Perspectives on Disability and Non-Communicable Diseases in Low- and Middle-Income Countries, with a Focus on Stroke and Dementia


{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
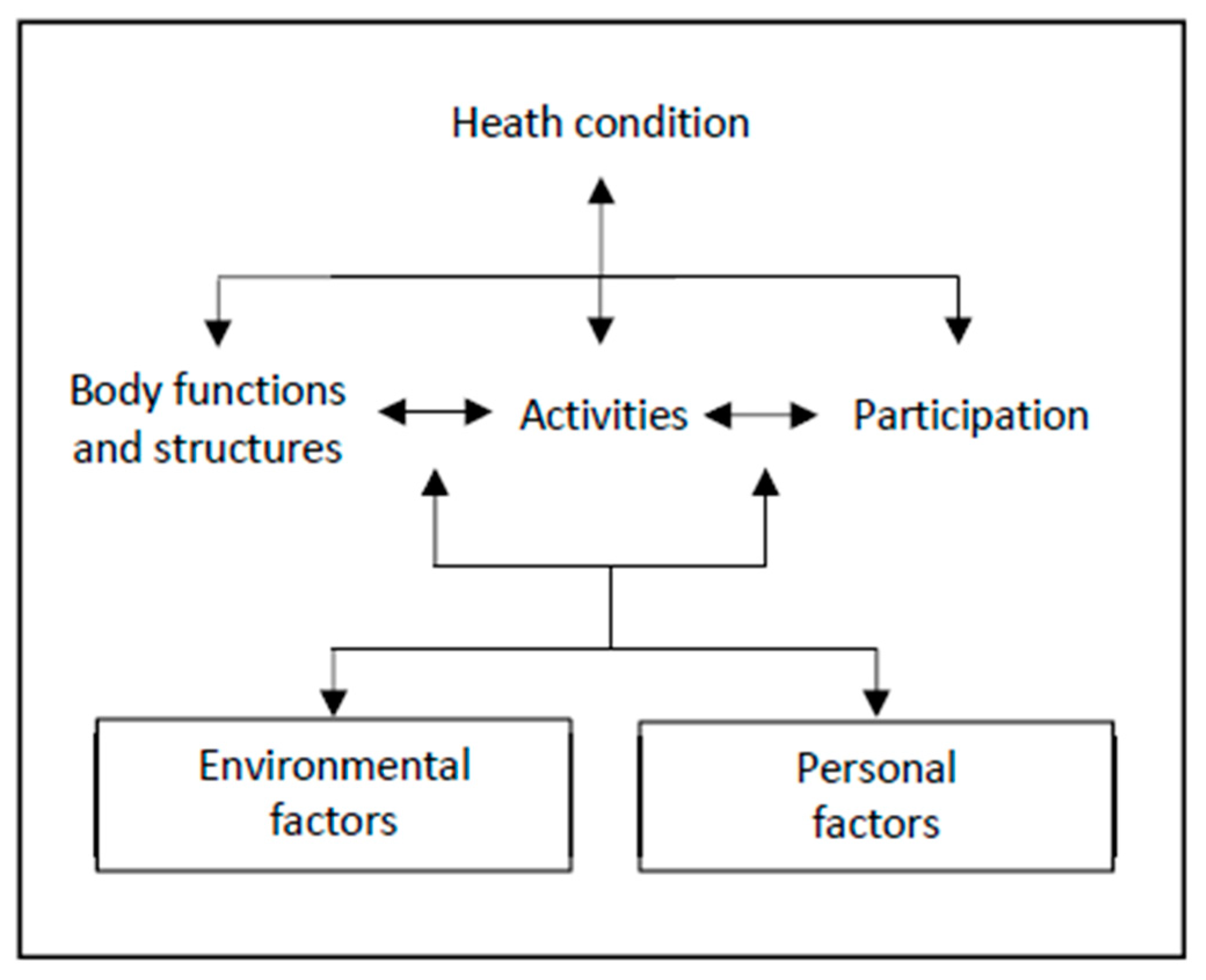
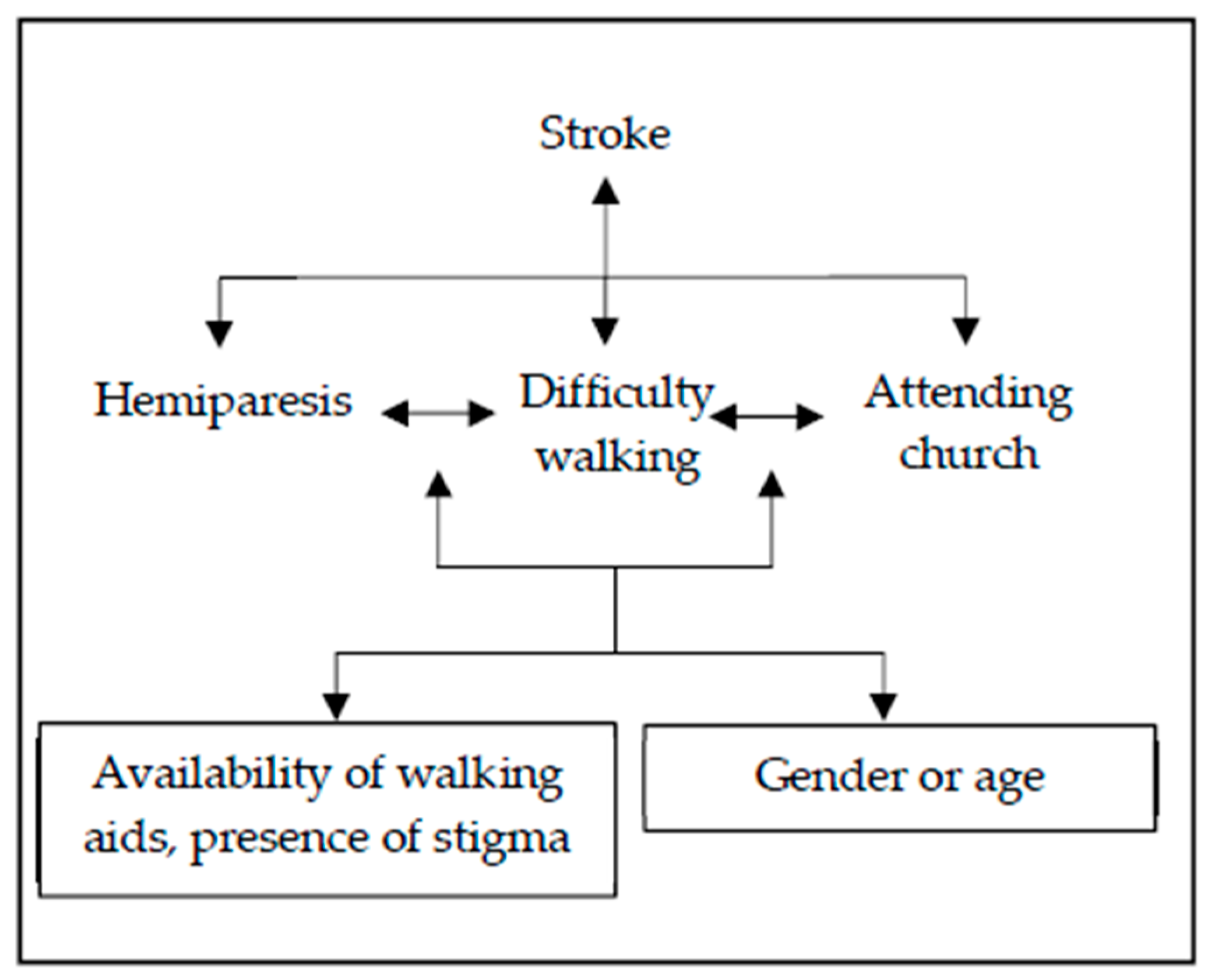
2. What Is Disability?
3. What Is the Association between NCDs and Disability?
3.1. NCDs as a Cause of Disability
3.2. Vulnerability to NCDs among People Living with Disabilities
3.3. Difficulties in Access to Healthcare for People with Disabilities
4. What Should Be Done about the Link between NCDs and Disability?
4.1. Improving Rehabilitation for People with NCD-Related Disabilities
4.2. Improving Access to Healthcare Services for People with Disabilities
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organisation. World Report on Disability; World Health Organisation: Geneva, Switzerland, 2011. [Google Scholar]
- Roth, G.A.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar] [CrossRef]
- World Health Organisation. Global Action Plan for the Prevention and Control of Noncommunicable Diseases; World Health Organisation: Geneva, Switzerland, 2013. [Google Scholar]
- Institute for Health Metrics and Evaluation (IHME). Findings from the Global Burden of Disease Study 2017; Institute for Health Metrics and Evaluation: Seattle, WA, USA, 2018. [Google Scholar]
- World Health Organisation. Global Status Report on Noncommunicable Diseases; World Health Organisation: Geneva, Switzerland, 2014. [Google Scholar]
- Feigin, V.L.; Forouzanfar, M.H.; Krishnamurthi, R.; Mensah, G.A.; Connor, M.; Bennett, D.A.; Moran, A.E.; Sacco, R.L.; Anderson, L.; Truelsen, T.; et al. Global and regional burden of stroke during 1990–2010: Findings from the Global Burden of Disease Study 2010. Lancet 2014, 383, 245–254. [Google Scholar] [CrossRef]
- Feigin, V.L.; Lawes, C.M.M.; Bennett, D.A.; Barker-Collo, S.L.; Parag, V. Worldwide stroke incidence and early case fatality reported in 56 population-based studies: A systematic review. Lancet Neurol. 2009, 8, 355–369. [Google Scholar] [CrossRef]
- Nichols, E.; Szoeke, C.E.I.; Vollset, S.E.; Abbasi, N.; Abd-Allah, F.; Abdela, J.; Aichour, M.T.E.; Akinyemi, R.O.; Alahdab, F.; Asgedom, S.W.; et al. Global, regional, and national burden of Alzheimer’s disease and other dementias, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 88–106. [Google Scholar] [CrossRef]
- Prince, M.; Wimo, A.; Guerchet, M.; Ali, G.-C.; Wu, Y.-T.; Prina, M. World Alzheimer Report: The Global Impact of Dementia, an Analysis of Prevalence, Incidence, Cost and Trends; Alzheimer’s Disease International: London, UK, 2015. [Google Scholar]
