
Depth and Well Type Related to Groundwater Microbiological Contamination

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
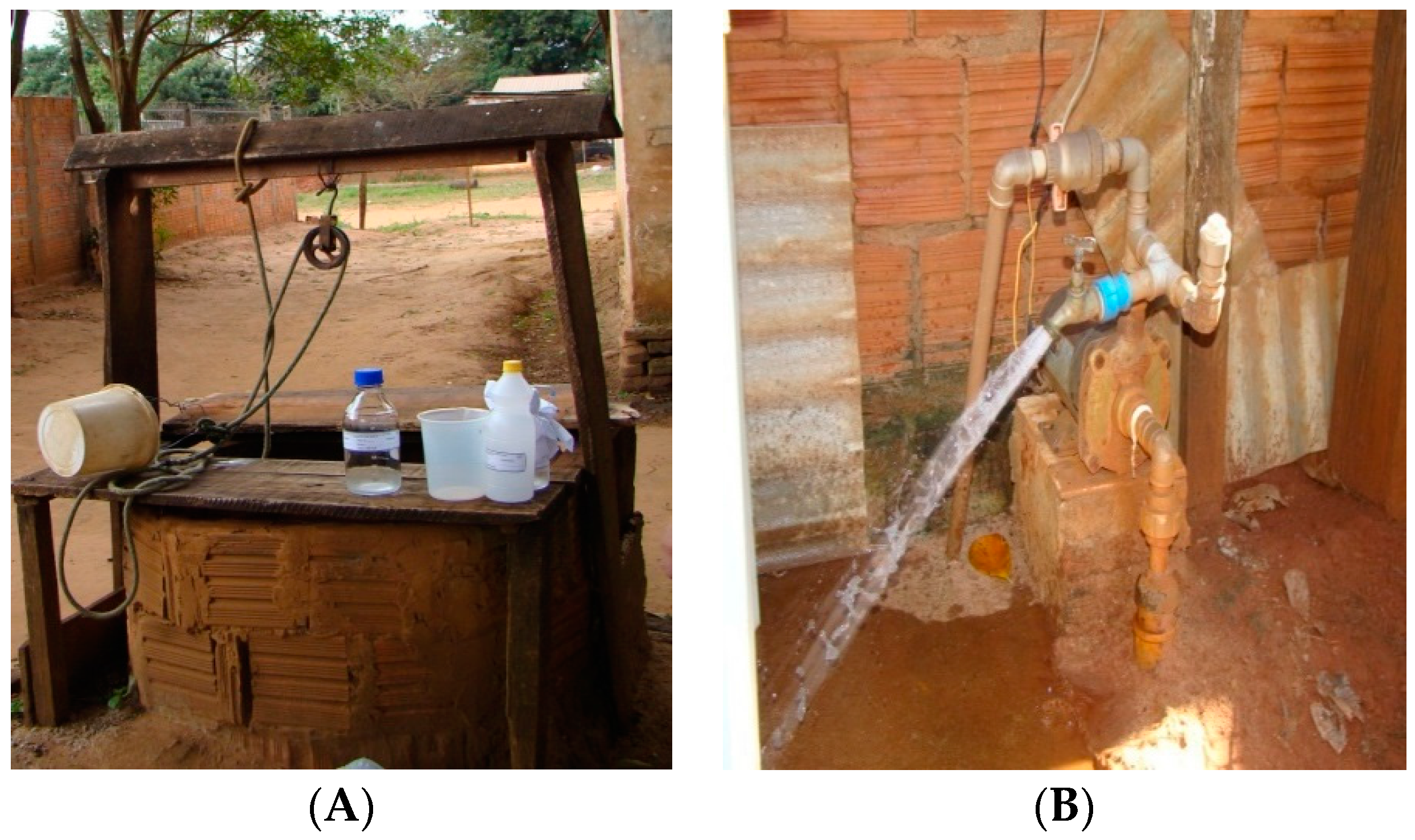
2.1. Study Area and Well Types
2.2. Physico-Chemical Analyses
2.3. Microbiological Analyses
2.4. Identifying Heterotrophic Bacteria and Testing for Antimicrobial Susceptibility
3. Results
3.1. Physico-Chemical Parameters
3.2. Isolated Microorganisms and Antibiotic Resistance
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Freeman, M.C.; Trinies, V.; Boisson, S.; Mak, G.; Clasen, T. Promoting household water treatment through women’s self help groups in rural India: Assessing impact on drinking water quality and equity. PLoS ONE 2012, 7, e44068. [Google Scholar] [CrossRef] [PubMed]
- Risebro, H.L.; Breton, L.; Aird, H.; Hooper, A.; Hunter, P.R. Contaminated small drinking water supplies and risk of infectious intestinal disease: A prospective cohort study. PLoS ONE 2012, 7, e42762. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Preventing Diarrhoea through Better Water, Sanitation and Hygiene: Exposures and Impacts in Low- and Middle-Income Countries; WHO Press: Geneva, Switzerland, 2014. [Google Scholar]
- World Health Organization. Investing in Water and Sanitation: Increasing Access, Reducing Inequalities; GLAAS: Barnsley, UK, 2014. [Google Scholar]
- Breitenmoser, A.; Fretz, R.; Schmid, J.; Besl, A.; Etter, R. Outbreak of acute gastroenteritis due to a washwater-contaminated water supply, Switzerland, 2008. J. Water Health 2011, 9, 569–576. [Google Scholar] [CrossRef] [PubMed]
- Emmanuel, E.; Pierre, M.G.; Perrodin, Y. Groundwater contamination by microbiological and chemical substances released from hospital wastewater: Health risk assessment for drinking water consumers. Environ. Int. 2009, 35, 718–726. [Google Scholar] [CrossRef] [PubMed]
- Wellington, E.M.; Boxall, A.B.; Cross, P.; Feil, E.J.; Gaze, W.H.; Hawkey, P.M.; Jhonson-Rollings, A.S.; Jones, D.L.; Lee, N.M.; Otten, W.; et al. The role of the natural environment in the emergence of antibiotic resistance in gram-negative bacteria. Lancet Infect. Dis. 2013, 13, 155–165. [Google Scholar] [CrossRef]
