Accessibility and Acceptability of Infectious Disease Interventions Among Migrants in the EU/EEA: A CERQual Systematic Review

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Selection Criteria
2.2. Study Selection and Data Extraction
2.3. Data Synthesis
3. Results
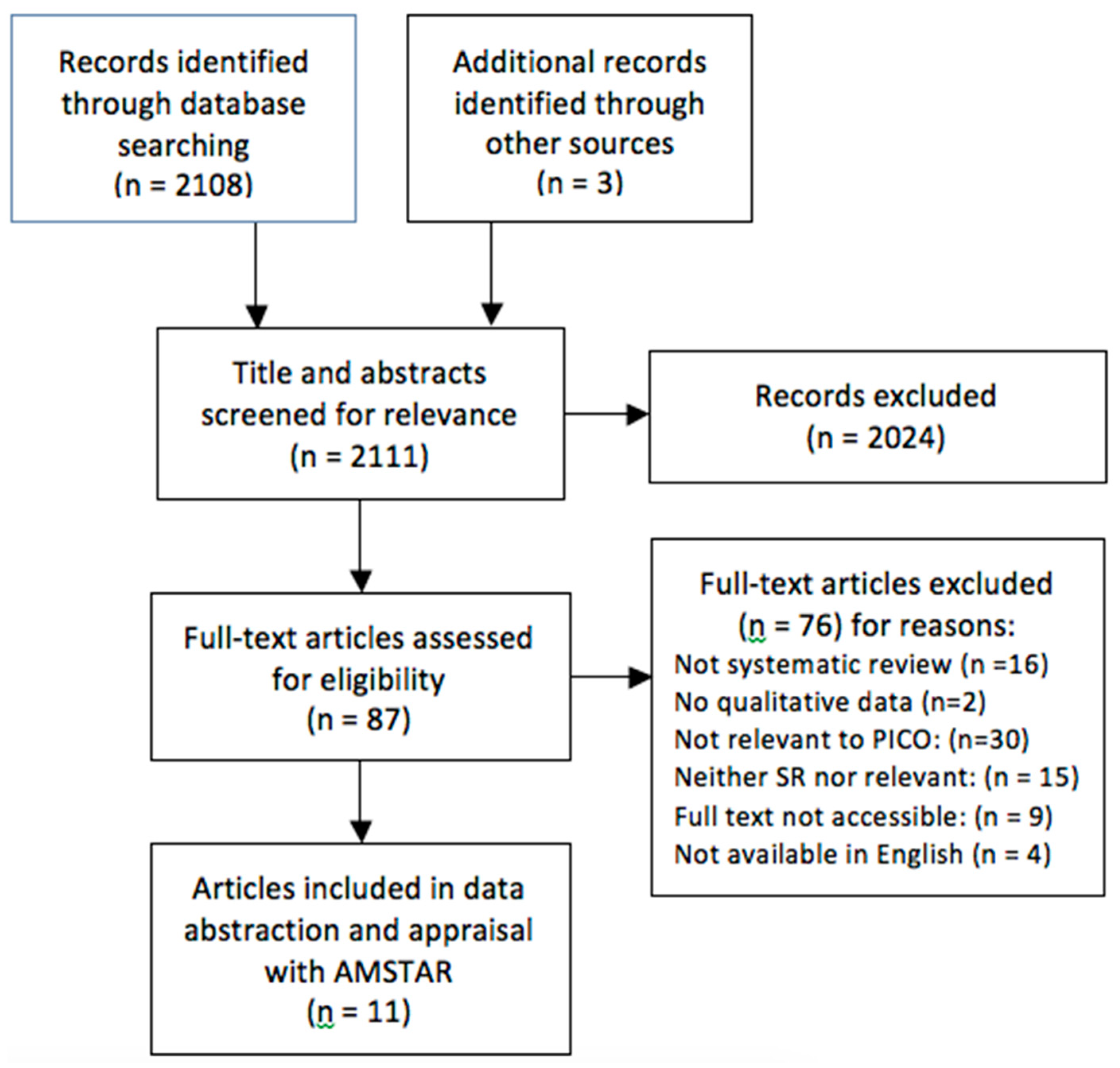
3.1. Study Selection
3.2. Methodological Quality
3.3. Migrants’ Perceptions of Acceptability
3.4. Migrants’ Values on Outcomes of Interventions
3.5. Accessibility of Health Services
3.6. Confidence in Findings
4. Discussion
4.1. Implications for Practice
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A. Determinants of Interest
- The importance placed upon the main outcomes of an intervention. These outcomes include those directly related to the disease (e.g., cure, symptom reduction, diagnosis), or costs or benefits resulting from the downstream effects of the intervention (e.g., side effects, time spent at the hospital, stigma, disclosure of disease status, cultural beliefs)
- The willingness of the patient to request or adhere to the intervention based on their subjective attitudes and preferences towards the intervention itself or the process of receiving it (e.g., adherence challenges, social/cultural attitudes, fears about the procedure)
- The ease with which patients use an infectious disease intervention. Determinants of accessibility include policies, community factors, healthcare service organization, or the delivery of the intervention itself.