- World Health Organisation. How to Use the ICF: A Practical Manual for Using the International Classification of Functioning, Disability and Health (ICF); World Health Organisation: Geneva, Switzerland, 2013. [Google Scholar]
- Badarunisa, M.B.; Sebastian, D.; Rangasayee, R.R.; Kala, B. ICF-Based Analysis of Communication Disorders in Dementia of Alzheimer’s Type. Dement. Geriatr. Cogn. Disord. Extra 2015, 5, 459–469. [Google Scholar] [CrossRef]
- Lisy, K.; Campbell, J.M.; Tufanaru, C.; Moola, S.; Lockwood, C. The prevalence of disability among people with cancer, cardiovascular disease, chronic respiratory disease and/or diabetes: A systematic review. Int. J. Evid.-Based Healthc. 2018, 16, 154–166. [Google Scholar] [CrossRef] [PubMed]
- Basu, S.; King, A.C. Disability and Chronic Disease Among Older Adults in India: Detecting Vulnerable Populations Through the WHO SAGE Study. Am. J. Epidemiol. 2013, 178, 1620–1628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Global Burden of Disease Study 2013 Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 386, 743–800. [Google Scholar]
- World Health Organisation. About Diabetes; World Health Organisation: Geneva, Switzerland, 2019. [Google Scholar]
- Wong, E.; Backholer, K.; Gearon, E.; Harding, J.; Freak-Poli, R.; Stevenson, C.; Peeters, A. Diabetes and risk of physical disability in adults: A systematic review and meta-analysis. Lancet Diabetes Endocrinol. 2013, 1, 106–114. [Google Scholar] [CrossRef]
- Prynn, J.; Dube, A.; Mwaiyeghele, E.; Mwiba, O.; Geis, S.; Koole, O.; Nyirenda, M.; Kuper, H.; Crampin, A. Self-reported disability in rural Malawi: Prevalence, incidence, and relationship to chronic disease [version 1; peer review: Awaiting peer review]. Wellcome Open Res. 2019, 4. [Google Scholar]
- Smith, S.R.; Zheng, J.Y.; Silver, J.; Haig, A.J.; Cheville, A. Cancer rehabilitation as an essential component of quality care and survivorship from an international perspective. Disabil. Rehabil. 2018, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Habtamu, K.; Alem, A.; Medhin, G.; Fekadu, A.; Hanlon, C. Functional impairment among people with severe and enduring mental disorder in rural Ethiopia: A cross-sectional study. Soc. Psychiatry Psychiatr. Epidemiol. 2018, 53, 803–814. [Google Scholar] [CrossRef] [PubMed]
- Ormel, J.; Petukhova, M.; Chatterji, S.; Aguilar-Gaxiola, S.; Alonso, J.; Angermeyer, M.C.; Bromet, E.J.; Burger, H.; Demyttenaere, K.; de Girolamo, G.; et al. Disability and treatment of specific mental and physical disorders across the world. British J. Psychiatry 2008, 192, 368–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, P.; Clark, M. Clinical Medicine, 9th ed.; Elsevier: Amsterdam, The Netherlands, 2017. [Google Scholar]
