Trauma Informed Child Welfare Systems—A Rapid Evidence Review


Abstract
:1. Introduction
1.1. Trauma Informed Care
1.2. Trauma Informed Care and the Child Welfare System
2. Materials and Methods
2.1. Review Question
2.2. Search Strategy
2.3. Selection Criteria
2.3.1. Trauma Informed Care
2.3.2. Study Population
2.3.3. Outcomes
2.3.4. Study Design
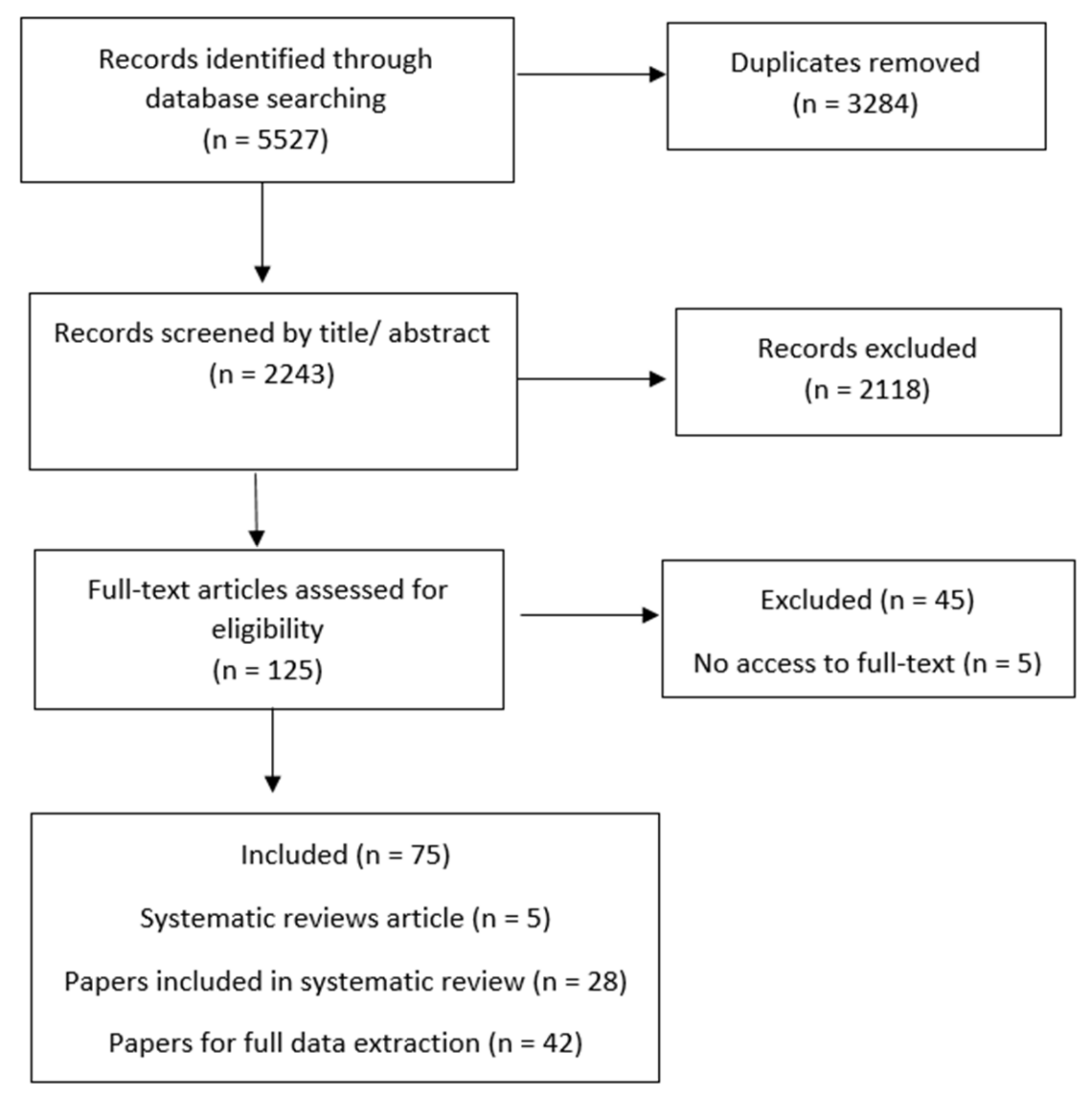
2.4. Screening
2.5. Data Extraction and Synthesis
3. Results
3.1. Service User Outcomes
Training
3.2. Workforce Development
3.2.1. On-Going Staff Support
3.2.2. Staff Support/Self-Care
3.3. Trauma-Focused Services
3.3.1. Screening and Assessment
3.3.2. Evidence-Based Treatment and Trauma-Focused Services
3.4. Organisational Change
3.4.1. Leadership Buy-In and Strategic Planning
3.4.2. Developing Policy, Procedures and Data Systems
3.4.3. Service User Involvement and Changes to the Physical Environment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Felitti, V.J.; Anda, R.F.; Nordenberg, D.; Williamson, D.F.; Spitz, A.M.; Edwards, V.; Loss, M.P.; Marks, J.S. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The Adverse Childhood Experiences (ACE) Study. Am. J. Prev. Med. 1998, 14, 245–258. [Google Scholar] [CrossRef]
- Anda, R.F.; Felitti, V.J.; Bremner, J.D.; Walker, J.D.; Whitfield, C.H.; Perry, B.D.; Dube, S.R.; Giles, W.H. The enduring effects of abuse and related adverse experiences in childhood. Eur. Arch. Psychiatry Clin. Neurosci. 2006, 256, 174–186. [Google Scholar] [CrossRef] [PubMed]
- Anda, R.F.; Butchart, A.; Felitti, V.J.; Brown, D.W. Building a framework for global surveillance of the public health implications of adverse childhood experiences. Am. J. Prev. Med. 2010, 39, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Bellis, M.A.; Ashton, K.; Hughes, K.; Ford, K.; Bishop, J.; Paranjothy, S. Adverse childhood experiences and their impact on health-harming behaviours in the Welsh adult population. Public Health Wales 2015, 36, 1–36. [Google Scholar]
- Hughes, K.; Bellis, M.A.; Hardcastle, K.A.; Sethi, D.; Butchart, A.; Mikton, C.; Jones, L.; Dunne, M.P. The effect of multiple adverse childhood experiences on health: A systematic review and meta-analysis. Lancet Public Health 2017, 2, e356–e366. [Google Scholar] [CrossRef]
- Van der Kolk, B.A.; Roth, S.; Pelcovitz, D.; Sunday, S.; Spinazzola, J. Disorders of extreme stress: The empirical foundation of a complex adaptation to trauma. J. Trauma. Stress 2005, 18, 389–399. [Google Scholar] [CrossRef] [PubMed]