Appendix B. Determinants of Interest
- Study design: Systematic reviews (qualitative or qualitative/quantitative) defined as any review that includes selection criteria, search strategy, and use of at least one database
- Time: Published after 1 January 2010
- Language: English language
- Relevant to the PICO question:
- Population: Migrants from Low- and Middle-Income Countries residing in High-Income Countries (i.e., permanent resettlement countries)
- Intervention: Prevention, screening, and treatment interventions for infectious diseases (tuberculosis, hepatitis, VPDs, HIV, parasitic diseases)
- Comparison: No intervention
- Outcome: Valuation of outcomes, views about acceptability and accessibility of interventions
Appendix C. Data Abstraction Tables

{kind=link}
| Citation |
|---|
| Disease |
| Knowledge of Disease Status |
| Behavioral Prevention |
| Vaccination |
| Treatment of Asymptomatic Disease |
| Cure of Symptomatic Disease |
| Citation |
|---|
| Demand-Side Determinants |
| User’s attitudes and Expectations |
| Household attitudes and expectations |
| Information on healthcare choice/providers |
| Disease-related knowledge |
| Intervention-related knowledge |
| Stigma |
| Indirect costs |
| Acculturation |
| SocialSupply-Side Determinants |
| Characteristics of the Health Services |
| Management/Staff Efficiency |
| Technology |
| Staff Interpersonal Skills, Including Trust |
| Wages and Quality of Staff |
| Language Barriers |
| Citations |
|---|
| Demand-Side Determinants |
| Indirect costs to household (e.g. transport, legal status) |
| Household income and willingness to pay |
| Opportunity costs |
| Means of transport available |
| System navigation |
| Low self-esteem and little assertivenessSupply-Side Determinants |
| Service/household location |
| Availablity of health workers, drugs, equipment |
| Direct price of service, including informal fees |
| Waiting time |
| Unqualified health woerks, absenteeism |
| Non-integration of health services |
| Lack of opportunity (exclusion from services) |
| Late or no referral |
References
- Mladovsky, P.; Shadwick, R.; Odone, A.; Ingleby, D.; Tillman, T.; Rechel, B.; McKee, M. Assessing the Burden of Key Infectious Diseases Affecting Migrant Populations in the EU/EEA; European Centre for Disease Prevention and Control: Stockholm, Sweden, 2014. [Google Scholar]
- Pottie, K.; Greenaway, C.; Feightner, J.; Welch, V.; Swinkels, H.; Rashid, M.; Narasiah, L.; Kirmayer, L.J.; Ueffing, E.; MacDonald, N.E. Evidence-based clinical guidelines for immigrants and refugees. CMAJ 2011, 183, E824–E925. [Google Scholar] [CrossRef] [PubMed]
- Chaves, N.; Biggs, B.A.; Thambiran, A.; Smith, M.; Williams, J.; Gardiner, J.; Davis, J.S. Recommendations for Comprehensive Post-Arrival Health Assessment for People from Refugee-Like Backgrounds; Australasian Society for Infectious Diseases and Refugee Health Network: Surrey Hills, Australia, 2016.
