
Older Male Physicians Have Lower Risk of Trochanteric but Not Cervical Hip Fractures


Abstract
:1. Introduction
2. Methods
2.1. Database
2.2. Ethics Statement
2.3. Study Cohort
2.4. Outcomes
2.5. Confounders
2.6. Statistics
3. Results
3.1. Baseline Characteristics
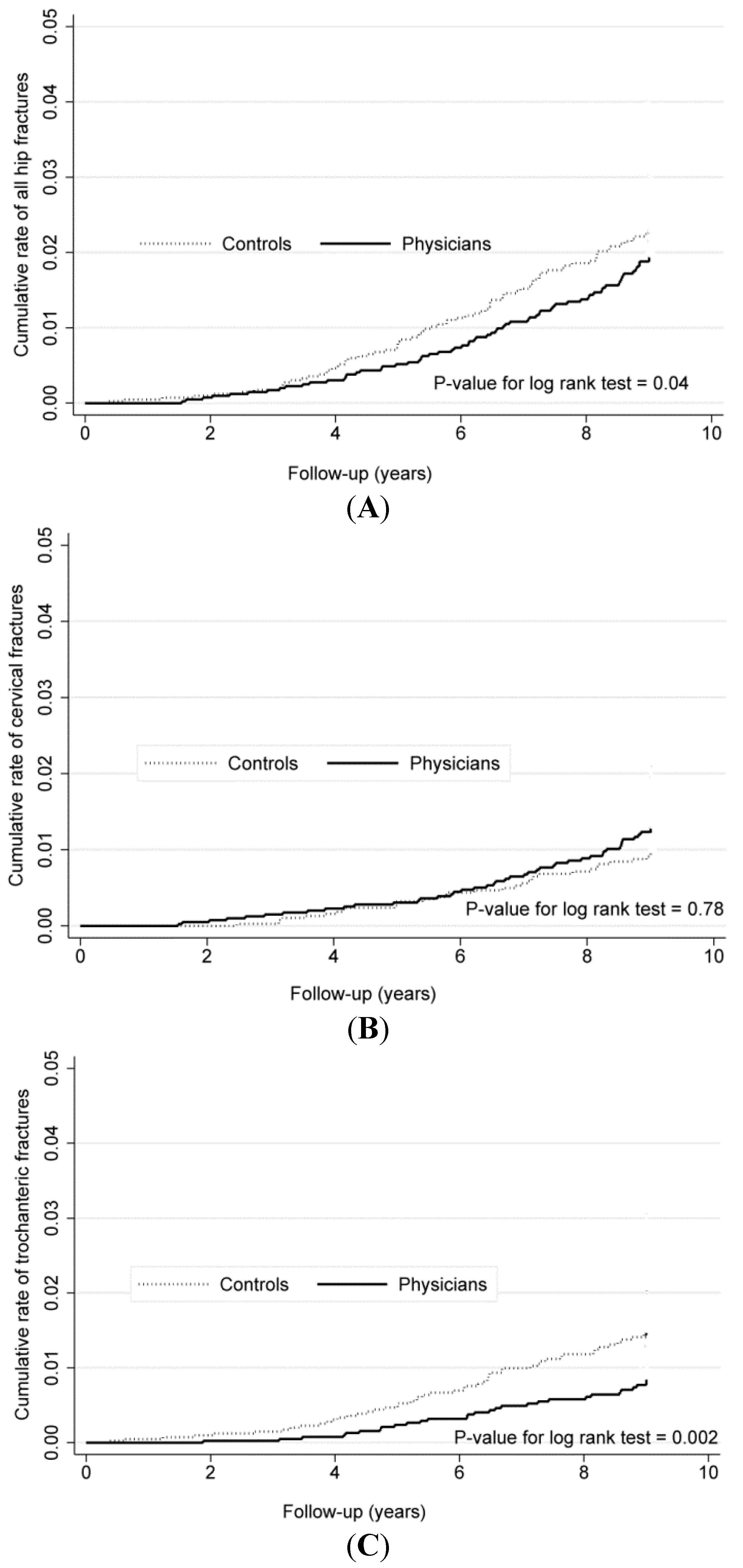
3.2. Incidence Rates and Risks of Hip Fractures

{kind=link}
{kind=link}
| Variables | Physicians (n = 4303) | Controls (n = 4303) | p Values |
|---|---|---|---|
| Mean age ± SD | 74.1 ± 5.6 | 74.1 ± 5.6 | matched |
| Male, % | 97.9 | 97.9 | matched |
| Income level, % | -- | -- | matched |
| Zero | 13.6 | 13.6 | |
| Low | 56.5 | 56.5 | |
| Middle | 5.2 | 5.2 | |
| High | 24.8 | 24.8 | |
| Urbanization, % | -- | -- | matched |
| Urban | 70.5 | 70.5 | |
| Suburban | 22.7 | 22.7 | |
| Rural | 6.8 | 6.8 | |
| Charlson’s score (mean ± SD) | 0.56 ± 0.97 | 0.63 ± 1.02 | 0.002 |
| 0 | 65.8 | 62.8 | |
| 1 | 20.2 | 20.7 | |
| 2 | 9.0 | 10.1 | |
| ≥3 | 5.1 | 6.3 |
| Hip Fracture | Physicians | Controls | ||
| N | IR (95% CI) | N | IR (95% CI) | |
| All | 140 | 4.18 (3.54–4.93) | 169 | 5.19 (4.44–6.01) |
| Cervical | 82 | 2.45 (1.96–3.03) | 69 | 2.12 (1.66–2.66) |
| Trochanteric | 58 | 1.73 (1.33–2.23) | 100 | 3.07 (2.51–3.71) |
| Hip Fracture | Cox Model | Competing Risk Model | ||
| Crude HR (95% CI) | Adjusted HR (95% CI) a | Crude SHR (95% CI) | Adjusted SHR (95% CI) a | |
| All | 0.77 (0.59–0.99) | 0.78 (0.60–1.02) | 0.83 (0.66–1.03) | 0.83 (0.67–1.04) |
| Cervical | 1.07 (0.74–1.55) | 1.14 (0.78–1.67) | 1.19 (0.86–1.64) | 1.20 (0.88–1.66) |
| Trochanteric | 0.55 (0.38–0.79) | 0.54 (0.37–0.79) | 0.58 (0.42–0.80) | 0.58 (0.42–0.82) |

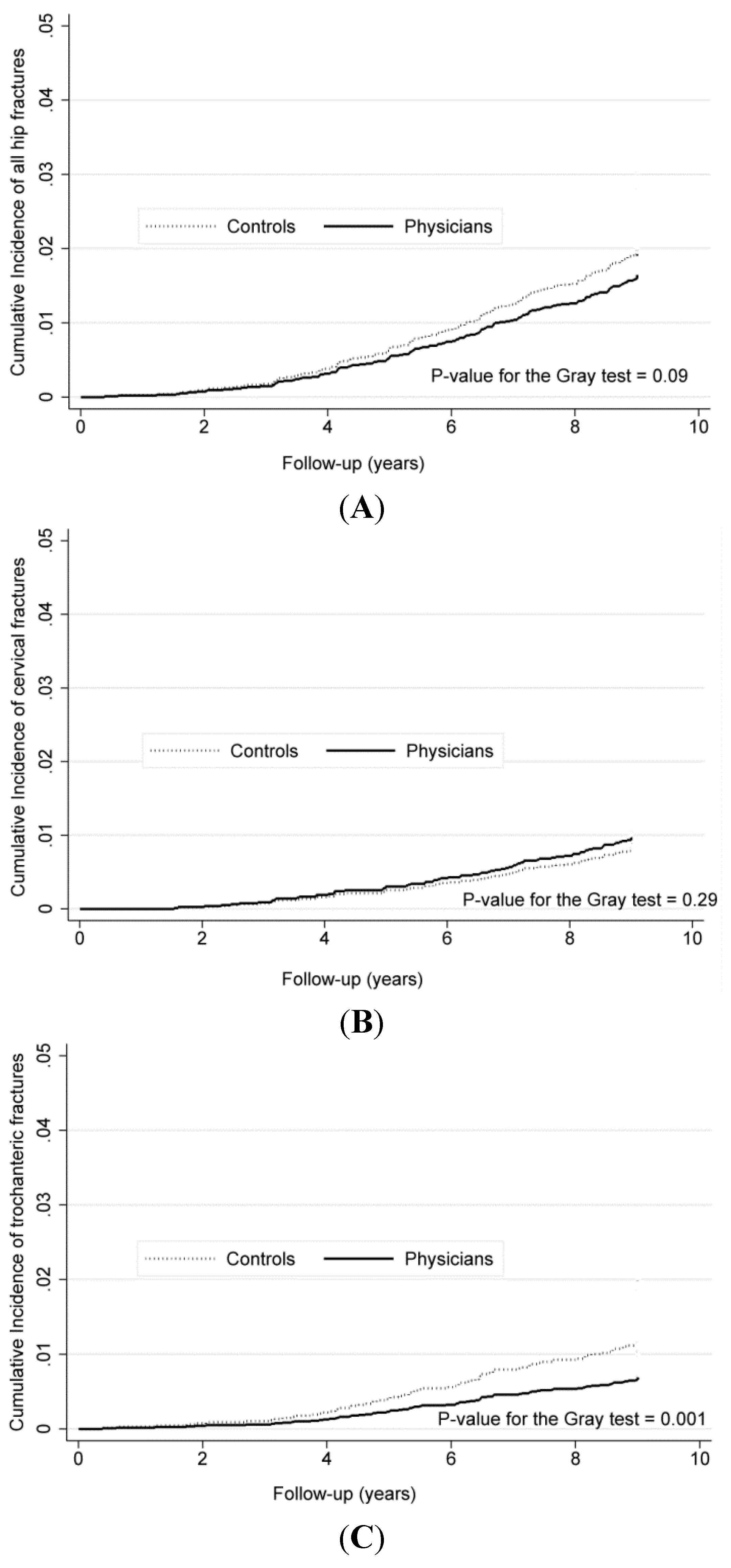
3.3. Competing Risk Analysis

4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Burckhardt, P. Are hip fractures preventable with nutritional measures and exercise in the elderly? Osteoporos. Int. 1996, 6, 56–59. [Google Scholar] [CrossRef] [PubMed]
- Segal, E.; Raichlin, V.; Rimbrot, S.; Zinman, C.; Raz, B.; Ish-Shalom, S. Hip fractures in the elderly in Israel-possible impact of preventable conditions. Arch. Gerontol. Geriatr. 2009, 48, 182–185. [Google Scholar] [CrossRef] [PubMed]
