
The Role of Stress Management in the Relationship between Purpose in Life and Self-Rated Health in Teachers: A Mediation Analysis

 and
and
Abstract
:1. Introduction
2. Subjects and Methods
2.1. Subjects and Data Collection
2.2. Measurement of SRH
2.3. Measurement of Purpose in Life
2.4. Measurement of Stress Management
2.5. Statistical Analysis
2.6. Ethic Statement
3. Results
3.1. Sample Characteristics and Correlations between Study Variables
3.2. Confirmatory Factor Analysis of the Subscales
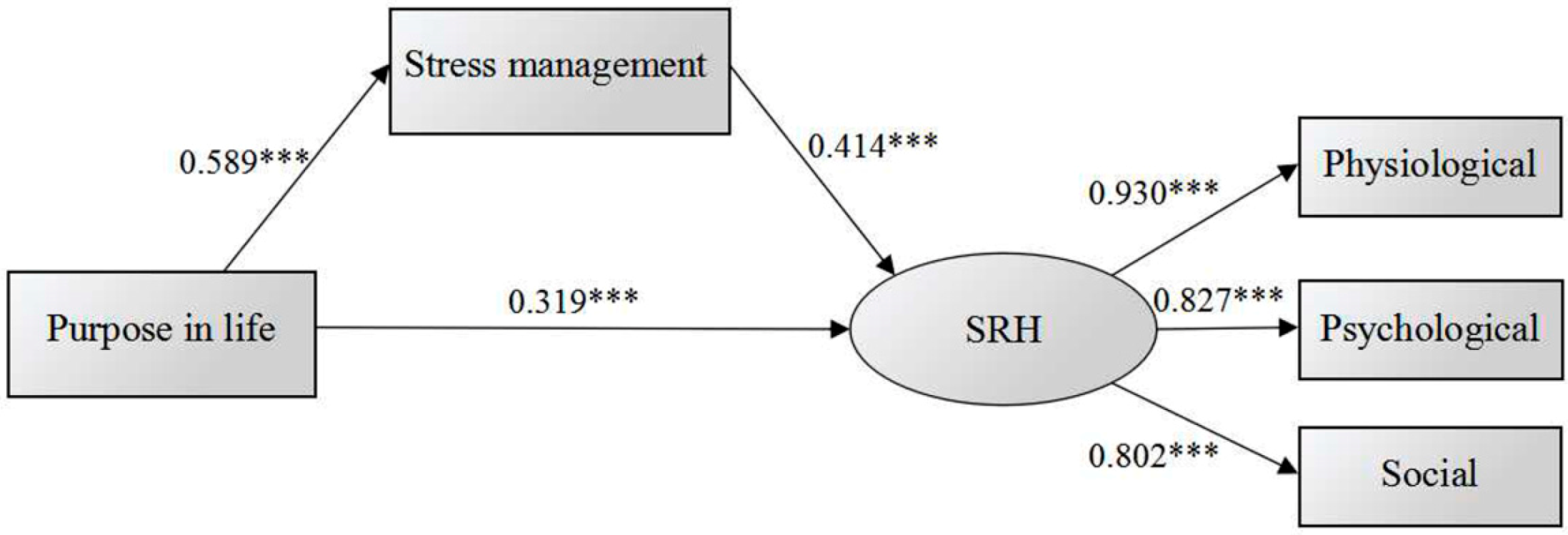
3.3. Structural Equation Modeling
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- McKnight, P.E.; Kashdan, T.B. Purpose in life as a system that creates and sustains health and well-being: An integrative, testable theory. Rev. Gen. Psychol. 2009, 13, 242–251. [Google Scholar] [CrossRef]
- Hooker, K.; Siegler, I.C. Life goals, satisfaction, and self-rated health: Preliminary findings. Exp. Aging Res. 1993, 19, 97–110. [Google Scholar] [CrossRef] [PubMed]
- Bruin, A.D.; Picavet, H.S.; Nossikov, A. Health interview surveys: Towards international harmonization of methods and instruments. WHO Reg. Publ. Eur. Ser. 1996, 58, 1–161. [Google Scholar]
- Holahan, C.K.; Suzuki, R. Motivational factors in health promoting behavior in later aging. Act. Adapt. 2006, 30, 47–60. [Google Scholar] [CrossRef]
- Wells, J.N.B.; Bush, H.A. Purpose-in-life and breast health behavior in Hispanic and Anglo women. J. Holist. Nurs. 2002, 20, 232–249. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.S.; Strecher, V.J.; Ryff, C.D. Purpose in life and use of preventive health care services. Proc. Natl. Acad. Sci. USA 2014, 111, 16331–16336. [Google Scholar] [CrossRef] [PubMed]
- Zilioli, S.; Slatcher, R.B.; Ong, A.D.; Gruenewald, T.L. Purpose in life predicts allostatic load ten years later. J. Psychosom. Res. 2015, 79, 451–457. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.S.; Hershner, S.D.; Strecher, V.J. Purpose in life and incidence of sleep disturbances. J. Behav. Med. 2015, 38, 590–597. [Google Scholar] [CrossRef] [PubMed]
- Yu, L.; Boyle, P.A.; Wilson, R.S.; Levine, S.R.; Schneider, J.A.; Bennett, D.A. Purpose in life and cerebral infarcts in community-dwelling older people. Stroke 2015, 46, 1071–1076. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.S.; Sun, J.K.; Park, N.; Peterson, C. Purpose in life and reduced incidence of stroke in older adults: “The Health and Retirement Study”. J. Psychosom. Res. 2013, 74, 427–432. [Google Scholar] [CrossRef] [PubMed]
- Cohen, R.; Bavishi, C.; Rozanski, A. Purpose in life and its relationship to all-cause mortality and cardiovascular events: A meta-analysis. Psychosom. Med. 2016, 78, 122–133. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, S.M.; Morozink, B.J.; van Reekum, C.M.; Lapate, R.C.; Norris, C.J.; Ryff, C.D.; Davidson, R.J. Purpose in life predicts better emotional recovery from negative stimuli. PLoS ONE 2013, 8, e80329. [Google Scholar] [CrossRef] [PubMed]