- HPSC Scientific Advisory Committee. Infectious Disease Assessment for Migrants; Health Protection Surveillance Centre: Dublin, Ireland, 2015. [Google Scholar]
- Alonso-Coello, P.; Oxman, A.D.; Moberg, J.; Brignardello-Petersen, R.; Akl, E.A.; Davoli, M.; Treweek, S.; Mustafa, R.A.; Vandvik, P.O.; Meerpohl, J. Grade evidence to decision (ETD) frameworks: A systematic and transparent approach to making well informed healthcare choices. 2: Clinical practice guidelines. BMJ 2016, 353, i2089. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agudelo-Suárez, A.A.; Gil-González, D.; Vives-Cases, C.; Love, J.G.; Wimpenny, P.; Ronda-Pérez, E. A metasynthesis of qualitative studies regarding opinions and perceptions about barriers and determinants of health services’ accessibility in economic migrants. BMC Health Serv. Res. 2012, 12, 461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gil-González, D.; Carrasco-Portino, M.; Vives-Cases, C.; Agudelo-Suarez, A.A.; Castejón Bolea, R.; Ronda-Pérez, E. Is health a right for all? An umbrella review of the barriers to health care access faced by migrants. Ethn. Health 2015, 20, 523–541. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Consolidated Guidelines on HIV Testing Services. Available online: http://www.who.int/hiv/pub/guidelines/hiv-testing-services/en/ (accessed on 1 August 2016).
- Lawson, E.; Calzavara, L.; Husbands, W.; Myers, T.; Tharao, W.E. HIV/AIDS Stigma, Denial, Fear and Discrimination: Experiences and Responses of People from African and Caribbean Communities in Toronto; African and Carribean Council on HIV/AIDS in Ontario (AACHO): Toronto, ON, Canada, 2006. [Google Scholar]
- Mitra, D.; Jacobsen, M.; O’Connor, A.; Pottie, K.; Tugwell, P. Assessment of the decision support needs of women from HIV endemic countries regarding voluntary HIV testing in Canada. Patient Educ. Couns. 2006, 63, 292–300. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.; Shommu, N.S.; Rumana, N.; Barron, G.R.; Wicklum, S.; Turin, T.C. Barriers to access of primary healthcare by immigrant populations in Canada: A literature review. J. Immigr. Minor. Health 2016, 18, 1522–1540. [Google Scholar] [CrossRef] [PubMed]
- Pottie, K.; Morton, R.; Greenaway, C.; Akl, E.; Rahman, P.; Zenner, D.; Pareek, M.; Tugwell, P.; Welch, V.; Meerpohl, J.; et al. Prevention and assessment of infectious diseases among children and adult migrants arriving to the European Union/European Economic Association: A protocol for a suite of systematic reviews for public health and health systems. BMJ Open 2017, 7, e014608. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schünemann, H.J.; Wiercioch, W.; Brozek, J.; Etxeandia-Ikobaltzeta, I.; Mustafa, R.A.; Manja, V.; Brignardello-Petersen, R.; Neumann, I.; Falavigna, M.; Alhazzani, W. GRADE evidence to decision (ETD) frameworks for adoption, adaptation, and de novo development of trustworthy recommendations: Grade-adolopment. J. Clin. Epidemiol. 2017, 81, 101–110. [Google Scholar] [CrossRef] [PubMed]
- Endnote Clarivate Analytics. Available online: endnote.com (accessed on 15 May 2016).
