The Associations among Psychological Distress, Coping Style, and Health Habits in Japanese Nursing Students: A Cross-Sectional Study

Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Participants and Data Collection
2.3. Content of the Questionnaires
2.3.1. The 12-Item General Health Questionnaire
2.3.2. Brief Coping Orientation Questionnaire
2.3.3. Health Habits
2.4. Ethical Considerations
2.5. Data Analysis
3. Results
3.1. Descriptive Analysis
3.2. Correlations Between Variables
3.3. Associations between Health Habits, Coping Styles, and Psychological Distress
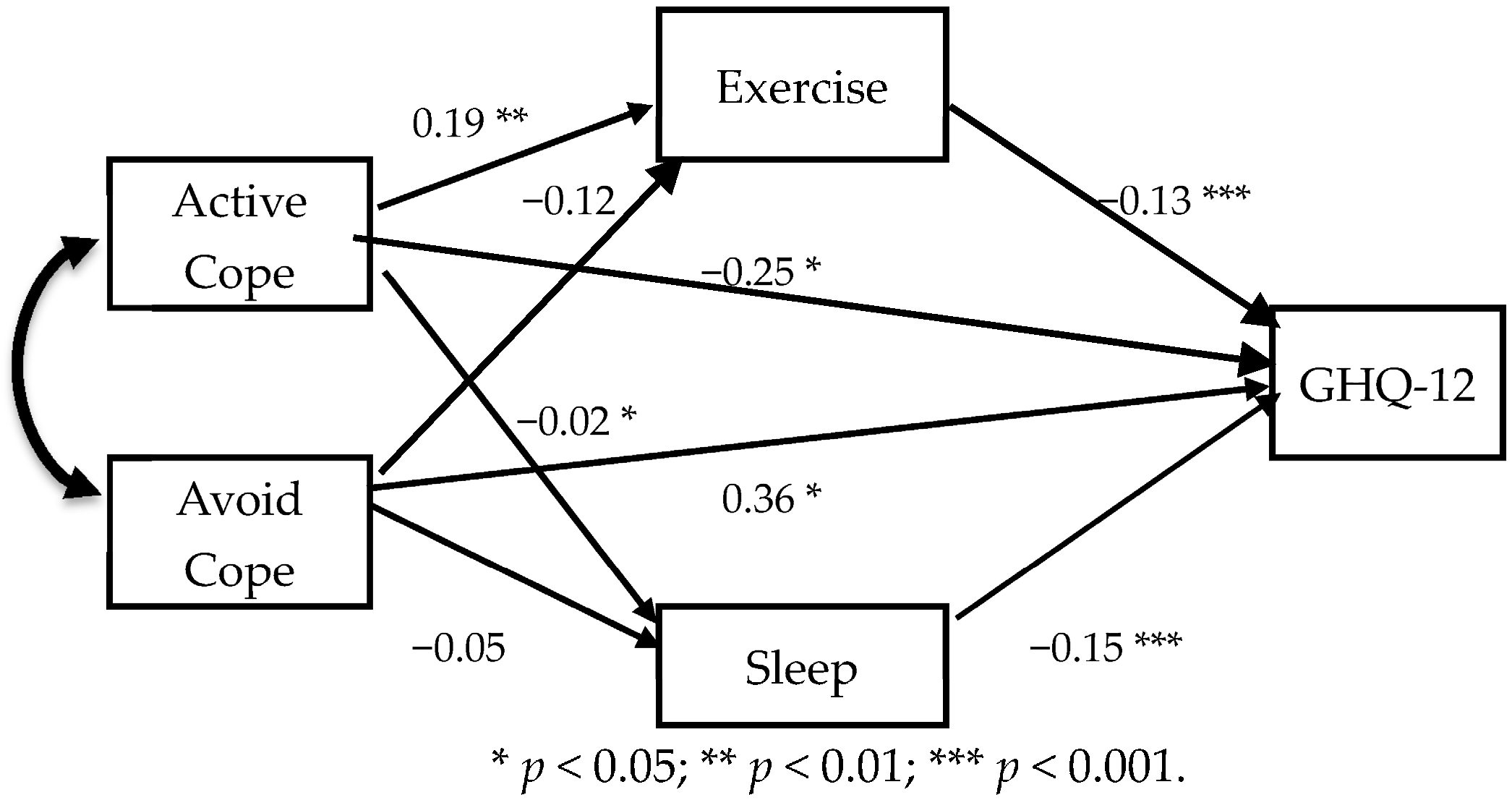
3.4. Associations among Health Habits, Coping Styles, and Psychological Distress
4. Discussion
Limitations of Research
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Watson, R.; Gardiner, E.; Hogston, R.; Gibson, H.; Stimpson, A.; Wrate, R.; Deary, I. A longitudinal study of stress and psychological distress in nurses and nursing students. J. Clin. Nurs. 2009, 18, 270–278. [Google Scholar] [CrossRef] [PubMed]
- Pryjmachuk, S.; Richards, D.A. Predicting stress in pre-registration nursing students. Br. J. Health Psychol. 2007, 12, 125–144. [Google Scholar] [CrossRef] [PubMed]
- Cilingir, D.; Gursoy, A.A.; Hintistan, S.; Ozturk, H. Nursing and midwifery college student’s expectations of their educators and perceived stressors during their education: A pilot study in Turkey. Int. J. Nurs. Pract. 2011, 17, 486–494. [Google Scholar] [CrossRef] [PubMed]
- Reeve, K.L.; Shumaker, C.J.; Yearwood, E.L.; Crowell, N.A.; Riley, J.B. Perceived stress and social support in undergraduate nursing students’ educational experiences. Nurse Educ. Today 2013, 33, 419–424. [Google Scholar] [CrossRef] [PubMed]
- Lahey, B.B. Public health significance of neuroticism. Am. Psychol. 2009, 64, 241–256. [Google Scholar] [CrossRef] [PubMed]
- Rahnama, M.; Shahdadim, H.; Bagheri, S.; Moghadam, M.P.; Absalan, A. The relationship between anxiety and coping strategies in family caregivers of patients with trauma. J. Clin. Diagn. Res. 2017, 11, IC06–IC09. [Google Scholar] [CrossRef] [PubMed]
- Morimoto, H.; Furuta, N.; Kono, M.; Kabeya, M. Stress-buffering effect of coping strategies on interrole conflict among family caregivers of people with dementia. Clin. Gerontol. 2017, 23, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Chan, D.E. Stress, Coping Strategies, and psychological distress among secondary school teachers in Hong Kong. Am. Educ. Res. J. 1998, 35, 145–163. [Google Scholar] [CrossRef]
- Cunningham, T.J.; Wheaton, A.G.; Giles, W.H. The association between psychological distress and self-reported sleep duration in a population-based sample of women and men. Sleep Disord. 2015, 172064. [Google Scholar] [CrossRef] [PubMed]
- Felder, J.N.; Laraia, B.; Coleman-Phox, K.; Bush, N.; Suresh, M.; Thomas, M.; Adler, N.; Epel, E.; Prather, A.A. Poor sleep quality, psychological distress, and the buffering effect of mindfulness training during pregnancy. Behav. Sleep Med. 2017, 6, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Kleppang, A.L.; Thurston, M.; Hartz, I.; Hagquist, C. Psychological distress among Norwegian adolescents: Changes between 2001 and 2009 and associations with leisure time physical activity and screen-based sedentary behaviour. Scand. J. Public Health, 2017, 1. [Google Scholar] [CrossRef] [PubMed]