- SAMHSA. SAMHSA’s Concept of Trauma and Guidance for Trauma-Informed Approach. Available online: https://www.nasmhpd.org/sites/default/files/SAMHSA_Concept_of_Trauma_and_Guidance.pdf (accessed on 22 August 2018).
- Ko, S.J.; Ford, J.D.; Kassam-Adams, N.; Berkowitz, S.J.; Wilson, C.; Wong, M.; Layne, C.M. Creating trauma-informed systems: Child welfare, education, first responders, health care, juvenile justice. Prof. Psychol. Res. Pract. 2008, 39, 396. [Google Scholar] [CrossRef]
- Hanson, R.F.; Lang, J. A critical look at trauma-informed care among agencies and systems serving maltreated youth and their families. Child Maltreatment 2016, 21, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Bryson, S.A.; Gauvin, E.; Jamieson, A.; Rathgeber, M.; Faulkner-Gibson, L.; Bell, S.; Burke, S. What are effective strategies for implementing trauma-informed care in youth inpatient psychiatric and residential treatment settings? A realist systematic review. Int. J. Ment. Health Syst. 2017, 11, 36. [Google Scholar] [CrossRef]
- Bailey, C.; Klas, A.; Cox, R.; Bergmeier, H.; Avery, J.; Skouteris, H. Systematic review of organisation-wide, trauma-informed care models in out-of-home care (Oo HC) settings. Health Soc. Care Community 2018. [Google Scholar] [CrossRef] [PubMed]
- Purtle, J. Systematic Review of Evaluations of Trauma-Informed Organizational Interventions That Include Staff Trainings. Trauma Violence Abuse 2018. [Google Scholar] [CrossRef] [PubMed]
- Branson, C.E.; Baetz, C.L.; Horwitz, S.M.; Hoagwood, K.E. Trauma-informed juvenile justice systems: A systematic review of definitions and core components. Psychol. Trauma Theory Res. Pract. Policy 2017, 9, 635. [Google Scholar] [CrossRef] [PubMed]
- Muskett, C. Trauma-informed care in inpatient mental health settings: A review of the literature. Int. J. Ment. Health Nurs. 2014, 23, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Bunting, L.; Montgomery, L.; Mooney, S.; MacDonald, M.; Coulter, S.; Hayes, D.; Davidson, G.; Forbes, T. Evidence Review-Developing Trauma-informed practice in Northern Ireland: Key Message; Safeguarding Board: Belfast, Northern Ireland, UK, 2018. [Google Scholar]
- Ryan, R. Data synthesis and analysis, Cochrane Consumers and Communication Review Group. 2013, pp. 1–5. Available online: https://cccrg.cochrane.org/sites/cccrg.cochrane.org/files/public/uploads/Analysis.pdf (accessed on 01 July 2019).
