Association between Breakfast Frequency and Atherosclerotic Cardiovascular Disease Risk: A Cross-Sectional Study of KNHANES Data, 2014–2016



Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection and Participants
2.2. Dependent Variable
2.3. Independent Variable
2.4. Control Variables
2.5. Statistical Analysis
3. Results
3.1. Study Population
3.2. Association between Breakfast Frequency and ASCVD Risk
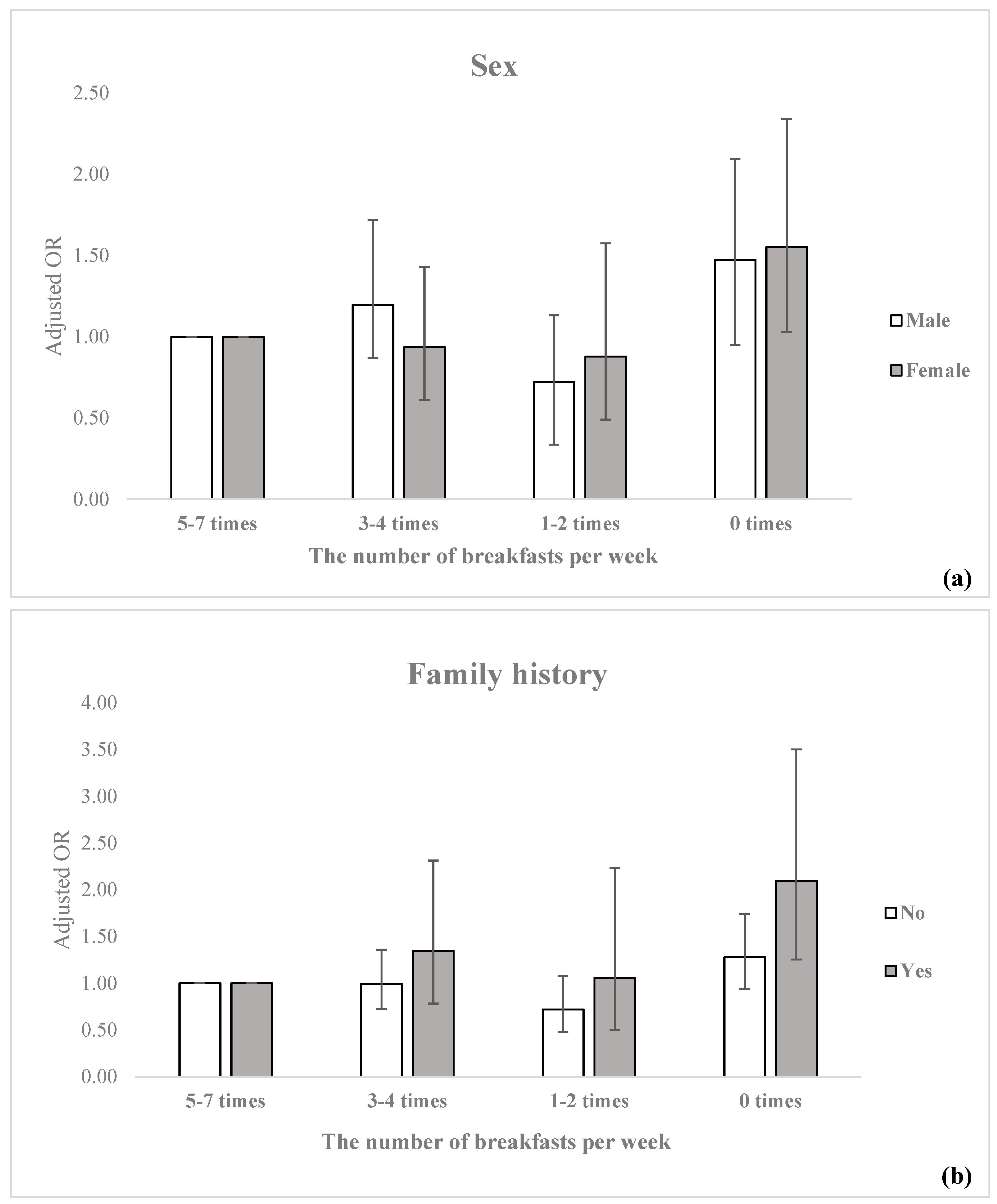
3.3. Association between ASCVD High-Risk and Breakfast Frequency Stratified by Sex and Family History
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization World Heart Day 2017. Available online: http://www.who.int/cardiovascular_diseases/world-heart-day-2017/en/ (accessed on 25 May 2019).
