Interaction of Health Literacy and Problematic Mobile Phone Use and Their Impact on Non-Suicidal Self-Injury among Chinese Adolescents



Abstract
:1. Introduction
2. Methods
2.1. Study Participants and Procedures
2.2. Demographic Information
2.3. Questionnaire Data
2.4. Statistical Analysis
3. Results
3.1. Univariate Analyses
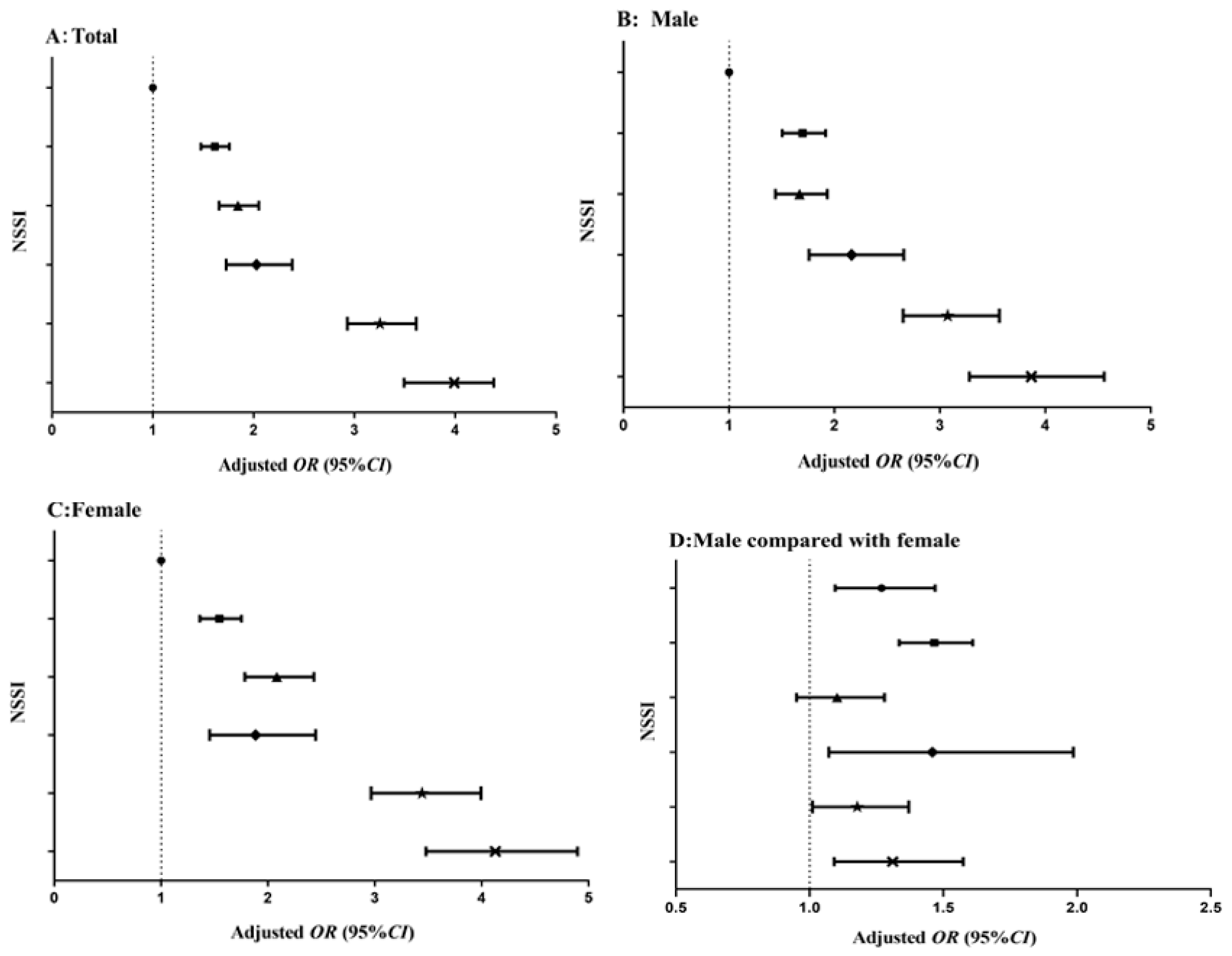
3.2. Multivariate Logistic Regression Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Groups | n (%) | Crude OR (95 % CI) A | Adjusted OR (95 % CI) a | n (%) | Crude OR (95 % CI) B | Adjusted OR (95 % CI) a | n (%) | Crude OR (95 % CI) C | Adjusted OR (95 % CI) a | Crude OR (95 % CI) D | Adjusted OR (95 % CI) a |
|---|---|---|---|---|---|---|---|---|---|---|---|
| No + High | 4630 (20.5) | 1.000 | 1.000 | 2255 (20.5) | 1.000 | 1.000 | 2375 (20.4) | 1.000 | 1.000 | 1.221 (1.059−1.408) ** | 1.269 (1.096−1.469) *** |
| No + Medium | 8923 (39.4) | 1.589 (1.461−1.729) *** | 1.614 (1.479−1.760) *** | 4120 (37.5) | 1.761 (1.565−1.982) *** | 1.698 (1.505−1.916) *** | 4803 (41.3) | 1.456 (1.290−1.643) *** | 1.545 (1.363−1.752) *** | 1.447 (1.348−1.619) *** | 1.466 (1.335−1.610) *** |
| No + Low | 3323 (15.7) | 1.853 (1.674−2.051) *** | 1.844 (1.657−2.051) *** | 1699 (15.5) | 1.782 (1.547−2.052) *** | 1.668 (1.440−1.933) *** | 1624 (14.0) | 1.920 (1.658−2.224) *** | 2.082 (1.784−2.429) *** | 1.133 (0.980−1.311) | 1.103 (0.951−1.280) |
| Yes + High | 856 (3.8) | 2.060 (1.760−2.412) *** | 2.028 (1.727−2.381) *** | 512 (4.7) | 2.209 (1.802−2.707) *** | 2.162 (1.760−2.657) *** | 344 (3.0) | 1.739 (1.349−2.242) *** | 1.885 (1.454−2.445) *** | 1.551 (1.158−2.079) ** | 1.459 (1.072−1.986) * |
| Yes + Medium | 2919 (12.9) | 3.133 (2.830−3.470) *** | 3.253 (2.930−3.613) *** | 1383 (12.6) | 3.162 (2.736−3.655) *** | 3.074 (2.652−3.564) *** | 1536 (13.2) | 3.138 (2.717−3.623) *** | 3.441 (2.965−3.993) *** | 1.231 (1.063−1.425) ** | 1.178 (1.011−1.371) * |
References
- Favazza, A.R. Bodies under Siege: Self-Mutilation and Body Modification in Culture and Psychiatry, 2nd ed.; Johns Hopkins: London, UK, 1996. [Google Scholar]