- Hedberg, P.; Gustafson, Y.; Alèx, L.; Brulin, C. Depression in relation to purpose in life among a very old population: A five-year follow-up study. Aging Ment. Health 2010, 14, 757–763. [Google Scholar] [CrossRef] [PubMed]
- Pietrzak, R.H.; Cook, J.M. Psychological resilience in older U.S. veterans: Results from the national health and resilience in veterans study. Depress. Anxiety 2013, 30, 432–443. [Google Scholar] [CrossRef] [PubMed]
- Pinquart, M. Creating and maintaining purpose in life in old age: A meta-analysis. Ageing Int. 2002, 27, 90–114. [Google Scholar] [CrossRef]
- Dehnavi, S.R.; Heidarian, F.; Ashtari, F.; Shaygannejad, V. Psychological well-being in people with multiple sclerosis in an Iranian population. J. Res. Med. Sci. 2015, 20, 535–539. [Google Scholar] [CrossRef] [PubMed]
- Shen, X.; Yang, Y.L.; Wang, Y.; Liu, L.; Wang, S.; Wang, L. The association between occupational stress and depressive symptoms and the mediating role of psychological capital among Chinese university teachers: A cross-sectional study. BMC Psychiatry 2014, 14, 329. [Google Scholar] [CrossRef] [PubMed]
- Bauer, J.; Stamm, A.; Virnich, K.; Wissing, K.; Müller, U.; Wirsching, M.; Schaarschhmidt, U. Correlation between burnout syndrome andpsychological and psychosomatic symptoms among teachers. Int. Arch. Occup. Environ. Health 2006, 79, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Tian, D.; Liu, Y.Q. Self-rated health status and its influencing factors among urban occupational populations in Liaoning Province. Chin. J. Public Health 2011, 27, 353–354. (In Chinese) [Google Scholar]
- Noh, J.W.; Yun, H.Y.; Park, H.; Yu, S.E. A study of predictive factors affecting health: Promoting behaviors of North Korean adolescent refugees. J. Prev. Med. Public Health 2015, 48, 231–238. [Google Scholar] [CrossRef] [PubMed]
- McGregor, B.A.; Antoni, M.H.; Boyers, A.; Alferi, S.M.; Blomberg, B.B.; Carver, C.S. Cognitive-behavioral stress management increases benefit finding and immune function among women with early-stage breast cancer. J. Psychosom. Res. 2004, 56, 1–8. [Google Scholar] [CrossRef]
- Teraoka, S.; Hayashida, N.; Shinkawa, T.; Taira, Y.; Nagai-Sekitani, Y.; Irie, S.; Kamasaki, T.; Nakashima-Hashiguchi, K.; Yoshida, K.; Orita, M.; et al. Good stress management capability is associated with lower body mass index and restful sleep. Tohoku J. Exp. Med. 2013, 229, 5–10. [Google Scholar] [CrossRef] [PubMed]
- Bruflat, A.K.; Balter, J.E.; McGuire, D.; Fethke, N.B.; Maluf, K.S. Stress management as an adjunct to physical therapy for chronic neck pain. Phys. Ther. 2012, 92, 1348–1359. [Google Scholar] [CrossRef] [PubMed]
- Rahe, R.H.; Taylor, C.B.; Tolles, R.L.; Newhall, L.M.; Veach, T.L.; Bryson, S. A novel stress and coping workplace program reduces illness and healthcare utilization. Psychosom. Med. 2002, 64, 278–286. [Google Scholar] [CrossRef] [PubMed]
- Nakata, A.; Takahashi, M.; Otsuka, Y.; Swanson, N.G. Is self-rated health associated with blood immune markers in healthy individuals. Int. J. Behav. Med. 2010, 7, 234–242. [Google Scholar] [CrossRef] [PubMed]
