Dose Tapering Strategy for Heroin Abstinence among Methadone Maintenance Treatment Participants: Evidence from A Retrospective Study in Guangdong, China

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting
2.2. Data Collection
2.3. Definitions
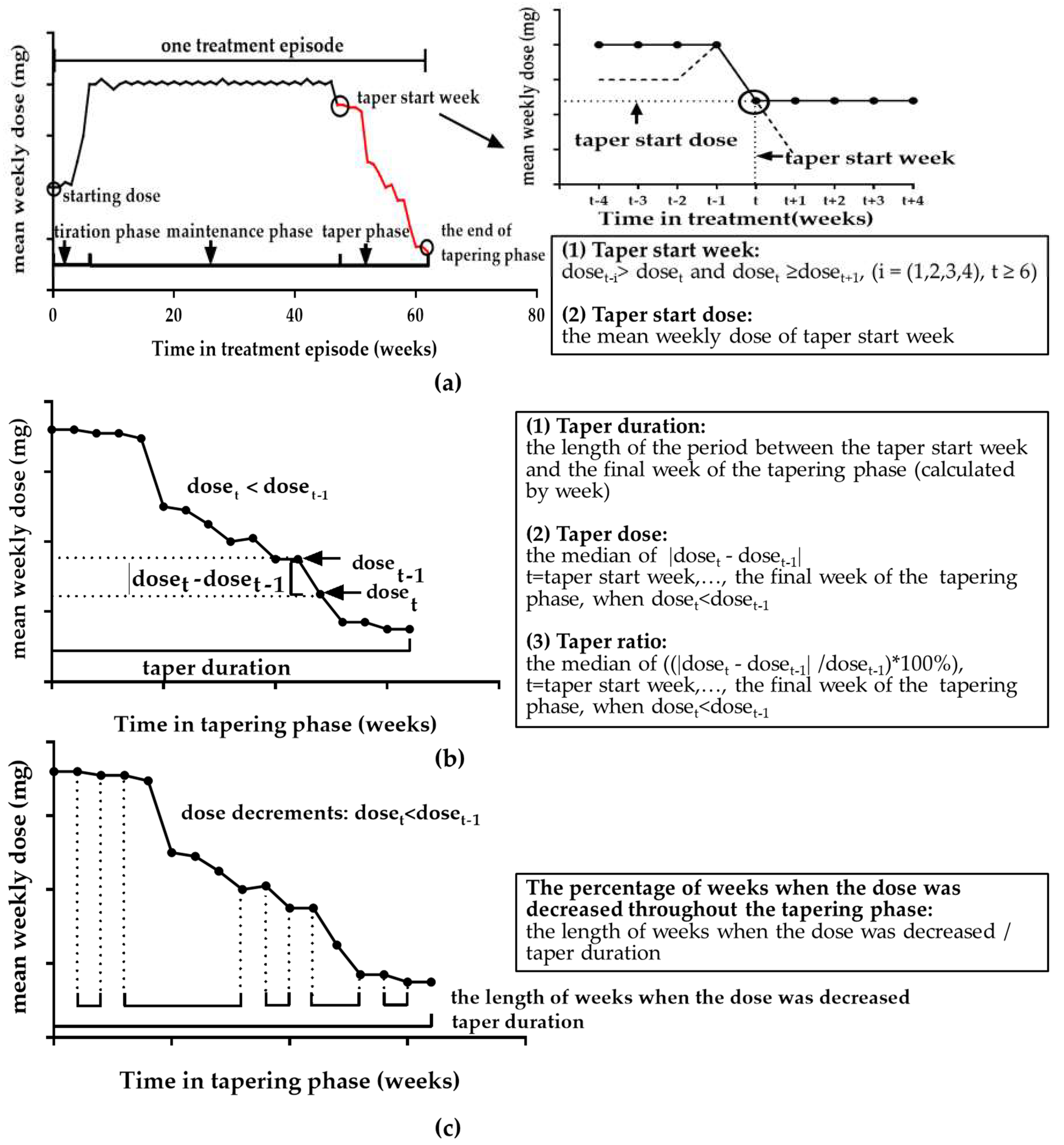
2.3.1. Treatment Episode
2.3.2. Tapering Phase Characteristics
2.4. Study Subjects
2.5. Measures
2.5.1. Dependent Variable
2.5.2. Independent Variables
2.6. Statistical Analysis
2.7. Ethical Statement
3. Results
3.1. Demographic Characteristics, Drug Use Behaviors and HIV/HCV Infection Status
3.2. Characteristics of Treatment Episode Which Contained a Tapering Phase
3.3. Association between Tapering Phase Characteristics and Heroin Abstinence
3.4. Subgroup Analyzes
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- United Nations Office on Drugs and Crime. World Drug Report 2018. United Nations Office on Drugs and Crime. 2018. Available online: http://www.unodc.org/wdr2018/ (accessed on 8 April 2019).
