
A Meta-Analysis of Association between Methylenetetrahydrofolate Reductase Gene (MTHFR) 677C/T Polymorphism and Diabetic Retinopathy

Abstract
:
1. Introduction
2. Methods
2.1. Identification and Eligibility of Relevant Studies
2.2. Data Extraction and Conversion
2.3. Quality Assessment and Study Stratification
2.4. Meta-Analysis
3. Results
3.1. Literature Search
3.2. Eligible Studies and Study Characteristics
3.3. Summary Statistics
3.4. Main Results, Stratification, and Sensitivity Analyses
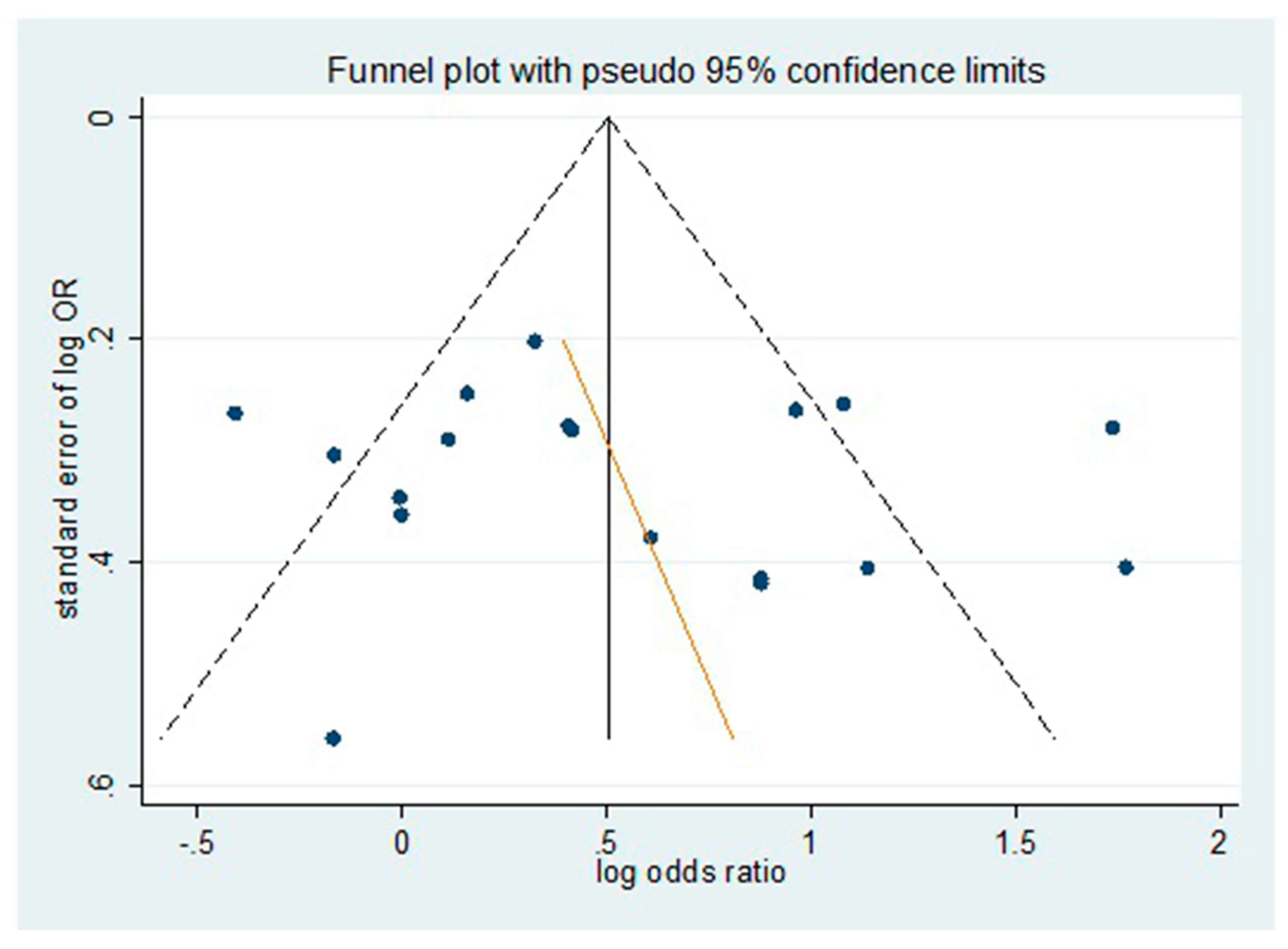
3.5. Source of Heterogeneity and Publication Bias
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Cheung, N.; Mitchell, P.; Wong, T.Y. Diabetic retinopathy. Lancet 2010, 376, 124–136. [Google Scholar] [CrossRef]
- Ting, D.S.; Cheung, G.C.; Wong, T.Y. Diabetic retinopathy: Global prevalence, major risk factors, screening practices and public health challenges: A review. Clin. Exp. Ophthalmol. 2015, 44, 206–277. [Google Scholar] [CrossRef] [PubMed]
- Klein, R.; Klein, B.E.; Moss, S.E.; Linton, K.L. The beaver dam eye study. Retinopathy in adults with newly discovered and previously diagnosed diabetes mellitus. Ophthalmology 1992, 99, 58–62. [Google Scholar] [CrossRef]
- Klein, R.; Klein, B.E.; Moss, S.E.; Cruickshanks, K.J. Relationship of hyperglycemia to the long-term incidence and progression of diabetic retinopathy. Arch. Intern. Med. 1994, 154, 2169–2178. [Google Scholar] [CrossRef] [PubMed]
- Klein, R.; Klein, B.E.; Moss, S.E.; Cruickshanks, K.J. The wisconsin epidemiologic study of diabetic retinopathy: Xvii. The 14-year incidence and progression of diabetic retinopathy and associated risk factors in type 1 diabetes. Ophthalmology 1998, 105, 1801–1815. [Google Scholar] [CrossRef]
- Nathan, D.M. Long-term complications of diabetes mellitus. N. Engl. J. Med. 1993, 328, 1676–1685. [Google Scholar] [CrossRef] [PubMed]
- Cho, H.; Sobrin, L. Genetics of diabetic retinopathy. Curr.Diabetes Rep. 2014, 14, 515. [Google Scholar] [CrossRef] [PubMed]
- Welch, G.N.; Loscalzo, J. Homocysteine and atherothrombosis. N. Engl. J. Med. 1998, 338, 1042–1050. [Google Scholar] [PubMed]
- DAngelo, A.; Selhub, J. Homocysteine and thrombotic disease. Blood 1997, 90, 1–11. [Google Scholar]
- Engbersen, A.M.; Franken, D.G.; Boers, G.H.; Stevens, E.M.; Trijbels, F.J.; Blom, H.J. Thermolabile 5,10-methylenetetrahydrofolate reductase as a cause of mild hyperhomocysteinemia. Am. J. Hum. Genet. 1995, 56, 142–150. [Google Scholar] [PubMed]
- Friedman, G.; Goldschmidt, N.; Friedlander, Y.; Ben-Yehuda, A.; Selhub, J.; Babaey, S.; Mendel, M.; Kidron, M.; Bar-On, H. A common mutation a1298c in human methylenetetrahydrofolate reductase gene: Association with plasma total homocysteine and folate concentrations. J. Nutr. 1999, 129, 1656–1661. [Google Scholar] [PubMed]
- Neugebauer, S.; Baba, T.; Kurokawa, K.; Watanabe, T. Defective homocysteine metabolism as a risk factor for diabetic retinopathy. Lancet 1997, 349, 473–474. [Google Scholar] [CrossRef]