- Ojagbemi, A.; Akpa, O.; Elugbadebo, F.; Owolabi, M.; Ovbiagele, B. Depression after Stroke in Sub-Saharan Africa: A Systematic Review and Meta-Analysis. Behav. Neurol. 2017, 2017, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kisoli, A.; Gray, W.K.; Dotchin, C.L.; Orega, G.; Dewhurst, F.; Paddick, S.-M.; Longdon, A.; Chaote, P.; Dewhurst, M.; Walker, R.W. Levels of functional disability in elderly people in Tanzania with dementia, stroke and Parkinson’s disease. Acta Neuropsychiatr. 2015, 27, 206–212. [Google Scholar] [CrossRef] [PubMed]
- Kusambiza-Kiingi, A.; Maleka, D.; Ntsiea, V. Stroke survivors’ levels of community reintegration, quality of life, satisfaction with the physiotherapy services and the level of caregiver strain at community health centres within the Johannesburg area. Afr. J. Disabil. 2017, 6, 296. [Google Scholar] [CrossRef] [PubMed]
- Glickman, L.B.; Chimatiro, G. Clients with stroke and non-stroke and their guardians’ views on community reintegration status after in-patient rehabilitation. Malawi Med. J. 2018, 30, 174–179. [Google Scholar] [CrossRef] [PubMed]
- Gadanya, M.A.; Ahmad, R.Y.; Abdullahi, I.; Lawal, I.U. A 24-hour assessment of lifestyle constraint in stroke survivors: A six patient case-based study. Niger. J. Basic Clin. Sci. 2017, 14, 109–112. [Google Scholar]
- Rhoda, A.; Cunningham, N.; Azaria, S.; Urimubenshi, G. Provision of inpatient rehabilitation and challenges experienced with participation post discharge: Quantitative and qualitative inquiry of African stroke patients. BMC Health Serv. Res. 2015, 15, 423. [Google Scholar] [CrossRef]
- Badaru, U.M.; Ogwumike, O.O.; Adeniyi, A.F. Quality of life of Nigerian stroke survivors and its determinants. Afr. J. Biomed. Res. 2015, 18, 1–5. [Google Scholar]
- World Health Organisation. Global Burden of Disease 2004 Update: Disability Weights for Diseases and Conditions; World Health Organisation: Geneva, Switzerland, 2004. [Google Scholar]
- Knopman, D.S.; Petersen, R.C. Mild cognitive impairment and mild dementia: A clinical perspective. Mayo Clin. Proc. 2014, 89, 1452–1459. [Google Scholar] [CrossRef] [PubMed]
- Burgener, S.C.; Buckwalter, K.; Perkhounkova, Y.; Liu, M.F.; Riley, R.; Einhorn, C.J.; Fitzsimmons, S.; Hahn-Swanson, C. Perceived stigma in persons with early-stage dementia: Longitudinal findings: Part 1. Dementia 2013, 14, 589–608. [Google Scholar] [CrossRef] [PubMed]