- Ali, N.; Aziz, S.A.; Nordin, S.; Mi, N.C.; Abdullah, N.; Paranthaman, V.; Mahmud, M.; Yee, A.; Danaee, M. Evaluation of Methadone Treatment in Malaysia: Findings from the Malaysian Methadone Treatment Outcome Study (Mytos). Subst. Use Misuse 2018, 53, 239–248. [Google Scholar] [CrossRef] [PubMed]
- Marienfeld, C.; Liu, P.; Wang, X.; Schottenfeld, R.; Zhou, W.; Chawarski, M.C. Evaluation of an Implementation of Methadone Maintenance Treatment in China. Drug Alcohol Depend. 2015, 157, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Amato, L.; Davoli, M.; Perucci, C.A.; Ferri, M.; Faggiano, F.; Mattick, R.P. An Overview of Systematic Reviews of the Effectiveness of Opiate Maintenance Therapies: Available Evidence to Inform Clinical Practice and Research. J. Subst. Abuse Treat. 2005, 28, 321–329. [Google Scholar] [CrossRef] [PubMed]
- Calsyn, D.A.; Malcy, J.A.; Saxon, A.J. Slow Tapering from Methadone Maintenance in a Program Encouraging Indefinite Maintenance. J. Subst. Abuse Treat. 2006, 30, 159–163. [Google Scholar] [CrossRef] [PubMed]
- Center for Substance Abuse, Treatment. Samhsa/Csat Treatment Improvement Protocols. In Medication-Assisted Treatment for Opioid Addiction in Opioid Treatment Programs; Substance Abuse and Mental Health Services Administration: Rockville, MD, USA, 2005. [Google Scholar]
- Nosyk, B.; Marsh, D.C.; Sun, H.; Schechter, M.T.; Anis, A.H. Trends in Methadone Maintenance Treatment Participation, Retention, and Compliance to Dosing Guidelines in British Columbia, Canada: 1996–2006. J. Subst. Abuse Treat. 2010, 39, 22–31. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Chen, W. Dosage Using in Community Methadone Maintenance Treatment at Clinics in Guangdong and Its Adjustment Strategy. Modern Prev. Med. 2010, 37, 1687–1689. [Google Scholar]
- Volkow, N.D.; Frieden, T.R.; Hyde, P.S.; Cha, S.S. Medication-Assisted Therapies--Tackling the Opioid-Overdose Epidemic. N. Engl. J. Med. 2014, 370, 2063–2066. [Google Scholar] [CrossRef]
- Health Canada. Best Practices-Methadone Maintenance Treatment; Health Canada: Ottawa, ON, Canada, 2002; ISBN 0-662-31812-9. [Google Scholar]
- Nguyen, T.T.; Luong, A.N.; Nham, T.T.T.; Chauvin, C.; Feelemyer, J.; Nagot, N.; Jarlais, D.D.; Le, M.G.; Jauffret-Roustide, M. Struggling to Achieve a ‘Normal Life’: A Qualitative Study of Vietnamese Methadone Patients. Int. J. Drug Policy 2019, 68, 18–26. [Google Scholar] [CrossRef]
- Lowinson, J.; Berle, B.; Langrod, J. Detoxification of Long-Term Methadone Patients: Problems and Prospects. Int. J. Addict. 1976, 11, 1009–1018. [Google Scholar] [CrossRef]
- Senay, E.C.; Dorus, W.; Goldberg, F.; Thornton, W. Withdrawal from Methadone Maintenance: Rate of Withdrawal and Expectation. Arch. Gen. Psychiatry 1977, 34, 361–367. [Google Scholar] [CrossRef]
- Eklund, C.; Hiltunen, A.J.; Melin, L.; Borg, S. Factors Associated with Successful Withdrawal from Methadone Maintenance Treatment in Sweden. Subst. Use Misuse 1995, 30, 1335–1353. [Google Scholar] [CrossRef]