- Fujita, H.; Narita, T.; Meguro, H.; Ishii, T.; Hanyu, O.; Suzuki, K.; Kamoi, K.; Ito, S. No association between mthfr gene polymorphism and diabetic nephropathy in Japanese type II diabetic patients with proliferative diabetic retinopathy. J. Diabetes Complicat. 1999, 13, 284–287. [Google Scholar] [CrossRef]
- Lauszus, F.F.; Gron, P.L.; Klebe, J.G. Association of polymorphism of methylene-tetrahydro-folate-reductase with urinary albumin excretion rate in type 1 diabetes mellitus but not with preeclampsia, retinopathy, and preterm delivery. Acta Obstet. Gynecol. Scand. 2001, 80, 803–806. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Wang, J.; Xue, Y.; Chen, Y.; Zou, Y. Relationship between methylenetetrahydrofolate reductase gene polymorphism and diabetic retinopathy. Chin. J. Ocul. Fundus Dis. 2001, 17, 31–33. [Google Scholar]
- Yang, G.; Lu, J.; Pan, C. Study on the relationship between n5, 10-methylenetetrahydrofolate reductase gene polymorphism and the susceptibility to microangiopathy in type 2 diabetes mellitus. Chin. J. Endocrinol. Metab. 2001, 17, 36–39. [Google Scholar]
- Maeda, M.; Yamamoto, I.; Fukuda, M.; Nishida, M.; Fujitsu, J.; Nonen, S.; Igarashi, T.; Motomura, T.; Inaba, M.; Fujio, Y.; et al. Mthfr gene polymorphism as a risk factor for diabetic retinopathy in type 2 diabetic patients without serum creatinine elevation. Diabetes Care 2003, 26, 547–548. [Google Scholar] [CrossRef] [PubMed]
- Santos, K.G.; Tschiedel, B.; Schneider, J.; Souto, K.; Roisenberg, I. Diabetic retinopathy in euro-brazilian type 2 diabetic patients: Relationship with polymorphisms in the aldose reductase, the plasminogen activator inhibitor-1 and the methylenetetrahydrofolate reductase genes. Diabetes Res. Clin. Pract. 2003, 61, 133–136. [Google Scholar] [CrossRef]
- Sun, J.; Xu, Y.; Zhu, Y.; Lu, H.; Deng, H.; Fan, Y.; Sun, S.; Zhang, Y. The relationship of methylenetetrahydrofolate reductase gene polymorphism and plasma homocysteine levels in type 2 diabetes mellitus patients with diabetic retinopathy. Zhonghua Yi Xue Yi Chuan Xue Za Zhi 2003, 20, 131–134. [Google Scholar] [PubMed]
- Yoshioka, K.; Yoshida, T.; Takakura, Y.; Kogure, A.; Umekawa, T.; Toda, H.; Yoshikawa, T. No association between the mthfr gene polymorphism and diabetic retinopathy in type 2 diabetic patients without overt nephropathy. Diabetes Care 2003, 26, 1947–1948; author reply 1948. [Google Scholar] [CrossRef] [PubMed]
- Huang, D.F.; Cao, H.; Mao, L. The relationship of homocysteine, methylenetetrahydrofolate reductasegene polymorphism and diabetic retinopathy. J. Chin. Microcirc. 2005, 9, 229–231. [Google Scholar]
- Yi, X.; Yu, Y.; Zhang, Y. The study on tcm syndrome differentiation of DR and the correlativity between its syndromes and types and gene polymorphism. J. Tradit. Chin. Ophthalmol. 2005, 15, 125–128. [Google Scholar]
