
H-Type Hypertension and C Reactive Protein in Recurrence of Ischemic Stroke

Abstract
:1. Introduction
2. Materials and Methods
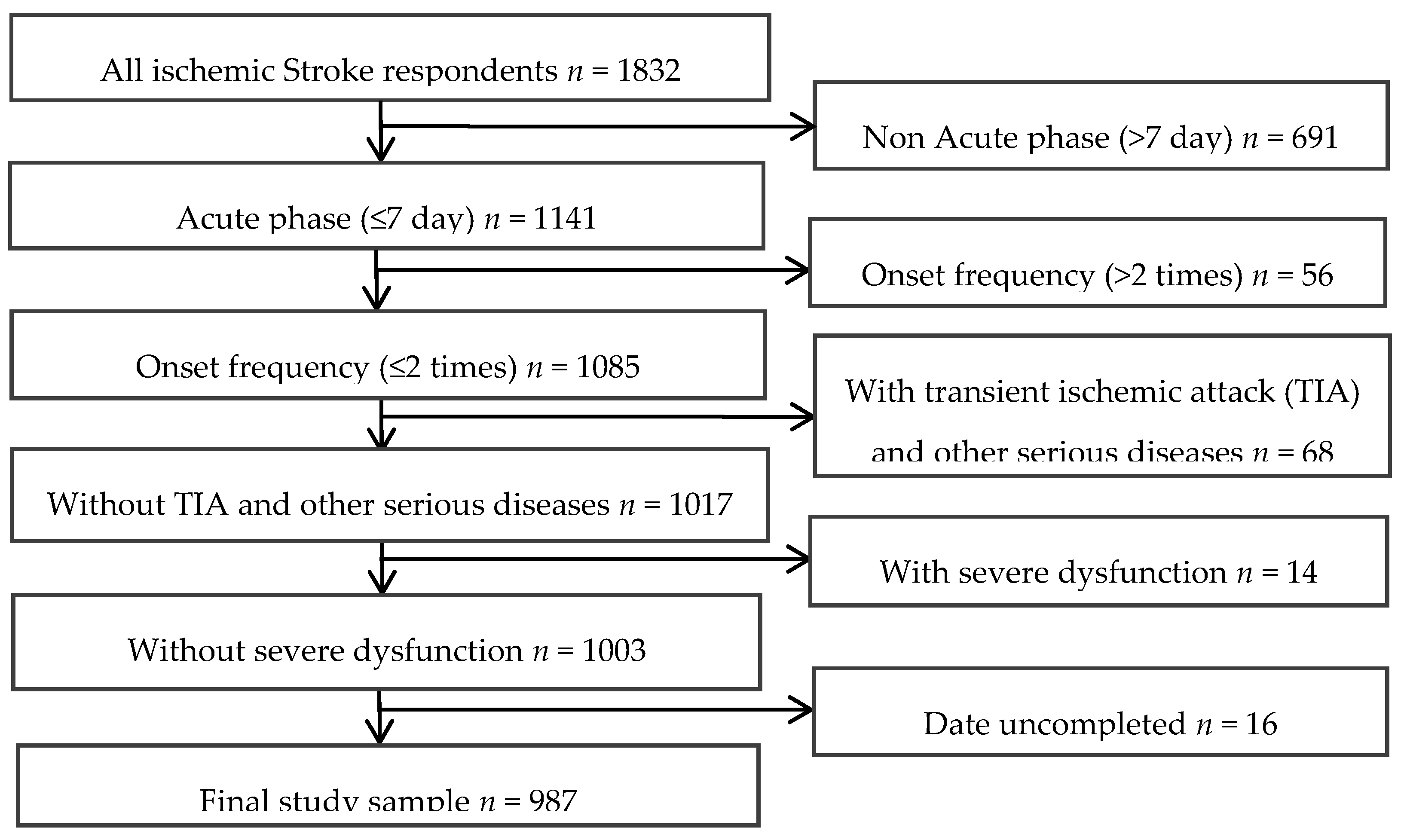
2.1. Study Subjects
2.1.1. Socio-Demographic and Lifestyle Variables
2.1.2. Blood Collection and Laboratory Test
2.2. Statistical Analysis
3. Results
3.1. General Characteristics of Subjects
3.2. The Effect of CRP, Hypertension and HHcy on the Incidence of RIS
3.3. Multivariate Logistic Regression Analysis
4. Discussion
5. Limitations of the Study
6. Conclusions
Acknowledgments
Author Contributions
Abbreviations
| CRP | C reactive protein |
| RIS | Recurrent ischemic stroke |
| FIS | First-ever ischemic stroke |
| Hcy | Homocysteine |
References
- Ministry of Health, People’s Republic of China. The main situation of the third National Death survey. Chin. J. Oncol. 2008, 17, 344–345. [Google Scholar]
- Hardie, K.; Hankey, G.J.; Jamrozik, K.; Broadhurst, R.J.; Anderson, C. Ten-year risk of first recurrent stroke and disability after first ever stroke in the Perth Community stroke study. Stroke 2004, 35, 731–735. [Google Scholar] [CrossRef] [PubMed]
- Leoo, T.; Lindgren, A.; Petersson, J.; von Arbin, M. Risk factors and treatment at recurrent stroke onset: Results from the Recurrent Stroke Quality and Epidemiology (RESQUE) Study. Cerebrovasc. Dis. 2008, 25, 254–260. [Google Scholar] [CrossRef] [PubMed]
- Ueshima, H.; Choudhury, S.R.; Okayama, A.; Hayakawa, T.; Kita, Y.; Kadowaki, T.; Okamura, T.; Minowa, M.; Iimura, O. Cigarette smoking as a risk factor for stroke death in Japan: NIPPON DATA80. Stroke 2004, 35, 1836–1841. [Google Scholar] [CrossRef] [PubMed]
- Turan, T.N.; Cotsonis, G.; Lynn, M.J.; Chaturvedi, S.; Chimowitz, M.; Warfarin–Aspirin Symptomatic Intracranial Disease (WASID) Trial Investigators. Relationship between blood pressure and stroke recurrence in patients with intracranial arterial stenosis. Circulation 2007, 115, 2969–2975. [Google Scholar] [CrossRef] [PubMed]
- Laloux, P.; Lemonnier, F.; Jamart, J. Risk factors and treatment of stroke at the time of recurrence. Acta Neurol. Belg. 2010, 110, 299–302. [Google Scholar] [PubMed]
- Zhang, Y.; Huo, Y. Hypertension with Elevated Homocysteine—H-Type Hypertension. Adv. Cardiovasc. Dis. 2011, 32, 3–6. [Google Scholar]
- Hu, D.; Xu, X. Prevention of stroke relies on valid control H-type hypertension. Chin. J. Intern. Med. 2008, 47, 976–977. (In Chinese) [Google Scholar]
- Towfighi, A.; Markovic, D.; Ovbiagele, B. Pronounced association of elevated serum homocysteine with stroke in subgroups of individuals: A nationwide study. J. Neurol. Sci. 2010, 298, 153–157. [Google Scholar] [CrossRef] [PubMed]