- Liu, Z.Z.; Chen, H.; Bo, Q.G.; Chen, R.H.; Li, F.W.; Lv, L.; Jia, C.X.; Liu, X.C. Psychological and behavioral characteristics of suicide attempts and non-suicidal self-injury in Chinese adolescents. J. Affect. Disord. 2018, 226, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Whitlock, J.; Muehlenkamp, J.; Eckenrode, J.; Purington, A.; Abrams, G.B.; Barreira, P. Nonsuicidal self-injury as a gateway to suicide in young adults. J. Adolesc. Health 2013, 52, 486–492. [Google Scholar] [CrossRef] [PubMed]
- Nock, M.K. Self-injury. Annu. Rev. Clin. Psychol. 2010, 6, 339–363. [Google Scholar] [CrossRef] [PubMed]
- Monto, M.A.; McRee, N.; Deryck, F.S. Nonsuicidal self-injury among a representative sample of US adolescents, 2015. Am. J. Public Health 2018, 108, 1042–1048. [Google Scholar] [CrossRef] [PubMed]
- Calvete, E.; Orue, I.; Aizpuru, L.; Brotherton, H. Prevalence and functions of non-suicidal self-injury in Spanish adolescents. Psicothema 2015, 27, 223–228. [Google Scholar] [CrossRef] [PubMed]
- Swannell, S.V.; Martin, G.E.; Page, A.; Hasking, P.; St John, N.J. Prevalence of non-suicidal self-injury in nonclinical samples: Systematic review, meta-analysis and meta-regression. Suicide Life Threat. Behav. 2014, 44, 273–303. [Google Scholar] [CrossRef] [PubMed]
- Lang, J.J.; Yao, Y.S. Prevalence of nonsuicidal self-injury in Chinese middle school and high school students: A meta-analysis. Medicine 2018, 97, e12916. [Google Scholar] [CrossRef] [PubMed]
- Stewart, J.G.; Esposito, E.C.; Glenn, C.R.; Gilman, S.E.; Pridgen, B.; Gold, J.; Auerbach, R.P. Adolescent self-injurers: Comparing non-ideators, suicide ideators, and suicide attempters. J. Psychiatr. Res. 2017, 84, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Kiekens, G.; Claes, L.; Demyttenaere, K.; Auerbach, R.P.; Green, J.G.; Kessler, R.C.; Mortier, P.; Nock, M.K.; Bruffaerts, R. Lifetime and 12-month nonsuicidal self-injury and academic performance in college freshmen. Suicide Life Threat. Behav. 2016, 46, 563–576. [Google Scholar] [CrossRef] [PubMed]
- U.S. National Library of Medicine. Health Literacy. 2018. Available online: https://medlineplus.gov/healthliteracy.html (accessed on 19 May 2019).