- Roach, P.; Drummond, N. ‘It’s nice to have something to do’: Early-Onset dementia and maintaining purposeful activity. J. Psychiatr. Ment. Health Nurs. 2014, 21, 889–895. [Google Scholar] [CrossRef] [PubMed]
- Dixon-Ibarra, A.; Horner-Johnson, W. Disability status as an antecedent to chronic conditions: National Health Interview Survey, 2006–2012. Prev. Chronic Dis. 2014, 11, 130251. [Google Scholar] [CrossRef] [PubMed]
- Rasch, E.K.; Magder, L.; Hochberg, M.C.; Magaziner, J.; Altman, B.M. Health of community-dwelling adults with mobility limitations in the united states: incidence of secondary health conditions. Part II. Arch. Phys. Med. Rehabil. 2008, 89, 219–230. [Google Scholar] [CrossRef] [PubMed]
- Banks, L.M.; Kuper, H.; Polack, S. Poverty and disability in low- and middle-income countries: A systematic review. PLoS ONE 2017, 12, e0189996. [Google Scholar] [CrossRef] [PubMed]
- Hashemi, G.; Kuper, H.; Wickenden, M. SDGs, Inclusive Health and the path to Universal Health Coverage. Disabil. Glob. South 2017, 4, 1088–1111. [Google Scholar]
- Marmot, M. Social determinants of health inequalities. Lancet 2005, 365, 1099–1104. [Google Scholar] [CrossRef] [Green Version]
- Ko, K.D.; Lee, K.Y.; Cho, B.; Park, M.S.; Son, K.Y.; Ha, J.H.; Park, S.M. Disparities in health-risk behaviors, preventive health care utilizations, and chronic health conditions for people with disabilities: the korean national health and nutrition examination survey. Arch. Phys. Med. Rehabil. 2011, 92, 1230–1237. [Google Scholar] [CrossRef]
- Froehlich-Grobe, K.; Jones, D.; Businelle, M.S.; Kendzor, D.E.; Balasubramanian, B.A. Impact of disability and chronic conditions on health. Disabil. Health J. 2016, 9, 600–608. [Google Scholar] [CrossRef]
- Australian Institute of Health and Welfare. Health of Australians with Disability: Health Status and Risk Factors; Australian Institute of Health and Welfare: Canberra, Australia, 2010. [Google Scholar]
- Ahlskog, J.E.; Geda, Y.E.; Graff-Radford, N.R.; Petersen, R.C. Physical exercise as a preventive or disease-modifying treatment of dementia and brain aging. Mayo Clin. Proc. 2011, 86, 876–884. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, M.J.; Chin, S.L.; Rangarajan, S.; Xavier, D.; Liu, L.; Zhang, H.; Rao-Melacini, P.; Zhang, X.; Pais, P.; Agapay, S.; et al. Global and regional effects of potentially modifiable risk factors associated with acute stroke in 32 countries (INTERSTROKE): A case-control study. Lancet 2016, 388, 761–775. [Google Scholar] [CrossRef]
- Yusuf, S.; Hawken, S.; Ôunpuu, S.; Dans, T.; Avezum, A.; Lanas, F.; McQueen, M.; Budaj, A.; Pais, P.; Varigos, J.; et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): Case-control study. Lancet 2004, 364, 937–952. [Google Scholar] [CrossRef]