- Ridker, P.M. C-reactive protein: Eighty years from discovery to emergence as a major risk marker for cardiovascular disease. Clin. Chem. 2009, 55, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Schillinger, M.; Exner, M.; Mlekusch, W.; Sabeti, S.; Amighi, J.; Nikowitsch, R.; Timmel, E.; Kickinger, B.; Minar, C.; Pones, M.; et al. Inflammation and Carotid Artery—Risk for Atherosclerosis Study (ICARAS). Circulation 2005, 111, 2203–2209. [Google Scholar] [CrossRef] [PubMed]
- Kotlęga, D.; Białecka, M.; Kurzawski, M.; Droździk, M.; Ciećwież, S.; Gołąb-Janowska, M.; Nowacki, P. Risk factors of stroke and -717A>G (rs2794521) CRP gene polymorphism among stroke patients in West Pomerania province of Poland. Neurol. Neurochir. Pol. 2014, 48, 30–34. [Google Scholar] [CrossRef] [PubMed]
- The Neuroscience Society. All kinds of cerebrovascular disease diagnosis points. Chin. J. Neurol. 1996, 29, 379. [Google Scholar]
- Morris, D.L.; Rosamond, W.; Madden, K.; Schultz, C.; Hamilton, S. Prehospital and emergency department delays after acute stroke: The Genentech Stroke Presentation Survey. Stroke 2000, 31, 2585–2590. [Google Scholar] [CrossRef] [PubMed]
- Qin, X.; Huo, Y. H Type hypertension, stroke and diabetes in China: Opportunities for primary prevention. J. Diabetes 2016, 8, 38–40. [Google Scholar] [CrossRef] [PubMed]
- McCully, K.S. Homocysteine, vitamins, and vascular disease prevention. Homocysteine, vitamins, and vascular disease prevention. Am. J. Clin. Nutr. 2007, 86, 1563–1568. [Google Scholar]
- Asplund, K.; Karvanen, J.; Giampaoli, S.; Jousilahti, P.; Niemelä, M.; Broda, G.; Cesana, G.; Dallongeville, J.; Ducimetriere, P.; Evans, A.; et al. Relative Risks for Stroke by Age, Sex, and Population Based on Follow-Up of 18 European Populations in the MORGAM Project. Stroke 2009, 40, 2319–2326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinho, J.; Braga, C.G.; Rocha, S.; Santos, A.F.; Gomes, A.; Cabreiro, A.; Magalhães, S.; Ferreira, C. Atrial ectopic activity in cryptogenic ischemic stroke and TIA: A risk factor for recurrence. Natl. Stroke Assoc. 2015, 24, 507–510. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.; Ma, Z.Y.; Shi, L.N. Risk factors of recurrence in patients with ischemic stroke in Ningxia area of China. J. Ningxia Med. Coll. 2014, 36, 401–404. [Google Scholar]
- Wang, X.; Shi, J.X. Study on the related factors of recurrence in patients with ischemic stroke. Chin. J. Postgrad. Med. 2006, 13, 44–45. [Google Scholar]
- Modrego, P.J.; Pina, M.A.; Fraj, M.M.; Llorens, N. Type, causes, and prognosis of stroke recurrence in the province of Teruel, Spain. A 5-year analysis. Neurol. Sci. 2000, 21, 355–360. [Google Scholar] [CrossRef] [PubMed]