- Department of Health, Ministry of Health. Guideline on Methadone Therapy and Treatment of Drug Dependence in Myanmar; Department of Health, Ministry of Health: Nay Pyi Taw, Myanmar, 2012. [Google Scholar]
- Public Health England. Drug Misuse and Dependence: UK Guidelines on Clinical Management; Department of Health: London, UK, 2017. [Google Scholar]
- Cushman, P.; Dole, V.P. Detoxification of Rehabilitated Methadone-Maintained Patients. JAMA J. Am. Med Assoc. 1973, 226, 747–752. [Google Scholar] [CrossRef]
- Nosyk, B.; Sun, H.; Evans, E.; Marsh, D.C.; Anglin, M.D.; Hser, Y.I.; Anis, A.H. Defining Dosing Pattern Characteristics of Successful Tapers Following Methadone Maintenance Treatment: Results from a Population-Based Retrospective Cohort Study. Addiction 2012, 107, 1621–1629. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, S.G.; Wu, Z.; Rou, K.; Pang, L.; Luo, W.; Wang, C.; Cao, X.; Yin, W.; Liu, E.; Mi, G. Who Uses Methadone Services in China? Monitoring the World’s Largest Methadone Program. Addiction 2015, 110 (Suppl. 1), 29–39. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.; Zhao, M. Meeting the Challenges of Opioid Dependence in China: Experience of Opioid Agonist Treatment. Curr. Opin. Psychiatry 2019, 32, 282–287. [Google Scholar] [CrossRef] [PubMed]
- Deng, S.; Weng, S. Investigation Report About the Trend Change of Drug Addicts in Guangdong Province. Justice China 2017, 85–91. [Google Scholar] [CrossRef]
- Food and Drug Administration of China. Guidelines on the Management of Methadone Maintenance Treatment in China; CFDA: Beijing, China, 2015. [Google Scholar]
- Cushman, P., Jr. Detoxification after Methadone Maintenance Treatment. Ann. N. Y. Acad. Sci. 1981, 362, 217–230. [Google Scholar] [CrossRef] [PubMed]
- Reid, G.; Sharma, M.; Higgs, P. The Long Winding Road of Opioid Substitution Therapy Implementation in South-East Asia: Challenges to Scale Up. J. Public Health Res. 2014, 3, 204. [Google Scholar] [CrossRef] [PubMed]
- Dhawan, A.; Rao, R.; Ambekar, A.; Chopra, A.; Jain, R.; Yadav, D.; Ray, R. Methadone Maintenance Treatment in India (a Feasibility and Effectiveness Report); UNODC (ROSA) and NDDTC (AIIMS): New Delhi, India, 2014. [Google Scholar]
- Hser, Y.I.; Evans, E.; Huang, D.; Anglin, D.M. Relationship between Drug Treatment Services, Retention, and Outcomes. Psychiatr. Serv. 2004, 55, 767–774. [Google Scholar] [CrossRef]
- Fareed, A.; Casarella, J.; Amar, R.; Vayalapalli, S.; Drexler, K. Benefits of Retention in Methadone Maintenance and Chronic Medical Conditions as Risk Factors for Premature Death among Older Heroin Addicts. J. Psychiatr. Pract. 2009, 15, 227–234. [Google Scholar] [CrossRef]