- Shea, B.J.; Hamel, C.; Wells, G.A.; Bouter, L.M.; Kristjansson, E.; Grimshaw, J.; Henry, D.A.; Boers, M. AMSTAR is a reliable and valid measurement tool to assess the methodological quality of systematic reviews. J. Clin. Epidemiol. 2009, 62, 1013–1020. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, B.; Bigdeli, M.; Annear, P.L.; Van Damme, W. Addressing access barriers to health services: An analytical framework for selecting appropriate interventions in low-income Asian countries. Health Policy Plan 2011, 27, 288–300. [Google Scholar] [CrossRef] [PubMed]
- Rosenstock, I.M.; Strecher, V.J.; Becker, M.H. The health belief model and HIV risk behavior change. Springer 1994, 2, 5–24. [Google Scholar] [CrossRef]
- Glanz, K.; Bishop, D.B. The role of behavioral science theory in development and implementation of public health interventions. Annu. Rev. Public Health 2010, 31, 399–418. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-del Arco, D.; Monge, S.; Azcoaga, A.; Rio, I.; Hernando, V.; Gonzalez, C.; Alejos, B.; Caro, A.; Perez-Cachafeiro, S.; Ramirez-Rubio, O.; et al. HIV testing and counselling for migrant populations living in high-income countries: A systematic review. Eur. J. Public Health 2013, 23, 1039–1045. [Google Scholar] [CrossRef] [PubMed]
- Pottie, K.; Vissandjée, B.; Grant, J. Human immunodeficiency virus. Evidence review for newly arriving immigrants and refugees. CMAJ 2010. [Google Scholar] [CrossRef]
- Rosenstock, I.M. Historical origins of the health belief model. Health Educ. Monogr. 1974, 4, 328–335. [Google Scholar] [CrossRef]
- Lewin, S.; Glenton, C.; Munthe-Kaas, H.; Carlsen, B.; Colvin, C.J.; Gülmezoglu, M.; Noyes, J.; Booth, A.; Garside, R.; Rashidian, A. Using qualitative evidence in decision making for health and social interventions: An approach to assess confidence in findings from qualitative evidence syntheses (GRADE-CERQual). PLoS Med. 2015, 12, e1001895. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blondell, S.J.; Kitter, B.; Griffin, M.P.; Durham, J. Barriers and facilitators to HIV testing in migrants in high-income countries: A systematic review. AIDS Behav. 2015, 19, 2012–2024. [Google Scholar] [CrossRef] [PubMed]
- Owiti, J.A.; Greenhalgh, T.; Sweeney, L.; Foster, G.R.; Bhui, K.S. Illness perceptions and explanatory models of viral hepatitis b & c among immigrants and refugees: A narrative systematic review. BMC Public Health 2015, 15, 151. [Google Scholar] [CrossRef] [Green Version]
- Tomás, B.A.; Pell, C.; Cavanillas, A.B.; Solvas, J.G.; Pool, R.; Roura, M. Tuberculosis in migrant populations: A systematic review of the qualitative literature. PLOS ONE 2013, 8, e82440. [Google Scholar]
- Greenaway, C.; Sandoe, A.; Vissandjee, B.; Kitai, I.; Gruner, D.; Wobeser, W.; Pottie, K.; Ueffing, E.; Menzies, D.; Schwartzman, K. Tuberculosis: Evidence review for newly arriving immigrants and refugees. CMAJ 2011, 183, E939–E951. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, E.M.; Shapiro, A.; Golub, J.; Kranzer, K.; Portocarrero, A.V.; Najlis, C.A.; Ngamvithayapong-Yanai, J.; Lönnroth, K. Acceptability of TB Screening among At-Risk and Vulnerable Groups: A Systematic Qualitative/Quantitative Literature Metasynthesis; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- de Vries, S.G.; Cremers, A.L.; Heuvelings, C.C.; Greve, P.F.; Visser, B.J.; Bélard, S.; Janssen, S.; Spijker, R.; Shaw, B.; Hill, R.A. Barriers and facilitators to the uptake of tuberculosis diagnostic and treatment services by hard-to-reach populations in countries of low and medium tuberculosis incidence: A systematic review of qualitative literature. Lancet Infect Dis. 2017, 17, e128–e143. [Google Scholar] [CrossRef]
- Do, T.N.; Nam, S. Knowledge, awareness and medical practice of Asian Americans/Pacific Islanders on chronic hepatitis B infection: Review of current psychosocial evidence. Pogon Sahoe Yongu 2011, 31, 341. [Google Scholar] [PubMed]
- Nguyen-Truong, C.K.; Lee-Lin, F.; Gedaly-Duff, V. Contributing factors to colorectal cancer and Hepatitis B screening among Vietnamese Americans. Oncol. Nurs. Forum. 2013, 40, 238–251. [Google Scholar] [CrossRef] [PubMed]