- Korean Statistical Information Service Cause of death statistics. Available online: http://kosis.kr/statHtml/statHtml.do?orgId=101&tblId=DT_1B34E01&vw_cd=MT_ZTITLE&list_id=D11&seqNo=&lang_mode=ko&language=kor&obj_var_id=&itm_id=&conn_path=MT_ZTITLE# (accessed on 25 May 2019).
- Son, M.; Seong, S. National Health Insurance Statistical Yearbook; Health Insurance Review and Assessment Service, National Health Insurance Service: Wonju, Korea, 2016. [Google Scholar]
- Mokdad, A.H.; Ford, E.S.; Bowman, B.A.; Dietz, W.H.; Vinicor, F.; Bales, V.S.; Marks, J.S. Prevalence of obesity, diabetes, and obesity-related health risk factors, 2001. JAMA 2003, 289, 76–79. [Google Scholar] [CrossRef] [PubMed]
- Damen, J.A.; Hooft, L.; Schuit, E.; Debray, T.P.; Collins, G.S.; Tzoulaki, I.; Lassale, C.M.; Siontis, G.C.; Chiocchia, V.; Roberts, C. Prediction models for cardiovascular disease risk in the general population: Systematic review. BMJ 2016, 353, i2416. [Google Scholar] [CrossRef] [PubMed]
- Goff, D.C.; Lloyd-Jones, D.M.; Bennett, G.; Coady, S.; D’Agostino, R.B.; Gibbons, R.; Greenland, P.; Lackland, D.T.; Levy, D.; O’Donnell, C.J. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2014, 63, 2935–2959. [Google Scholar] [CrossRef] [PubMed]
- Muntner, P.; Colantonio, L.D.; Cushman, M.; Goff, D.C.; Howard, G.; Howard, V.J.; Kissela, B.; Levitan, E.B.; Lloyd-Jones, D.M.; Safford, M.M. Validation of the Atherosclerotic Cardiovascular Disease Pooled Cohort Risk EquationsCardiovascular Disease Risk EquationsCardiovascular Disease Risk Equations. JAMA 2014, 311, 1406–1415. [Google Scholar] [CrossRef]
- World Health Organization. Prevention of Cardiovascular Disease; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Kant, A.K.; Schatzkin, A.; Graubard, B.I.; Schairer, C. A prospective study of diet quality and mortality in women. JAMA 2000, 283, 2109–2115. [Google Scholar] [CrossRef]
- O’Neil, C.E.; Byrd-Bredbenner, C.; Hayes, D.; Jana, L.; Klinger, S.E.; Stephenson-Martin, S. The role of breakfast in health: Definition and criteria for a quality breakfast. J. Acad. Nutr. Diet. 2014, 114, S8–S26. [Google Scholar]
- Keski-Rahkonen, A.; Kaprio, J.; Rissanen, A.; Virkkunen, M.; Rose, R.J. Breakfast skipping and health-compromising behaviors in adolescents and adults. Eur. J. Clin. Nutr. 2003, 57, 842. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health and Welfare. Korea Health Promotion Foundation. Health Plan 2020 (2016–2020); Korea Health Promotion Foundation: Seoul, Korea, 2015. [Google Scholar]
- Korea Centers for Disease Control and Prevention. Korea Health Statistics 2016: Korea National Health and Nutrition Examination Survey (KNHANES Ⅶ-1); Korea Centers for Disease Control and Prevention: Sejong Cheongju, Korea, 2017. [Google Scholar]