- Hu, F.B.; Sigal, R.J.; Rich-Edwards, J.W.; Colditz, G.A.; Solomon, C.G.; Willett, W.C.; Speizer, F.E.; Manson, J.E. Walking compared with vigorous physical activity and risk of type 2 diabetes in womena prospective study. JAMA 1999, 282, 1433–1439. [Google Scholar] [CrossRef] [PubMed]
- Eide, A.H.; Mannan, H.; Khogali, M.; van Rooy, G.; Swartz, L.; Munthali, A.; Hem, K.-G.; MacLachlan, M.; Dyrstad, K. Perceived Barriers for Accessing Health Services among Individuals with Disability in Four African Countries. PLoS ONE 2015, 10, e0125915. [Google Scholar] [CrossRef] [PubMed]
- Mahmoudi, E.; Meade, M.A. Disparities in access to health care among adults with physical disabilities: Analysis of a representative national sample for a ten-year period. Disabil. Health J. 2015, 8, 182–190. [Google Scholar] [CrossRef] [PubMed]
- Reichard, A.; Stransky, M.; Phillips, K.; McClain, M.; Drum, C. Prevalence and reasons for delaying and foregoing necessary care by the presence and type of disability among working-age adults. Disabil. Health J. 2017, 10, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Floud, S.; Barnes, I.; Verfürden, M.; Kuper, H.; Gathani, T.; Blanks, R.G.; Alison, R.; Patnick, J.; Beral, V.; Green, J.; et al. Disability and participation in breast and bowel cancer screening in England: A large prospective study. Br. J. Cancer 2017, 117, 1711–1714. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, M.; Inagaki, M.; Nakaya, N.; Fujimori, M.; Higuchi, Y.; Hayashibara, C.; So, R.; Kakeda, K.; Kodama, M.; Uchitomi, Y.; et al. Cancer screening participation in schizophrenic outpatients and the influence of their functional disability on the screening rate: A cross-sectional study in Japan. Psychiatry Clin. Neurosci. 2017, 71, 813–825. [Google Scholar] [CrossRef]
- Reichard, A.; Stolzle, H.; Fox, M.H. Health disparities among adults with physical disabilities or cognitive limitations compared to individuals with no disabilities in the United States. Disabil. Health J. 2011, 4, 59–67. [Google Scholar] [CrossRef]
- Park, J.H.; Park, J.H.; Lee, S.Y.; Kim, S.Y.; Shin, Y. Disparities in antihypertensive medication adherence in persons with disabilities and without disabilities: Results of a Korean population-based study. Arch. Phys. Med. Rehabil. 2008, 89, 1460–1467. [Google Scholar] [CrossRef] [PubMed]
- Levesque, J.-F.; Harris, M.F.; Russell, G. Patient-centred access to health care: Conceptualising access at the interface of health systems and populations. Int. J. Equity Health 2013, 12, 18. [Google Scholar] [CrossRef] [PubMed]