- Zhou, K.; Zhuang, G. Retention in Methadone Maintenance Treatment in Mainland China, 2004-2012: A Literature Review. Addict. Behav. 2014, 39, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Amato, L.; Davoli, M.; Minozzi, S.; Ali, R.; Ferri, M. Methadone at Tapered Doses for the Management of Opioid Withdrawal. Cochrane Database Syst. Rev. (Online) 2005, 28. [Google Scholar] [CrossRef]
- Magura, S.; Rosenblum, A. Leaving Methadone Treatment: Lessons Learned, Lessons Forgotten, Lessons Ignored. Mount Sinai J. Med. 2001, 68, 62–74. [Google Scholar]
- Luo, X.; Zhao, P.; Gong, X.; Zhang, L.; Tang, W.; Zou, X.; Chen, W.; Ling, L. Concurrent Heroin Use and Correlates among Methadone Maintenance Treatment Clients: A 12-Month Follow-up Study in Guangdong Province, China. Int. J. Environ. Res. Public Health 2016, 13. [Google Scholar] [CrossRef] [PubMed]
- Oppenheimer, E.; Stimson, G.V.; Thorley, A. Seven-Year Follow-up of Heroin Addicts: Abstinence and Continued Use Compared. Br. Med. J. 1979, 2, 627–630. [Google Scholar] [CrossRef]
- Capone, C.T.; Haggerty, E.L.; Acer, K.; Melchionda, R.; Holley, E.; Adams, H.; Logan, F. Client Variables Associated with Selection and Outcome in a Methadone Tapering Program. Subst. Use Misuse 1994, 29, 387–394. [Google Scholar] [CrossRef]
- WHO. Guidelines for the Psychosocially Assisted Pharmacological Treatment of Opioid Dependence; WHO: Geneva, Switzerland, 2009. [Google Scholar]
- Richardson, L.; Wood, E.; Montaner, J.; Kerr, T. Addiction treatment-related employment barriers: The impact of methadone maintenance. J. Subst. Abus. Treat. 2012, 43, 276–284. [Google Scholar] [CrossRef] [Green Version]
- Nong, V.M.; Boggiano, V.L.; Nguyen, L.H.T.; Nguyen, C.T.; Nguyen, L.H.; Bach, T.X.; Nguyen, H.V.; Hoang, C.D.; Latkin, C.A.; Vu, M.T.T. Ability to join the workforce and work productivity among drug users under methadone maintenance treatment in a mountainous area of Northern Vietnam: A cross-sectional study. BMJ Open 2017, 7, e016153. [Google Scholar] [CrossRef]
- Wang, R.; Ding, Y.; Bai, H.; Duan, S.; Ye, R.; Yang, Y.; Wang, J.; Tang, R.; Gao, M.; He, N. Illicit Heroin and Methamphetamine Use among Methadone Maintenance Treatment Patients in Dehong Prefecture of Yunnan Province, China. PLoS ONE 2015, 10, e0133431. [Google Scholar] [CrossRef]


{kind=link}
| Variables | No. (%) | cOR (95% CI) |
|---|---|---|
| Demographic characteristics | ||
| Gender | ||
| male | 773 (90.6) | ref. |
| female | 80 (9.4) | 0.95 (0.61–1.48) |
| Age, mean ± SD | 37.2 ± 6.72 | 1.00 (0.98–1.02) |
| Marital status | ||
| married | 367 (43.0) | ref. |
| single/divorced/widowed | 486 (57.0) | 0.88 (0.68–1.15) |
| Education | ||
| primary school or below | 138 (16.2) | ref. |
| middle school | 559 (65.5) | 1.03 (0.72–1.48) |
| high school or above | 156 (18.3) | 0.77 (0.49–1.20) |
| Employment status | ||
| unemployed | 649 (76.1) | ref. |
| employed | 204 (23.9) | 1.24 (0.91–1.68) * |
| Drug use behaviors | ||
| Age at initial drug use, mean ± SD | 23.8 ± 6.05 | 1.00 (0.97–1.02) |
| Intravenous drug use before enrolment in MMT | ||
| no | 89 (10.4) | ref. |
