1. Introduction
The New Health Care Reform Plan issued by the Chinese government in 2009 re-emphasized the central role of Community Health Centers (CHCs) in providing cost-effective and convenient primary care to the public, which aimed to improve equitable access to basic healthcare for its residents by building a strong, primary care-based delivery system [
1]. To achieve the above goals, there is an urgent need to promote the work status and health status of community healthcare workers [
2]. As the population ages and lifestyle changes, CHCs play a much more significant role in the healthcare system, and CHC healthcare workers, as the main pillar of primary care providers, should take on more workload than before.
The current tense physician-patient relationship particularly caused by workplace violence is widely recognized to be an exigent social problem that might impact the health status and the work status of healthcare workers in CHCs. The issue of workplace violence used to be a hot research topic of public health [
3,
4,
5]. Workplace violence is the intentional use of physical force or power, such as physical assaults and threats of assaults, directly towards people at work or on duty [
6]. Workplace violence, as an occupational hazard in the healthcare setting, can lead to a variety of adverse consequences for the victims, including anger, anxiety, depression, fear, sleep disruption, job strain, job dissatisfaction and job turnover of health workers [
7,
8,
9,
10]. It is demonstrated that the incidence of workplace violence against medical workers in general hospitals is only about 9.5% in the U.K., but this study only reports physical violence [
11]. The situation is more serious in the USA and Turkey: 78% [
12] and 87% [
13], respectively. Similarly, the incidence rate is about 71% in China [
14]. Besides, some studies had proven that workplace violence influences employee’s work status, like job performance [
15,
16]. Schermerhorm has defined job performance as the quality and quantity of tasks of an individual or a group, which also has been called staff productivity [
17]. In a previous study, Schat’s research confirmed that U.S. workers’ job performance was damaged by workplace violence [
15]. However, few studies have been conducted to investigate the situation in primary care facilities. Additionally, studies examining the association between workplace violence and job performance in primary care settings are rare.
In addition, quality of life (QOL) has been introduced to estimate people’s health status, which is defined as an individual’s satisfaction or happiness with the eight dimensions of life [
18]. Teles’s study demonstrated that QOL was decreased by workplace violence [
19]. Not only does QOL relate to an individual’s own mental and physical health, but it significantly influences the quality and safety of the health services that they provide [
20]. Studies have identified the relationship between workplace violence and QOL [
20,
21], as well as the association between QOL and job performance [
22]. However, few studies have performed research on the triadic connections in CHC healthcare workers in China. There might especially be a spatial relationship between those.
Therefore, this study tries to investigate the current status of workplace violence in primary care settings in China and probes into the relationship of these three variables. Last, we attempt to analyze the mechanism of how workplace violence affects job performance. One hypothesis is that there might a spatial relationship between workplace violence and job performance, which might be mediated by QOL.
3. Results
Of the 1404 respondents, about three quarters were female (73.29%). Approximately one half was aged 30~40 years old. About 76.21% of the respondents described themselves as married (
Table 1). More than half of the respondents had an education level of college or above. About 40% of the respondents were GPs, whilst another 40% were nurses. Most of them were fixed-term workers in CHCs. Almost 70% of the respondents had a monthly income between RMB 2000 and 6000, which was equivalent to the area’s median income.
In the past 12 months, more than half of the respondents (51.64%) experienced workplace violence (
Table 1). The incidence of PA was 9.69%; EA was 46.23%; T was 23.08%; VSH was 10.54%; and SA was 4.34%. The chi square test showed that the incidence of workplace violence had no significant difference among the respondents with different socio-demographic characteristics, including gender and marital status. However, significant differences did exist in age (
p = 0.005), education level (
p = 0.001), occupation (
p = 0.003) and monthly income (
p = 0.002).
There were significant differences in the job performance between the respondents who experienced workplace violence and those who did not (
p < 0.001) (
Table 2). Significant differences were also identified in the three dimensions used to measure job performance, including JD, TP and IF. As for QOL, the respondents who did not experience workplace violence had a higher QOL score when compared to those who had experienced it. Similar findings were observed for the eight dimensions under QOL, as well.
A correlation matrix for the study variables is presented in
Table 3. It was shown that workplace violence was negatively related to job performance (
r = −0.205,
p < 0.001), whilst there was a significantly negative correlation between workplace violence and QOL (
r = −0.313,
p < 0.001). However, a positive correlation was identified between job performance and QOL (
r = 0.365,
p < 0.001).