- Tankimovich, M. Barriers to and interventions for improved tuberculosis detection and treatment among homeless and immigrant populations: A literature review. J. Community Health Nurs. 2013, 30, 83–95. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Cheng, J.; Liu, Z.; Ma, J.; Li, J.; Wang, J.; Yang, K. Epidemiology, quality and reporting characteristics of meta-analyses of observational studies published in chinese journals. BMJ Open 2015, 5. [Google Scholar] [CrossRef] [PubMed]
- Kung, J.; Chiappelli, F.; Cajulis, O.O.; Avezova, R.; Kossan, G.; Chew, L.; Maida, C.A. From systematic reviews to clinical recommendations for evidence-based health care: Validation of revised assessment of multiple systematic reviews (R-AMSTAR) for grading of clinical relevance. Open Dent. J. 2010, 4, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Kleinman, A.; Benson, P. Anthropology in the clinic: The problem of cultural competency and how to fix it. PLoS Med. 2006, 3, e294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mota, L.; Mayhew, M.; Grant, K.J.; Batista, R.; Pottie, K. Rejecting and accepting international migrant patients into primary care practices: A mixed method study. Int. J. Migr. Health Soc. Care 2015, 11, 108–129. [Google Scholar] [CrossRef]
- Helman, C.G. Culture, Health and Illness, 5th ed.; CRC Press: Boca Raton, FL, USA, 2007. [Google Scholar]
- Farmer, P. Pathologies of Power: Health, Human Rights, and the New War on the Poor; University of California Press: Berkeley, CA, USA, 2004; ISSN 0520931475. [Google Scholar]
- Asylverfahrensbeschleunigungsgesetz (Act on the Acceleration of Asylum Procedures). Available online: http://www.bgbl.de/xaver/bgbl/start.xav?startbk=Bundesanzeiger_BGBl&jumpTo=bgbl115s1722.pdf (accessed on 20 July 2016).
- Kleinman, A.; Eisenberg, L.; Good, B. Culture, illness, and care: Clinical lessons from anthropologic and cross-cultural research. Ann. Intern. Med. 1978, 88, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Beach, M.C.; Price, E.G.; Gary, T.L.; Robinson, K.A.; Gozu, A.; Palacio, A.; Smarth, C.; Jenckes, M.W.; Feuerstein, C.; Bass, E.B.; et al. Cultural competency: A systematic review of health care provider educational interventions. Med. Care 2005, 43, 356–373. [Google Scholar] [CrossRef] [PubMed]
- Wallerstein, N.; Duran, B. Community-based participatory research contributions to intervention research: The intersection of science and practice to improve health equity. Am. J. Public Health 2010, 100, S40–S46. [Google Scholar] [CrossRef] [PubMed]
- Beach, M.C.; Gary, T.L.; Price, E.G.; Robinson, K.; Gozu, A.; Palacio, A.; Smarth, C.; Jenckes, M.; Feuerstein, C.; Bass, E.B. Improving health care quality for racial/ethnic minorities: A systematic review of the best evidence regarding provider and organization interventions. BMC Public Health 2006, 6, 104. [Google Scholar] [CrossRef] [PubMed]
- Grol, R. Improving the quality of medical care: Building bridges among professional pride, payer profit, and patient satisfaction. JAMA 2001, 286, 2578–2585. [Google Scholar] [CrossRef] [PubMed]
- Seedat, F.; Hargreaves, S.; Friedland, J.S. Engaging new migrants in infectious disease screening: A qualitative semi-structured interview study of UK migrant community health-care leads. PLOS ONE 2014, 9, e108261. [Google Scholar] [CrossRef] [PubMed]

| Citation | Years Searched | Population | Intervention/Service Setting | Analysis/Synthesis Approach | EU/EEA Settings Included? | 1’ Study Design | # of 1′ Studies | AMSTAR Score (/11) |
|---|---|---|---|---|---|---|---|---|
| Alvarez-del Arco et al. [20] | 2005–2009 | Migrants and ethnic minorities populations living in high-income countries Migrants were largely from sub-Saharan Africa and Latin America, (1) and other regions. | HIV testing and/or counselling in health and community settings | None specified-Narrative | Yes | Quantitative (25); mixed-methods (2); qualitative (6); literature reviews (4) | 37 | 1 |
| Blondell et al. [24] | 1997–2014 | Foreign-born: African, particularly Sub-Saharan, and Hispanic/Latino migrants were the most studied populations. | HIV screening, testing | None specified - narrative | Yes | quantitative (n = 21) (descriptive/non-randomized) and qualitative (n = 10). | 31 | 3 |
