
Use of a Sampling Area-Adjusted Adenosine Triphosphate Bioluminescence Assay Based on Digital Image Quantification to Assess the Cleanliness of Hospital Surfaces


Abstract
:1. Introduction
2. Materials and Methods
2.1. Phase One
2.1.1. Hospital Cleaning Methods
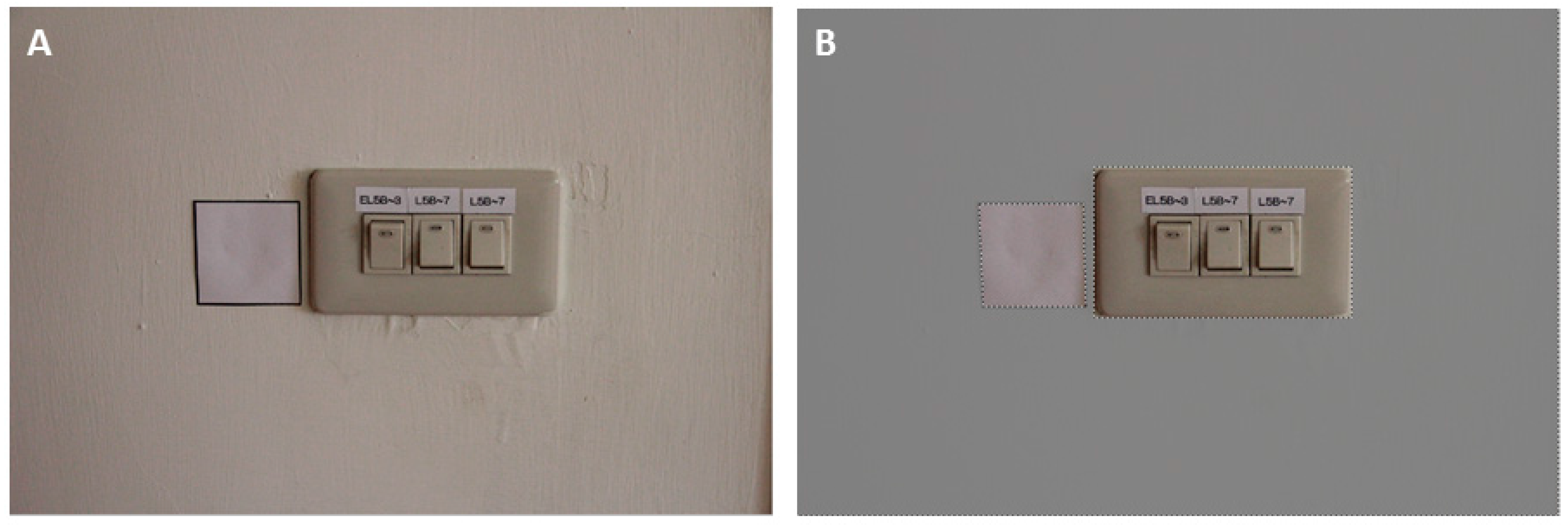
2.1.2. Sampling Sites and Determining the Sampling Areas
2.1.3. ATP Bioluminescence and Microbiological Assessment
2.2. Phase Two
2.3. Test Standards and Pass Rates
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Boyce, J.M.; Havill, N.L.; Dumigan, D.G.; Golebiewski, M.; Balogun, O.; Rizvani, R. Monitoring the effectiveness of hospital cleaning practices by use of an adenosine triphosphate bioluminescence assay. Infect. Control Hosp. Epidemiol. 2009, 30, 678–684. [Google Scholar] [CrossRef] [PubMed]
- Amodio, E.; Dino, C. Use of ATP bioluminescence for assessing the cleanliness of hospital surfaces: A review of the published literature (1990–2012). J. Infect. Public Health 2014, 7, 92–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boyce, J.M.; Havill, N.L.; Havill, H.L.; Mangione, E.; Dumigan, D.G.; Moore, B.A. Comparison of fluorescent marker systems with 2 quantitative methods of assessing terminal cleaning practices. Infect. Control Hosp. Epidemiol. 2011, 32, 1187–1193. [Google Scholar] [CrossRef] [PubMed]
- Griffith, C.J.; Cooper, R.A.; Gilmore, J.; Davies, C.; Lewis, M. An evaluation of hospital cleaning regimes and standards. J. Hosp. Infect. 2000, 45, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Mulvey, D.; Redding, P.; Robertson, C.; Woodall, C.; Kingsmore, P.; Bedwell, D.; Dancer, S.J. Finding a benchmark for monitoring hospital cleanliness. J. Hosp. Infect. 2011, 77, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Cooper, R.A.; Griffith, C.J.; Malik, R.E.; Obee, P.; Looker, N. Monitoring the effectiveness of cleaning in four British hospitals. Am. J. Infect. Control 2007, 35, 338–341. [Google Scholar] [CrossRef] [PubMed]
- Smith, P.W.; Sayles, H.; Hewlett, A.; Cavalieri, R.J.; Gibbs, S.G.; Rupp, M.E. A study of three methods for assessment of hospital environmental cleaning. Healthc. Infect. 2013, 18, 80–85. [Google Scholar] [CrossRef]
- White, L.F.; Dancer, S.J.; Robertson, C.; McDonald, J. Are hygiene standards useful in assessing infection risk? Am. J. Infect. Control 2008, 36, 381–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, R.; Young, V.; Stewart, M.; Robertson, C.; Dancer, S. Cleanliness audit of clinical surfaces and equipment: Who cleans what? J. Hosp. Infect. 2011, 78, 178–181. [Google Scholar] [CrossRef] [PubMed]