- Errera, F.I.; Silva, M.E.; Yeh, E.; Maranduba, C.M.; Folco, B.; Takahashi, W.; Pereira, A.C.; Krieger, J.E.; Passos-Bueno, M.R. Effect of polymorphisms of the mthfr and apoe genes on susceptibility to diabetes and severity of diabetic retinopathy in Brazilian patients. Braz. J. Med. Biol. Res. 2006, 39, 883–888. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.; Fan, X.; Sun, Y.; Yu, D.; Zhang, J. Study on the relationship between homocys teine &n5,10-methylenetetrahydrofolate reductase and diabetic retinopathy. Tianjin Med. J. 2006, 34, 4–6. [Google Scholar]
- Maeda, M.; Yamamoto, I.; Fukuda, M.; Motomura, T.; Nishida, M.; Nonen, S.; Fujio, Y.; Kasayama, S.; Azuma, J. Mthfr gene polymorphism is susceptible to diabetic retinopathy but not to diabetic nephropathy in japanese type 2 diabetic patients. J. Diabetes Complicat. 2008, 22, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Ukinc, K.; Ersoz, H.O.; Karahan, C.; Erem, C.; Eminagaoglu, S.; Hacihasanoglu, A.B.; Yilmaz, M.; Kocak, M. Methyltetrahydrofolate reductase c677t gene mutation and hyperhomocysteinemia as a novel risk factor for diabetic nephropathy. Endocrine 2009, 36, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Min, R. Study on Risk Factors and Susceptibility Genes of Diabetic Retinopathy in Patients with Type 2 Diabetes Mellitus. Master Thesis, Tianjin Medical University, Tianjin, China, 2011. [Google Scholar]
- Yigit, S.; Karakus, N.; Inanir, A. Association of mthfr gene c677t mutation with diabetic peripheral neuropathy and diabetic retinopathy. Mol. Vis. 2013, 19, 1626–1630. [Google Scholar] [PubMed]
- Simoes, M.J.; Lobo, C.; Egas, C.; Nunes, S.; Carmona, S.; Costa, M.A.; Duarte, T.; Ribeiro, L.; Faro, C.; Cunha-Vaz, J.G. Genetic variants in icam1, ppargc1a and mthfr are potentially associated with different phenotypes of diabetic retinopathy. Ophthalmologica 2014, 232, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Niu, W.; Qi, Y. An updated meta-analysis of methylenetetrahydrofolate reductase gene 677c/t polymorphism with diabetic nephropathy and diabetic retinopathy. Diabetes Res. Clin. Pract. 2012, 95, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Zintzaras, E.; Chatzoulis, D.Z.; Karabatsas, C.H.; Stefanidis, I. The relationship between c677t methylenetetrahydrofolate reductase gene polymorphism and retinopathy in type 2 diabetes: A meta-analysis. J. Hum. Genet. 2005, 50, 267–275. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Chen, Y.; Cao, X.; Liu, C.; Xie, Y. Association between plasma homocysteine status and hypothyroidism: A meta-analysis. Int. J. Clin. Exp. Med. 2014, 7, 4544–4553. [Google Scholar] [PubMed]