- Agência Nacional de Águas Brazil (ANA). Atlas Brasil: Abastecimento Urbano De Água; Panorama Nacional/Agência Nacional de Águas; Engecorps/Cobrape: Brasilia, Brazil, 2010.
- Hynds, P.; Misstear, B.D.; Gill, L.W.; Murphy, H.M. Groundwater source contamination mechanisms: Physicochemical profile clustering, risk factor analysis and multivariate modelling. J. Contam. Hydrol. 2014, 159, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Azizullah, A.; Khattak, M.N.K.; Richter, P.; Häder, D.P. Water pollution in Pakistan and its impact on public health—A review. Environ. Int. 2011, 37, 479–497. [Google Scholar] [CrossRef] [PubMed]
- Ministério do Meio Ambiente, Brasil MMA. Águas Subterrâneas um Recurso a Ser Conhecido e Protegido; CRIO: Brasília, Brazil, 2007.
- Jimmy, D.H.; Sundufu, A.J.; Malanoski, A.P.; Jacobsen, K.H.; Ansumana, R.; Leski, T.A.; Bangura, U.; Bockarie, A.S.; Tejan, E.; Lin, B.; et al. Water quality associated public health risk in Bo, Sierra Leone. Environ. Monit. Assess. 2013, 185, 241–251. [Google Scholar] [CrossRef] [PubMed]
- IBGE—Instituto Brasileiro de Geografia e Estatística, Cidades. 2010. Available online: http://www.cidades.ibge.gov.br/xtras/home.php (accessed on 3 May 2015).
- Pereira, J.G.; Comar, V.; Macedo, G.Z. Atlas Dos Recursos Hídricos Superficíais do Territorio da Grande Dourados; Editora da UFGD: Dourados, Brazil, 2012; p. 37. [Google Scholar]
- American Public Health Association (APHA). Standard Methods for the Examination of Water and Wastewater, 21st ed.; American Public Health Association: Washington, DC, USA, 2005. [Google Scholar]
- Mukhopadhyay, C.; Vishwanath, S.; Eshwara, V.K.; Shankaranarayana, S.A.; Sagir, A. Microbial quality of well water from rural and urban households in Karnataka, India: A cross-sectional study. J. Infect. Public Health 2012, 5, 257–262. [Google Scholar] [CrossRef] [PubMed]
- IDEXX Laboratories, Inc. Colilert Test Kit. 2012. Available online: https://www.idexx.com/pubwebresources/pdf/en_us/water/colilert-18-pkg-insert.pdf (accessed on 5 March 2014).