- Whiteley, G.S.; Derry, C.; Glasbey, T.; Fahey, P. The perennial problem of variability in adenosine triphosphate (ATP) tests for hygiene monitoring within healthcare settings. Infect. Control Hosp. Epidemiol. 2015, 36, 658–663. [Google Scholar] [CrossRef] [PubMed]
- Clasen, T.; Edmondson, P. Sodium dichloroisocyanurate (NaDCC) tablets as an alternative to sodium hypochlorite for the routine treatment of drinking water at the household level. Int. J. Hyg. Environ. Health 2006, 209, 173–181. [Google Scholar] [CrossRef] [PubMed]
- Mazzola, P.G.; Penna, T.C.; da S Martins, A.M. Determination of decimal reduction time (D value) of chemical agents used in hospitals for disinfection purposes. BMC Infect. Dis. 2003, 3, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nascimento, M.; Silva, N.; Catanozi, M.; Silva, K. Effects of different disinfection treatments on the natural microbiota of lettuce. J. Food Protect. 2003, 66, 1697–1700. [Google Scholar]
- Chen, B.; Fu, Z.; Pan, Y.; Wang, J.; Zeng, Z. Single leaf area measurement using digital camera image. In Computer and Computing Technologies in Agriculture IV; Li, D., Liu, Y., Chen, Y., Eds.; Springer: Berlin, Germany; Heidelberg, Germany, 2011; Volume 345, pp. 525–530. [Google Scholar]
- Chaudary, P.; Godara, S. Fast and accurate method for leaf area measurement. Int. J. Comput. Appl. 2012, 49, 22–25. [Google Scholar] [CrossRef]
- Venkateswaran, K.; Hattori, N.; La Duc, M.T.; Kern, R. ATP as a biomarker of viable microorganisms in clean-room facilities. J. Microbiol. Methods 2003, 52, 367–377. [Google Scholar] [CrossRef]
- Hsiao, P.-K.; Chen, W.-T.; Chang, K.-C.; Ke, Y.-J.; Kuo, C.-L.; Tseng, C.-C. Performance of CHROMagar Staph aureus and CHROMagar MRSA for detection of airborne methicillin-resistant and methicillin-sensitive Staphylococcus aureus. Aerosol Sci. Technol. 2012, 46, 297–308. [Google Scholar] [CrossRef]
- Hsiao, P.-K.; Cheng, C.-C.; Chang, K.-C.; Yiin, L.-M.; Hsieh, C.-J.; Tseng, C.-C. Performance of CHROMagar VRE Medium for the Detection of Airborne Vancomycin-Resistant/Sensitive Enterococcus Species. Aerosol Sci. Technol. 2014, 48, 173–183. [Google Scholar] [CrossRef]
- Boyce, J.M.; Havill, N.L.; Lipka, A.; Havill, H.; Rizvani, R. Variations in hospital daily cleaning practices. Infect. Control Hosp. Epidemiol. 2010, 31, 99–101. [Google Scholar] [CrossRef] [PubMed]