- Molla, J.H.; Salabifard, S.; Mousavi, S.M.; Sobhani, Z. The effectiveness of group training of CBT-based stress management on anxiety, psychological hardiness and general self-efficacy among university students. Glob. J. Health Sci. 2015, 8, 53526. [Google Scholar]
- Griffith, J.; Steptoe, A.; Cropley, M. An investigation of coping strategies associated with job stress in teachers. Br. J. Educ. Psychol. 1999, 69, 517–531. [Google Scholar] [CrossRef] [PubMed]
- Shimazu, A.; Okada, Y.; Sakamoto, M.; Miura, M. Effects of stress management program for teachers in Japan: A pilot study. J. Occup. Health 2003, 45, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Xu, K.; Feng, L.Y.; Luo, R.; Qiu, J.C.; Zhang, J.H.; Zhao, X.S.; Lu, Y.; Wei, Q. Assessment of the reliability and validity of the Sub-Health Measurement Scale Version1.0. Nan Fang Yi Ke Da Xue Xue Bao 2011, 31, 33–38. (In Chinese) [Google Scholar] [PubMed]
- Ryff, C.D. Happiness is everything, or is it? Explorations on the meaning of psychological well-being. J. Pers. Soc. Psychol. 1989, 57, 1069–1081. [Google Scholar] [CrossRef]
- Ryff, C.D.; Keyes, C.L. The structure of psychological well-being revisited. J. Pers. Soc. Psychol. 1995, 69, 719–727. [Google Scholar] [CrossRef] [PubMed]
- Walker, S.N.; Sechrist, K.R.; Pejder, N.J. The health-promoting lifestyle profile: Development and psychometric characteristics. Nurs. Res. 1987, 36, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Leung, S.S.; Chiang, V.C.; Chui, Y.Y.; Mak, Y.W.; Wong, D.F. A brief cognitive-behavioral stress management program for secondary school teachers. J. Occup. Health 2011, 53, 23–35. [Google Scholar] [CrossRef] [PubMed]
- Bower, J.E.; Kemeny, M.E.; Taylor, S.E.; Fahey, J.L. Finding positive meaning and its association with natural killer cell cytotoxicity among participants in a bereavement-related disclosure intervention. Ann. Behav. Med. 2003, 25, 146–155. [Google Scholar] [CrossRef] [PubMed]
- Eyler, A.A.; Brownson, R.C.; Donatelle, R.J.; King, A.C.; Brown, D.; Sallis, J.F. Physical activity social support and middle- and older-age minority women: Results from a U.S. survey. Soc. Sci. Med. 1999, 49, 781–789. [Google Scholar] [CrossRef]
- Ishida, R.; Okada, M. Factors influencing the development of “Purpose in Life” and its relationship to coping with mental stress. Psychology 2011, 2, 29–34. [Google Scholar] [CrossRef]
- Ishida, R.; Okada, M. Effects of a firm purpose in life on anxiety and sympathetic nervous activity caused by emotional stress: Assessment by psychophysiological method. Stress Health 2006, 22, 275–281. [Google Scholar] [CrossRef]
- Holahan, C.K.; Holahan, C.J.; Velasquez, K.E.; Jung, S.; North, R.J.; Pahl, S.A. Purposiveness and leisure-time physical activity in women in early midlife. Women Health 2011, 51, 661–675. [Google Scholar] [CrossRef] [PubMed]
- Hooker, S.A.; Masters, K.S. Purpose in life is associated with physical activity measured by accelerometer. J. Health Psychol. 2016, 21, 962–971. [Google Scholar] [CrossRef] [PubMed]