- Hillen, T.; Coshall, C.; Tilling, K.; Rudd, A.G.; McGovern, R.; Wolfe, C.D.; South London Stroke Register. Cause of stroke recurrence is multifactorial: Patterns, risk factors, and outcomes of stroke recurrence in the South London stroke register. Stroke 2003, 34, 1457–1463. [Google Scholar] [CrossRef] [PubMed]
- Hankey, G.J.; Jamrozik, K.; Broadhurst, R.J.; Forbes, S.; Burvill, P.W.; Anderson, C.S.; Stewart-Wynne, E.G. Long-term risk of first recurrent stroke in the Perth Community Stroke Study. Stroke 1998, 29, 2491–2500. [Google Scholar] [CrossRef] [PubMed]
- Hankey, G.J.; Jamrozik, K.; Broadhurst, R.J.; Forbes, S.; Burvill, P.W.; Anderson, C.S.; Stewart-Wynne, E.G. Diabetes is an Independent Risk Factor for Stroke Recurrence in Stroke Patients: A Meta-analysis. J. Stroke Cerebrovasc. Dis. 2015, 24, 1961–1968. [Google Scholar]
- Han, J.H.; Ho, S.S.; Lam, W.W.; Wong, K.S. Total cerebral blood flow estimated by color velocity imaging quantification ultrasound: A predictor for recurrent stroke. J. Cereb. Blood Flow Metab. 2007, 27, 850–856. [Google Scholar] [CrossRef] [PubMed]
- Mather, K.J.; Steinberg, H.O.; Baron, A.D. Insulin resistance in the vasculature. J. Clin. Investig. 2013, 123, 1003–1004. [Google Scholar] [CrossRef] [PubMed]
- Schoch, H.J.; Fischer, S.; Marti, H.H. Hypoxia-induced vascular endothelial growth factor expression causes vascular leak age in the brain. Brain 2002, 125, 2549–2557. [Google Scholar] [CrossRef] [PubMed]
- Capes, S.E.; Hunt, D.; Malmberg, K.; Pathak, P.; Gerstein, H.C. Stress hyperglycemia and prognosis of stroke in nondiabetic and diabetic patients: A systematic overview. Stroke 2001, 32, 2426–2432. [Google Scholar] [CrossRef] [PubMed]
- Venugopal, S.K.; Devaraj, S.; Jialal, I. Effect of C-reactive protein on vascular cells: Evidence for a proinflammatory, proatherogenic role. Curr. Opin. Nephrol. Hypertens. 2005, 14, 33–37. [Google Scholar] [CrossRef] [PubMed]
- Di Napoli, M.; Schwaninger, M.; Cappelli, R.; Ceccarelli, E.; di Gianfilippo, G.; Donati, C.; Emsley, H.C.; Forconi, S.; Hopkins, S.J.; Masotti, L.; et al. Evaluation of C-reactive protein measurement for assessing the risk and prognosis in ischemic stroke: A statement for health care professionals from the CRP Pooling Project members. Stroke 2005, 36, 1316–1329. [Google Scholar] [CrossRef] [PubMed]
- Curb, J.D.; Abbott, R.D.; Rodriguez, B.L.; Sakkinen, P.; Popper, J.S.; Yano, K.; Tracy, R.P. C-reactive protein and the future risk of thromboembolic stroke in healthy men. Circulation 2003, 107, 2016–2020. [Google Scholar] [CrossRef] [PubMed]
- Elkind, M.S.; Luna, J.M.; Moon, Y.P.; Liu, K.M.; Spitalnik, S.L.; Paik, M.C.; Sacco, R.L. High-sensitivity C-reactive protein predicts mortality but not stroke in a multi-ethnic cohort: The Northern Manhattan Study. Neurology 2009, 73, 1300–1307. [Google Scholar] [CrossRef] [PubMed]