- Nutbeam, D. The evolving concept of health literacy. Soc. Sci. Med. 2008, 67, 2072–2078. [Google Scholar] [CrossRef] [PubMed]
- Olyani, S.; Tehrani, H.; Esmaily, H.; Rezaii, M.M.; Vahedian-Shahroodi, M. Assessment of health literacy with the Newest Vital Sign and its correlation with body mass index in female adolescent students. Int. J. Adolesc. Med. Health 2017. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.C.; Tao, F.B.; Wu, X.Y.; Tao, S.M.; Fang, J. Low health literacy and psychological symptoms potentially increase the risks of non-suicidal self-injury in Chinese middle school students. BMC Psychiatry 2016, 16, 327. [Google Scholar] [CrossRef]
- Dharmapuri, S.; Best, D.; Kind, T.; Silber, T.J.; Simpson, P.; D’Angelo, L. Health literacy and medication adherence in adolescents. J. Pediatr. 2015, 166, 378–382. [Google Scholar] [CrossRef] [PubMed]
- Mottus, R.; Johnson, W.; Murray, C.; Wolf, M.S.; Starr, J.M.; Deary, I.J. Towards understanding the links between health literacy and physical health. Health Psychol. 2014, 33, 164–173. [Google Scholar] [CrossRef] [PubMed]
- Chari, R.; Warsh, J.; Ketterer, T.; Hossain, J.; Sharif, I. Association between health literacy and child and adolescent obesity. Patient Educ. Couns. 2014, 94, 61–66. [Google Scholar] [CrossRef]
- Rolová, G.; Barták, M.; Rogalewicz, V.; Gavurová, B. Health literacy in people undergoing treatment for alcohol abuse-A pilot study. Kontakt 2018, 20, 394–400. [Google Scholar] [CrossRef]
- Choudhury, S.; Saha, I.; Som, T.K.; Ghose, G.; Patra, M.; Paul, B. Mobile phone involvement and dependence among undergraduate medical students in a medical college of west Bengal, India. J. Educ. Health Promot. 2019. [Google Scholar] [CrossRef]
- Tao, S.M.; Wu, X.Y.; Wan, Y.H.; Zhang, S.C.; Hao, J.H.; Tao, F.B. Interactions of problematic mobile phone use and psychopathological symptoms with unintentional injuries: A school-based sample of Chinese adolescents. BMC Public Health 2016, 16, 88. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Science, ICT and Future Planning of Korea. Internet Addiction Survey 2014. 2015. Available online: http://www.msip.go.kr/cms/www/news/notice/__icsFiles/afieldfile/2015/04/14/2014%EB%85%84_%EC%9D%B8%ED%84%B0%EB%84%B7%EC%A4%91%EB%8F%85_%EC%8B%A4%ED%83%9C%EC%A1%B0%EC%82%AC_%EA%B2%B0%EA%B3%BC.hwp (accessed on 19 May 2019).