- Ryff, C.D.; Dienberg Love, G.; Urry, H.L.; Muller, D.; Rosenkranz, M.A.; Friedman, E.M.; Davidson, R.J.; Singer, B. Psychological well-being and ill-being: Do they have distinct or mirrored biological correlates? Psychother. Psychosom. 2006, 75, 85–95. [Google Scholar] [CrossRef] [PubMed]
- Bronk, K.C.; Hill, P.L.; Lapsley, D.K.; Talib, N.; Finch, H. Purpose, hope, and life satisfaction in three age groups. J. Posit. Psychol. 2009, 4, 500–510. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Total (n = 6840) | |
|---|---|---|
| n | % | |
| Sex | ||
| Male | 2518 | 36.8 |
| Female | 4322 | 63.2 |
| Marital status | ||
| Single | 552 | 8.1 |
| Married | 6288 | 91.9 |
| Education level | ||
| College degree or below | 2093 | 30.6 |
| Bachelor degree or above | 4747 | 69.4 |
| Age, mean (SD) | 38.24 (7.46) | |
| Body mass index | 22.45 (3.10) | |
| Purpose in life, mean (SD) | 8.75 (2.17) | |
| Stress management, mean (SD) | 20.29 (4.18) | |
| SHS, mean (SD) | 65.42 (12.03) | |
| Self-rated physiological health, mean (SD) | 66.97 (13.35) | |
| Self-rated psychological health, mean (SD) | 63.98 (15.54) | |
| Self-rated social health, mean (SD) | 64.93 (14.17) | |
| Variables | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|
| 1. Purpose in life | - | 0.589 *** | 0.462 *** | 0.302 *** | 0.448 *** | 0.471 *** |
| 2. Stress management | - | 0.547 *** | 0.416 *** | 0.511 *** | 0.498 *** | |
| 3. SRH | - | 0.866 *** | 0.915 *** | 0.780 *** | ||
| 4. Self-rated physiological health | - | 0.681 *** | 0.463 *** | |||
| 5. Self-rated psychological health | - | 0.655 *** | ||||
| 6. Self-rated social health | - |
| Items | Subscales | Estimate | S.E. | Standardized Estimate | C.R. | p | CR | |
|---|---|---|---|---|---|---|---|---|
| 1 | <--- | Purpose in life | 1.087 | 0.021 | 0.777 | 50.996 | <0.001 | 0.798 |
| 2 | <--- | 0.94 | 0.019 | 0.713 | 50.048 | <0.001 | ||
| 3 | <--- | 1 | 0.772 | |||||
| 4 | <--- | Stress management | 0.481 | 0.019 | 0.33 | 25.106 | <0.001 | 0.813 |
| 5 | <--- | 0.74 | 0.017 | 0.567 | 42.775 | <0.001 | ||
| 6 | <--- | 0.64 | 0.016 | 0.516 | 39.041 | <0.001 | ||
| 7 | <--- | 0.671 | 0.019 | 0.46 | 34.891 | <0.001 | ||
| 8 | <--- | 0.715 | 0.018 | 0.539 | 40.769 | <0.001 | ||
| 9 | <--- | 1.031 | 0.018 | 0.773 | 57.062 | <0.001 | ||
| 10 | <--- | 1.033 | 0.018 | 0.787 | 57.901 | <0.001 | ||
| 11 | <--- | 1 | 0.718 | |||||
| 12 | <--- | Self-rated physiological health | 0.677 | 0.025 | 0.402 | 26.658 | <0.001 | 0.84 |
| 13 | <--- | 0.985 | 0.031 | 0.503 | 31.536 | <0.001 | ||
| 14 | <--- | 0.89 | 0.036 | 0.371 | 25.007 | <0.001 | ||
| 15 | <--- | 0.883 | 0.027 | 0.531 | 32.661 | <0.001 | ||
| 16 | <--- | 0.966 | 0.029 | 0.542 | 32.933 | <0.001 | ||
| 17 | <--- | 0.965 | 0.029 | 0.534 | 32.785 | <0.001 | ||
| 18 | <--- | 1.191 | 0.032 | 0.669 | 37.786 | <0.001 | ||
| 19 | <--- | 1.235 | 0.034 | 0.636 | 36.743 | <0.001 | ||
| 20 | <--- | 1.116 | 0.032 | 0.57 | 34.387 | <0.001 | ||
| 21 | <--- | 0.932 | 0.029 | 0.511 | 31.868 | <0.001 | ||
| 22 | <--- | 0.964 | 0.03 | 0.528 | 32.589 | <0.001 | ||