| yes | 764 (89.6) | 0.86 (0.56–1.30) |
| Years of drug abuse before enrolment in MMT | ||
| <5 | 53 (6.2) | 1.37 (0.75–2.51) |
| 5–9 | 131 (15.4) | 1.49 (1.01–2.20) ** |
| ≥10 | 669 (78.4) | ref. |
| Infection status | ||
| HIV-infected | ||
| no | 781 (91.6) | ref. |
| yes | 60 (7.0) | 0.66 (0.39–1.14) |
| missing information | 12 (1.4) | - |
| HCV-infected | ||
| no | 160 (18.8) | ref. |
| yes | 676 (79.2) | 0.86 (0.62–1.19) |
| missing information | 17 (2.0) | - |
| No. of treatment episode, median (IQR) | 1 (1,1) | |
| Variables | Urine Test Negative (N = 419) | Urine Test Positive (N = 542) | Total(N = 961) | cOR (95% CI) |
|---|---|---|---|---|
| No. (%) | No. (%) | No. (%) | ||
| Adherence to MMT | ||||
| Treatment attendance (%) | ||||
| <50 | 12 (2.9) | 27 (5.0) | 39 (4.1) | ref. |
| 50–80 | 87 (20.8) | 135 (24.9) | 222 (23.1) | 1.45 (0.69–3.05) |
| >80 | 320 (76.4) | 380 (70.1) | 700 (72.8) | 1.90 (0.94–3.85) * |
| Characteristics of the whole treatment episode | ||||
| Duration of treatment episode (years), mean ± SD | 1.8 ± 1.13 | 2.8 ± 1.97 | 2.3 ± 1.72 | 0.65 (0.59–0.72) *** |
| % change in dose throughout the treatment episode per week (%) | ||||
| <1 | 320 (76.4) | 459 (84.7) | 779 (81.0) | ref. |
| 1–4 | 40 (9.5) | 49 (9.0) | 89 (9.3) | 1.18 (0.75–1.84) |
| >4 | 59 (14.1) | 34 (6.3) | 93 (9.7) | 2.51 (1.59–3.95) *** |
| Tapering phase characteristics | ||||
| Taper start week | ||||
| <16 | 215 (51.3) | 279 (51.5) | 494 (51.4) | ref. |
| 16–52 | 161 (38.4) | 218 (40.2) | 379 (39.4) | 0.96 (0.73–1.26) |
| >52 | 43 (10.3) | 45 (8.3) | 88 (9.2) | 1.24 (0.78–1.97) |
| Taper start dose (mg) | ||||
| <60 | 304 (72.6) | 329 (60.7) | 633 (65.9) | 1.76 (1.32–2.34) *** |
| 60–120 | 108 (25.8) | 206 (38.0) | 314 (32.7) | ref. |
| >120 | 7 (1.7) | 7 (1.3) | 14 (1.5) | 1.90 (0.64–5.64) |
| Taper duration (weeks) | ||||
| <13 | 109 (26.0) | 54 (10.0) | 163 (17.0) | 5.24 (3.53–7.80) *** |
| 13–25 | 97 (23.2) | 75 (13.8) | 172 (17.9) | 3.35 (2.30–4.88) *** |
| 26–52 | 94 (22.4) | 106 (19.6) | 200 (20.8) | 2.31 (1.62–3.30) *** |
| >52 | 119 (28.4) | 307 (56.6) | 426 (44.3) | ref. |
| Taper dose (mg/week) | ||||
| <5 (guidelines’ recommendations) | 343 (81.9) | 398 (73.4) | 741 (77.1) | ref. |
| 5–10 | 72 (17.2) | 128 (23.6) | 200 (20.8) | 0.65 (0.47–0.91) ** |
| >10 | 4 (1.0) | 16 (3.0) | 20 (2.1) | 0.29 (0.09–0.88) ** |
| Taper ratio (%/week) | ||||
| <5 | 52 (12.4) | 53 (9.8) | 105 (10.9) | 1.59 (1.02–2.47) ** |
| 5–10 (guidelines’ recommendations) | 142 (33.9) | 230 (42.4) | 372 (38.7) | ref. |
| >10 | 225 (53.7) | 259 (47.8) | 484 (50.4) | 1.40 (1.06–1.85) ** |
| % of weeks when the dose was decreased in the tapering phase (%) | ||||
| <25 | 74 (17.7) | 137 (25.3) | 211 (22.0) | ref. |
| 25–49 | 147 (35.1) | 267 (49.3) | 414 (43.1) | 1.02 (0.72–1.46) |
| 50–74 | 112 (26.7) | 109 (20.1) | 221 (23.0) | 1.91 (1.28–2.84) *** |
| 75–89 | 49 (11.7) | 17 (3.1) | 66 (6.9) | 5.42 (2.88–10.20) *** |