- Gussekloo, J.; Schaap, M.C.; Frölich, M.; Blauw, G.J.; Westendorp, R.G. C-reactive protein is a strong but nonspecific risk factor of fatal stroke in elderly persons. Arterioscler. Thromb. Vasc. Biol. 2000, 20, 1047–1451. [Google Scholar] [CrossRef] [PubMed]
- Di Napoli, M.; Papa, F.; Bocola, V. Prognostic Influence of Increased C-Reactive Protein and Fibrinogen Levels in Ischemic Stroke. Stroke 2001, 32, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Elkind, M.S.; Luna, J.M.; McClure, L.A.; Zhang, Y.; Coffey, C.S.; Roldan, A.; Del Brutto, O.H.; Pretell, E.J.; Pettigrew, L.C.; Meyer, B.C.; et al. C-reactive protein as a prognostic marker after lacunar stroke: Levels of inflammatory markers in the treatment of stroke study. Stroke 2014, 45, 707–716. [Google Scholar] [CrossRef] [PubMed]
- Wakugawa, Y.; Kiyohara, Y.; Tanizaki, Y.; Kubo, M.; Ninomiya, T.; Hata, J.; Doi, Y.; Okubo, K.; Oishi, Y.; Shikata, K.; et al. C-reactive protein and risk of first-ever ischemic and hemorrhagic stroke in a general Japanese population: The Hisayama Study. Stroke 2006, 37, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Song, I.U.; Kim, Y.D.; Kim, J.S.; Lee, K.S.; Chung, S.W. Can high-sensitivity C-reactive protein and plasma homocysteine levels independently predict the prognosis of patients with functional disability after first-ever ischemic stroke? Eur. Neurol. 2010, 64, 304–310. [Google Scholar] [CrossRef] [PubMed]
- Lorenz, M.W.; Karbstein, P.; Markus, H.S.; Sitzer, M. High-sensitivity C-reactive protein is not associated with carotid intima-media progression: The carotid atherosclerosis progression study. Stroke 2007, 38, 1774–1779. [Google Scholar] [CrossRef] [PubMed]
- Chapman, C.M.; Beilby, J.P.; McQuillan, B.M.; Thompson, P.L.; Hung, J. Monocyte count, but not C-reactive protein or interleukin-6, is an independent risk marker for subclinical carotid atherosclerosis. Stroke 2004, 35, 1619–1624. [Google Scholar] [CrossRef] [PubMed]
- Kharbanda, R.K.; Walton, B.; Allen, M.; Klein, N.; Hingorani, A.D.; MacAllister, R.J.; Vallance, P. Prevention of inflammation-induced endothelial dysfunction: A novel vasculo-protective action of aspirin. Circulation 2002, 105, 2600–2604. [Google Scholar] [CrossRef] [PubMed]
- Albert, M.A.; Ridker, P.M. The role of C-reactive protein in cardiovascular disease risk. Curr. Cardiol. Rep. 1999, 1, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Sen, U.; Mishra, P.K.; Tyagi, N.; Tyagi, S.C. Homocysteine to hydrogen sulfide or hypertension. Cell Biochem. Biophys. 2010, 57, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Sun, K.; Chen, J.; Liao, Y.; Qin, Q.; Ma, A.; Wang, D.; Zhu, Z.; Wang, Y.; Hui, R. High plasma homocysteine levels contribute to the risk of stroke recurrence and all-cause mortality in a large prospective stroke population. Clin. Sci. (Lond.) 2009, 118, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Xu, G.; Liu, X.; Wu, W.; Zhang, R.; Yin, Q. Recurrence after ischemic stroke in Chinese patients: Impact of uncontrolled modifiable risk factors. Cerebrovasc. Dis. 2007, 23, 117–120. [Google Scholar] [CrossRef] [PubMed]