- Toyoshima, M.; Kaneko, Y.; Motohashi, Y. Leisure-time activities and psychological distress in a suburban community in Japan. Prev. Med. Rep. 2016, 22, 1–5. [Google Scholar] [CrossRef] [PubMed]
- LeBouthillier, D.M.; Asmundson, G.J.G. The efficacy of aerobic exercise and resistance training as transdiagnostic interventions for anxiety-related disorders and constructs: A randomized controlled trial. J. Anxiety Disord. 2017, 52, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Freeman, D.; Sheaves, B.; Goodwin, G.M.; Yu, L.M.; Nickless, A.; Harrison, P.J.; Emsley, R.; Luik, A.I.; Foster, R.G.; Wadekar, V.; et al. The effects of improving sleep on mental health (OASIS): A randomised controlled trial with mediation analysis. Lancet Psychiatry 2017, 4, 749–758. [Google Scholar] [CrossRef]
- Johnson, R.; Robertson, W.; Towey, M.; Stewart-Brown, S.; Clarke, A. Changes over time in mental well-being, fruit and vegetable consumption and physical activity in a community-based lifestyle intervention: A before and after study. Public Health 2017, 146, 118–125. [Google Scholar] [CrossRef] [PubMed]
- De Ridder, D.; de Wit, J. Self-Regulation in Health Behavior; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2006. [Google Scholar]
- Mann, T.; de Ridder, D.; Fujita, K. Self-regulation of health behavior: Social psychological approaches to goal setting and goal striving. Health Psychol. 2013, 32, 487–498. [Google Scholar] [CrossRef] [PubMed]
- Compas, B.E.; Jaser, S.S.; Dunbar, M.J.P.; Watson, K.H.; Bettis, A.H.; Gruhn, M.A.; Williams, E.K. Coping and Emotion Regulation from Childhood to Early Adulthood: Points of Convergence and Divergence. Aust. J. Psychol. 2014, 66, 71–81. [Google Scholar] [CrossRef] [PubMed]
- De la Fuente, J.; Zapata, L.; Martínez-Vicente, J.M.; Sander, P.; Cardelle-Elawar, M. The role of personal self-regulation and regulatory teaching to predict motivational-affective variables, achievement, and satisfaction: A structural model. Front. Psychol. 2014, 6, 399. [Google Scholar] [CrossRef] [PubMed]
- Deasy, C.; Coughlan, B.; Pironom, J.; Jourdan, D.; Mannix-McNamara, P. Psychological distress and coping amongst higher education students: A mixed method enquiry. PLoS ONE 2014, 9, e115193. [Google Scholar] [CrossRef] [PubMed]
- Roohafza, H.; Sadeghi, M.; Shirani, S.; Bahonar, A.; Mackie, M.; Sarafzadegan, N. Association of socioeconomic status and life-style factors with coping strategies in Isfahan Healthy Heart Program, Iran. Croat. Med. J. 2009, 50, 380–386. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, D.; Williams, P.A. Users Guide to the General Health Questionnaire; NFER-Nelson: Windsor, UK, 1988. [Google Scholar]
- Doi, Y.; Minowa, M. Factor structure of the 12-item General Health Questionnaire in the Japanese general adult population. Psychiatry Clin. Neurosci. 2003, 57, 379–383. [Google Scholar] [CrossRef] [PubMed]