- Silva, N.; Junqueira, V.C.A.; Silveira, N.F.A.; Taniwaki, M.H.; Santos, R.F.S.; Gomes, R.A.R. Manual de métodos de análises microbiológicas de alimentos e água. Ed Varela 2010, 4, 624. [Google Scholar]
- Ishida, K.; Ueda-Yamaguchi, M.; Ueda-Nakamura, T.; Dias Filho, B.P.; Yamada-Ogatta, S.F.; Nakamura, C.V. Performance of methods for identification of yeasts isolated from bottled water: High prevalence of Candida parapsilosis. Semina: Ciências Biológicas e da Saúde 2013, 34, 205–214. [Google Scholar]
- Clinical and Laboratory, Standards Institute. M100-S24 Performance Standards for Antimicrobial Susceptibility Testing, Twenty-fourth Informational Supplement; Clinical Laboratory Standards Institute: Wayne, AB, Canada, 2014. [Google Scholar]
- World Health Organization. Guidelines for Drinking-Water Quality; WHO Press: Geneva, Switzerland, 2011; pp. 1–541. [Google Scholar]
- Ramírez Castillo, F.Y.; Avelar González, F.J.; Garneau, P.; Márquez Díaz, F.; Guerrero Barrera, A.L.; Harel, J. Presence of multi-drug resistant pathogenic Escherichia coli in the San Pedro River located in the State of Águas Calientes, México. Front. Microbiol. 2013, 4, 1–16. [Google Scholar] [CrossRef] [PubMed]
- BRASIL. Ministério da Saúde. Portaria 2.914, de 12 de Dezembro de 2011. Dispõe Sobre os Procedimentos de Controle e Vigilância da Qualidade da Água para o Consumo Humano e Seu Padrão de Potabilidade; Ministério da Saúde: Brasília, Brazil, 2011. Available online: http://bvsms.saude.gov.br/bvs/saudelegis/gm/2011/prt2914_12_12_2011.html (accessed on 5 March 2014).
- World Health Organization. Guías Para la Calidad del Água Potable; WHO Press: Geneva, Switzerland, 2006; Volume 1, pp. 1–98. [Google Scholar]
- Spera, S.T.; Reatto, A.; Correia, J.R.; Silva, J.C.S. Características físicas de um latossolo vermelho-escuro no cerrado de Planaltina, DF, submetido à ação do fogo. Pesqui. Agropec. Bras. 2000, 35, 1817–1824. [Google Scholar] [CrossRef]
- Scorsafava, M.A.; de Souza, A.; Stofer, M.; Nunes, C.A.; Milanez, T.V. Avaliação físico-química da qualidade de água de poços e minas destinada ao consumo humano. Rev. Inst. Adolfo Lutz 2010, 69, 229–232. [Google Scholar]
- Cazotti, C.A.; Francisco, K.M.S.; Gomes Filho, D.L.; Presta, A.A.; Moimaz, S.A.S. Fluorine content in water of shallow wells. Biosci. J. 2012, 28, 494–499. [Google Scholar]
- Ogbu, I.S.I.; Okoro, O.I.O.; Ugwuja, E.I. Well waters fluorine in Enugu, Nigeria. Int. J. Occup. Environ. Med. 2012, 3, 96–98. [Google Scholar] [PubMed]
- Gwala, P.; Andey, S.; Nagarnaik, P.; Ghosh, S.P.; Pal, P.; Deshmukh, P.; Labhasetwar, P. Design and development of sustainable remediation process for mitigation of fluorine contamination in ground water and field application for domestic use. Sci. Total Environ. 2014, 488, 588–594. [Google Scholar] [CrossRef] [PubMed]
- Arnold, M.; Vanderslice, J.A.; Taylor, B.; Benson, S.; Allen, S.; Johnson, M.; Ansong, D. Drinking water quality and source reliability in rural Ashanti region, Ghana. J. Water Health 2013, 11, 161–172. [Google Scholar] [CrossRef] [PubMed]
- Odeleye, F.O.; Idowu, A.O. Bacterial pathogens associated with hand-dug wells in Ibadan City. Afr. J. Microbiol. Res. 2015, 9, 701–707. [Google Scholar] [CrossRef]