- Zintzaras, E.; Lau, J. Synthesis of genetic association studies for pertinent gene-disease associations requires appropriate methodological and statistical approaches. J. Clin. Epidemiol. 2008, 61, 634–645. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Fang, Q.; Yu, N.; Zhao, D.; Zhang, Y.; Wang, J.; Wang, Q.; Zhou, X.; Cao, X.; Fan, X. Association between genetic polymorphism of the angiotensin-converting enzyme and diabetic nephropathy: A meta-analysis comprising 26,580 subjects. J. Renin-Angiotensin-Aldosterone Syst. JRAAS 2012, 13, 161–174. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef] [PubMed]
- Goyette, P.; Sumner, J.S.; Milos, R.; Duncan, A.M.; Rosenblatt, D.S.; Matthews, R.G.; Rozen, R. Human methylenetetrahydrofolate reductase: Isolation of cdna, mapping and mutation identification. Nat. Genet. 1994, 7, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Doupis, J.; Eleftheriadou, I.; Kokkinos, A.; Perrea, D.; Pavlatos, S.; Gonis, A.; Katsilambros, N.; Tentolouris, N. Acute hyperhomocysteinemia impairs endothelium function in subjects with type 2 diabetes mellitus. Exp. Clin. Endocrinol. Diabetes 2010, 118, 453–458. [Google Scholar] [CrossRef] [PubMed]
- Akalin, A.; Alatas, O.; Colak, O. Relation of plasma homocysteine levels to atherosclerotic vascular disease and inflammation markers in type 2 diabetic patients. Eur. J. Endocrinol. 2008, 158, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Hoogeveen, E.K.; Kostense, P.J.; Eysink, P.E.; Polak, B.C.; Beks, P.J.; Jakobs, C.; Dekker, J.M.; Nijpels, G.; Heine, R.J.; Bouter, L.M.; et al. Hyperhomocysteinemia is associated with the presence of retinopathy in type 2 diabetes mellitus: The hoorn study. Arch. Intern. Med. 2000, 160, 2984–2990. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldstein, M.; Leibovitch, I.; Yeffimov, I.; Gavendo, S.; Sela, B.A.; Loewenstein, A. Hyperhomocysteinemia in patients with diabetes mellitus with and without diabetic retinopathy. Eye 2004, 18, 460–465. [Google Scholar] [CrossRef] [PubMed]
- Frosst, P.; Blom, H.J.; Milos, R.; Goyette, P.; Sheppard, C.A.; Matthews, R.G.; Boers, G.J.; den Heijer, M.; Kluijtmans, L.A.; van den Heuvel, L.P.; et al. A candidate genetic risk factor for vascular disease: A common mutation in methylenetetrahydrofolate reductase. Nat. Genet. 1995, 10, 111–113. [Google Scholar] [CrossRef] [PubMed]
- Weisberg, I.; Tran, P.; Christensen, B.; Sibani, S.; Rozen, R. A second genetic polymorphism in methylenetetrahydrofolate reductase (MTHFR) associated with decreased enzyme activity. Mol. Genet. Metab. 1998, 64, 169–172. [Google Scholar] [CrossRef] [PubMed]
- Weisberg, I.S.; Jacques, P.F.; Selhub, J.; Bostom, A.G.; Chen, Z.; Curtis Ellison, R.; Eckfeldt, J.H.; Rozen, R. The 1298a→c polymorphism in methylenetetrahydrofolate reductase (MTHFR): In vitro expression and association with homocysteine. Atherosclerosis 2001, 156, 409–415. [Google Scholar] [CrossRef]