- Barto, B.; Bartlett, J.D.; Von Ende, A.; Bodian, R.; Noroña, C.R.; Griffin, J.; Fraser, J.G.; Kinniburgh, K.; Spinazzola, J.; Montagna, C.; et al. The impact of a statewide trauma-informed child welfare initiative on children’s permanency and maltreatment outcomes. Child Abuse Neglect 2018, 81, 149–160. [Google Scholar] [CrossRef]
- Barnett, E.R.; Cleary, S.E.; Butcher, R.L.; Jankowski, M.K. Children’s behavioral health needs and satisfaction and commitment of foster and adoptive parents: Do trauma-informed services make a difference? Psychol Trauma 2019, 11, 73–81. [Google Scholar] [CrossRef]
- Arvidson, J.; Kinniburgh, K.; Howard, K.; Spinazzola, J.; Strothers, H.; Evans, M.; Blaustein, M.E. Treatment of complex trauma in young children: Developmental and cultural considerations in application of the ARC intervention model. J. Child Adolesc. Trauma 2011, 4, 34–51. [Google Scholar] [CrossRef]
- Lucero, N.M.; Bussey, M. A collaborative and trauma-informed practice model for urban Indian child welfare. Child Welfare 2012, 91, 89. [Google Scholar]
- Suarez, E.; Jackson, D.S.; Slavin, L.A.; Michels, M.S.; McGeehan, K.M. Project Kealahou: Improving Hawai ‘i’s system of care for at-risk girls and young women through gender-responsive, trauma-informed care. Hawai’i J. Med. Public Health 2014, 73, 387. [Google Scholar]
- Hodgdon, H.B.; Blaustein, M.; Kinniburgh, K.; Peterson, M.L.; Spinazzola, J. Application of the ARC model with adopted children: Supporting resiliency and family well-being. J. Child Adolesc. Trauma 2016, 9, 43–53. [Google Scholar] [CrossRef]
- Murphy, K.; Moore, K.A.; Redd, Z.; Malm, K. Trauma-informed child welfare systems and children’s well-being: A longitudinal evaluation of KVC’s bridging the way home initiative. Child. Youth Serv. Rev. 2017, 75, 23–34. [Google Scholar] [CrossRef]
- Hall, S.F.; Jones, A.S. Implementation of intensive permanence services: A trauma-informed approach to preparing foster youth for supportive relationships. Child Adolesc. Soc. Work J. 2018, 35, 587–598. [Google Scholar] [CrossRef]
- Fraser, J.G.; Griffin, J.L.; Barto, B.L.; Lo, C.; Wenz-Gross, M.; Spinazzola, J.; Bodian, R.A.; Nisenbaum, J.L.; Bartlett, J.D. Implementation of a workforce initiative to build trauma-informed child welfare practice and services: Findings from the Massachusetts Child Trauma Project. Child. Youth Serv. Rev. 2014, 44, 233–242. [Google Scholar] [CrossRef]
- Bartlett, J.D.; Barto, B.; Griffin, J.L.; Fraser, J.G.; Hodgdon, H.; Bodian, R. Trauma-informed care in the Massachusetts child trauma project. Child Maltreatment 2016, 21, 101–112. [Google Scholar] [CrossRef]
- Redd, Z.; Malm, K.; Moore, K.; Murphy, K.; Beltz, M. KVC’s Bridging the way home: An innovative approach to the application of Trauma Systems Therapy in child welfare. Child. Youth Serv. Rev. 2017, 76, 170–180. [Google Scholar] [CrossRef]
- Kerns, S.E.; Pullmann, M.D.; Negrete, A.; Uomoto, J.A.; Berliner, L.; Shogren, D.; Silverman, E.; Putnam, B. Development and implementation of a child welfare workforce strategy to build a trauma-informed system of support for foster care. Child Maltreatment 2016, 21, 135–146. [Google Scholar] [CrossRef] [PubMed]
- Kramer, T.L.; Sigel, B.A.; Conners-Burrow, N.A.; Savary, P.E.; Tempel, A. A statewide introduction of trauma-informed care in a child welfare system. Child. Youth Serv. Rev. 2013, 35, 19–24. [Google Scholar] [CrossRef]
- Conners-Burrow, N.A.; Kramer, T.L.; Sigel, B.A.; Helpenstill, K.; Sievers, C.; McKelvey, L. Trauma-informed care training in a child welfare system: Moving it to the front line. Child. Youth Serv. Rev. 2013, 35, 1830–1835. [Google Scholar] [CrossRef]
- Lang, J.M.; Campbell, K.; Shanley, P.; Crusto, C.A.; Connell, C.M. Building capacity for trauma-informed care in the child welfare system: Initial results of a statewide implementation. Child Maltreatment 2016, 21, 113–124. [Google Scholar] [CrossRef]
- Henry, J.; Richardson, M.; Black-Pond, C.; Sloane, M.; Atchinson, B.; Hyter, Y. A grassroots prototype for trauma-informed child welfare system change. Child Welfare 2011, 90, 169–186. [Google Scholar]
- Atkinson, A.J.; Riley, D.B. Training for adoption competency: Building a community of adoption-competent clinicians. Fam. Soc. J. Contemp. Soc. Serv. 2017, 98, 235–242. [Google Scholar] [CrossRef]
- Counts, J.M.; Gillam, R.J.; Perico, S.; Eggers, K.L. Lemonade for Life—A pilot study on a hope-infused, trauma-informed approach to help families understand their past and focus on the future. Child. Youth Serv. Rev. 2017, 79, 228–234. [Google Scholar] [CrossRef]
- Middleton, J.; Harvey, S.; Esaki, N. Transformational leadership and organizational change: how do leaders approach trauma-informed organizational change twice? Fam. Soc. J. Contemp. Soc. Serv. 2015, 96, 155–163. [Google Scholar] [CrossRef]
- Kenny, M.C.; Vazquez, A.; Long, H.; Thompson, D. Implementation and program evaluation of trauma-informed care training across state child advocacy centers: An exploratory study. Child. Youth Serv. Rev. 2016, 73, 15–23. [Google Scholar] [CrossRef]
- Lang, J.M.; Ake, G.; Barto, B.; Caringi, J.; Little, C.; Baldwin, M.J.; Sullivan, K.; Tunno, A.M.; Bodian, R.; Stewart, C.J.; et al. Trauma screening in child welfare: Lessons learned from five states. J. Child Adolesc. Trauma 2017, 10, 405–416. [Google Scholar] [CrossRef]