| de Vries et al. [29] | 2010–2017 (OECD countries); or 1990–2017 (EU, EEA, EU candidate countries) | Hard-to-reach populations including homeless, migrants, travelers (including Roma), refugees, others. 7/10 studies were of migrants only. One study included homeless, migrants, and drug users. | TB services of any kind | Thematic and content analysis | Yes | Qualitative: Interviews (6), focus groups (2), both Interviews and Focus groups (3) multi-method participatory research (1) | 12 | 7 |
| Do et al. [30] | 2002–2009 | Asian Americans and Pacific Islanders (69% foreign-born). | Health education, screening, and vaccination for HBV | None specified - narrative | No | Cross-sectional (13); RCT (1); quasi-experimental (1); Longitudinal (1) | 20 | 1 |
| Greenaway et al. [27] | 1950 to 17 December 2008) * | Immigrants (subgroup). | Screening and treatment of latent TB | Summary of findings table (GRADE) | Not specified | SRs (7) and guidelines (2) | 9 | 2 |
| Mitchell et al. [28] | 1985–April 2011 | 30 individual risk groups * Data extracted from two groups only—Internally Displaced Populations (IDPs), and “Migrants/Immigration” | TB screening (CXR, Mantoux TST) | Metasynthesis | Yes | Qualitative and Quantitative literature. | 21 | 2 |
| Nguyen-Truong et al. [31] | 1998–2012 | Vietnamese Americans—most studies report that majority of sample are immigrants, but most aggregated immigrant and native-born. | Screening (HBV and Colorectal cancer) | None specified | No | Descriptive (15); Interventional (2); Qualitative (3); Chart/medical record review (2); Mixed-method (1) | 23 | 2 |
| Owiti et al. [25] | 1970–2014 ** | High-risk 1st- or 2nd-gen immigrants from high-prevalence countries or intermediate prevalence countries who migrated to traditionally low prevalence countries. | Knowledge of HBV and/or HCV infections and/or with targeted screening, vaccination, and treatment | Narrative synthesis | Yes | Quantitative surveys (39) and qualitative studies (11); mixed-methods (1) | 51 | 6 |
| Pottie et al. [21] | 1995–2008 | Immigrants and refugees (subgroup). | HIV Screening and treatment | Summary of findings table (GRADE) | Not specified | SRs (7) and guidelines (2) | 8 | 4 |
| Tankimovich et al. [32] | 1998–2012 | Homeless and immigrants with TB. | TB detection and treatment (active and latent) | None specified—narrative | Yes | Quantitative (17); Qualitative (5); Intervention studies (10) | 22 | 2 |
| Tomas et al. [26] | 1995–2011 | Immigrants, and intra-national migrants and including migrants, asylum-seekers, refugees. | Screening and treatment of TB (active and latent) | Meta-ethnography | Yes | In-depth interviews (24); focus groups (12); participant observation (5); case studies (1); Other (6) Many combined qualitative and quantitative methods. | 30 | 3 |
| Main Theme | Reviews Cited (Lead Authors) | Disease-Specific Supporting Examples | |
|---|---|---|---|
| Knowledge of Risk Factors | Low level of knowledge of risk factors and transmission of disease may make migrants less likely to seek screening, immunization, or treatment. | (5) de Vries, Owiti, Lee, Nguyen, Blondell | TB:
|
| Perceived Susceptibility | Low perceived personal risk of acquiring an infectious disease may make migrants less likely to seek screening | (3) Greenaway, Pottie, Alvarez |
|
| Perceived Severity | The severity and consequences (medical, social, economic) of diseases varied between studies, were generally well understood. However, the literature is divided on whether this is a motivating factor, or a perceived barrier to screening (i.e. risk of realizing the negative consequences through screening). | (4) Blondell, Lin, de Vries, Owiti) | Tuberculosis:
|
| Perceived Benefits | Several distinct, tangible benefits to screening, vaccination, and treatment were reported by reviews, especially reassurance of negative status and prevention of spread to others. | (4) Tomas, Do, Pottie Blondell, | Tuberculosis:
|