- Otsuka, Y.; Sasaki, T.; Iwasaki, K.; Otsuka, Y.; Sasaki, T. Working hours, coping skills, and psychological health in Japanese daytime workers. Ind. Health 2009, 47, 22–32. [Google Scholar] [CrossRef] [PubMed]
- Carver, C.S. You want to measure coping but your protocol’s too long: Consider the brief COPE. Int. J. Behav. Med. 1997, 4, 92–100. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, K.; Saito, M.; Takao, T. Stress and coping styles in Japanese nursing students. Int. J. Nurs. Pract. 2012, 18, 489–496. [Google Scholar] [CrossRef] [PubMed]
- Fortune, D.G.; Smith, J.V.; Garvey, K. Perceptions of psychosis, coping, appraisals, and psychological distress in the relatives of patients with schizophrenia: An exploration using self-regulation theory. Br. J. Clin. Psychol. 2005, 44, 319–331. [Google Scholar] [CrossRef] [PubMed]
- Jaser, S.S.; Linsky, R.; Grey, M. Coping and psychological distress in mothers of adolescents with type 1 diabetes. Matern. Child Health J. 2014, 18, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Hansen, M.C.; Ghafoori, B. Correlates of psychological distress among urban trauma-exposed adults: Influence of age and coping preferences. Psychol. Trauma 2017, 9, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Ong, H.C.; Ibrahim, N.; Wahab, S. Psychological distress, perceived stigma, and coping among caregivers of patients with schizophrenia. Psychol. Res. Behav. Manag. 2016, 9, 211–218. [Google Scholar] [CrossRef] [PubMed]
- De Feudis, R.; Lanciano, T.; Rinaldi, S. Coping Strategies of Southern Italian Women Predict Distress Following Breast Cancer Surgery. Eur. J. Psychol. 2015, 11, 280–294. [Google Scholar] [CrossRef] [PubMed]
- Kobosko, J.; Jedrzejczak, W.W.; Pilka, E.; Pankowska, A.; Skarzynski, H. Satisfaction with cochlear implants in postlingually deaf adults and its nonaudiological predictors: Psychological distress, coping strategies, and self-esteem. Ear Hear. 2015, 36, 605–618. [Google Scholar] [CrossRef] [PubMed]
- Matamura, M.; Tochigi, M.; Usami, S.; Yonehara, H.; Fukushima, M.; Nishida, A.; Togo, F.; Sasaki, T. Associations between sleep habits and mental health status and suicidality in a longitudinal survey of monozygotic twin adolescents. J. Sleep Res. 2014, 23, 290–294. [Google Scholar] [CrossRef] [PubMed]
- Kawada, T.; Otsuka, T.; Inagaki, H.; Wakayama, Y.; Katsumata, M.; Li, Q.; Li, Y.J. Relationship among lifestyles, aging and psychological wellbeing using the General Health Questionnaire 12-items in Japanese working men. Aging Male 2011, 14, 115–118. [Google Scholar] [CrossRef] [PubMed]
- Guszkowska, M.; Langwald, M.; Sempolska, K. Does physical exercise help maintain mental health during pregnancy? A comparison of changes in mental health in participants of physical exercise classes and childbirth classes. J. Phys. Act. Health. 2015, 12, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Mortazavi, S.S.; Mohammad, K.; Ardebili, H.E.; Beni, R.D.; Mahmoodi, M.; Keshteli, A.H. Mental disorder prevention and physical activity in Iranian elderly. Int. J. Prev. Med. 2012, 3, S64–S72. [Google Scholar] [PubMed]