- Emshoff, J.G.; Darnell, A.J.; Darnell, D.A.; Erickson, S.W.; Schneider, S.; Hudgins, R. Systems change as an outcome and a process in the work of community collaboratives for health. Am. J. Community Psychol. 2007, 39, 255–267. [Google Scholar] [CrossRef] [PubMed]
- Foster-Fishman, P.G.; Behrens, T.R. Systems change reborn: Rethinking our theories, methods, and efforts in human services reform and community-based change. Am. J. Community Psychol. 2007, 39, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Foster-Fishman, P.G.; Nowell, B.; Yang, H. Putting the system back into systems change: A framework for understanding and changing organizational and community systems. Am. J. Community Psychol. 2007, 39, 197–215. [Google Scholar] [CrossRef] [PubMed]
- Barnett, E.R.; Yackley, C.R.; Licht, E.S. Developing, implementing, and evaluating a trauma-informed care program within a youth residential treatment center and special needs school. Resid. Treat. Child. Youth 2018, 35, 95–113. [Google Scholar] [CrossRef]
- Damian, A.J.; Gallo, J.; Leaf, P.; Mendelson, T. Organizational and provider level factors in implementation of trauma-informed care after a city-wide training: an explanatory mixed methods assessment. BMC Health Serv. Res. 2017, 17, 750. [Google Scholar] [CrossRef] [PubMed]
- Lotzin, A.; Buth, S.; Sehner, S.; Hiller, P.; Martens, M.S.; Pawils, S.; Metzner, F.; Read, J.; Härter, M.; Schäfer, I. “Learning how to ask”: Effectiveness of a training for trauma inquiry and response in substance use disorder healthcare professionals. Psychol. Trauma: Theory Res. Pract. Policy 2018, 10, 229. [Google Scholar] [CrossRef] [PubMed]
- Decker, M.R.; Flessa, S.; Pillai, R.V.; Dick, R.N.; Quam, J.; Cheng, D.; McDonald-Mosley, R.; Alexander, K.A.; Holliday, C.N.; Miller, E. Implementing trauma-informed partner violence assessment in family planning clinics. J. Women’s Health 2017, 26, 957–965. [Google Scholar] [CrossRef] [PubMed]
- Miller, E.; McCauley, H.L.; Decker, M.R.; Levenson, R.; Zelazny, S.; Jones, K.A.; Anderson, H.; Silverman, J.G. Implementation of a family planning clinic–based partner violence and reproductive coercion intervention: Provider and patient perspectives. Perspect. Sex. Reprod. Health 2017, 49, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Quigg, Z.; Wallis, S.; Butler, N. Routine Enquiry About Adverse Childhood Experiences Implementation Pack Pilot Evaluation (Final Report); Public Health Institute, John Moore’s University: Liverpool, UK, 2018. [Google Scholar]
- Holstead, J.; Lamond, D.; Dalton, J.; Horne, A.; Crick., R. Restraint reduction in children’s residential facilities: Implementation at damar services. Resid. Treat. Child. Youth 2010, 1, 1–13. [Google Scholar] [CrossRef]
- Caldwell, B.; Albert, C.; Azeem, M.W.; Beck, S.; Cocoros, D.; Cocoros, T.; Reddy, B. Successful seclusion and restraint prevention efforts in child and adolescent programs. J. Psychosoc. Nurs. Ment. Health Serv. 2014, 52, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Borckardt, J.J.; Madan, A.; Grubaugh, A.L.; Danielson, C.K.; Pelic, C.G.; Hardesty, S.J.; Hanson, R.; Herbert, J.; Cooney, H.; Benson, A.; et al. Systematic investigation of initiatives to reduce seclusion and restraint in a state psychiatric hospital. Psychiatr. Serv. 2011, 62, 477–483. [Google Scholar]


{kind=link}
| Workforce Development | Trauma-Focused Services | Organisational Change |
|---|---|---|
| • Training of all staff on the impact of abuse or trauma • Measuring staff knowledge/practice • Strategies/procedures to address/reduce traumatic stress among staff • Knowledge/skills in accessing evidence-based services | • Screening/assessment to identify trauma history and symptoms • Child’s trauma history included in case record/plan • Availability of evidence-based trauma-focused practices | • Collaboration, coordination, and information sharing (internal and external) • Procedures to reduce risk for client re-traumatisation • Promotion of consumer engagement • Provision of strength-based services • Safe physical environment • Written policies that include/support TIC principles |
| Project/Reference | Outcomes | Workforce Development | Trauma-Focused Services | Organisational Change: | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Training | On-Going Support | Staff-Care | Screening/ Assessment | Evidence-Based Treatment | Trauma-Focused Practices/Services | Leadership Buy-In and Strategic Planning | Developing Policy, Procedures and Data Systems | Service User Involvement | Safe Physical Environment | ||
| Massachusetts Child Trauma Project [17,25,26] | x | x | x | x | x | x | |||||
| New Hampshire Adoption Preparation and Preservation/Partners for Change Project [18] | x | x | |||||||||
| Attachment, Regulation and Competency (ARC) Model [19] | x | x | |||||||||
| Indian Child Welfare Family Preservation Services [20] | x | x | |||||||||
| Project Kealahou (PK) [21] | x | x | |||||||||
| ADOPTS program [22] | x | x | |||||||||
| KVC Kansas [23,27] | x | x | x | x | x | ||||||
| Intensive Permanence Services (IPS) [24] | x | x | |||||||||
| Creating Connections [28] | x | ||||||||||
| Arkansas Initiative [29,30] | x | ||||||||||
| The Connecticut Collaborative on Effective Practices for Trauma (CONCEPT) [31] | x | x | |||||||||
| Michigan Children’s Trauma Assessment Centre (CTAC) [32] | x | x | x | x | |||||||