- Rotarou, E.S.; Sakellariou, D. Inequalities in access to health care for people with disabilities in Chile: The limits of universal health coverage. Crit. Public Health 2017, 27, 604–616. [Google Scholar] [CrossRef]
- Vergunst, R.; Swartz, L.; Mji, G.; MacLachlan, M.; Mannan, H. You must carry your wheelchair—Barriers to accessing healthcare in a South African rural area. Glob. Health Action 2015, 8, 29003. [Google Scholar] [CrossRef] [PubMed]
- Van Hees, S.; Cornielje, H.; Wagle, P.; Veldman, E. Disability Inclusion in Primary Health Care in Nepal: An Explorative Study of Perceived Barriers to Access Governmental Health Services. Disabil. CBR Incl. Dev. 2014, 25, 99–118. [Google Scholar] [CrossRef]
- Gudlavalleti, S.V. Challenges in Accessing Health Care for People with Disability in the South. Asian Context: A Review. Int. J. Environ. Res. Public Health 2018, 15, 2366. [Google Scholar] [CrossRef] [PubMed]
- Brinda, E.M.; Andrés, R.A.; Enemark, U. Correlates of out-of-pocket and catastrophic health expenditures in Tanzania: Results from a national household survey. BMC Int. Health Hum. Rights 2014, 14, 5. [Google Scholar]
- Somkotra, T.; Lagrada, L.P. Which households are at risk of catastrophic health spending: experience in thailand after universal coverage. Health Aff. 2009, 28, 467–478. [Google Scholar] [CrossRef]
- Yardim, M.S.; Cilingiroglu, N.; Yardim, N. Catastrophic health expenditure and impoverishment in Turkey. Health Policy 2010, 94, 26–33. [Google Scholar] [CrossRef]
- Mulumba, M.; Nantaba, J.; Brolan, C.E.; Ruano, A.L.; Brooker, K.; Hammonds, R. Perceptions and experiences of access to public healthcare by people with disabilities and older people in Uganda. Int. J. Equity Health 2014, 13, 76. [Google Scholar] [CrossRef]
- Cawood, J.; Visagie, S. Environmental factors influencing participation of stroke survivors in a Western Cape setting. Afr. J. Disabil. 2015, 4, 198. [Google Scholar] [CrossRef] [PubMed]
- Bunn, F.; Burn, A.-M.; Goodman, C.; Rait, G.; Norton, S.; Robinson, L.; Schoeman, J.; Brayne, C. Comorbidity and dementia: A scoping review of the literature. BMC Med. 2014, 12, 192. [Google Scholar] [CrossRef] [PubMed]
- Bunn, F.; Burn, A.-M.; Robinson, L.; Poole, M.; Rait, G.; Brayne, C.; Schoeman, J.; Norton, S.; Goodman, C. Healthcare organisation and delivery for people with dementia and comorbidity: A qualitative study exploring the views of patients, carers and professionals. BMJ Open 2017, 7, e013067. [Google Scholar] [CrossRef] [PubMed]