- Bawab, W.; Saad, M.; Hajjar, N.; Rachidi, S.; Al Hajje, A.; Awada, S.; Salameh, P. Evaluation of hip fracture risk factors in older adults in the lebanese population. J. Res. Health Sci. 2014, 14, 193–197. [Google Scholar] [PubMed]
- Bazargan, M.; Makar, M.; Bazargan-Hejazi, S.; Ani, C.; Wolf, K.E. Preventive, lifestyle, andpersonal health behaviors among physicians. Acad. Psychiatr. 2009, 33, 289–295. [Google Scholar] [CrossRef]
- Frank, E.; Segura, C. Health practices of Canadian physicians. Can. Fam. Phys. 2009, 55, 810–811. [Google Scholar]
- Peklar, J.; Henman, M.C.; Kos, M.; Richardson, K.; Kenny, R.A. Concurrent use of drugs and supplements in a community-dwelling population aged 50 years or more: Potential benefits and risks. Drugs Aging 2014, 31, 527–540. [Google Scholar] [CrossRef] [PubMed]
- Riggs, B.L.; Wahner, H.W.; Seeman, E.; Offord, K.P.; Dunn, W.L.; Mazess, R.B.; Johnson, K.A.; Melton, L.J., 3rd. Changes in bone mineral density of the proximal femur and spine with aging. Differences between the postmenopausal and senile osteoporosis syndromes. J. Clin. Investig. 1982, 70, 716–723. [Google Scholar] [CrossRef] [PubMed]
- Vega, E.; Mautalen, C.; Gomez, H.; Garrido, A.; Melo, L.; Sahores, A.O. Bone mineral density in patients with cervical and trochanteric fractures of the proximal femur. Osteoporos. Int. 1991, 1, 81–86. [Google Scholar] [CrossRef] [PubMed]
- Mautalen, C.A.; Vega, E.M.; Einhorn, T.A. Are the etiologies of cervical and trochanteric hipfractures different? Bone 1996, 18, 133–137. [Google Scholar] [CrossRef] [PubMed]
- Holzer, G.; von Skrbensky, G.; Holzer, L.A.; Pichl, W. Hip fractures and the contribution of cortical vs. trabecular bone to femoral neck strength. J. Bone Miner. Res. 2009, 24, 468–474. [Google Scholar] [CrossRef] [PubMed]
- Pulkkinen, P.; Gluer, C.C.; Jamsa, T. Investigation of differences between hip fracture types: A worthy strategy for improved risk assessment and fracture prevention. Bone 2011, 49, 600–604. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Meehan, J.P.; Blumenfeld, T.; Szabo, R.M. Hip fractures in the United States: 2008 nationwide emergency department sample. Arthritis Care Res. 2012, 64, 751–757. [Google Scholar] [CrossRef]
- Shanafelt, T.D.; Boone, S.; Tan, L.; Dyrbye, L.N.; Sotile, W.; Satele, D.; West, C.P.; Sloan, J.; Oreskovich, M.R. Burnout and satisfaction with work-life balance among US physicians relative to the general US population. Arch. Intern. Med. 2012, 172, 1377–1385. [Google Scholar] [CrossRef] [PubMed]