- Chowdhury, S. Heterotrophic bacteria in drinking water distribution system: A review. Environ. Monit. Assess. 2012, 184, 6087–6137. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Gardea, M.C.; Tamez-Guerra, P.; Gomez-Flores, R.; Zavala-Díaz de la Serna, F.J.; Eroza-de la Vega, G.; Nevárez-Moorillón, G.V.; Pérez-Recoder, M.C.; Sánchez-Ramírez, B.; del Carmen González-Horta, M.; Infante-Ramírez, R. Multidrug-resistant bacteria isolated from surface water in Bassaseachic Falls National Park, Mexico. Int. J. Environ. Res. Public Health 2016, 13, 597. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.J.; Hu, H.Y.; Lu, S.Q.; Li, Y.; Tang, F.; Lu, Y.; Wei, B. Monitoring and evaluation of antibiotic-resistant bacteria at a municipal wastewater treatment plant in China. Environ. Int. 2012, 42, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Gupta, N.; Hocevar, S.N.; Moulton-Meissner, H.A.; Stevens, K.M.; McIntyre, M.G.; Jensen, B.; Kuhar, D.T.; Noble-Wang, J.A.; Schnatz, R.G.; Becker, S.C.; et al. Outbreak of Serratia marcescens blood stream infections in patients receiving parenteral nutrition prepared by a compounding pharmacy. Clin. Infect. Dis. 2014, 59, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Montagnani, C.; Cocchi, P.; Lega, L.; Campana, S.; Biermann, K.P.; Braggion, C.; Pecile, P.; Chiappini, E.; de Martino, M.; Galli, L. Serratia marcescens outbreak in a neonatal intensive care unit: Crucial role of implementing hand hygiene among external consultants. BMC Infect. Dis. 2015, 15, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.F.; Liu, J.W. Investigation and containment of an outbreak of healthcare-associated infections caused by Serratia marcescens in a liver surgical ward and a surgical intensive-care unit at a medical centre. J. Microbiol. Immunol. Infect. 2015, 48, S85. [Google Scholar] [CrossRef]
- Machado, A.; Bordalo, A.A. Prevalence of antibiotic resistance in bacteria isolated from drinking well water available in Guinea-Bissau (West Africa). Ecotoxicol. Environ. Saf. 2014, 106, 188–194. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Physico-Chemical Parameters | Caarapó | Itaporã | Total n = 66 | Reference Values | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Dug n = 10 | Drilled n = 26 | Dug n = 17 | Drilled n = 13 | |||||||||
| n | % | n | % | n | % | n | % | n | % | |||
| pH | <6.5 | 7 | 70 | 25 | 96 | 16 | 94 | 12 | 92 | 60 | 91 | 6.5–8.5 * |
| 6.5–8.5 | 3 | 30 | 1 | 4 | 1 | 6 | 1 | 8 | 6 | 9 | ||
| Temperature | 15.1–24 °C | 7 | 70 | 6 | 23 | 5 | 29 | 1 | 8 | 19 | 29 | 24.2 °C ** |
| >24 °C | 3 | 30 | 20 | 77 | 12 | 71 | 12 | 92 | 47 | 71 | ||
| Turbidity | ≤5.0 NTU | 10 | 100 | 26 | 100 | 16 | 94 | 12 | 92 | 64 | 97 | ≤5.0 NTU * |
| >5.0 NTU | 0 | 0 | 0 | 0 | 1 | 6 | 1 | 8 | 2 | 3 | ||
| Chlorine | <0.1 mg/L | 8 | 80 | 24 | 92 | 16 | 94 | 12 | 92 | 60 | 91 | ≤5.0 mg/L * |
| 0.1–1.25 mg/L | 2 | 20 | 2 | 8 | 1 | 6 | 1 | 8 | 6 | 9 | ||
| Fluorine | <0.1 mg/L | 7 | 70 | 17 | 65 | 16 | 94 | 9 | 69 | 49 | 74 | ≤1.5 mg/L * |
| 0.1–0.65 mg/L | 3 | 30 | 9 | 35 | 1 | 6 | 4 | 31 | 17 | 26 | ||
| Microorganisms | Caarapó | Itaporã | Totals * | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Dug n = 10 | Drilled n = 26 | Total n = 36 | Dug n = 17 | Drilled n = 13 | Total n = 30 | |||||||||
| n | % | n | % | n | % | n | % | n | % | n | % | n | % | |
| Total Coliforms | 10 | 100 | 7 | 27 | 17 | 47.2 | 16 | 94 | 7 | 54 | 23 | 76.6 | 40 | 67 |
| E. coli | 6 | 60 | 1 | 4 | 7 | 19.4 | 12 | 71 | 3 | 23 | 15 | 50 | 22 | 33 |
| Depth | Total Number of Wells | Total Col. * | E. coli * | Heterotrophic ** | Yeast * | ||||
|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | ||
| ≤5 m | 10 | 9 | 90 | 6 | 60 | 2 | 20 | 7 | 70 |
| >5–10 m | 19 | 15 | 79 | 9 | 48 | 2 | 11 | 10 | 53 |
| >10–15 m | 16 | 10 | 63 | 6 | 38 | 1 | 6 | 8 | 50 |
| >15 m | 21 | 6 | 28 | 1 | 5 | - | 5 | 24 | |