- Pare, G.; Chasman, D.I.; Parker, A.N.; Zee, R.R.; Malarstig, A.; Seedorf, U.; Collins, R.; Watkins, H.; Hamsten, A.; Miletich, J.P.; et al. Novel associations of cps1, mut, nox4, and dpep1 with plasma homocysteine in a healthy population: A genome-wide evaluation of 13,974 participants in the women’s genome health study. Circ. Cardiovasc. Genet. 2009, 2, 142–150. [Google Scholar] [CrossRef] [PubMed]
- Lange, L.A.; Croteau-Chonka, D.C.; Marvelle, A.F.; Qin, L.; Gaulton, K.J.; Kuzawa, C.W.; McDade, T.W.; Wang, Y.; Li, Y.; Levy, S.; et al. Genome-wide association study of homocysteine levels in filipinos provides evidence for cps1 in women and a stronger mthfr effect in young adults. Hum. Mol. Genet. 2010, 19, 2050–2058. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Zellweger-Zahner, T.; Schneider, M.; Junker, C.; Lengeler, C.; Antes, G. Language bias in randomised controlled trials published in English and German. Lancet 1997, 350, 326–329. [Google Scholar] [CrossRef]
- Yau, J.W.; Rogers, S.L.; Kawasaki, R.; Lamoureux, E.L.; Kowalski, J.W.; Bek, T.; Chen, S.J.; Dekker, J.M.; Fletcher, A.; Grauslund, J.; et al. Global prevalence and major risk factors of diabetic retinopathy. Diabetes Care 2012, 35, 556–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fu, Y.P.; Hallman, D.M.; Gonzalez, V.H.; Klein, B.E.; Klein, R.; Hayes, M.G.; Cox, N.J.; Bell, G.I.; Hanis, C.L. Identification of diabetic retinopathy genes through a genome-wide association study among Mexican-Americans from Starr County, Texas. J. Ophthalmol. 2010, 2010, 73–74. [Google Scholar] [CrossRef] [PubMed]
- Grassi, M.A.; Tikhomirov, A.; Ramalingam, S.; Below, J.E.; Cox, N.J.; Nicolae, D.L. Genome-wide meta-analysis for severe diabetic retinopathy. Hum. Mol. Genet. 2011, 20, 2472–2481. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.C.; Lin, J.M.; Lin, H.J.; Chen, C.C.; Chen, S.Y.; Tsai, C.H.; Tsai, F.J. Genome-wide association study of diabetic retinopathy in a Taiwanese population. Ophthalmology 2011, 118, 642–648. [Google Scholar] [CrossRef] [PubMed]
- Sheu, W.H.; Kuo, J.Z.; Lee, I.T.; Hung, Y.J.; Lee, W.J.; Tsai, H.Y.; Wang, J.S.; Goodarzi, M.O.; Klein, R.; Klein, B.E.; et al. Genome-wide association study in a Chinese population with diabetic retinopathy. Hum. Mol. Genet. 2013, 22, 3165–3173. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Ref *) | Year | Ethnicity | Design | Case | Control | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sample Size | Age (year) | DM Duration (year) | Definition | Sample Size | Age (year) | DM Duration (year) | Definition | HWE # | MAF & | NOS (Stars) | ||||
| Neugebauer, S. et al. [12] | 1997 | Japan | CS | 76 | 55.5 ± 7.9 | 16.5 ± 5.1 | DR | 36 | 50.5 ± 9.7 | 11.2 ± 4.2 | NCTDM | 0.67 | 0.26 | 7 |
| Fujita, H. et al. [13] | 1999 | Japan | CS | 105 | 60±12 | NR | PDR + DN | 68 | 62 ± 10 | NR | T2DM | 0.14 | 0.42 | 6 |
| Lauszus, F.F. et al. [14] | 2001 | Denmark | CS | 112 | NR | NR | DR | 1084 | NR | NR | T1DM | 0.53 | 0.29 | 5 |
| Wang, L.Q. et al. [15] | 2001 | China | CC | 62 | 62.50 ± 8.08 | 8.29 ± 6.40 | DR | 202 | 59.42 ± 14.87 for T2DM41.83 ± 17.10 for Healthy | 7.29 ± 5.80 for T2DM | Healthy + T2DM | 0.73 | 0.32 | 8 |