- O’Neil, C.E.; Nicklas, T.A.; Fulgoni, V.L., III. Nutrient intake, diet quality, and weight/adiposity parameters in breakfast patterns compared with no breakfast in adults: National Health and Nutrition Examination Survey 2001–2008. J. Acad. Nutr. Diet. 2014, 114, S27–S43. [Google Scholar]
- Drewnowski, A.; Rehm, C.; Vieux, F. Breakfast in the United States: Food and Nutrient Intakes in Relation to Diet Quality in National Health and Examination Survey 2011–2014. A Study from the International Breakfast Research Initiative. Nutrients 2018, 10, 1200. [Google Scholar] [CrossRef] [PubMed]
- Haines, P.S.; Guilkey, D.K.; POPKIN, B. Trends in breakfast consumption if US adults between 1965 and 1991. J. Am. Diet. Assoc. 1996, 96, 464–470. [Google Scholar] [CrossRef]
- Lee, S.A.; Park, E.-C.; Ju, Y.J.; Lee, T.H.; Han, E.; Kim, T.H. Breakfast consumption and depressive mood: A focus on socioeconomic status. Appetite 2017, 114, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Odegaard, A.O.; Jacobs, D.R.; Steffen, L.M.; Van Horn, L.; Ludwig, D.S.; Pereira, M.A. Breakfast frequency and development of metabolic risk. Diabetes Care 2013, 36, 3100–3106. [Google Scholar] [CrossRef] [PubMed]
- Yoo, K.-B.; Suh, H.-J.; Lee, M.-J.; Kim, J.-H.; Kwon, J.A.; Park, E.-C. Breakfast eating patterns and the metabolic syndrome: The Korea National Health and Nutrition Examination Survey (KNHANES) 2007–2009. Asia Pac J Clin Nutr. 2014, 23, 128–137. [Google Scholar] [PubMed]
- Cahill, L.E.; Chiuve, S.E.; Mekary, R.A.; Jensen, M.K.; Flint, A.J.; Hu, F.B.; Rimm, E.B. Prospective study of breakfast eating and incident coronary heart disease in a cohort of male US health professionals. Circulation 2013, 128, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Yokoyama, Y.; Onishi, K.; Hosoda, T.; Amano, H.; Otani, S.; Kurozawa, Y.; Tamakoshi, A. Skipping breakfast and risk of mortality from cancer, circulatory diseases and all causes: Findings from the Japan Collaborative Cohort Study. Yonago Acta Med. 2016, 59, 55. [Google Scholar]
- Yim, K.S. Effects of Lifestyle and Dietary Behavior on Cardiovascular Risks in Middle-aged Korean Men. J. Community Nutr. 2000, 2, 119–128. [Google Scholar]
- Kubota, Y.; Iso, H.; Sawada, N.; Tsugane, S.; Group, J.S. Association of breakfast intake with incident stroke and coronary heart disease: The Japan Public Health Center-Based Study. Stroke 2016, 47, 477–481. [Google Scholar] [CrossRef]
- Jung, C.-H.; Lee, J.S.; Ahn, H.J.; Choi, J.-S.; Noh, M.Y.; Lee, J.J.; Lee, E.Y.; Lim, J.H.; Lee, Y.R.; Yoon, S.Y. Association of meal frequency with metabolic syndrome in Korean adults: From the Korea National Health and Nutrition Examination Survey (KNHANES). Diabetol. Metab. Syndr. 2017, 9, 77. [Google Scholar] [CrossRef]