- Richards, N.C.; Gouda, H.N.; Durham, J.; Rampatige, R.; Rodney, A.; Whittaker, M. Disability, noncommunicable disease and health information. Bull. World Health Organ. 2016, 94, 230–232. [Google Scholar] [CrossRef]
- World Health Organisation. Rehabilitation 2030: A Call for Action; World Health Organisation: Geneva, Switzerland, 2017. [Google Scholar]
- National Institute for Health and Care Excellence. Stroke Rehabilitation in Adults; National Institute for Health and Care Excellence: London, UK, 2013. [Google Scholar]
- Clare, L. Rehabilitation for people living with dementia: A practical framework of positive support. PLoS Med. 2017, 14, e1002245. [Google Scholar] [CrossRef] [PubMed]
- Pollock, A.; Baer, G.; Campbell, P.; Choo, P.L.; Forster, A.; Morris, J.; Pomeroy, V.M.; Langhorne, P. Physical rehabilitation approaches for the recovery of function and mobility following stroke. Cochrane Database Syst. Rev. 2014, 4. [Google Scholar] [CrossRef]
- Knox, M.; Stewart, A.; Richards, C.L. Six hours of task-orientated training optimizes walking competency post stroke: A randomized controlled trial in the public health-care system of South Africa. Clin. Rehabil. 2018, 32, 1057–1068. [Google Scholar] [CrossRef]
- Bahar-Fuchs, A.; Clare, L.; Woods, B. Cognitive training and cognitive rehabilitation for mild to moderate Alzheimer’s disease and vascular dementia. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef]
- Kamenov, K.; Mills, J.-A.; Chatterji, S.; Cieza, A. Needs and unmet needs for rehabilitation services: A scoping review. Disabil. Rehabil. 2019, 41, 1227–1237. [Google Scholar] [CrossRef]
- Liu, H.; Lindley, R.; Alim, M.; Felix, C.; Gandhi, D.B.; Verma, S.J.; Tugnawat, D.K.; Syrigapu, A.; Ramamurthy, R.K.; Pandian, J.D.; et al. Family-led rehabilitation in India (ATTEND)-Findings from the process evaluation of a randomized controlled trial. Int. J. Stroke 2019, 14, 53–60. [Google Scholar] [CrossRef]
- Sureshkumar, K.; Murthy, G.V.S.; Natarajan, S.; Naveen, C.; Goenka, S.; Kuper, H. Evaluation of the feasibility and acceptability of the ‘Care for Stroke’ intervention in India, a smartphone-enabled, carer-supported, educational intervention for management of disability following stroke. BMJ Open 2016, 6, e009243. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. Community-Based Rehabilitation: CBR Guidelines; World Health Organisation: Geneva, Switzerland, 2010. [Google Scholar]
- Rubin, S.E.; Roessler, R.T. Foundations of the Vocational Rehabilitation Process, 5th ed.; PRO-ED: Austin, TX, USA, 2001. [Google Scholar]