| Yang, G.Q. et al. [16] | 2001 | China | CC | 60 | 50.7 ± 12.1 | 1 (0.1–4) | DR | 231 | 51.1 ± 12.8 for T2DM with DN63.0 ± 8.8 for T2DM with NCD52.6 ± 14.9 for Healthy | 2 (1–4) for T2DM with DN14 (11–18) for T2DM with NCD | Healthy + T2DM | 0.73 | 0.44 | 8 |
| Maeda, M. et al. [17] | 2003 | Japan | CS | 51 | NR | NR | DR | 105 | NR | NR | T2DM | 0.06 | 0.37 | 5 |
| Santos, K.G. et al. [18] | 2003 | Brazil | CS | 99 | NA | NA | DR | 111 | NA | NA | T2DM | 0.98 | 0.39 | 6 |
| Sun, J. et al. [19] | 2003 | China | CC | 110 | 55.6 ± 6.7 | <5 | DR | 155 | 54.7 ± 7.1 for NDR42.3 ± 6.1 for Healthy | >10 for NDR | T2DM | 0.00 | 0.33 | 7 |
| Yoshioka, K. et al. [20] | 2003 | Japan | CS | 98 | NA | NA | DR | 268 | NA | NA | T2DM | 0.46 | 0.38 | 6 |
| Huang, D.F. et al. [21] | 2005 | China | CC | 50 | NR | NR | DR | 47 | NR | NR | Healthy | 0.96 | 0.26 | 5 |
| Yi, X.X. et al. [22] | 2005 | China | CC | 249 | 56.53 ± 10.45 | 5.9 ± 4 | DR | 65 | NR | NR | Healthy | 0.01 | 0.31 | 5 |
| Errera, F.I. et al. [23] | 2006 | Brazil | CC | 141 | 55.43 ± 15.33 | 18 ± 8.67 | DR | 107 | 66.11 ± 7.06 | NA | Healthy | 0.24 | 0.40 | 6 |
| Liu, D.M. et al. [24] | 2006 | China | CC | 44 | 51.9 ± 7.5 | NR | DR | 84 | 54.0 ± 13.2 | NA | Healthy | 0.01 | 0.29 | 5 |
| Maeda, M. et al. [25] | 2008 | Japan | CS | 75 | NA | NA | DR | 115 | NA | NA | T2DM | 0.06 | 0.36 | 5 |
| Ukinc, K. et al. [26] | 2009 | Turkey/ | CS | 25 | NA | NA | DR | 27 | NA | NA | T2DM | 0.10 | 0.24 | 5 |
| Ren, M. et al. [27] | 2011 | China | CC | 161 | 59.95 ± 10.55 | 11 | DR | 213 | 58.52 ± 12.61 | 7 | T2DM | 0.23 | 0.42 | 7 |
| Yigit, S. et al. [28] | 2013 | Turkey | CS | 81 | NA | NA | DR | 149 | NA | NA | T1DM + T2DM | 0.98 | 0.24 | 5 |
| Simoes, M.J. et al. [29] | 2014 | Portugal | CS | 148 | 58.5 ± 8.4 | 10.5 ± 5.3 | PDR | 79 | 61.8 ± 7.8 | 8.9 ± 4.8 | T2DM | 0.73 | 0.24 | 7 |
| Author (Ref) | Prevalence of MTHFR C677T Genotype | Prevalence of Allele Frequency | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| CC | CT | TT | C | T | ||||||
| Case | Control | Case | Control | Case | Control | Case | Control | Case | Control | |
| Neugebauer, S. et al. [12] | 26 | 20 | 38 | 13 | 12 | 3 | 90 | 53 | 62 | 19 |
| Fujita, H. et al. [13] | 31 | 20 | 57 | 39 | 17 | 9 | 119 | 79 | 91 | 57 |
| Lauszus, F.F. et al. [14] | 47 | 542 | 57 | 455 | 8 | 87 | 151 | 1539 | 73 | 629 |
| Wang, L.Q. et al. [15] | 8 | 94 | 27 | 86 | 27 | 22 | 43 | 274 | 81 | 130 |
| Yang, G.Q. et al. [16] | 8 | 75 | 33 | 111 | 19 | 45 | 49 | 261 | 71 | 201 |
| Maeda, M. et al. [17] | 18 | 37 | 20 | 58 | 13 | 10 | 56 | 132 | 46 | 78 |
| Santos, K.G. et al. [18] | 34 | 41 | 53 | 53 | 12 | 17 | 121 | 135 | 77 | 87 |
| Sun, J. et al. [19] | 33 | 82 | 46 | 45 | 31 | 28 | 112 | 209 | 108 | 101 |
| Yoshioka, K. et al. [20] | 33 | 100 | 50 | 132 | 15 | 36 | 116 | 332 | 80 | 204 |