- Callaghan, P.; Khalil, E.; Morres, I.; Carter, T. Pragmatic randomised controlled trial of preferred intensity exercise in women living with depression. BMC Public Health 2011, 11, 465. [Google Scholar] [CrossRef] [PubMed]
- Kwok, J.Y.Y.; Kwan, J.C.Y.; Auyeung, M.; Mok, V.C.T.; Chan, H.Y.L. The effects of yoga versus stretching and resistance training exercises on psychological distress for people with mild-to-moderate Parkinson’s disease: Study prxotocol for a randomized controlled trial. Trials 2017, 18, 509. [Google Scholar] [CrossRef] [PubMed]
- Awick, E.A.; Ehlers, D.K.; Aguiñaga, S.; Daugherty, A.M.; Kramer, A.F.; McAuley, E. Effects of a randomized exercise trial on physical activity, psychological distress and quality of life in older adults. Gen. Hosp. Psychiatry 2017, 49, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Perales, F.; Pozo-Cruz, J.D.; Pozo-Cruz, B.D. Impact of physical activity on psychological distress: A prospective analysis of an Australian national sample. Am. J. Public Health 2014, 104, e91–e97. [Google Scholar] [CrossRef] [PubMed]
- Cairney, J.; Kwan, M.Y.; Veldhuizen, S.; Faulkner, G.E. Who uses exercise as a coping strategy for stress? Results from a national survey of Canadians. J. Phys. Act. Health 2014, 11, 908–916. [Google Scholar] [CrossRef] [PubMed]
- Treviño, L.A.; Baker, L.; McIntosh, S.; Mustian, K.; Seplaki, C.L.; Guido, J.J.; Ossip, D.J. Physical activity as a coping strategy for smoking cessation in mid-life and older adults. Addict. Behav. 2014, 39, 885–888. [Google Scholar] [CrossRef] [PubMed]
- Elias, A.N.; Iyer, K.; Pandian, M.R.; Weathersbee, P.; Stone, S.; Tobis, J. Beta-endorphin/beta-lipotropin release and gonadotropin secretion after acute exercise in normal males. J. Appl. Physiol. 1986, 61, 2045–2049. [Google Scholar] [PubMed]
- Elliot, D.L.; Goldberg, L.; Watts, W.J.; Orwoll, E. Resistance exercise and plasma beta-endorphin/beta-lipotrophin immunoreactivity. Life Sci. 1984, 34, 515–518. [Google Scholar] [CrossRef]
- Farrell, P.A.; Kjaer, M.; Bach, F.W.; Galbo, H. Beta-endorphin and adrenocorticotropin response to supramaximal treadmill exercise in trained and untrained males. Acta Physiol. Scand. 1987, 130, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Heijnen, S.; Hommel, B.; Kibele, A.; Colzato, L.S. Neuromodulation of Aerobic Exercise—A Review. Front. Psychol. 2016, 6, 1890. [Google Scholar] [CrossRef] [PubMed]
- Young, S.N. How to increase serotonin in the human brain without drugs. J. Psychiatry Neurosci. 2007, 32, 394–399. [Google Scholar] [PubMed]
- Erdem, Ö.; Riva, E.; Prins, R.G.; Burdorf, A.; Van der Doef, M. Health-related behaviours mediate the relation between ethnicity and (mental) health in the Netherlands. Ethn. Health 2017, 5, 1–14. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| GHQ-12 | Exe | Sle | Dis | Act | Den | Sub | Emo | Ins | |
|---|---|---|---|---|---|---|---|---|---|