- Ashok, P.; Kharche, J.S.; Raju, R.; Godbole, G. Metabolic equivalent task assessment for physical activity in medical students. Natl. J. Physiol. Pharm. Pharmacol. 2017, 7, 236. [Google Scholar] [CrossRef]
- Kim, H.R. Quality of Diet and Nutritional Intake and Mortality Risk among South Korean Adults Based on 12-year Follow-up Data. Korean J. Community Nutr. 2016, 21, 354–365. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.S.; Kim, H.Y.; Hwang, J.Y.; Kwon, S.; Chung, H.R.; Kwak, T.-K.; Kang, M.H.; Choi, Y.S. Development of Nutrition Quotient for Korean adults: Item selection and validation of factor structure. J. Nutr. Health 2018, 51, 340–356. [Google Scholar] [CrossRef]
- Barr, S.I.; DiFrancesco, L.; Fulgoni, V.L. Association of breakfast consumption with body mass index and prevalence of overweight/obesity in a nationally-representative survey of Canadian adults. Nutri. J. 2015, 15, 33. [Google Scholar] [CrossRef] [Green Version]
- Kant, A.K.; Andon, M.B.; Angelopoulos, T.J.; Rippe, J.M. Association of breakfast energy density with diet quality and body mass index in American adults: National Health and Nutrition Examination Surveys, 1999–2004. Am. J. Clin. Nutr. 2008, 88, 1396–1404. [Google Scholar]
- Song, W.O.; Chun, O.K.; Obayashi, S.; Cho, S.; Chung, C.E. Is consumption of breakfast associated with body mass index in US adults? J. Am. Diet. Assoc. 2005, 105, 1373–1382. [Google Scholar] [CrossRef]
- Mohiuddin, A. Skipping Breakfast Everyday Keeps Well-Being Away. J. Dairy Sci. Technol. 2019, 7, 20–30. [Google Scholar]
- Witbracht, M.; Keim, N.L.; Forester, S.; Widaman, A.; Laugero, K. Female breakfast skippers display a disrupted cortisol rhythm and elevated blood pressure. Physiol. Behav. 2015, 140, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Deshmukh-Taskar, P.; Nicklas, T.A.; Radcliffe, J.D.; O’Neil, C.E.; Liu, Y. The relationship of breakfast skipping and type of breakfast consumed with overweight/obesity, abdominal obesity, other cardiometabolic risk factors and the metabolic syndrome in young adults. The National Health and Nutrition Examination Survey (NHANES): 1999–2006. Public Health Nutr. 2013, 16, 2073–2082. [Google Scholar]
- Mosca, L.; Barrett-Connor, E.; Kass Wenger, N. Sex/gender differences in cardiovascular disease prevention: What a difference a decade makes. Circulation 2011, 124, 2145–2154. [Google Scholar] [CrossRef]
- Levitsky, D.A.; Pacanowski, C.R. Effect of skipping breakfast on subsequent energy intake. Physiol. Behav. 2013, 119, 9–16. [Google Scholar] [CrossRef]
- Chia, Y.C.; Lim, H.M.; Ching, S.M. Validation of the pooled cohort risk score in an Asian population—A retrospective cohort study. BMC Cardiovasc. Disord. 2014, 14, 163. [Google Scholar] [CrossRef] [PubMed]