| Huang, D.F. et al. [21] | 17 | 26 | 25 | 18 | 8 | 3 | 59 | 70 | 41 | 24 |
| Yi, X.X. et al. [22] | 68 | 35 | 110 | 19 | 71 | 11 | 246 | 89 | 252 | 41 |
| Errera, F.I. et al. [23] | 61 | 36 | 66 | 57 | 14 | 14 | 188 | 129 | 94 | 85 |
| Liu, D.M. et al. [24] | 18 | 47 | 16 | 25 | 10 | 12 | 52 | 119 | 36 | 49 |
| Maeda, M. et al. [25] | 31 | 43 | 28 | 62 | 16 | 10 | 90 | 148 | 60 | 82 |
| Ukinc, K. et al. [26] | 14 | 14 | 11 | 13 | 0 | 0 | 39 | 41 | 11 | 13 |
| Ren, M. et al. [27] | 26 | 77 | 78 | 95 | 57 | 41 | 130 | 249 | 192 | 177 |
| Yigit, S. et al. [28] | 38 | 85 | 30 | 55 | 13 | 9 | 106 | 225 | 56 | 73 |
| Simoes, M.J. et al. [29] | 69 | 45 | 60 | 30 | 19 | 4 | 198 | 120 | 98 | 38 |
| Total | 580 | 1419 | 805 | 1366 | 362 | 361 | 1965 | 4204 | 1529 | 2088 |
| Subgroup | Genetic Model | Studies No (All/Sensitivity) | OR (95% CI) | p * | I2 (%) | OR se (95% CI) # |
|---|---|---|---|---|---|---|
| Overall | CT vs. CC | 18/15 | 1.46 (1.15–1.86) | 0.00 | 60.0 | 1.32 (1.02–1.70) |
| TT vs. CC | 18/15 | 2.45 (1.66–3.60) | 0.00 | 69.0 | 2.27 (1.44–3.58) | |
| Allele contrast | 18/15 | 1.52 (1.26–1.84) | 0.00 | 72.4 | 1.45 (1.17–1.79) | |
| Recessive model | 18/15 | 1.67 (1.19–2.40) | 0.00 | 71.9 | 1.87 (1.32–2.66) | |
| Dominant model | 18/15 | 1.71 (1.28–2.28) | 0.00 | 75.3 | 1.50 (1.13–1.98) | |
| Asian | CT vs. CC | 12/9 | 1.71 (1.22–2.39) | 0.00 | 64.9 | 1.52 (1.01–2.30) |
| TT vs. CC | 12/9 | 2.97 (2.06–4.29) | 0.02 | 51.5 | 3.07 (1.83–5.14) | |
| Allele contrast | 12/9 | 1.75 (1.42–2.18) | 0.00 | 67.3 | 1.69 (1.28–2.24) | |
| Recessive model | 12/9 | 2.16 (1.75–2.65) | 0.11 | 35.1 | 2.34(1.62–3.38) | |
| Dominant model | 12/9 | 1.98 (1.42–2.76) | 0.00 | 68.6 | 1.83 (1.20–2.81) | |
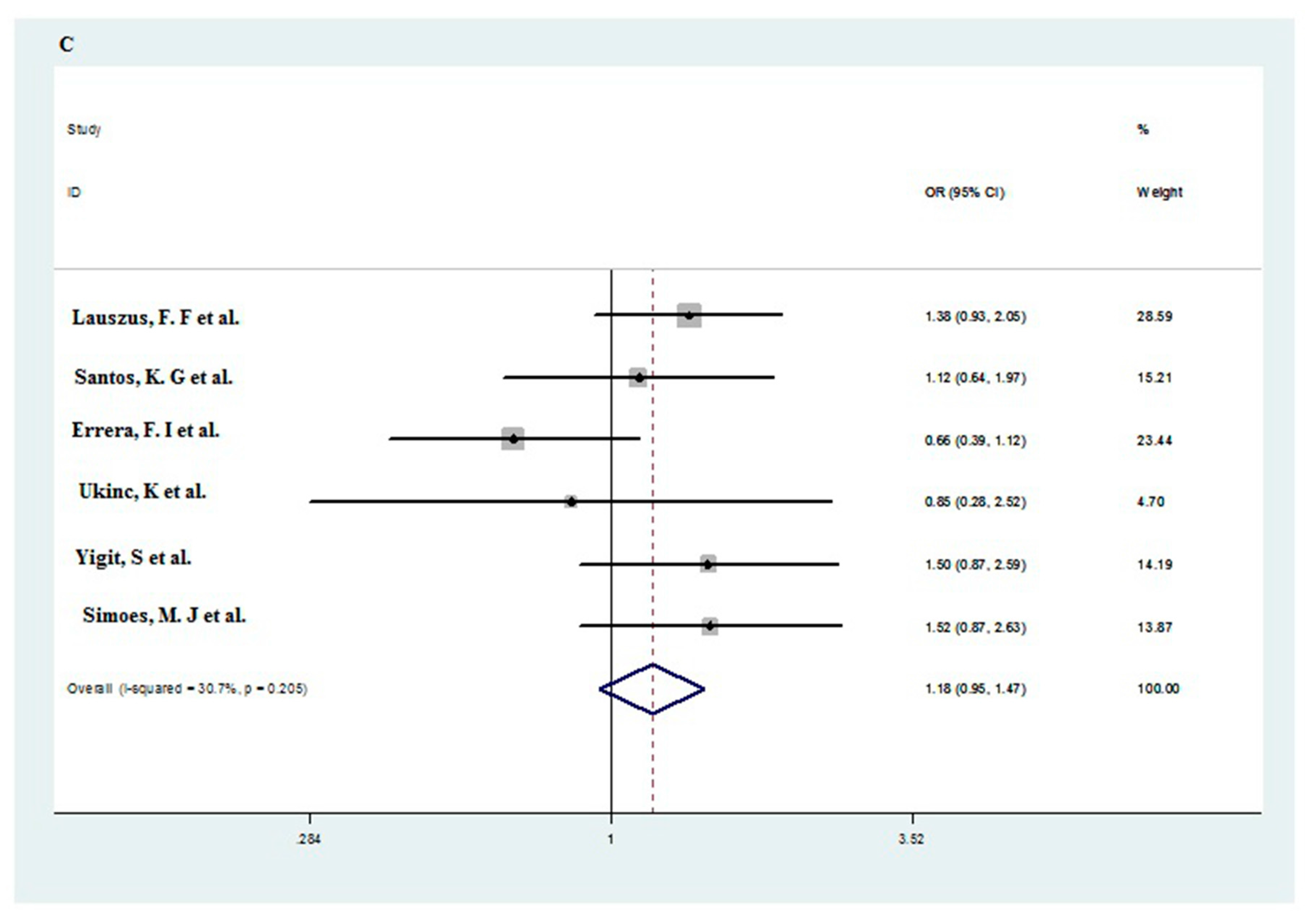
| Non-Asian | CT vs. CC | 6/6 | 1.15 (0.92–1.45) | 0.38 | 5.4 | 1.15 (0.92–1.45) |
| TT vs. CC | 6/6 | 1.33 (0.69–2.54) | 0.04 | 61.4 | 1.33 (0.69–2.54) | |
| Allele contrast | 6/6 | 1.14 (0.89–1.46) | 0.07 | 51.5 | 1.14 (0.89–1.46) | |
| Recessive model | 6/6 | 1.24 (0.69–2.23) | 0.05 | 57.7 | 1.24 (0.69–2.23) | |
| Dominant model | 6/6 | 1.18 (0.95–1.47) | 0.21 | 30.70 | 1.18 (0.95–1.47) | |
| T2DM | CT vs. CC | 12/10 | 1.50 (1.08–2.09) | 0.00 | 66.5 | 1.32 (0.93–1.86) |
| TT vs. CC | 12/10 | 2.68 (1.74–4.13) | 0.00 | 66.2 | 2.61 (1.50–4.53) | |
| Allele contrast | 12/10 | 1.59 (1.26–2.01) | 0.00 | 74.0 | 1.49 (1.14–1.96) | |
| Recessive model | 12/10 | 2.05 (1.47–2.84) | 0.01 | 56.9 | 2.10 (1.38–3.17) | |
| Dominant model | 12/10 | 1.72 (1.23–2.42) | 0.00 | 72.1 | 1.54 (1.06–2.24) | |
| Non-T2DM | CT vs. CC | 6/5 | 1.30 (1.02–1.66) | 0.12 | 43.5 | 1.32 (0.89–1.97) |
| TT vs. CC | 6/5 | 1.75 (0.93–3.27) | 0.05 | 55.9 | 1.70 (0.80–3.63) | |
| Allele contrast | 6/5 | 1.38 (1.02–1.88) | 0.02 | 64.5 | 1.34 (0.95–1.91) | |
| Recessive model | 6/5 | 1.38 (0.96–2.00) | 0.14 | 39.5 | 1.32 (0.89–1.97) | |