- Lewis, T.; Griffith, C.; Gallo, M.; Weinbren, M. A modified ATP benchmark for evaluating the cleaning of some hospital environmental surfaces. J. Hosp. Infect. 2008, 69, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Moore, G.; Smyth, D.; Singleton, J.; Wilson, P. The use of adenosine triphosphate bioluminescence to assess the efficacy of a modified cleaning program implemented within an intensive care setting. Am. J. Infect. Control 2010, 38, 617–622. [Google Scholar] [CrossRef] [PubMed]
- Sherlock, O.; O‘Connell, N.; Creamer, E.; Humphreys, H. Is it really clean? An evaluation of the efficacy of four methods for determining hospital cleanliness. J. Hosp. Infect. 2009, 72, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Willis, C.; Morley, R.; Westbury, J.; Greenwood, M.; Pallett, A. Evaluation of ATP bioluminescence swabbing as a monitoring and training tool for effective hospital cleaning. Br. J. Infect. Control 2007, 8, 17–21. [Google Scholar] [CrossRef]
- Ferreira, A.M.; Andrade, D.D.; Rigotti, M.A.; Ferreira, M.V.F. Condition of cleanliness of surfaces close to patients in an intensive care unit. Rev. Lat. Am. Enferm. 2011, 19, 557–564. [Google Scholar] [CrossRef]
- Goodman, E.R.; Platt, R.; Bass, R.; Onderdonk, A.B.; Yokoe, D.S.; Huang, S.S. Impact of an environmental cleaning intervention on the presence of methicillin-resistant Staphylococcus aureus and vancomycin-resistant enterococci on surfaces in intensive care unit rooms. Infect. Control Hosp. Epidemiol. 2008, 29, 593–599. [Google Scholar] [CrossRef] [PubMed]
- Hayden, M.K.; Bonten, M.J.; Blom, D.W.; Lyle, E.A.; van de Vijver, D.A.; Weinstein, R.A. Reduction in acquisition of vancomycin-resistant enterococcus after enforcement of routine environmental cleaning measures. Clin. Infect. Dis. 2006, 42, 1552–1560. [Google Scholar] [CrossRef] [PubMed]
- Kusumaningrum, H.D.; Paltinaite, R.; Koomen, A.J.; Hazeleger, W.C.; Rombouts, F.M.; Beumer, R.R. Tolerance of Salmonella enteritidis and Staphylococcus aureus to surface cleaning and household bleach. J. Food Prot. 2003, 66, 2289–2295. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Surface | Before Intervention | After Intervention | ||||
|---|---|---|---|---|---|---|
| Pre-Clean (Range) | Post-Clean (Range) | p | Pre-Clean (Range) | Post-Clean (Range) | p | |
| bedside rails | 17.7 (3.9–144.7) | 4.4 (0.6–75.4) | 0.06 | 24.5 (7.2–298.1) | 3.3 (0.7–95.0) | 0.11 |