| GHQ-12 | ※ | −0.26 *** | −0.19 ** | 0.09 | −0.19 ** | 0.06 | 0.07 | −0.08 | −0.01 |
| Exe | ※ | 0.28 ** | −0.12 | 0.10 | −0.03 | 0.02 | 0.04 | 0.12 | |
| Sle | ※ | −0.13 | −0.01 | −0.06 | −0.13 | 0.06 | −0.05 | ||
| Dis | ※ | 0.22 ** | 0.15 * | 0.10 | 0.22 ** | 0.21 ** | |||
| Act | ※ | −0.03 | 0.13 | 0.32 *** | 0.41 *** | ||||
| Den | ※ | 0.36 *** | 0.09 | 0.02 | |||||
| Sub | ※ | 0.16 * | 0.07 | ||||||
| Emo | ※ | 0.72 ** | |||||||
| Ins | ※ | ||||||||
| Dise | |||||||||
| Ven | |||||||||
| Ref | |||||||||
| Pla | |||||||||
| Hum | |||||||||
| Acc | |||||||||
| Rel | |||||||||
| Bla |
| Dise | Ven | Ref | Pla | Hum | Acc | Rel | Bla | |
|---|---|---|---|---|---|---|---|---|
| GHQ | 0.25 ** | 0.16 * | −0.29 ** | −0.12 | −0.16 | −0.03 | −0.02 | 0.36 *** |
| Exe | −0.12 | 0.01 | 0.18* | 0.03 | 0.15 * | −0.03 | 0.03 | −0.15 * |
| Sle | −0.04 | 0.05 | −0.08 | 0.11 | −0.02 | −0.02 | 0.09 | −0.06 |
| Dis | 0.26 ** | 0.24 ** | 0.14 | −0.01 | 0.08 | 0.06 | 0.09 | 0.17 * |
| Act | −0.26 *** | 0.13 | 0.39 *** | 0.53 *** | 0.24 ** | 0.42 *** | 0.15 * | −0.52 |
| Den | 0.39 *** | 0.07 | 0.06 | −0.05 | 0.11 | −0.31 *** | 0.30 *** | 0.18 * |
| Sub | 0.04 | 0.09 | 0.07 | 0.02 | 0.15 * | 0.01 | 0.23 ** | 0.04 |
| Emo | −0.06 | 0.32 *** | 0.28 *** | 0.12 | 0.16 * | 0.07 | 0.21 ** | 0.08 |
| Ins | −0.13 | 0.33 *** | 0.25 ** | 0.29 *** | 0.06 | 0.28 *** | 0.16 * | 0.13 |
| Dise | ※ | 0.08 | −0.14 | −0.31 *** | 0.08 | −0.36 *** | −0.08 | 0.21 ** |
| Ven | ※ | 0.07 | 0.05 | 0.11 | 0.03 | 0.23 ** | 0.17 * | |
| Ref | ※ | 0.36 *** | 0.34 *** | 0.19 * | 0.21 ** | −0.05 | ||
| Pla | ※ | 0.09 | 0.49 *** | 0.09 | 0.03 | |||
| Hum | ※ | 0.07 | 0.19 * | −0.12 | ||||
| Acc | ※ | −0.06 | 0.07 | |||||
| Rel | ※ | 0.18 * | ||||||
| Bla | ※ |
| GHQ-12 | Exercise | Sleep | Active coping | Avoidance coping | |
|---|---|---|---|---|---|
| GHQ-12 | ※ | −0.26 *** | −0.19 ** | −0.28 *** | 0.39 *** |
| Exercise | ※ | 0.28 *** | 0.20 ** | −0.13 | |
| Sleep | ※ | 0.17 * | −0.05 | ||
| Active coping | ※ | −0.05 | |||
| Avoidance coping | ※ |
| Variables | Effects | Significance Factors | |||
|---|---|---|---|---|---|
| Exercise | Sleep | Active Coping | Avoidance Coping | ||
| Psychological | Direct | −0.13 | −0.15 | −0.25 | 0.36 |
| distress | Indirect | 0.00 | 0.00 | −0.02 | 0.02 |
| Total | −0.13 | −0.15 | −0.27 | 0.38 | |
© 2017 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tada, A. The Associations among Psychological Distress, Coping Style, and Health Habits in Japanese Nursing Students: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2017, 14, 1434. https://doi.org/10.3390/ijerph14111434
Tada A. The Associations among Psychological Distress, Coping Style, and Health Habits in Japanese Nursing Students: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2017; 14(11):1434. https://doi.org/10.3390/ijerph14111434
Chicago/Turabian StyleTada, Akio. 2017. "The Associations among Psychological Distress, Coping Style, and Health Habits in Japanese Nursing Students: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 14, no. 11: 1434. https://doi.org/10.3390/ijerph14111434