| Dominant model | 6/5 | 1.46 (1.00–2.13) | 0.04 | 57.4 | 1.42 (0.92–2.19) | |
| Asian with T2DM | CT vs. CC | 9/7 | 1.64 (1.07–2.50) | 0.00 | 73.8 | 1.40 (0.86–2.29) |
| TT vs. CC | 9/7 | 3.00 (1.92–4.68) | 0.01 | 63.8 | 2.99 (1.63–5.50) | |
| Allele contrast | 9/7 | 1.73 (1.33–2.26) | 0.00 | 76.0 | 1.64 (1.17–2.29) | |
| Recessive model | 9/7 | 2.21 (1.59–3.06) | 0.03 | 51.9 | 2.33 (1.52–3.57) | |
| Dominant model | 9/7 | 1.94 (1.27–2.94) | 0.00 | 76.7 | 1.72 (1.03–2.89) | |
| Asian with Non-T2DM | CT vs. CC | 3/2 | 1.99 (1.22–3.25) | 0.87 | 0.0 | 2.19 (1.19–4.01) |
| TT vs. CC | 3/2 | 2.80 (1.39–5.66) | 0.77 | 0.0 | 3.50 (1.28–9.62) | |
| Allele contrast | 3/2 | 1.86 (1.32–2.60) | 0.90 | 0.0 | 1.97 (1.28–3.05) | |
| Recessive model | 3/2 | 2.06 (1.06–4.02) | 0.87 | 0.0 | 2.38 (0.91–6.24) | |
| Dominant model | 3/2 | 2.17 (1.38–3.42) | 0.85 | 0.0 | 2.40 (1.35–4.28) | |
| Non-Asian with T2DM | CT vs. CC | 3/3 | 1.20 (0.81–1.76) | 0.79 | 0.0 | 1.20 (0.81–1.76) |
| TT vs. CC | 3/3 | 1.54 (0.43–5.46) | 0.08 | 68.2 | 1.54 (0.43–5.46) | |
| Allele contrast | 3/3 | 1.18 (0.90–1.56) | 0.25 | 27.0 | 1.18 (0.90–1.56) | |
| Recessive model | 3/3 | 1.37 (0.39–4.82) | 0.06 | 70.8 | 1.37 (0.39–4.82) | |
| Dominant model | 3/3 | 1.24 (0.86–1.80) | 0.58 | 0.0 | 1.24 (0.86–1.80) | |
| Non-Asian with Non-T2DM | CT vs. CC | 3/3 | 1.09 (0.69–1.71) | 0.09 | 58.0 | 1.09 (0.69–1.71) |
| TT vs. CC | 3/3 | 1.24 (0.49–3.14) | 0.03 | 71.9 | 1.24 (0.49–3.14) | |
| Allele contrast | 3/3 | 1.13 (0.76–1.68) | 0.02 | 73.3 | 1.13 (0.76–1.68) | |
| Recessive model | 3/3 | 1.21 (0.54–2.72) | 0.05 | 66.9 | 1.21 (0.54–2.72) | |
| Dominant model | 3/3 | 1.13 (0.69–1.83) | 0.05 | 66.7 | 1.13 (0.69–1.83) |
| Subgroup | Egger Test | Begg Test | ||
|---|---|---|---|---|
| Dominant | Recessive | Dominant | Recessive | |
| all study | 0.59 | 0.48 | 0.65 | 0.48 |
| T2DM | 0.91 | 0.94 | 0.84 | 0.64 |
| Non-T2DM | 0.28 | 0.16 | 0.06 | 0.26 |
| Asian | 0.62 | 0.91 | 0.63 | 0.54 |
| Non-Asian | 0.57 | 0.10 | 1.00 | 0.46 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luo, S.; Wang, F.; Shi, C.; Wu, Z. A Meta-Analysis of Association between Methylenetetrahydrofolate Reductase Gene (MTHFR) 677C/T Polymorphism and Diabetic Retinopathy. Int. J. Environ. Res. Public Health 2016, 13, 806. https://doi.org/10.3390/ijerph13080806
Luo S, Wang F, Shi C, Wu Z. A Meta-Analysis of Association between Methylenetetrahydrofolate Reductase Gene (MTHFR) 677C/T Polymorphism and Diabetic Retinopathy. International Journal of Environmental Research and Public Health. 2016; 13(8):806. https://doi.org/10.3390/ijerph13080806
Chicago/Turabian StyleLuo, Shasha, Furu Wang, Chao Shi, and Zhifeng Wu. 2016. "A Meta-Analysis of Association between Methylenetetrahydrofolate Reductase Gene (MTHFR) 677C/T Polymorphism and Diabetic Retinopathy" International Journal of Environmental Research and Public Health 13, no. 8: 806. https://doi.org/10.3390/ijerph13080806