| bedside tables | 1.9 (0.2–22.6) | 0.3 (0.1–3.7) | 0.02 | 1.8 (0.6–7.7) | 0.3 (0.2–1.0) | 0.00 |
| chairs | 10.2 (1.6–259.8) | 9.1 (0.2–19.6) | 0.04 | 6.0 (1.2–59.1) | 5.3 (0.3–287.4) | 0.53 |
| doorknobs | 325.2 (31.3–33130) | 41.1 (8.0–10698.2) | 0.53 | 36.1 (11.8–1202.9) | 12.1 (2.5–160.4) | 0.01 |
| drawer handles | 49.6 (15.2–260.1) | 17.7 (2.4–102.7) | 0.05 | 16.5 (8.5–90.3) | 5.2 (2.2–789.6) | 0.05 |
| emergency buttons | 15.9 (3.4–200.1) | 14.2 (2.2–50.2) | 0.14 | 13.7 (2.6–116.5) | 4.8 (0.8–21.7) | 0.03 |
| light switches | 10.7 (2.4–207.3) | 5.0 (3.4–16.6) | 0.02 | 5.0 (1.6–114.2) | 2.4 (0.4–149.7) | 0.09 |
| hand sanitizer pump | 0.8 (0.3–6.9) | 0.9 (0.3–7.0) | 0.86 | 0.7 (0.3–9.8) | 0.1 (0–2.2) | 0.26 |
| toilet flush handles | 205.0 (9.0–1049.7) | 75.2 (27.2–1532.6) | 0.21 | 23.6 (8.5–249.7) | 10.8 (2.9–1134.0) | 0.29 |
| toilet safety rails | 8.5 (0.6–65.4) | 5.3 (0.5–17.7) | 0.09 | 1.5 (0.4–162.3) | 5.3 (0.2–114.6) | 0.93 |
| wardrobe handles | 288.6 (16.0–992.0) | 80.0 (15.4–2564.0) | 0.21 | 205.5 (4.6–1920.3) | 164.6 (012.6–2019.7) | 0.86 |
| Surface | Before Intervention | After Intervention | ||||
|---|---|---|---|---|---|---|
| Pre-Clean (Range) | Post-Clean (Range) | p | Pre-Clean (Range) | Post-Clean (Range) | p | |
| bedside rails | 15.0 (0.4–587.9) | 0.7 (0.0–19.3) | 0.00 | 15.9 (0.0–107.5) | 3.9 (0.2–3434.2) | 0.09 |
| bedside tables | 1.7 (0.0–88.3) | 0.1 (0.0–7.1) | 0.00 | 6.2 (0.0–248.1) | 0.2 (0.0–2.3) | 0.00 |
| chairs | 34.7 (1.8–330.0) | 0.6 (0.0–49.4) | 0.00 | 3.8 (0.0–450.0) | 0.9 (0.0–179.4) | 0.08 |
| doorknobs | 50.9 (0.0–1198.2) | 14.3 (0.0–141.1) | 0.04 | 28.6 (0.0–23026.8) | 1.8 (0.0–312.5) | 0.00 |
| drawer handles | 28.4 (0.0–958.2) | 1.2 (0.0–2274.0) | 0.43 | 15.8 (0.0–3486.6) | 0.9 (0.0–23.9) | 0.00 |
| emergency buttons | 14.6 (0.0–1761.0) | 4.4 (0.0–58.5) | 0.12 | 2.4 (0.0–37.1) | 0.0 (0.0–13268.3) | 0.09 |
| light switches | 10.0 (0.0–34.1) | 2.9 (0.0–55.2) | 0.02 | 4.9 (0.0–259.5) | 0.8 (0.0–78.6) | 0.18 |
| hand sanitizer pump | 0.8 (0.0–6.7) | 0.3 (0.0–29.3) | 0.46 | 0.5 (0.0–41.6) | 0.0 (0.0–17.0) | 0.04 |
| toilet flush handles | 51.9 (0.0–690.7) | 23.9 (0.0–561.4) | 0.09 | 2.1 (0.0–17381.1) | 2.8 (0.0–13.2.2) | 0.07 |
| toilet safety rails | 3.8 (0.0–17.9) | 0.8 (0.0–112.7) | 0.60 | 12.8 (0.0–1187.2) | 5.9 (0.0–4738.2) | 0.59 |
| wardrobe handles | 32.3 (0.0–584.6) | 9.2 (0.0–3750.8) | 0.15 | 18.5 (0.0–2200.0) | 9.2 (0.0–2935.4) | 0.81 |