| ≥90 | 37 (8.8) | 12 (2.2) | 49 (5.1) | 5.82 (2.82–11.99) *** |
| Variables | Model 1 | Model 2 | ||
|---|---|---|---|---|
| aOR (95% CI) | p | aOR (95% CI) | p | |
| Employment Status | ||||
| unemployed | ref. | ref. | ||
| employed | 0.88 (0.60–1.28) | 0.502 | 0.88 (0.61–1.29) | 0.525 |
| Years of drug abuse before enrolment in MMT | ||||
| <5 | 1.43 (0.70–2.90) | 0.323 | 1.52 (0.75–3.09) | 0.243 |
| 5–9 | 1.43 (0.92–2.23) | 0.117 | 1.40 (0.90–2.18) | 0.139 |
| ≥10 | ref. | ref. | ||
| Treatment attendance (%) | ||||
| <50 | ref. | ref. | ||
| 50–80 | 1.72 (0.72–4.11) | 0.229 | 1.62 (0.67–3.92) | 0.296 |
| >80 | 3.40 (1.44–7.98) | 0.009 | 3.29 (1.38–7.87) | 0.012 |
| Duration of the treatment episode (years) | 0.63 (0.52–0.77) | <0.001 | 0.64 (0.53–0.78) | <0.001 |
| % change in dose throughout the treatment episode per week (%) | ||||
| <1 | ref. | ref. | ||
| 1–4 | 0.77 (0.42–1.39) | 0.388 | 0.79 (0.43–1.45) | 0.453 |
| >4 | 1.08 (0.53–2.17) | 0.840 | 0.93 (0.46–1.88) | 0.841 |
| Taper start week | ||||
| <16 | ref. | ref. | ||
| 16–52 | 1.29 (0.90–1.83) | 0.170 | 1.33 (0.93–1.90) | 0.122 |
| >52 | 2.81 (1.48–5.34) | 0.003 | 2.86 (1.50–5.47) | 0.003 |
| Taper start dose (mg) | ||||
| <60 | 2.08 (1.44–3.00) | <0.001 | 1.60 (1.11–2.31) | 0.018 |
| 60–120 | ref. | ref. | ||
| >120 | 0.87 (0.23–3.26) | 0.835 | 1.36 (0.38–4.87) | 0.642 |
| Taper duration (weeks) | ||||
| <13 | 1.77 (0.90–3.50) | 0.106 | 2.15 (0.87–5.34) | 0.112 |
| 13–25 | 1.42 (0.78–2.58) | 0.255 | 1.58 (0.86–2.90) | 0.142 |
| 26–52 | 1.14 (0.68–1.91) | 0.625 | 1.20 (0.71–2.01) | 0.494 |
| >52 | ref. | ref. | ||
| Taper ratio (%/week) | ||||
| <5 | 2.08 (1.18–3.64) | 0.015 | ||
| 5–10 (guidelines recommendations) | ref. | |||
| >10 | 0.82 (0.57–1.18) | 0.291 | ||
| Taper dose (mg/week) | ||||
| <5 (guidelines’ recommendations) | ref. | |||
| 5–10 | 0.55 (0.36–0.84) | 0.013 | ||
| >10 | 0.18 (0.05–0.62) | 0.014 | ||
| % weeks when dose decreased in tapering phase (%) | ||||
| <25 | ref. | ref. | ||
| 25–50 | 0.97 (0.63–1.47) | 0.872 | 0.91 (0.60–1.39) | 0.669 |
| 50–74 | 1.23 (0.72–2.12) | 0.449 | 1.08 (0.63–1.88) | 0.776 |
| 75–89 | 3.07 (1.22–7.68) | 0.020 | 2.71 (1.07–6.85) | 0.039 |
| ≥90 | 2.53 (0.93–6.88) | 0.075 | 2.14 (0.78–5.89) | 0.145 |
| AIC | 3714.03 | 3722.27 | ||
| Variables | Employed (N = 204) | Unemployed (N = 649) | ||
|---|---|---|---|---|
| aOR (95% CI) | p | aOR (95% CI) | p | |
| Taper start week | ||||
| <16 | ref. | ref. | ||
| 16–52 | 0.70 (0.33–1.48) | 0.349 | 1.53 (1.05–2.23) | 0.027 |
| >52 | 2.68 (0.70–10.29) | 0.149 | 2.94 (1.49–5.81) | 0.002 |
| Taper start dose (mg) | ||||
| <60 | 1.79 (1.09–2.95) | 0.043 | 1.98 (1.33–2.93) | 0.001 |
| 60–120 | ref. | ref. | ||
| >120 | 1.14 (0.27–4.79) | 0.858 | 1.10 (0.29–4.11) | 0.889 |
| Taper duration (weeks) | ||||
| <13 | 2.48 (0.55–11.25) | 0.238 | 2.03 (1.01–4.10) | 0.048 |
| 13–25 | 1.23 (0.33–4.52) | 0.760 | 1.67 (0.90–3.09) | 0.106 |