- Park, S.Y.; Chin, S.O.; Rhee, S.Y.; Oh, S.; Woo, J.-T.; Kim, S.W.; Chon, S. Cardio-ankle vascular index as a surrogate marker of early atherosclerotic cardiovascular disease in Koreans with type 2 diabetes mellitus. Diabetes Metab. J. 2018, 42, 285–295. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.G. Cardiovascular Risk Prediction in Korean Adults. Korean J. Fam. Med. 2018, 39, 135–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, X.; Du, R.; Hu, C.; Cheng, D.; Ma, L.; Li, M.; Xu, Y.; Xu, M.; Chen, Y.; Li, D. Resting heart rate is associated with metabolic syndrome and predicted 10-Year risk of cardiovascular disease: A cross-sectional study. J. Diabetes 2019. [Google Scholar] [CrossRef] [PubMed]
- Lee, K. Muscle Mass and Body Fat in Relation to Cardiovascular Risk Estimation and Lipid-Lowering Eligibility. J. Clin. Densitom. 2017, 20, 247–255. [Google Scholar] [CrossRef]
- Kim, M.H.; Kim, Y.S.; Oh, H.J.; Kwon, Y.R.; Kim, H.W. The association between 10-year atherosclerotic cardiovascular diseases risk score calculated using 2013 American College of Cardiology/American Heart Association guidelines and serum 25-hydroxyvitamin D level among aged 40–79 years in Korea: The sixth Korea National Health and Nutrition Examination Surveys. Korean J. Fam. Med. 2018, 39, 174. [Google Scholar]
- Lin, L.; Long, W.; LIU, S.S.; ZHAO, Z.Y.; Mian, L.; WANG, T.G.; Min, X.; LU, J.L.; CHEN, Y.H.; WANG, S.Y. Association between Coronary Atherosclerotic Plaque Composition and Cardiovascular Disease Risk. Biomed. Environ. Sci. 2019, 32, 75–86. [Google Scholar]
- Satoh-Asahara, N.; Kotani, K.; Yamakage, H.; Yamada, T.; Araki, R.; Okajima, T.; Adachi, M.; Oishi, M.; Shimatsu, A.; Group, M.S.S.J. Cardio-ankle vascular index predicts for the incidence of cardiovascular events in obese patients: A multicenter prospective cohort study (Japan Obesity and Metabolic Syndrome Study: JOMS). Atherosclerosis 2015, 242, 461–468. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Total | ASCVD Risk | p-Value | ||||
|---|---|---|---|---|---|---|---|
| High-Risk | Normal | ||||||
| n | % | n | % | n | % | ||
| Breakfasts per week | <0.0001 | ||||||
| 5–7 times | 5589 | 77.6 | 2,414 | 43.2 | 3175 | 56.8 | |
| 3–4 times | 597 | 8.3 | 137 | 22.9 | 460 | 77.1 | |
| 1–2 times | 425 | 5.9 | 66 | 15.5 | 359 | 84.5 | |
| 0 times | 594 | 8.2 | 169 | 28.5 | 425 | 71.5 | |
| Sex | <0.0001 | ||||||
| Male | 2916 | 40.5 | 1726 | 59.2 | 1190 | 40.8 | |
| Female | 4289 | 59.5 | 1060 | 24.7 | 3229 | 75.3 | |
| Age | <0.0001 | ||||||
| 40-49 | 2158 | 30.0 | 154 | 7.1 | 2004 | 92.9 | |
| 50-59 | 2189 | 30.4 | 524 | 23.9 | 1665 | 76.1 | |
| >60 | 2858 | 39.7 | 2108 | 73.8 | 750 | 26.2 | |
| Marital status | <0.0001 | ||||||
| Married | 5930 | 82.3 | 2164 | 36.5 | 3766 | 63.5 | |
| Single, separated, or divorced | 1275 | 17.7 | 622 | 48.8 | 653 | 51.2 | |