- Liu, Q.Q.; Zhou, Z.K.; Yang, X.J.; Kong, F.C.; Niu, G.F.; Fan, C.Y. Mobile phone addiction and sleep quality among Chinese adolescents: A moderated mediation model. Comput. Human Behav. 2017, 72, 108–114. [Google Scholar] [CrossRef]
- Tamura, H.; Nishida, T.; Tsuji, A.; Sakakibara, H. Association between excessive use of mobile phone and insomnia and depression among Japanese adolescents. Int. J. Environ. Res. Public Health 2017, 14, 701. [Google Scholar] [CrossRef]
- Tao, S.M.; Wu, X.Y.; Zhang, S.C.; Tong, S.L.; Hao, J.H.; Tao, F.B. Association of alcohol use with problematic mobile phone use and depressive symptoms among college students in Anhui, China. J. Public Health 2016, 25, 103–112. [Google Scholar] [CrossRef]
- Jun, S. The reciprocal longitudinal relationships between mobile phone addiction and depressive symptoms among Korean adolescents. Comput. Hum. Behav. 2016, 58, 179–186. [Google Scholar] [CrossRef]
- Kantor, J.R. Behaviorism, behavior analysis, and the career of psychology. Psychol. Rec. 1976, 26, 305–312. [Google Scholar] [CrossRef]
- Sloan, T. Critical Psychology: Voices for Changes; Macmillan: London, UK, 2000. [Google Scholar]
- Olyani, S.; Peyman, N. Assessing health literacy and its relationship with using cell Phone among adolescents. Health Educ. Health Promot. 2016, 4, 47–57. [Google Scholar]
- Zhang, S.C.; Yang, R.; Li, D.L.; Wang, J.; Wan, Y.H.; Xu, S.J.; Xu, H.L.; Ma, S.S.; Wang, W.; Zeng, H.J.; et al. Interactive effects between health literacy and mobile phone dependence as well as its relation with unintentional injuries in middle school students. Chin. J. Epidemiol. 2018, 39, 1549–1554. (In Chinese) [Google Scholar] [CrossRef]
- Zhang, S.C.; Wan, Y.H.; Tao, S.M.; Chen, J.; Tao, F.B. Reliability and construct validity of the adolescent interactive health literacy questionnaire. Chin. J. Sch. Health 2014, 35, 332–336. (In Chinese) [Google Scholar] [CrossRef]
- Tao, S.M.; Fu, J.L.; Wang, H.; Hao, J.H.; Tao, F.B. Development of self-rating questionnaire for adolescent problematic mobile phone use and the psychometric evaluation in undergraduates. Chin. J. Sch. Health 2013, 34, 26–29. (In Chinese) [Google Scholar] [CrossRef]
- Wan, Y.H.; Hu, C.L.; Hao, J.H.; Sun, Y.; Tao, F.B. Deliberate self-harm behaviors in Chinese adolescents and young adults. Eur. Child Adolesc. Psychiatry 2011, 20, 517–525. [Google Scholar] [CrossRef]
- Wan, Y.H.; Xu, S.J.; Chen, J.; Hu, C.L.; Tao, F.B. Longitudinal effects of psychological symptoms on non-suicidal self-injury: A difference between adolescents and young adults in China. Soc. Psychiatry Psychiatr. Epidemiol. 2015, 50, 237–247. [Google Scholar] [CrossRef]
- Kidger, J.; Heron, J.; Lewis, G.; Evans, J.; Gunnell, D. Adolescent self-harm and suicidal thoughts in the ALSPAC cohort: A self-report survey in England. BMC Psychiatry 2012, 12, 69. [Google Scholar] [CrossRef]
- Chan, S.; Denny, S.; Fleming, T.; Fortune, S.; Peiris-John, R.; Dyson, B. Exposure to suicide behaviour and individual risk of self-harm: Findings from a nationally representative New Zealand high school survey. Aust. N. Z. J. Psychiatry 2018, 52, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Ceylan, M.F.; Tural Hesapcioglu, S.; Kasak, M.; Yavas, C.P. High prevalence of nonsuicidal self-injury, tattoos, and psychiatric comorbidity among male adolescent prisoners and their sociodemographic characteristics. Asian J. Psychiatry 2019, 43, 45–49. [Google Scholar] [CrossRef] [PubMed]