| 23 | <--- | 0.873 | 0.029 | 0.478 | 30.371 | <0.001 | ||
| 24 | <--- | 0.819 | 0.02 | 0.483 | 40.787 | <0.001 | ||
| 25 | <--- | 1 | 0.537 | |||||
| 26 | <--- | Self-rated psychological health | 1.692 | 0.05 | 0.611 | 33.823 | <0.001 | 0.876 |
| 27 | <--- | 1.319 | 0.042 | 0.527 | 31.069 | <0.001 | ||
| 28 | <--- | 1.313 | 0.042 | 0.535 | 31.36 | <0.001 | ||
| 29 | <--- | 1.565 | 0.048 | 0.577 | 32.766 | <0.001 | ||
| 30 | <--- | 1.397 | 0.042 | 0.593 | 33.225 | <0.001 | ||
| 31 | <--- | 1.414 | 0.04 | 0.683 | 35.764 | <0.001 | ||
| 32 | <--- | 1.788 | 0.049 | 0.712 | 36.306 | <0.001 | ||
| 33 | <--- | 1.69 | 0.047 | 0.709 | 36.224 | <0.001 | ||
| 34 | <--- | 1.915 | 0.053 | 0.71 | 36.422 | <0.001 | ||
| 35 | <--- | 1.714 | 0.048 | 0.68 | 35.724 | <0.001 | ||
| 36 | <--- | 1.126 | 0.031 | 0.46 | 36.231 | <0.001 | ||
| 37 | <--- | 1 | 0.483 | |||||
| 38 | <--- | Self-rated social health | 1.325 | 0.041 | 0.638 | 32.143 | <0.001 | 0.861 |
| 39 | <--- | 1.483 | 0.045 | 0.693 | 33.283 | <0.001 | ||
| 40 | <--- | 1.32 | 0.041 | 0.647 | 32.215 | <0.001 | ||
| 41 | <--- | 1.344 | 0.042 | 0.65 | 32.354 | <0.001 | ||
| 42 | <--- | 1.741 | 0.052 | 0.692 | 33.343 | <0.001 | ||
| 43 | <--- | 1.564 | 0.049 | 0.636 | 32.027 | <0.001 | ||
| 44 | <--- | 1.656 | 0.05 | 0.7 | 33.436 | <0.001 | ||
| 45 | <--- | 1.322 | 0.036 | 0.617 | 37.057 | <0.001 | ||
| 46 | <--- | 1 | 0.458 | |||||
| Path | Estimate | S.E. | Standardized Estimate | C.R. | p | ||
|---|---|---|---|---|---|---|---|
| Stress management | <--- | Purpose in life | 1.132 | 0.019 | 0.589 | 60.241 | <0.001 |
| SRH | <--- | Purpose in life | 1.817 | 0.09 | 0.319 | 20.13 | <0.001 |
| SRH | <--- | Stress management | 1.227 | 0.038 | 0.414 | 32.17 | <0.001 |
| 2/df | SRMR | GFI | AGFI | PGFI | NFI | IFI | TLI | CFI | RMSEA |
|---|---|---|---|---|---|---|---|---|---|
| 25.721 | 0.011 | 0.997 | 0.978 | 0.133 | 0.996 | 0.997 | 0.983 | 0.997 | 0.06 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, F.; Chen, J.; Yu, L.; Jing, Y.; Jiang, P.; Fu, X.; Wu, S.; Sun, X.; Luo, R.; Kwan, H.; et al. The Role of Stress Management in the Relationship between Purpose in Life and Self-Rated Health in Teachers: A Mediation Analysis. Int. J. Environ. Res. Public Health 2016, 13, 719. https://doi.org/10.3390/ijerph13070719
Li F, Chen J, Yu L, Jing Y, Jiang P, Fu X, Wu S, Sun X, Luo R, Kwan H, et al. The Role of Stress Management in the Relationship between Purpose in Life and Self-Rated Health in Teachers: A Mediation Analysis. International Journal of Environmental Research and Public Health. 2016; 13(7):719. https://doi.org/10.3390/ijerph13070719
Chicago/Turabian StyleLi, Fei, Jieyu Chen, Lin Yu, Yuan Jing, Pingping Jiang, Xiuqiong Fu, Shengwei Wu, Xiaomin Sun, Ren Luo, Hiuyee Kwan, and et al. 2016. "The Role of Stress Management in the Relationship between Purpose in Life and Self-Rated Health in Teachers: A Mediation Analysis" International Journal of Environmental Research and Public Health 13, no. 7: 719. https://doi.org/10.3390/ijerph13070719