- Aiyagari, V.; Badruddin, A. Management of hypertension in acute stroke. Expert Rev. Cardiovasc. Ther. 2009, 7, 637–646. [Google Scholar] [CrossRef] [PubMed]
- Saposnik, G.; Ray, J.G.; Sheridan, P.; McQueen, M.; Lonn, E.; Heart Outcomes Prevention Evaluation 2 Investigators. Homocysteine-lowering therapy and stroke risk, severity, and disability: Additional findings from the HOPE 2 trial. Stroke 2009, 40, 1365–1372. [Google Scholar] [CrossRef] [PubMed]
- Graham, I.M.; Daly, L.E.; Refsum, H.M.; Robinson, K.; Brattström, L.E.; Ueland, P.M.; Palma-Reis, R.J.; Boers, G.H.; Sheahan, R.G.; Israelsson, B.; et al. Plasma homocysteine as a risk factor for vascular disease. The European Concerted Action Project. J. Am. Med. Assoc. 1997, 277, 1775–1781. [Google Scholar] [CrossRef]
- Mi, G.Q.; Fu, Y.; Mao, J.J.; Xu, M.Z. Relationship between “H type” hypertension and senile recurrent cerebral infarction. Chin. J. Gerontol. 2011, 31, 1859–1860. [Google Scholar]
- Jacob, R.A.; Wu, M.M.; Henning, S.M.; Swendseid, M.E. Homocysteine increases as folate decreases in plasma of healthy men during short-term dietary folate and methyl group restriction. J. Nutr. 1994, 124, 1072–1080. [Google Scholar] [PubMed]
- Yang, H.T.; Lee, M.; Hong, K.S.; Ovbiagele, B.; Saver, J.L. Efficacy of folic acid supplementation in cardiovascular disease prevention: An updated meta-analysis of randomized controlled trials. Eur. J. Intern. Med. 2012, 23, 745–754. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | FIS (n = 753) | RIS (n = 234) | Total (n = 987) | p Value |
|---|---|---|---|---|
| Age (%) | 0.004 | |||
| <60 | 287 (38.1) | 65 (27.8) | 352 (35.7) | |
| ≥60 | 466 (61.9) | 169 (72.2) | 635 (64.3) | |
| Gender, n (%) | 0.001 | |||
| Male | 432 (57.4) | 163 (69.7) | 595 (60.3) | |
| Female | 321 (42.6) | 71 (30.3) | 392 (39.7) | |
| Marital status, n (%) | 0.679 | |||
| Single | 114 (15.1) | 38 (16.2) | 152 (15.4) | |
| Married | 639 (84.9) | 196 (83.8) | 835 (84.6) | |
| Residence, n (%) | 0.010 | |||
| Urban | 410 (54.4) | 150 (64.1) | 560 (56.7) | |
| Rural | 343 (45.6) | 84 (35.9) | 427 (43.3) | |
| Risk factors: | ||||
| Smoking, n (%) | 210 (27.9) | 85 (36.3) | 295 (29.9) | 0.018 |
| Alcohol drinking, n (%) | 171 (22.7) | 54 (23.1) | 225 (22.8) | 0.929 |
| Family history, n (%) | 118 (15.7) | 46 (19.7) | 164 (16.6) | 0.160 |
| Hypertension | 406 (53.9) | 158 (67.5) | 564 (57.1) | <0.001 |