- Somer, O.; Bildik, T.; Kabukçu-Başay, B.; Güngör, D.; Başay, Ö.; Farmer, R.F. Prevalence of non-suicidal self-injury and distinct groups of self-injurers in a community sample of adolescents. Soc. Psychiatry Psychiatr. Epidemiol. 2015, 50, 1163–1171. [Google Scholar] [CrossRef] [PubMed]
- Wan, Y.H.; Chen, J.; Sun, Y.; Tao, F.B. Impact of childhood abuse on the risk of non-suicidal self-injury in mainland Chinese adolescents. PLoS ONE 2015, 10, e0131239. [Google Scholar] [CrossRef] [PubMed]
- Tang, J.; Li, G.; Chen, B.; Huang, Z.; Zhang, Y.; Chang, H.; Wu, C.; Ma, X.; Wang, J.; Yu, Y. Prevalence of and risk factors for non-suicidal self-injury in rural China: Results from a nationwide survey in China. J. Affect. Disord. 2018, 226, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Poon, J.A.; Thompson, J.C.; Forbes, E.E.; Chaplin, T.M. Adolescent’ reward-related neural activation: Links to thoughts of nonsuicidal self-injury. Suicide Life Threat. Behav. 2019, 49, 76–89. [Google Scholar] [CrossRef] [PubMed]
- Plener, P.L.; Kaess, M.; Schmahl, C.; Pollak, S.; Fegert, J.M.; Brown, R.C. Nonsuicidal Self-Injury in Adolescents. Dtsch. Ärzteblatt Int. 2018, 115, 23–30. [Google Scholar] [CrossRef] [Green Version]
- Santangelo, P.S.; Koenig, J.; Funke, V.; Parzer, P.; Resch, F.; Ebner-Priemer, U.W.; Kaess, M. Ecological momentary assessment of affective and interpersonal instability in adolescent non-suicidal self-injury. J. Abnorm. Child Psychol. 2016, 45, 1429–1438. [Google Scholar] [CrossRef]
- Bronfenbrenner, U. Toward an experimental ecology of human development. Am. Psychol. 1977, 32, 513–531. [Google Scholar] [CrossRef]
- Brown, R.C.; Witt, A. Social factors associated with non-suicidal self-injury (NSSI). Child Adolesc. Psychiatry Ment. Health 2019, 13, 23. [Google Scholar] [CrossRef]
- Xavier, A.; Cunha, M.; Pinto-Gouveia, J. Daily peer hassles and non-suicidal self-injury in adolescence: Gender differences in avoidance-focused emotion regulation processes. J. Child Fam. Stud. 2017, 27, 59–68. [Google Scholar] [CrossRef]
- Bresin, K.; Schoenleber, M. Gender differences in the prevalence of nonsuicidal self-injury: A meta-analysis. Clin. Psychol. Rev. 2015, 38, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Bem, D.; Connor, C.; Palmer, C.; Channa, S.; Birchwood, M. Frequency and preventative interventions for non-suicidal self-injury and suicidal behaviour in primary school-age children: A scoping review protocol. BMJ Open 2017, 7, e017291. [Google Scholar] [CrossRef] [PubMed]
- You, J.; Leung, F.; Fu, K. Exploring the reciprocal relations between nonsuicidal self-injury, negative emotions and relationship problems in Chinese adolescents: A longitudinal cross-lag study. J. Abnorm. Child Psychol. 2012, 40, 829–836. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Health Promotion by social cognitive means. Health Educ. Behav. 2004, 31, 143. [Google Scholar] [CrossRef]
- Reyna, V.F.; Farley, F. Risk and rationality in adolescent decision making: Implications for theory, practice, and public policy. Psychol. Sci. Public Interest 2006, 7, 1–44. [Google Scholar] [CrossRef] [PubMed]
- Jorm, A.; Wright, A.; Morgan, A. Beliefs about appropriate first aid for young people with mental disorders: Findings from an Australian national survey of youth and parents. Early Interv. Psychiatry 2007, 1, 61–70. [Google Scholar] [CrossRef]