| Total | 66 | 40 | 60 | 22 | 33 | 5 | 8 | 30 | 45 |
| Microorganism | N | β-Lactams | LI | MA | QU & FL | AM | OX | AN | SU & PR | GP | |||||||
| Gram positive | P | OXI | CM | E | CIP | NOR | MXF | GM | LNZ | RA | SXT | TEC | VA | ||||
| Staphylococcus epidermidis | 1 | S | S | S | S | S | S | S | S | S | S | R | S | S | |||
| Staphylococcus hominis ssp. | 2 | R | S | S | R | S | S | S | S | S | S | R | S | S | |||
| Staphylococcus saprophyticus | 1 | R | R | S | S | S | S | S | S | S | S | R | S | S | |||
| Staphylococcus warneri | 2 | R | S | S | R | S | S | S | S | S | I | R | I | S | |||
| Gram negative | N | β-lactams | FU | QU & FL | AM | GC | |||||||||||
| ETP | AM | SAM | FEP | FOX | CAZ | CRO | CXM | IPM | MEM | TZP | CS | CIP | AN | GM | TGC | ||
| Acinetobacter haemolyticus | 4 | - | R | R | S | R | I | R | R | S | S | R | S | R | S | S | - |
| Acinetobacter lwoffii | 1 | - | R | S | S | R | I | R | R | S | S | S | S | S | S | S | - |
| Aeromonas hydrophila | 2 | - | - | - | S | - | S | S | - | S | S | S | S | S | S | S | - |
| Chromobacterium violaceum | 1 | - | - | - | S | - | S | R | - | I | - | R | R | S | S | S | - |
| Citrobacter freundii | 2 | S | R | S | S | R | S | S | R | S | S | S | - | S | S | S | - |
| Citrobacter sedlakii | 1 | S | R | S | S | R | S | S | R | S | S | S | - | S | S | S | - |
| Enterobacter asburiae | 2 | S | R | S | S | R | S | S | R | S | S | S | - | S | S | S | - |
| Enterobacter cloacae complex | 2 | S | R | R | S | R | S | S | R | S | S | S | - | S | S | I | - |
| Enterobacter gergoviae | 1 | S | R | S | S | S | S | S | R | S | S | S | - | S | S | S | - |
| Klebsiella oxytoca | 1 | S | R | S | S | S | S | S | S | S | S | S | - | S | S | S | - |
| Klebsiella pneumoniae spp. | 1 | S | R | S | S | S | S | S | S | S | S | S | - | S | S | S | - |
| Kluyvera intermédia | 1 | S | S | S | S | S | S | S | S | S | S | R | - | R | S | S | - |
| Ochrobactrum anthropi | 1 | - | - | - | S | - | R | R | - | S | S | R | S | R | S | I | - |
| Pantoea spp. | 1 | - | - | - | S | - | S | S | - | S | S | - | - | S | S | S | - |
| Pseudomonas aeroginosas | 5 | - | R | R | S | R | S | R | R | S | I | S | S | S | S | S | R |
| Pseudomonas putida | 1 | - | - | - | S | - | S | I | - | S | S | I | S | S | S | S | - |
| Ralstonia mannitolilytica | 1 | - | - | - | S | - | S | S | - | R | I | R | R | S | S | R | - |
| Serratia marcescens | 10 | S | R | R | S | R | S | S | R | I | S | S | R | S | S | S | - |
| Sphingomonas paucimobilis | 1 | - | - | - | I | - | R | I | - | S | S | S | R | R | S | S | - |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maran, N.H.; Crispim, B.D.A.; Iahnn, S.R.; Araújo, R.P.d.; Grisolia, A.B.; Oliveira, K.M.P.d. Depth and Well Type Related to Groundwater Microbiological Contamination. Int. J. Environ. Res. Public Health 2016, 13, 1036. https://doi.org/10.3390/ijerph13101036
Maran NH, Crispim BDA, Iahnn SR, Araújo RPd, Grisolia AB, Oliveira KMPd. Depth and Well Type Related to Groundwater Microbiological Contamination. International Journal of Environmental Research and Public Health. 2016; 13(10):1036. https://doi.org/10.3390/ijerph13101036
Chicago/Turabian StyleMaran, Nayara Halimy, Bruno Do Amaral Crispim, Stephanie Ramirez Iahnn, Renata Pires de Araújo, Alexeia Barufatti Grisolia, and Kelly Mari Pires de Oliveira. 2016. "Depth and Well Type Related to Groundwater Microbiological Contamination" International Journal of Environmental Research and Public Health 13, no. 10: 1036. https://doi.org/10.3390/ijerph13101036