| Training for Adoption Competency (TAC) [33] | x | ||||||||||
| Lemonade for Life [34] | x | x | |||||||||
| Sanctuary Model [35] | x | x | |||||||||
| Child Advocacy Centres Florida [36] | x | ||||||||||
| Colorado, Connecticut, Massachusetts, Montana & North Carolina Trauma Screening Initiative [37] | x | ||||||||||
| Evaluation Design and Measures | Service User/Training Outcomes and Limitations |
|---|---|
| Massachusetts Child Trauma Project [17,26] | |
| Design: Preliminary implementation and follow up evaluations using a multi-source, multi-method approach. For service user outcomes this included: baseline assessment and six-month follow up of children referred to treatments (n = 326); and comparison of outcomes for 55,145 children who received the MCTP intervention (Cohort I; northern and western areas of the state) and 36,108 who did not (Cohort II; Boston and southern areas of the state) during the first year of implementation. Measures: child/family outcomes measured via administrative data on child maltreatment report, out-of-home placements, and adoption; clinical outcomes from children measured using the Posttraumatic Stress Disorder Reaction Index (UCLA PTSD-RI) and the Child Behaviour Checklist (CBCL). | Outcomes: • After approximately six months of EBT treatment, children had fewer post traumatic symptoms and behaviour problems. Children in the MCTP intervention group had fewer total substantiated reports of maltreatment, including less physical abuse and neglect than the comparison group by the end of the intervention year. • However, children in the MCTP intervention group had more maltreatment reports (substantiated or not) and total out-of-home placements than did their counterparts in the comparison group. • Assignment to MCTP was not associated with an increase in kinship care or adoption. Limitations: children were not randomly assigned to intervention; intervention and control children differ systematically in their background characteristics although this was accounted for by conducting an inverse probability of treatment weighted analysis. |
| New Hampshire Adoption Preparation and Preservation/Partners for Change Project [18] | |
| Design: Online and postal survey of licensed foster families, formerly licensed foster families and adoptive families from the past 10 years of records in one U.S. state (not specified). Aimed at examining whether foster and adoptive parent perceptions of the quality of trauma-informed child welfare and mental health services moderate the relationship between children’s behavioural health needs and parent satisfaction and commitment. Family units totalling 1206 were identified and 512 responded (42%: fostering only (n = 168), adoptive only (n = 215), fostering and having adopted (n = 66)). Measures: survey instrument designed by researchers. | Outcomes: • Trauma-informed mental health services (but not child welfare services) moderated the relationship between child behavioural health needs and foster parent (but not adoptive parent) satisfaction and commitment. • There was a significant interaction between child behavioural health needs and parent satisfaction and commitment (at low levels) of trauma-informed mental health services suggesting that these can buffer against low satisfaction and commitment, and thereby, potentially improve placement stability. Limitations: No standardised or validated measures. Based on adoptive parent and foster carer subjective perception of child behaviour problems and the quality of trauma-informed mental-health and child welfare services. Low response rate. |
| Alaska Child Trauma Centre [19] | |
| Design: naturalistic pre-test, post-test programme evaluation of treatment outcomes and placement stability in 93 children treated using ARC model (only 26 completed the intervention). Measures: Agency data and clinical assessments using Trauma Symptom Checklist Alternate Version, the UCLA PTSD Index for DSM IV and the Child Behaviour Checklist—CBCL used with all children. Administered at baseline, at three-month intervals, and at discharge. | Outcomes • The average drop in CBCL scores for children completing treatment was 19 points. • 90% children moved to permanent placements compared to usual 40%. Limitations: no specific comparison group so not clear how it compares to treatment as usual or if those completing treatment differed from those who did not, small numbers. |
| Indian Child Welfare services [20] | |
| Design: Evaluation of three years of family preservation services which served 73 families and 179 children over three years. Involved two projects (the RMQIC program and the SSUF program). Measures: Family functioning assessed via the North Carolina Family Assessment Scale (NCFAS), the Family Assessment Device, and the Parent Behaviour Inventory. Child safety measured directly by re-reports to CPS and indirectly through improvement on the Family Safety subscale of the NCFAS-AI (American Indian version of the NCFAS). | Outcomes: • A positive trend was seen in family safety for those families in the RMQIC program. • Families in the SSUF program showed significant positive change in the area of environment, and positive trends in the areas of caregiver capabilities, family safety and child well-being. • There were no re-reports during program services or within six months for any of the 49 families served by the RMQIC project. One new report within six months after services for the 24 families served by the SSUF project. This compared favourably with national re-report rates. • In the RMQIC project, 81% of families had their children maintained in the home, returned (if out-of-home-care was used), or placed with extended family members. • In the SSUF project, 96% of families were preserved with children either at home with parents (the most common result) or with extended family members. Limitations: no previous program baseline data presented and comparison only by national averages. |