| Perceived Barriers | Stigma is an overarching barrier to screening and treatment that was reflected in most diseases and reviews. Stigma is also related to other perceived barriers (e.g. confidentiality issues with interpreters, hesitancy to report symptoms to family/healthcare providers) | (8) Tomas, Tankimovich, de Vries, Greenaway, Pottie, Owiti, Blondell, Alvarez, | Tuberculosis:
|
| Time spent accessing healthcare can incur a significant opportunity cost on migrants, especially when they are in a precarious employment situation or do not have basic needs met in their settlement process. | (6) Tomas, Greenaway, de Vries, Mitchell, Blondell, Alvarez | Tuberculosis:
| |
| Indirect costs that may be unique to migrants can reduce the value placed on these screening and treatment interventions. The most prominent of these was that a positive test result may have a negative impact on the migrant’s immigration status or refugee claim. | (5) Lin, Tankimovich, Blondell, Alvarez de Vries, | Tuberculosis:
| |
| Factors inherent to the migration process, including language proficiency, cultural barriers, and navigation of the healthcare system, can create barriers for migrants. However, reviews reported conflicting results regarding the influence of acculturation and language proficiency | (9) Tomas, Lin, Do, Owiti, Pottie, Blondell, Greenaway, de Vries, Alvarez, | Tuberculosis
| |
| Various attitudes and expectations of the intervention itself (the procedure or its side effects) may influence its acceptability among migrants | (4) Greenaway, Lin, Blondell, Tomas | Tuberculosis
| |
| Cues to Action | Recommendation from healthcare providers can influence healthcare seeking by migrant patients. | (3) Owiti, Do, Nguyen | HBV/HCV
|
| The importance of the patient-physician relationship was consistently emphasized. Trust, cultural sensitivity, and communication skills can act as facilitators to the acceptability of infectious disease interventions, whereas a negative relationship can serve as a barrier. | (7) Tomas, Greenaway, Mitchel, de Vries, Do, Nguyen, Owiti | Tuberculosis
| |
| The presence of symptoms can be a necessary cue to seeking healthcare among migrants who may not understand or value the importance of treating asymptomatic disease | (5) Tomas, Do, Blondell, de Vries, Nguyen | TB
|
| Key Finding | Studies Supporting Key Finding | Methodological Quality | Relevance-Research Question | Relevance-Population | Coherence | Adequacy-Reviews | Adequacy-Primary Studies | Overall Assessment of Confidence | Explanation of Judgement |
|---|---|---|---|---|---|---|---|---|---|
| Subjects may be reluctant to undergo screening due to negative indirect costs of having a positive result—on employment status, immigration status, and social status | [20,21,24,26,29,32] | Moderate methodological concerns | No relevance concernsFull (6/6) | Moderate relevance concerns Full (3/6) partial (3/6) | Minor coherence concerns Coherent (5/6) Among Latino migrants in Spain, legal and administrative fears were not found to be significant barriers [29] | Minor adequacy concerns 6 reviews | 20 studies | Low confidence | Lack of adequate evidence, including contradictory evidence, in addition to methodological concerns among reviews reporting this finding. |
| Patients value testing and treatment less if they are asymptomatic | [24,26,29,30,31] | Moderate methodological concerns | Minor relevance concerns Full (4/5) Indirect (1/5) | Moderate relevance concerns Full (2/5) Partial (3/5) | No coherence concerns Coherent (5/5) | Minor adequacy concerns 5 reviews | 25 studies | Low confidence | Methodological concerns, indirect/partial relevance of reviews supporting key finding. |
| Incorrect knowledge of infectious diseases and low self-perceived risk are barriers to acceptability of screening and vaccination | [20,21,24,25,26,27,28,29,30,31,32] | Moderate methodological concerns | Minor relevance concerns Full (8/11) Indirect (3/11) | Moderate relevance concerns Full (8/11) Partial (3/11) | Minor coherence concerns Coherent (10/11) Perceiving tuberculosis as a severe disease (OR 0.29, 95% CI 0.09-0.91) was associated with refusal of TST screening [28] | Minor adequacy concerns11 reviews | 81 studies | Moderate confidence | Some reviews have significant methodological concerns, yet the key finding is consistently supported by directly relevant data in reviews with only minor methodological concerns. |