| 26–52 | 0.74 (0.24–2.27) | 0.599 | 1.38 (0.80–2.36) | 0.243 |
| >52 | ref. | ref. | ||
| Taper ratio (%/week) | ||||
| <5 | 1.83 (0.65–5.16) | 0.248 | 1.72 (0.92–3.24) | 0.091 |
| 5–10 (guidelines recommendations) | ref. | |||
| >10 | 1.02 (0.47–2.19) | 0.966 | 0.86 (0.59–1.25) | 0.424 |
| % weeks when dose decreased in tapering phase (%) | ||||
| <25 | ref. | ref. | ||
| 25–50 | 0.61 (0.25–1.52) | 0.287 | 0.85 (0.54–1.34) | 0.494 |
| 50–74 | 0.65 (0.19–2.17) | 0.479 | 1.27 (0.71–2.28) | 0.427 |
| 75–89 | 1.03 (0.18–5.75) | 0.974 | 2.80 (1.07–7.31) | 0.036 |
| ≥90 | 0.91 (0.11–7.26) | 0.925 | 2.90 (0.96–8.79) | 0.059 |
| Variables | <10 years (N = 184) | ≥10 years (N = 669) | ||
|---|---|---|---|---|
| aOR (95% CI) | p | aOR (95% CI) | p | |
| Taper start week | ||||
| <16 | ref. | ref. | ||
| 16–52 | 0.86 (0.36–2.06) | 0.738 | 1.39 (0.93–2.07) | 0.110 |
| >52 | 4.70 (0.98–22.49) | 0.052 | 2.45 (1.18–5.11) | 0.016 |
| Taper start dose (mg) | ||||
| <60 | 2.87 (1.16–7.11) | 0.023 | 1.97 (1.30–3.00) | 0.001 |
| 60–120 | ref. | ref. | ||
| >120 | 1.49 (0.09–24.14) | 0.775 | 0.69 (0.15–3.23) | 0.635 |
| Taper duration (weeks) | ||||
| <13 | 0.58 (0.10–3.40) | 0.540 | 2.45 (1.14–5.25) | 0.022 |
| 13–25 | 0.53 (0.12–2.37) | 0.407 | 1.82 (0.92–3.61) | 0.085 |
| 26–52 | 0.40 (0.11–1.46) | 0.164 | 1.49 (0.83–2.68) | 0.176 |
| >52 | ref. | ref. | ||
| Taper ratio (%/week) | ||||
| <5 | 2.05 (0.59–7.07) | 0.256 | 2.26 (1.18–4.32) | 0.014 |
| 5–10 (guidelines recommendations) | ref. | ref. | ||
| >10 | 0.73 (0.31–1.72) | 0.473 | 0.85 (0.56–1.29) | 0.443 |
| % weeks when dose decreased in tapering phase (%) | ||||
| <25 | ref. | ref. | ||
| 25–50 | 0.94 (0.34–2.61) | 0.897 | 0.97 (0.60–1.56) | 0.894 |
| 50–74 | 1.82 (0.43–7.63) | 0.409 | 1.12 (0.61–2.06) | 0.716 |
| 75–89 | 5.80 (0.68–49.40) | 0.107 | 2.51 (0.87–7.23) | 0.089 |
| ≥90 | 11.58 (0.62–215.08) | 0.100 | 1.81 (0.59–5.50) | 0.297 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lu, Q.; Zou, X.; Liu, Y.; Gong, C.; Ling, L. Dose Tapering Strategy for Heroin Abstinence among Methadone Maintenance Treatment Participants: Evidence from A Retrospective Study in Guangdong, China. Int. J. Environ. Res. Public Health 2019, 16, 2800. https://doi.org/10.3390/ijerph16152800
Lu Q, Zou X, Liu Y, Gong C, Ling L. Dose Tapering Strategy for Heroin Abstinence among Methadone Maintenance Treatment Participants: Evidence from A Retrospective Study in Guangdong, China. International Journal of Environmental Research and Public Health. 2019; 16(15):2800. https://doi.org/10.3390/ijerph16152800
Chicago/Turabian StyleLu, Qian, Xia Zou, Yin Liu, Cheng Gong, and Li Ling. 2019. "Dose Tapering Strategy for Heroin Abstinence among Methadone Maintenance Treatment Participants: Evidence from A Retrospective Study in Guangdong, China" International Journal of Environmental Research and Public Health 16, no. 15: 2800. https://doi.org/10.3390/ijerph16152800