- Çimen, İ.D.; Coşkun, A.; Etiler, N. Non-suicidal self-injury behaviors’ features and relationship with adolescents’ daily life activities and mental status. Turk. J. Pediatr. 2017, 59, 113–121. [Google Scholar] [CrossRef]
- Pawłowska, B.; Potembska, E.; Zygo, M.; Olajossy, M.; Dziurzyńska, E. Prevalence of self-injury performed by adolescents aged 16–19 years. Psychiatr. Pol. 2016, 50, 29–42. [Google Scholar] [CrossRef]
- Tao, S.M.; Wu, X.Y.; Liu, Y.H.; Zhang, Y.K.; Zhang, S.C.; Tao, F.B. Self-harm in medical college students and its relation with mobile phone dependence and depressive symptoms. Chin. Ment. Health J. 2014, 28, 472–477. (In Chinese) [Google Scholar] [CrossRef]
- Oshima, N.; Nishida, A.; Shimodera, S.; Tochigi, M.; Ando, S.; Yamasaki, S.; Okazaki, Y.; Sasaki, T. The suicidal feelings, self-injury, and mobile phone use after lights out in adolescents. J. Pediatr. Psychol. 2012, 37, 1023–1030. [Google Scholar] [CrossRef] [PubMed]

| Variable | Total Sample (n = 22,628) | NSSI | χ2 | φ/V | |
|---|---|---|---|---|---|
| No (n = 15,367) | Yes (n = 7261) | ||||
| Gender | 96.332 *** | −0.065 *** | |||
| Male | 10990 (48.6) | 7119 (64.8) | 3871 (35.2) | ||
| Female | 11638 (51.4) | 8248 (70.9) | 3390 (29.1) | ||
| Grade | 65.487 *** | −0.054 *** | |||
| Middle school | 11993 (53.0) | 7861 (65.6) | 4132 (34.4) | ||
| High school | 10635 (47.0) | 7506 (70.6) | 3129 (29.4) | ||
| Registered residence | 26.357 *** | −0.034 *** | |||
| Rural | 10882 (48.1) | 7210 (66.3) | 3672 (33.7) | ||
| Urban | 11746 (51.9) | 8157 (69.4) | 3589 (30.6) | ||
| Any siblings | 0.239 | 0.003 | |||
| Yes | 12908 (57.0) | 8749 (67.8) | 4159 (32.2) | ||
| No | 9720 (43.0) | 6618 (68.1) | 3102 (31.9) | ||
| Accommodation type | 6.952 ** | −0.018 ** | |||
| Boarding student | 11320 (50.0) | 7595 (67.1) | 3725 (32.9) | ||
| Commuting student | 11308 (50.0) | 7772 (68.7) | 3536 (31.3) | ||
| Father’s educational level a | 8.823 ** | −0.020 ** | |||
| < High school degree | 13006 (57.5) | 8735 (67.2) | 4271 (32.8) | ||
| ≥ High school degree | 9424 (41.6) | 6506 (69.0) | 2918 (31.0) | ||
| Mother’s educational level b | 9.751 ** | −0.021 ** | |||
| < High school degree | 14335 (63.4) | 9639 (67.2) | 4696 (32.8) | ||
| ≥ High school degree | 8105 (35.8) | 5614 (69.3) | 2491 (30.7) | ||
| Self-reported family economy | 67.759 *** | 0.055 *** | |||
| Bad | 3240 (14.3) | 2005 (61.9) | 1235 (38.1) | ||
| General | 16345 (72.2) | 11316 (69.2) | 5029 (30.8) | ||
| Good | 3043 (13.4) | 2046 (67.2) | 997 (32.8) | ||
| Number of friends | 37.753 *** | 0.041 *** | |||
| ≤ 2 | 5514 (24.4) | 3560 (64.6) | 1954 (35.4) | ||
| 3-5 | 9620 (42.5) | 6622 (68.8) | 2998 (31.2) | ||
| ≥ 6 | 7494 (33.1) | 5185 (69.2) | 2309 (30.8) | ||
| City | 102.702 *** | 0.067 *** | |||
| Shenyang | 3217(14.2) | 2165(67.3) | 1052(32.7) | ||
| Xinxiang | 3230(14.3) | 2327(72.0) | 903(28.0) | ||
| Yangjiang | 5061(22.4) | 3525(69.7) | 1536(30.3) | ||
| Chongqing | 5588(24.7) | 3865(69.2) | 1723(30.8) | ||
| Ulanchap | 2333(10.3) | 1506(64.6) | 827(35.4) | ||
| Bengbu | 3199(14.1) | 1979(61.9) | 1220(38.1) | ||
| HL | 343.427 *** | 0.123 *** | |||
| High | 5486 (24.2) | 4230 (77.1) | 1256 (22.9) | ||
| Medium | 11842 (52.3) | 7917 (66.9) | 3925 (33.1) | ||
| Low | 5300 (23.4) | 3220 (60.8) | 2080 (39.2) | ||