| Project Kealahou (PK) [21] | |
| Design: Longitudinal design involving one to two hour-long structured interviews with youth and/or their caregivers at intake and at six-month intervals during the first two and a half years of PK services (September 2011–April 2014). Twenty-eight youth and 16 caregivers completed both baseline and six-month follow-up. Measures: Behavioural and Emotional Rating Scale, 2nd Edition (BERS–2C/2Y), Revised: Caregiver-Intake (CIQ-RC-I), Caregiver Strain Questionnaire (CGSQ), Child Behavior Checklist (CBCL 6–18), Columbia Impairment Scale (CIS), Education Questionnaire–Revision 2 (EQ–R2), Enrolment and Demographic Information Form (EDIF), Revised Children’s Manifest Anxiety Scale, Second Edition (RCMAS-2), Reynolds Adolescent Depression Scale, Second Edition (RADS–2), Youth Services Survey (YSS) | Outcomes: • Significant improvement from baseline to six-month follow-up on measures of youth strengths, competence, depression, impairment, behavioural problems, emotional problems, as well as caregiver strain. • A financial analysis indicated that these outcomes were obtained with a minimal overall increase in costs when compared to standard care alone ($365,803 vs. $344,141) Limitations: small number of participants, inability to determine which elements of PK services are responsible for its successful outcomes. |
| ADOPTS program [22] | |
| Design: Pre/post-test evaluation of the application of the ARC model with pre- or post-adoptive children and carers who had two or more lifetime traumatic exposures, with current post traumatic stress disorder (PTSD) and functional impairment in two domains. Twelve-month follow up. Measures: Clinician Administered PTSD Scale (CAPS); Trauma Symptom Checklist for Children (TSC-C); Behavioural Assessment System for Children (BASC); Parenting Stress Index (PSI). | Outcomes: • Significant lowering of Child Mental Health Symptoms with 76% of children assessed as having compared to 33.3% at follow-up. • The effect size for the reduction in PTSD symptoms was large (Cohen’s D = 1.88). • Significant reductions were found for child anxiety, depression, posttraumatic stress, dissociation and anger. • Significant reduction in care-giver stress. Limitations: lack of a control group, potential variability in treatment across clinicians, all evaluators were aware of treatment status of child. |
| KVC Behavioural Healthcare Kansas [23] | |
| Design: Longitudinal quasi-experimental study using administrative data to evaluate the impact of programme on 1499 children’s well-being and placement stability between over three of Trauma Systems Therapy (TST) implementations. Measures: KVC and researcher developed TST fidelity measures used to assess staff fidelity to TST implementation on a quarterly basis; child functioning was assessed by children’s caseworkers using the Child and Adolescent Functioning Assessment Scale (every 90 days), the Child Ecology Check-In (monthly basis); administrative placement history data were used to calculate children’s placement stability; fidelity scores and TST training dates of children’s care teams were used to calculate the level of TST or “dosage” that children received. | Service User Outcomes: • Increases in children’s exposure to TST (overall dosage) were associated with significantly greater improvements in functioning and behavioural regulation. • Increases in children’s exposure to TST (overall dosage) were not associated with greater improvements in emotional regulation; however, higher levels of fidelity to TST in children’s first quarter in KVC were associated with significantly greater improvements in emotional regulation. • In addition, TST fidelity in children’s first quarter in care, as well as increases in fidelity over time, were significantly associated with greater placement stability. • Increases across quarters in inner circle dosage (those who worked most closely with the children) were associated with significant improvements in children’s functioning and emotional regulation over time and increased placement stability. • Outer circle members’ implementation of TST in quarter one was significantly associated with improvements in functioning and placement stability. Limitations: Inability to randomly assign children to receive or not receive TST. The measure of TST dosage may not sensitively measure children’s level of exposure to TST. Reliance on secondary data to measure all outcomes. |
| Intensive Permanence Services (IPS) [24] | |