| Species | Before Intervention | Species | After Intervention | ||||
|---|---|---|---|---|---|---|---|
| Pre-Clean (Range) | Post-Clean (Range) | p | Pre-Clean (Range) | Post-Clean (Range) | p | ||
| CRAB (n = 2) | 101.7 (0.0–201.8) | N.D. | < 0.01 | CRAB (n = 10) | 8.5 (0.0–16.1) | 0.5 (0.0–0.6) | < 0.01 |
| VRE (n = 11) | 0.98 (0.0–32.1) | 0.0 (0.0–0.1) | VRE (n = 4) | 1.5 (0.0–8.4) | N.D. | ||
| MRSA (n = 48) | 1.1 (0.0–50.0) | 0.0 (0.0–6.2) | MRSA (n = 45) | 0.9 (0.0–447.3) | 0.0 (0.0–5.4) | ||
| Standard | <2.5 CFU/cm2 [3,5,7,20,22] | p * | <5 RLU/cm2 [22] | p * | <10 RLU/cm2 [23] | p * | <250 RLU [1,3,5,19,20,21] | p * | <500 RLU [4,6,21] | p * |
|---|---|---|---|---|---|---|---|---|---|---|
| Before intervention | 55/121 (45) | 0.004 | 47/121 (39) | 0.052 | 63/121 (52) | 0.017 | 65/121 (54) | 0.003 | 86/121 (71) | 0.082 |
| After intervention | 78/121 (64) | 63/121 (52) | 82/121 (68) | 88/121 (73) | 96/119 (81) |
| Microbial Species | CRAB | p * | MRSA | p * | VRE | p * |
|---|---|---|---|---|---|---|
| Before intervention | 110/121 (91) | 0.669 | 65/121 (54) | 0.703 | 107/121 (88) | 0.711 |
| After intervention | 112/121 (93) | 63/121 (52) | 109/121 (90) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ho, Y.-H.; Wang, L.-S.; Jiang, H.-L.; Chang, C.-H.; Hsieh, C.-J.; Chang, D.-C.; Tu, H.-Y.; Chiu, T.-Y.; Chao, H.-J.; Tseng, C.-C. Use of a Sampling Area-Adjusted Adenosine Triphosphate Bioluminescence Assay Based on Digital Image Quantification to Assess the Cleanliness of Hospital Surfaces. Int. J. Environ. Res. Public Health 2016, 13, 576. https://doi.org/10.3390/ijerph13060576
Ho Y-H, Wang L-S, Jiang H-L, Chang C-H, Hsieh C-J, Chang D-C, Tu H-Y, Chiu T-Y, Chao H-J, Tseng C-C. Use of a Sampling Area-Adjusted Adenosine Triphosphate Bioluminescence Assay Based on Digital Image Quantification to Assess the Cleanliness of Hospital Surfaces. International Journal of Environmental Research and Public Health. 2016; 13(6):576. https://doi.org/10.3390/ijerph13060576
Chicago/Turabian StyleHo, Yu-Huai, Lih-Shinn Wang, Hui-Li Jiang, Chih-Hui Chang, Chia-Jung Hsieh, Dan-Chi Chang, Hsin-Yu Tu, Tan-Yun Chiu, Huei-Jen Chao, and Chun-Chieh Tseng. 2016. "Use of a Sampling Area-Adjusted Adenosine Triphosphate Bioluminescence Assay Based on Digital Image Quantification to Assess the Cleanliness of Hospital Surfaces" International Journal of Environmental Research and Public Health 13, no. 6: 576. https://doi.org/10.3390/ijerph13060576