- Multani, S.K.; Sarathi, V.; Shivane, V.; Bandgar, T.R.; Menon, P.S.; Shah, N.S. Study of bone mineral density in resident doctors working at a teaching hospital. J. Postgrad. Med. 2010, 56, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.C.; Liu, C.C.; Hwang, S.L.; Li, C.Y.; Chou, L.P.; Liu, C.C. Are diabetic physicians at a lower riskof hospitalization for coronary heart disease? A nationwide cohort study in Taiwan. Asia Pac. J. Public Health 2012, 2012. [Google Scholar] [CrossRef]
- Silverman, M.N.; Sternberg, E.M. Glucocorticoid regulation of inflammation and its functional correlates: From HPA axis to glucocorticoid receptor dysfunction. Ann. N.Y. Acad. Sci. 2012, 1261, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Oberg, E.B.; Frank, E. Physiciansʼ health practices strongly influence patient health practices. J. R. Coll. Phys. Edinb. 2009, 39, 290–291. [Google Scholar] [CrossRef]
- Chen, Y.Y.; Cheng, P.Y.; Wu, S.L.; Lai, C.H. Parkinsonʼs disease and risk of hip fracture: An 8-year follow-up study in Taiwan. Parkinsonism Relat. Disord. 2012, 18, 506–509. [Google Scholar] [CrossRef] [PubMed]
- Lin, T.C.; Yang, C.Y.; Yang, Y.H.; Lin, S.J. Alendronate adherence and its impact onhip-fracture risk in patients with established osteoporosis in Taiwan. Clin. Pharmacol. Ther. 2011, 90, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.C.; Lin, C.S.; Shih, C.C.; Yeh, C.C.; Chang, Y.C.; Lee, Y.W.; Chen, T.L. Increased risk of fracture and postfracture adverse events in patients with diabetes: Two nationwide population-based retrospective cohort studies. Diabet. Care 2014, 37, 2246–2252. [Google Scholar] [CrossRef]
- Chie, W.C.; Yang, R.S.; Liu, J.P.; Tsai, K.S. High incidence rate of hip fracture in Taiwan: Estimated from a nationwide health insurance database. Osteoporos. Int. 2004, 15, 998–1002. [Google Scholar] [CrossRef] [PubMed]
- Shao, C.J.; Hsieh, Y.H.; Tsai, C.H.; Lai, K.A. A nationwide seven-year trend of hip fractures in the elderly population of Taiwan. Bone 2009, 44, 125–129. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.M.; Wu, E.C.; Chang, I.S.; Lin, K.M. Benzodiazepine and risk of hip fractures in older people: A nested case-control study in Taiwan. Am. J. Geriatr. Psychiat. 2008, 16, 686–692. [Google Scholar] [CrossRef]