| Design: presented placement and relational outcome data from the initial pilot project in relation to 20 youth who had completed at least 13 months of the service. Measures: used discharge outcome data and the Youth Connections Scale (YCS) to measure relational permanence from time of service initiation and time of discharge. | Service User Outcomes • Of the young people who were involved in the pilot project and completed at least 13 months, 80% (n = 20) achieved legal permanency. Youth who were unable to complete IPS did not achieve legal permanency at this rate. Significant increase in scores on the Youth Connections Scale (YCS) from the time youth-initiated services to the time they were discharged. Limitations: small sample, no comparison group. |
| Evaluation Design and Measures | Training Outcomes and Limitations |
|---|---|
| Massachusetts Child Trauma Project [26] | |
| Design: Preliminary implementation and follow up evaluations using a multi-source, multi-method approach. For training, this included a single group pre-test/post-test training evaluation with 190 community mental health practitioners with one year follow up and 81% retention. Measures: training measured via Trauma-Informed System Change Instrument | Outcomes: • pre/post-test training evaluation found significant changes in perceptions of trauma-informed agency policy as well as perceptions of individual practices. Limitations: training outcomes self-reported only. |
| Arkansas Initiative [29,30] | |
| Design: Pre-test/multiple post-tests evaluation of training with child welfare leaders (n = 102, three month follow-up, retention 78%), with all child welfare staff (n = 438, follow up immediately after training, retention 93%) and a random sample of child welfare staff (n = 161, three month follow up, retention 88%). Additionally, half of the child welfare staff who were followed at three months were asked to complete a longer interview that asked about their success in implementing the action steps listed on their individualized plan developed at the end of training (n = 68). Measures: knowledge of trauma-informed practice and self-reported use of trauma-informed practices measured via questionnaire developed by authors. | Outcomes: • Significant increases in child welfare leaders’ knowledge about trauma-informed practice between pre-test and immediately post-test. • Significant increases in child welfare leaders’ self-reported use of trauma-informed practices between pre-test and three-month follow-up. • Child welfare staff’s knowledge of trauma-informed practice increased significantly between pre-test and post-test, as did self-reported changes in practice, although effect sizes were small when it came to direct support services for children and moderate for indirect support services. • 43.3% reported that they were able to fully implement trauma-informed strategies identified at training, while another 43.3% were partially implemented and 13.4% were unable to implement the strategy. Limitations: short follow-up period and outcomes based on self-reporting. |
| The Connecticut Collaborative on Effective Practices for Trauma (CONCEPT) [31] | |
| Design: pre-test/post-test with a stratified random sample of child welfare staff: 223 staff (45.2% response rate) completed the survey in Year 1 (pre-implementation) and 231 staff (46.5% response rate) completed the survey in Year 3. Measures: Perceptions of individual and agency capacity to provide trauma-informed care, measured via Trauma System Readiness Tool. Perceptions of individual and agency capacity to provide trauma-informed care. | Outcomes: • perceptions of individual and agency capacity to provide trauma-informed care increased significantly for 11 of the 12 domains. Limitations: response rate less than 50% for pre-test and post-test, based on self-reporting. |
| Creating Connections [28] | |
| Design: pre-test/multiple post-tests evaluation of training with staff conducting screening (n = 44, with follow-up immediately after training and at six months, retention 70.5%) and child welfare staff (n = 71, follow up immediately after training with child welfare). Measures: self-reported knowledge and skills gained via questionnaire developed by intervention developers. | Outcomes: • Screening staff knowledge and skills for administering the screening tools increased significantly and was retained at six-months follow-up. • Child welfare professionals self-reported competency scores on nearly all items, including the total item score, significantly improved from pre- to post-training Limitations: no longer-term follow up for child welfare staff training, all findings based on self-reporting. |
| Child Advocacy Centres Florida [36] | |
| Design: pre-test/multiple post-test design to evaluate training with staff who participated in training (n = 203, follow-up immediately post training and at one year, retention 12%). Measures: knowledge about trauma-informed care via questionnaire developed by intervention developers. | Outcomes: • knowledge about trauma-informed care increased significantly between pre- and immediately post-training and was retained after one year. Limitations: 12% pre-test/one-year post-test follow-up, poor retention rate. |
| Lemonade for Life [34] | |
