, K.; Laitinen, T.T.; Magnussen, C.G.; Hutri-Kähönen, N.; Männistö, S.; Pälve, K.S.; Tammelin, T.; Tossavainen, P.; Jokinen, E. Childhood socioeconomic status and lifetime health behaviors: The young Finns study. Int. J. Cardiol. 2018, 258, 289–294. [Google Scholar] [CrossRef]
- Mackenbach, J.P.; Stronks, K. The development of a strategy for tackling health inequalities in the Netherlands. Int. J. Equity Health 2004, 3, 11. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variables | M | SD | SES | Lifestyle | Physical Health | Psychological Health |
|---|---|---|---|---|---|---|
| SES | 34.62 | 15.28 | — | |||
| Lifestyle | 12.77 | 4.80 | 0.56 ** | — | ||
| Physical health | 7.81 | 1.82 | 0.27 ** | 0.29 ** | — | |
| Psychological health | 17.38 | 3.10 | 0.12 ** | 0.21 ** | 0.36 ** | — |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, J.; Geng, L. Effects of Socioeconomic Status on Physical and Psychological Health: Lifestyle as a Mediator. Int. J. Environ. Res. Public Health 2019, 16, 281. https://doi.org/10.3390/ijerph16020281
Wang J, Geng L. Effects of Socioeconomic Status on Physical and Psychological Health: Lifestyle as a Mediator. International Journal of Environmental Research and Public Health. 2019; 16(2):281. https://doi.org/10.3390/ijerph16020281
Chicago/Turabian StyleWang, Jian, and Liuna Geng. 2019. "Effects of Socioeconomic Status on Physical and Psychological Health: Lifestyle as a Mediator" International Journal of Environmental Research and Public Health 16, no. 2: 281. https://doi.org/10.3390/ijerph16020281