- Deng, C.Y.; Huang, N.; Chou, Y.J.; Hsu, Y.J.; Chen, L.S.; Chou, P. Comparison of perforation risk among physicians, other medical professionals and general adults with acute appendicitisin Taiwan. Br. J. Surg. 2006, 93, 1297–1302. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.M.; Yang, C.H.; Sung, F.C.; Li, C.Y. Risks and causes of hospitalizations among physicians in Taiwan. Health Serv. Res. 2008, 43, 675–692. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.H.; Li, T.H.; Lin, Y.L.; Shiao, Y.J.; Wu, S.C.; Li, C.Y.; Sung, F.C.; Yang, C.Y.; Wu, T.N. Lower morbidity and disease risk among the Chinese medicine physicians in Taiwan. Tohoku J. Exp. Med. 2009, 219, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Lu, H.M.; Shih, S.F.; Kuo, K.N.; Chen, C.L.; Huang, L.C. Poverty related risk for potentially preventable hospitalisations among children in Taiwan. BMC Health Serv. Res. 2010, 10. [Google Scholar] [CrossRef] [PubMed]
- Karagas, M.R.; Lu-Yao, G.L.; Arett, J.A.; Beach, M.L.; Baron, J.A. Heterogeneity of hip fracture: Age, race, sex, and geographic patterns of femoral neck and trochanteric fractures among the US elderly. Am. J. Epidemiol. 1996, 143, 677–682. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Schneeweiss, S.; Liu, J.; Daniel, G.W.; Chang, C.L.; Garneau, K.; Solomon, D.H. Risk of osteoporotic fracture in a large population-based cohort of patients with rheumatoid arthritis. Arthritis Res. Ther. 2010, 12. [Google Scholar] [CrossRef] [PubMed]
- Dennison, E.M.; Compston, J.E.; Flahive, J.; Siris, E.S.; Gehlbach, S.H.; Adachi, J.D.; Boonen, S.; Chapurlat, R.; Díez-Pérez, A.; Anderson, F.A.; et al. GLOW Investigators effect of co-morbidities on fracture risk: Findings from the Global Longitudinal Study of Osteoporosis in Women (GLOW). Bone 2012, 50, 1288–1293. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifyingprognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef] [PubMed]
- Deyo, R.A.; Cherkin, D.C.; Ciol, M.A. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J. Clin. Epidemiol. 1992, 45, 613–619. [Google Scholar] [CrossRef] [PubMed]