| Educational level | <0.0001 | ||||||
| Middle school or less | 2757 | 38.3 | 1545 | 56.0 | 1212 | 44.0 | |
| High school | 2385 | 33.1 | 699 | 29.3 | 1686 | 70.7 | |
| College or over | 2063 | 28.6 | 542 | 26.3 | 1521 | 73.7 | |
| Household income level | <0.0001 | ||||||
| Low | 1298 | 18.0 | 823 | 63.4 | 475 | 36.6 | |
| Lower middle | 1810 | 25.1 | 796 | 44.0 | 1014 | 56.0 | |
| Upper middle | 1909 | 26.5 | 577 | 30.2 | 1332 | 69.8 | |
| High | 2188 | 30.4 | 590 | 27.0 | 1598 | 73.0 | |
| Occupation | <0.0001 | ||||||
| White collar | 1415 | 19.6 | 316 | 22.3 | 1099 | 77.7 | |
| Pink collar | 1008 | 14.0 | 203 | 20.1 | 805 | 79.9 | |
| Blue collar | 2033 | 28.2 | 957 | 47.1 | 1076 | 52.9 | |
| Unemployed or other | 2749 | 38.2 | 1310 | 47.7 | 1439 | 52.3 | |
| Region | <0.0001 | ||||||
| Urban area | 4472 | 62.1 | 1647 | 36.8 | 2825 | 63.2 | |
| Rural area | 2733 | 37.9 | 1139 | 41.7 | 1594 | 58.3 | |
| Alcohol status | <0.0001 | ||||||
| Non-drinker | 1003 | 13.9 | 480 | 47.9 | 523 | 52.1 | |
| Other | 6202 | 86.1 | 2306 | 37.2 | 3896 | 62.8 | |
| Perceived stress level | <0.0001 | ||||||
| Low | 5608 | 77.8 | 2284 | 40.7 | 3324 | 59.3 | |
| High | 1597 | 22.2 | 502 | 31.4 | 1095 | 68.6 | |
| Perceived health status | 0.0016 | ||||||
| Good | 2116 | 29.4 | 821 | 38.8 | 1295 | 61.2 | |
| Normal | 3752 | 52.1 | 1394 | 37.2 | 2358 | 62.8 | |
| Bad | 1337 | 18.6 | 571 | 42.7 | 766 | 57.3 | |
| Physical activity | 0.0001 | ||||||
| High | 1173 | 16.3 | 393 | 33.5 | 780 | 66.5 | |
| Moderate | 2990 | 41.5 | 1158 | 38.7 | 1832 | 61.3 | |
| Low | 3042 | 42.2 | 1235 | 40.6 | 1807 | 59.4 | |
| BMI (kg/m2) | <0.0001 | ||||||
| Underweight or Normal (<22.9) | 2810 | 39.0 | 953 | 33.9 | 1857 | 66.1 | |
| Overweight (23.0–24.9) | 1861 | 25.8 | 768 | 41.3 | 1093 | 58.7 | |
| Obesity (>25.0) | 2534 | 35.2 | 1065 | 42.0 | 1469 | 58.0 | |
| Family history | 0.0010 | ||||||
| No | 5539 | 76.9 | 2199 | 39.7 | 3340 | 60.3 | |
| Yes | 1666 | 23.1 | 587 | 35.2 | 1079 | 64.8 | |
| Nutritional status | <0.0001 | ||||||
| Good | 5284 | 73.3 | 1924 | 36.4 | 3360 | 63.6 | |
| Poor | 1921 | 26.7 | 862 | 44.9 | 1059 | 55.1 | |
| Calorie intake (kcal/day) * | 1973.6 | 861.5 | 1995.1 | 853.5 | 1960.0 | 866.3 | <0.0001 |
| Fat intake (g/day) * | 39.5 | 31.6 | 35.4 | 29.2 | 42.1 | 32.8 | <0.0001 |
| Carbohydrate intake (g/day) * | 313.7 | 127.7 | 325.7 | 133.1 | 306.0 | 123.6 | <0.0001 |
| Year | 0.7889 | ||||||
| 2014 | 2203 | 30.6 | 850 | 38.6 | 1353 | 61.4 | |
| 2015 | 2481 | 34.4 | 972 | 39.2 | 1509 | 60.8 | |
| 2016 | 2521 | 35.0 | 964 | 38.2 | 1557 | 61.8 | |
| Total | 7205 | 100.0 | 2786 | 38.7 | 4419 | 61.3 | |
| Variables | Total | |
|---|---|---|
| Adjusted OR * | 95% CI | |
| Breakfasts per week | ||
| 5–7 times | 1.00 | - |
| 3–4 times | 1.06 | (0.81–1.39) |