| Design: Pre/post-test evaluation of pilot training with home visitors and parent educators in Kansas and Iowa (n = 17, follow up approximately six weeks after training completion, retention 71%). Measures: survey data, included items from the Hope Scale and Lemonade for Life-specific questions including: demographic information; participant experiences with ACEs personally and professionally; participant perceptions of using Adverse Childhood Experiences (ACEs) in work with families. | Outcomes: • Mean scores increased from pre to post in several areas: understanding how early experiences influence life course; home visitors’ knowledge of and self-reflection on their own ACEs score; and, knowing where to refer someone who is struggling with childhood adversity. The mean score on both Hope items (“I have the power to make my future better” and “I make others feel excited about the future”) decreased from pre to post—this was a new concept which may have led to a more realistic view evaluation of their own perspectives. Limitations: small sample, largely self-reported, only portions of the Hope Scale were used, no family outcomes. |
| KVC Kansas [27] | |
| Design: evaluation of fidelity to the Trauma Systems Therapy (TST) model following training based on training dates and fidelity scores of children’s care teams (caregivers, family service coordinators, caseworkers, supervisors and therapists) collected quarterly over three years of model implementation. Measures: researcher developed TST fidelity measures used to assess staff fidelity to TST implementation at quarterly basis; child functioning was assessed by children’s caseworkers using the Child and Adolescent Functioning Assessment Scale (every 90 days), the Child Ecology Check-In (monthly basis); administrative placement history data were used to calculate children’s placement stability; fidelity scores and TST training dates of children’s care teams were used to calculate the level of TST or “dosage” that children received. | Outcomes: • 384 KVC staff members were trained during the course of the first formal trainings and approximately 69% of KVC’s 397 foster parents over the course of the study period. • Average TST “dosage” scores for each member of children’s care-teams indicate that on average from 2012 to 2014 KVC staff implemented TST with increasing fidelity, with the average dosage score for children’s care teams steadily increasing from 7.95 (SD = 2.25; out of 30) at the start of the roll-out (first quarter of 2012) to 20.77 (SD = 5.67) at the last quarter of 2014. Limitations: based on self-report. |
| Training for Adoption Competency (TAC) [33] | |
| Design: Evaluation of training fidelity using observation and feedback and pre/post-test evaluation of training outcome which involved 855 participants including mental health professionals, public and private mental health agencies, adoption-specialty organizations, family service agencies, private practices, child welfare agencies residential treatment facilities and other settings. Training outcomes assessed mid training and end of training—timing not specified. Reference to control group but details not provided. Measures: training outcomes measured/assessed via mid training and end of training surveys of participants and a self-assessment of adoption competency administered at the conclusion of the modules as a retrospective pre- and post-assessment.; training fidelity assessed using fidelity observations and feedback from participants and trainers to assess the quality and relevance of training and the fidelity of curriculum delivery. | Outcomes: • More than 300 fidelity observations of training delivery across 59 cohorts confirm full delivery, with fidelity, of nearly 100% of all content of all modules • TAC participants experienced an average gain in pre- to post-test scores of 46.08 points, while those in the control groups of comparably qualified professionals experienced a gain of only 1.58 points. • There was not a statistically significant difference in test scores between participant and control groups at pre-test. • There was a significant interaction between the training and time on test scores. • Based on 1148 responses containing 4928 separate narrative descriptions of the ways practices were influenced by the training, all TAC participants reported change in at least two of the six defined aspects of practice; 59.88% reported change in all five aspects at the individual clinician level and 51.75% reported that TAC influenced the procedures, programming and/or services in their organization. Limitations: measures of training outcomes and changes in practice primarily self-report, details of controls not provided and sample size not always clear. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bunting, L.; Montgomery, L.; Mooney, S.; MacDonald, M.; Coulter, S.; Hayes, D.; Davidson, G. Trauma Informed Child Welfare Systems—A Rapid Evidence Review. Int. J. Environ. Res. Public Health 2019, 16, 2365. https://doi.org/10.3390/ijerph16132365
Bunting L, Montgomery L, Mooney S, MacDonald M, Coulter S, Hayes D, Davidson G. Trauma Informed Child Welfare Systems—A Rapid Evidence Review. International Journal of Environmental Research and Public Health. 2019; 16(13):2365. https://doi.org/10.3390/ijerph16132365
Chicago/Turabian StyleBunting, Lisa, Lorna Montgomery, Suzanne Mooney, Mandi MacDonald, Stephen Coulter, David Hayes, and Gavin Davidson. 2019. "Trauma Informed Child Welfare Systems—A Rapid Evidence Review" International Journal of Environmental Research and Public Health 16, no. 13: 2365. https://doi.org/10.3390/ijerph16132365