- Brennan, S.L.; Pasco, J.A.; Urquhart, D.M.; Oldenburg, B.; Hanna, F.; Wluka, A.E. The associationbetween socioeconomic status and osteoporotic fracture in population-based adults: Asystematic review. Osteoporos. Int. 2009, 20, 1487–1497. [Google Scholar] [CrossRef] [PubMed]
- Leslie, W.D.; Lix, L.M.; Wu, X. Competing mortality and fracture risk assessment. Osteoporos. Int. 2013, 24, 681–688. [Google Scholar] [CrossRef] [PubMed]
- Fine, J.P.; Gray, R.J. A proportional hazards model for the subdistribution of competing risk. J. Am. Stat. Assoc. 1999, 94, 496–509. [Google Scholar] [CrossRef]
- Berry, S.D.; Ngo, L.; Samelson, E.J.; Kiel, D.P. Competing risk of death: An important consideration in studies of older adults. J. Am. Geriatr. Soc. 2010, 58, 783–787. [Google Scholar] [CrossRef] [PubMed]
- Singh-Manoux, A.; Gourmelen, J.; Ferrie, J.; Silventoinen, K.; Guéguen, A.; Stringhini, S.; Nabi, H.; Kivimaki, M. Trends in the association between height and socioeconomic indicators in France, 1970–2003. Econ. Hum. Biol. 2010, 8, 396–404. [Google Scholar] [CrossRef] [PubMed]
- Schneeweiss, S.; Wang, P.S. Association between SSRI use and hip fractures and the effect of residual confounding bias in claims database studies. J. Clin. Psychopharmacol. 2004, 24, 632–638. [Google Scholar] [CrossRef] [PubMed]
- Schneeweiss, S.; Wang, P.S. Claims data studies of sedative-hypnotics and hip fractures in older people: Exploring residual confounding using survey information. J. Am. Geriatr. Soc. 2005, 53, 948–954. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shen, H.-N.; Lin, W.-T.; Lu, C.-L.; Li, C.-Y. Older Male Physicians Have Lower Risk of Trochanteric but Not Cervical Hip Fractures. Int. J. Environ. Res. Public Health 2015, 12, 2249-2261. https://doi.org/10.3390/ijerph120202249
Shen H-N, Lin W-T, Lu C-L, Li C-Y. Older Male Physicians Have Lower Risk of Trochanteric but Not Cervical Hip Fractures. International Journal of Environmental Research and Public Health. 2015; 12(2):2249-2261. https://doi.org/10.3390/ijerph120202249
Chicago/Turabian StyleShen, Hsiu-Nien, Wei-Ting Lin, Chin-Li Lu, and Chung-Yi Li. 2015. "Older Male Physicians Have Lower Risk of Trochanteric but Not Cervical Hip Fractures" International Journal of Environmental Research and Public Health 12, no. 2: 2249-2261. https://doi.org/10.3390/ijerph120202249