| 1–2 times | 0.78 | (0.55–1.11) |
| 0 times | 1.46 | (1.12–1.89) |
| Sex | ||
| Male | 1.00 | - |
| Female | 0.06 | (0.05–0.07) |
| Age | ||
| 40–49 | 0.02 | (0.01–0.02) |
| 50–59 | 0.09 | (0.08–0.11) |
| >60 | 1.00 | - |
| Marital status | ||
| Married | 1.00 | - |
| Single, separated, or divorced | 1.50 | (1.26–1.78) |
| Educational level | ||
| Middle school or less | 1.49 | (1.19–1.88) |
| High school | 1.21 | (0.99–1.49) |
| College or over | 1.00 | - |
| Household income level | ||
| Low | 1.61 | (1.29–2.03) |
| Lower middle | 1.15 | (0.94–1.40) |
| Upper middle | 0.98 | (0.81–1.19) |
| High | 1.00 | - |
| Occupation | ||
| White collar | 1.00 | - |
| Pink collar | 0.83 | (0.63–1.11) |
| Blue collar | 0.98 | (0.77–1.25) |
| Unemployed or other | 1.56 | (1.22–1.99) |
| Region | ||
| Urban area | 1.00 | - |
| Rural area | 1.11 | (0.96–1.28) |
| Alcohol status | ||
| Non–drinker | 1.00 | - |
| Other | 0.76 | (0.63–0.92) |
| Perceived stress level | ||
| Low | 1.00 | - |
| High | 0.97 | (0.83–1.15) |
| Perceived health status | ||
| Good | 1.00 | - |
| Normal | 1.01 | (0.86–1.19) |
| Bad | 0.80 | (0.65–0.99) |
| Physical activity | ||
| High | 1.00 | - |
| Moderate | 1.22 | (0.99–1.50) |
| Low | 1.40 | (1.14–1.72) |
| BMI (kg/m2) | ||
| Underweight or Normal (<22.9) | 1.00 | - |
| Overweight (23.0–24.9) | 1.11 | (0.93–1.32) |
| Obesity (>25.0) | 1.19 | (1.02–1.40) |
| Family history | ||
| No | 1.00 | - |
| Yes | 0.88 | (0.75–1.03) |
| Nutritional status | ||
| Good | 1.00 | - |
| Poor | 1.18 | (0.99–1.41) |
| Calorie intake (kcal/day) | 1.00 | (1.00–1.00) |
| Fat intake (g/day) | 1.00 | (1.00–1.00) |
| Carbohydrate intake (g/day) | 1.00 | (0.99–1.00) |
| Year | ||
| 2014 | 1.04 | (0.88–1.23) |
| 2015 | 0.98 | (0.83–1.16) |
| 2016 | 1.00 | - |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, H.J.; Jang, J.; Lee, S.A.; Choi, D.-W.; Park, E.-C. Association between Breakfast Frequency and Atherosclerotic Cardiovascular Disease Risk: A Cross-Sectional Study of KNHANES Data, 2014–2016. Int. J. Environ. Res. Public Health 2019, 16, 1853. https://doi.org/10.3390/ijerph16101853
Lee HJ, Jang J, Lee SA, Choi D-W, Park E-C. Association between Breakfast Frequency and Atherosclerotic Cardiovascular Disease Risk: A Cross-Sectional Study of KNHANES Data, 2014–2016. International Journal of Environmental Research and Public Health. 2019; 16(10):1853. https://doi.org/10.3390/ijerph16101853
Chicago/Turabian StyleLee, Hyeon Ji, Jieun Jang, Sang Ah Lee, Dong-Woo Choi, and Eun-Cheol Park. 2019. "Association between Breakfast Frequency and Atherosclerotic Cardiovascular Disease Risk: A Cross-Sectional Study of KNHANES Data, 2014–2016" International Journal of Environmental Research and Public Health 16, no. 10: 1853. https://doi.org/10.3390/ijerph16101853