| PMPU | 623.184 *** | 0.166 *** | |||
| No | 16876 (74.6) | 12224 (72.4) | 4652 (27.6) | ||
| Yes | 5752 (25.4) | 3143 (54.6) | 2609 (45.4) | ||
| Items | Total Sample (n = 22628) | Male (n = 10990) | Female (n = 11638) | χ2 | φ/V |
|---|---|---|---|---|---|
| 1.Have you ever hit yourself? | 25.124 *** | −0.033 *** | |||
| No | 19425 (85.8) | 9303 (41.1) | 10122 (44.7) | ||
| Yes | 3203 (14.2) | 1687 (7.5) | 1516 (6.7) | ||
| 2. Have you ever pulled your hair yourself? | 139.819 *** | −0.079 *** | |||
| No | 20006 (88.4) | 9432 (41.7) | 10574 (46.7) | ||
| Yes | 2622 (11.6) | 1558 (6.9) | 1064 (4.7) | ||
| 3. Have you ever banged your head or fist against something? | 521.060 *** | −0.152 *** | |||
| No | 18118 (80.1) | 8114 (35.9) | 10004 (44.2) | ||
| Yes | 4510 (19.9) | 2876 (12.7) | 1634 (7.2) | ||
| 4. Have you ever pinched or scratched yourself? | 110.153 *** | 0.070 *** | |||
| No | 19918 (88.0) | 9930 (43.9) | 9988 (44.1) | ||
| Yes | 2710 (12.0) | 1060 (4.7) | 1650 (7.3) | ||
| 5. Have you ever bitten yourself? | 48.302 *** | 0.046 *** | |||
| No | 21044 (93.0) | 10354 (45.8) | 10690 (47.2) | ||
| Yes | 1584 (7.0) | 636 (2.8) | 948 (4.2) | ||
| 6. Have you ever cut or pierced yourself? | 32.246 *** | 0.038 *** | |||
| No | 21277 (94.0) | 10435 (46.1) | 10842 (47.9) | ||
| Yes | 1351 (6.0) | 555 (2.5) | 796 (3.5) | ||
| 7. Have you ever exposed yourself to smoke, fire and flames or come in contact with heat and hot substances? | 51.465 *** | −0.048 *** | |||
| No | 21692 (95.9) | 10428 (46.1) | 11264 (49.8) | ||
| Yes | 936 (4.1) | 562 (2.5) | 374 (1.7) | ||
| 8. Have you ever ingested a toxic substance or object? | 48.089 *** | −0.046 *** | |||
| No | 22332 (98.7) | 10787 (46.7) | 11545 (51.0) | ||
| Yes | 296 (1.3) | 203 (0.9) | 93 (0.4) |
| Variables | NSSI | ||
|---|---|---|---|
| n (%) | Crude OR (95 % CI) | Adjusted OR (95 % CI) a | |
| HL | |||
| High | 5415 (23.9) | 1.000 | 1.000 |
| Medium | 11686 (51.6) | 1.572 (1.459–1.693) *** | 1.609 (1.489–1.738) *** |
| Low | 5190 (22.9) | 1.878 (1.724–2.045) *** | 1.886 (1.723–2.065) *** |
| PMPU | |||
| No | 16644 (73.6) | 1.000 | 1.000 |
| Have | 5647 (25.0) | 2.027 (1.904–2.159) *** | 2.062 (1.934–2.199) *** |
| HL × PMPU | |||
| High × No | 1.000 | 1.000 | |
| Medium × Have | 2.108 (1.946–2.283) *** | 2.170 (2.000–2.354) *** | |
| Low × Have | 2.632 (2.395–2.891) *** | 2.617 (2.375–2.884) *** | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, D.; Yang, R.; Wan, Y.; Tao, F.; Fang, J.; Zhang, S. Interaction of Health Literacy and Problematic Mobile Phone Use and Their Impact on Non-Suicidal Self-Injury among Chinese Adolescents. Int. J. Environ. Res. Public Health 2019, 16, 2366. https://doi.org/10.3390/ijerph16132366
Li D, Yang R, Wan Y, Tao F, Fang J, Zhang S. Interaction of Health Literacy and Problematic Mobile Phone Use and Their Impact on Non-Suicidal Self-Injury among Chinese Adolescents. International Journal of Environmental Research and Public Health. 2019; 16(13):2366. https://doi.org/10.3390/ijerph16132366
Chicago/Turabian StyleLi, Danlin, Rong Yang, Yuhui Wan, Fangbiao Tao, Jun Fang, and Shichen Zhang. 2019. "Interaction of Health Literacy and Problematic Mobile Phone Use and Their Impact on Non-Suicidal Self-Injury among Chinese Adolescents" International Journal of Environmental Research and Public Health 16, no. 13: 2366. https://doi.org/10.3390/ijerph16132366