| Diabetes, n (%) | 170 (22.6) | 69 (29.5) | 239 (24.2) | 0.036 |
| Coronary heart disease, n (%) | 97 (12.9) | 31 (13.2) | 128 (13.0) | 0.911 |
| Hyperlipidemia, n (%) | 481 (63.9) | 131 (56.0) | 612 (62.0) | 0.031 |
| Laboratory findings, mean ± SD | ||||
| GLU (mmol/L) | 7.07 ± 0.20 | 7.06 ± 0.34 | 7.07 ± 0.17 | 0.987 |
| UA (μmol/L) | 286.77 ± 6.15 | 285.80 ± 12.62 | 286.54 ± 5.55 | 0.884 |
| FIB (mg/dL) | 305.77 ± 5.27 | 316.63 ± 12.63 | 308.34 ± 5.00 | 0.070 |
| WBC (109/L) | 9.60 ± 2.26 | 11.57 ± 6.84 | 10.07 ± 2.36 | 0.487 |
| RBC (1012/L) | 4.52 ± 0.04 | 5.63 ± 2.30 | 4.79 ± 0.55 | 0.090 |
| PLT (109/L) | 235.96 ± 4.49 | 228.81 ± 9.97 | 234.26 ± 4.16 | 0.151 |
| HCY (μmol/L) | 19.86 ± 1.07 | 21.07 ± 2.02 | 20.15 ± 0.94 | 0.287 |
| CRP (mg/L) | 8.11 ± 1.18 | 16.94 ± 5.08 | 10.20 ± 1,51 | 0.001 |
| HHcy, n (%) | 667 (88.6) | 214 (91.5) | 881 (89.3) | 0.229 |
| High CRP, n (%) | 232 (30.8) | 89 (38.0) | 321 (32.5) | 0.046 |
| Variable | FIS (n = 753) | RIS (n = 234) | χ2 Value | p Value |
|---|---|---|---|---|
| Hypertension and HHcy (%) | 14.989 | 0.002 | ||
| Normal | 46 (88.5) | 6 (11.5) | ||
| Simple hypertension | 40 (74.1) | 14 (25.9) | ||
| Simple HHcy | 301 (81.1) | 70 (18.9) | ||
| H-type hypertension | 366 (71.8) | 144 (28.2) |
| Factor | OR a | 95% CI | p |
|---|---|---|---|
| Age | |||
| <60 | Reference | ||
| ≥60 | 1.576 | 1.125–2.207 | 0.008 |
| Gender | |||
| Female | Reference | ||
| Male | 1.935 | 1.385–2.704 | <0.001 |
| Diabetes | |||
| No | Reference | ||
| Yes | 1.463 | 1.037–2.064 | 0.030 |
| CRP (mg/L) | 1.013 | 1.006–1.019 | <0.001 |
| H-type | |||
| Normal | Reference | ||
| Simple Hypertension | 3.370 | 1.115–10.183 | 0.031 |
| Simple HHCY | 1.843 | 0.710–4.782 | 0.209 |
| H-type Hypertension | 2.990 | 1.176–7.600 | 0.021 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Q.; Qiu, D.-X.; Fu, R.-L.; Xu, T.-F.; Jing, M.-J.; Zhang, H.-S.; Geng, H.-H.; Zheng, L.-C.; Wang, P.-X. H-Type Hypertension and C Reactive Protein in Recurrence of Ischemic Stroke. Int. J. Environ. Res. Public Health 2016, 13, 477. https://doi.org/10.3390/ijerph13050477
Zhang Q, Qiu D-X, Fu R-L, Xu T-F, Jing M-J, Zhang H-S, Geng H-H, Zheng L-C, Wang P-X. H-Type Hypertension and C Reactive Protein in Recurrence of Ischemic Stroke. International Journal of Environmental Research and Public Health. 2016; 13(5):477. https://doi.org/10.3390/ijerph13050477
Chicago/Turabian StyleZhang, Qing, De-Xing Qiu, Rong-Li Fu, Tian-Fen Xu, Meng-Juan Jing, Hui-Shan Zhang, He-Hong Geng, Long-Chao Zheng, and Pei-Xi Wang. 2016. "H-Type Hypertension and C Reactive Protein in Recurrence of Ischemic Stroke" International Journal of Environmental Research and Public Health 13, no. 5: 477. https://doi.org/10.3390/ijerph13050477