| The acceptability of screening and treatment interventions is highly dependent on the cultural sensitivity and relationship with healthcare professionals | [20,21,24,25,26,27,28,29,30,31,32] | Moderate methodological concerns | Minor relevance concerns Full (10/11) Indirect (1/11) | Minor relevance concerns Full (8/11) Partial (3/11) | No coherence concerns Coherent (11/11) | Minor adequacy concerns 11 reviews | 67 studies | Moderate confidence | Supported by all reviews. Although some reviews have significant methodological concerns, reviews with few methodological concerns report directly relevant data. |
| Stigma associated with infectious diseases is a barrier to the acceptability of screening interventions | [20,21,24,25,26,27,29] | Moderate methodological concerns | No relevance concerns Full (7/7) | Minor relevance concerns Full (6/7) Partial (1/7) | Minor coherence concerns Coherent (6/7) Stigma is not a significant factor in all studies. Two quantitative studies on stigma found it was not a significant deterrent to testing | Minor adequacy concerns 7 reviews | 71 studies | Moderate confidence | Well-supported by review data that is directly relevant. Direct support from reviews with few methodological concerns. |
| Key Finding | CERQual Assessment Rating for Assessment of Confidence | Explanation of Confidence Rating |
|---|---|---|
| Incorrect knowledge of infectious diseases and low self-perceived risk are barriers to acceptability of screening and vaccination | Moderate confidence | Some reviews have significant methodological concerns, yet the key finding is consistently supported by directly relevant data in reviews with only minor methodological concerns. |
| The acceptability of screening and treatment interventions is highly dependent on the cultural sensitivity and sense of trust in healthcare professionals and their recommendations | Moderate confidence | Supported by all reviews. Although some reviews have significant methodological concerns, reviews with few methodological concerns report directly relevant data. |
| Stigma associated with infectious diseases is a barrier to the acceptability of screening interventions | Moderate confidence | Well-supported by review data that is directly relevant. Direct support from reviews with only mild methodological concerns. |
| Subjects may be reluctant to undergo screening due to negative indirect costs of having a positive result—on employment status, immigration status, and social status | Low confidence | Lack of adequate evidence, including contradictory evidence, in addition to methodological concerns among reviews reporting this finding. |
| Patients value testing and treatment less if they are asymptomatic | Low confidence | Methodological concerns, indirect/partial relevance of reviews supporting key finding. |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Driedger, M.; Mayhew, A.; Welch, V.; Agbata, E.; Gruner, D.; Greenaway, C.; Noori, T.; Sandu, M.; Sangou, T.; Mathew, C.; et al. Accessibility and Acceptability of Infectious Disease Interventions Among Migrants in the EU/EEA: A CERQual Systematic Review. Int. J. Environ. Res. Public Health 2018, 15, 2329. https://doi.org/10.3390/ijerph15112329
Driedger M, Mayhew A, Welch V, Agbata E, Gruner D, Greenaway C, Noori T, Sandu M, Sangou T, Mathew C, et al. Accessibility and Acceptability of Infectious Disease Interventions Among Migrants in the EU/EEA: A CERQual Systematic Review. International Journal of Environmental Research and Public Health. 2018; 15(11):2329. https://doi.org/10.3390/ijerph15112329
Chicago/Turabian StyleDriedger, Matt, Alain Mayhew, Vivian Welch, Eric Agbata, Doug Gruner, Christina Greenaway, Teymur Noori, Monica Sandu, Thierry Sangou, Christine Mathew, and et al. 2018. "Accessibility and Acceptability of Infectious Disease Interventions Among Migrants in the EU/EEA: A CERQual Systematic Review" International Journal of Environmental Research and Public Health 15, no. 11: 2329. https://doi.org/10.3390/ijerph15112329