- Ntsiea, M.V.; Van Aswegen, H.; Lord, S.; Olorunju, S.S. The effect of a workplace intervention programme on return to work after stroke: A randomised controlled trial. Clin. Rehabil. 2015, 29, 663–673. [Google Scholar] [CrossRef] [PubMed]
- Iemmi, V.; Gibson, L.; Blanchet, K.; Kumar, K.S.; Rath, S.; Hartley, S.; Murthy, G.V.S.; Patel, V.; Weber, J.; Kuper, H. Community-based rehabilitation for people with disabilties in low- and middle-income countries: A systematic review. Campbell Syst. Rev. 2015, 15. [Google Scholar] [CrossRef]
- UN. Convention on the Rights of Persons with Disabilities; United Nations: New York, NY, USA, 2006. [Google Scholar]
- Tsolekile, L.P.; Puoane, T.; Schneider, H.; Levitt, N.S.; Steyn, K. The roles of community health workers in management of non-communicable diseases in an urban township. Afr. J. Prim. Health Care Fam. Med. 2014, 6, E1–E8. [Google Scholar] [CrossRef] [PubMed]
- Mishra, S.R.; Neupane, D.; Preen, D.; Kallestrup, P.; Perry, H.B. Mitigation of non-communicable diseases in developing countries with community health workers. Glob. Health 2015, 11, 43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neupane, D.; Kallestrup, P.; McLachlan, C.S.; Perry, H. Community health workers for non-communicable diseases. Lancet Glob. Health 2014, 2, e567. [Google Scholar] [CrossRef]
- Jeet, G.; Thakur, J.; Prinja, S.; Singh, M. Community health workers for non-communicable diseases prevention and control in developing countries: Evidence and implications. PLoS ONE 2017, 12, e0180640. [Google Scholar] [CrossRef]
- Pregel, A.; Vaughan Gough, T.; Jolley, E.; Buttan, S.; Bhambal, A. Ensuring universal access to eye health in urban slums in the Global South: The case of Bhopal (India). Stud. Health Technol. Inform. 2016, 229, 302–313. [Google Scholar]



© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prynn, J.E.; Kuper, H. Perspectives on Disability and Non-Communicable Diseases in Low- and Middle-Income Countries, with a Focus on Stroke and Dementia. Int. J. Environ. Res. Public Health 2019, 16, 3488. https://doi.org/10.3390/ijerph16183488
Prynn JE, Kuper H. Perspectives on Disability and Non-Communicable Diseases in Low- and Middle-Income Countries, with a Focus on Stroke and Dementia. International Journal of Environmental Research and Public Health. 2019; 16(18):3488. https://doi.org/10.3390/ijerph16183488
Chicago/Turabian StylePrynn, Josephine E., and Hannah Kuper. 2019. "Perspectives on Disability and Non-Communicable Diseases in Low- and Middle-Income Countries, with a Focus on Stroke and Dementia" International Journal of Environmental Research and Public Health 16, no. 18: 3488. https://doi.org/10.3390/ijerph16183488