Regression analysis among variables is presented in
Table 4. The effect of workplace violence on job performance, including its three dimensions, was examined. Results showed that workplace violence had a relatively negative predictive effect on job performance (
β = −0.205,
p < 0.001), job dedication (
β = −0.197,
p < 0.001), task performance (
β = −0.166,
p < 0.001) and interpersonal facilitation (
β = −0.181,
p < 0.001) of healthcare workers in CHCs. The effect of workplace violence on the quality of life was explored, and a relatively negative predictive effect was reported (
β = −0.313,
p < 0.001). The effect of workplace violence and quality of life on job performance was also tested, and the standardized regression coefficients were
β = −0.100 and
β = 0.333, respectively (all
p < 0.001).
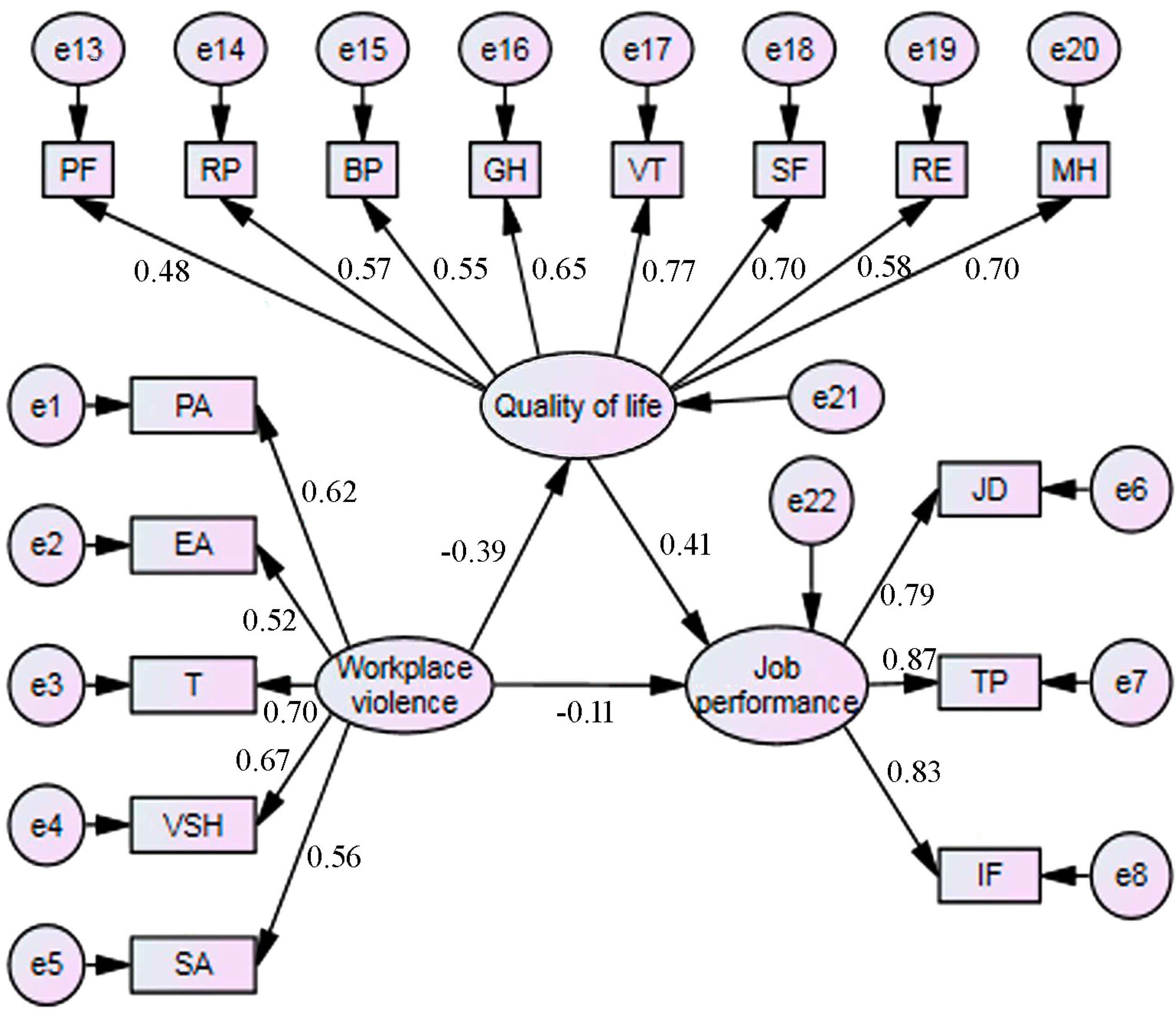
Path analysis on the original model was performed, which is shown in
Figure 1. According to the modification index values, the correlation between EA and T (
r = 0.548,
p < 0.001), PA and VSH (
r = 0.419,
p < 0.001), PF and RP (
r = 0.429,
p < 0.001), RP and RE (
r = 0.546,
p < 0.001), BP and GH (
r = 0.450,
p < 0.001) and VT and MH (
r = 0.657,
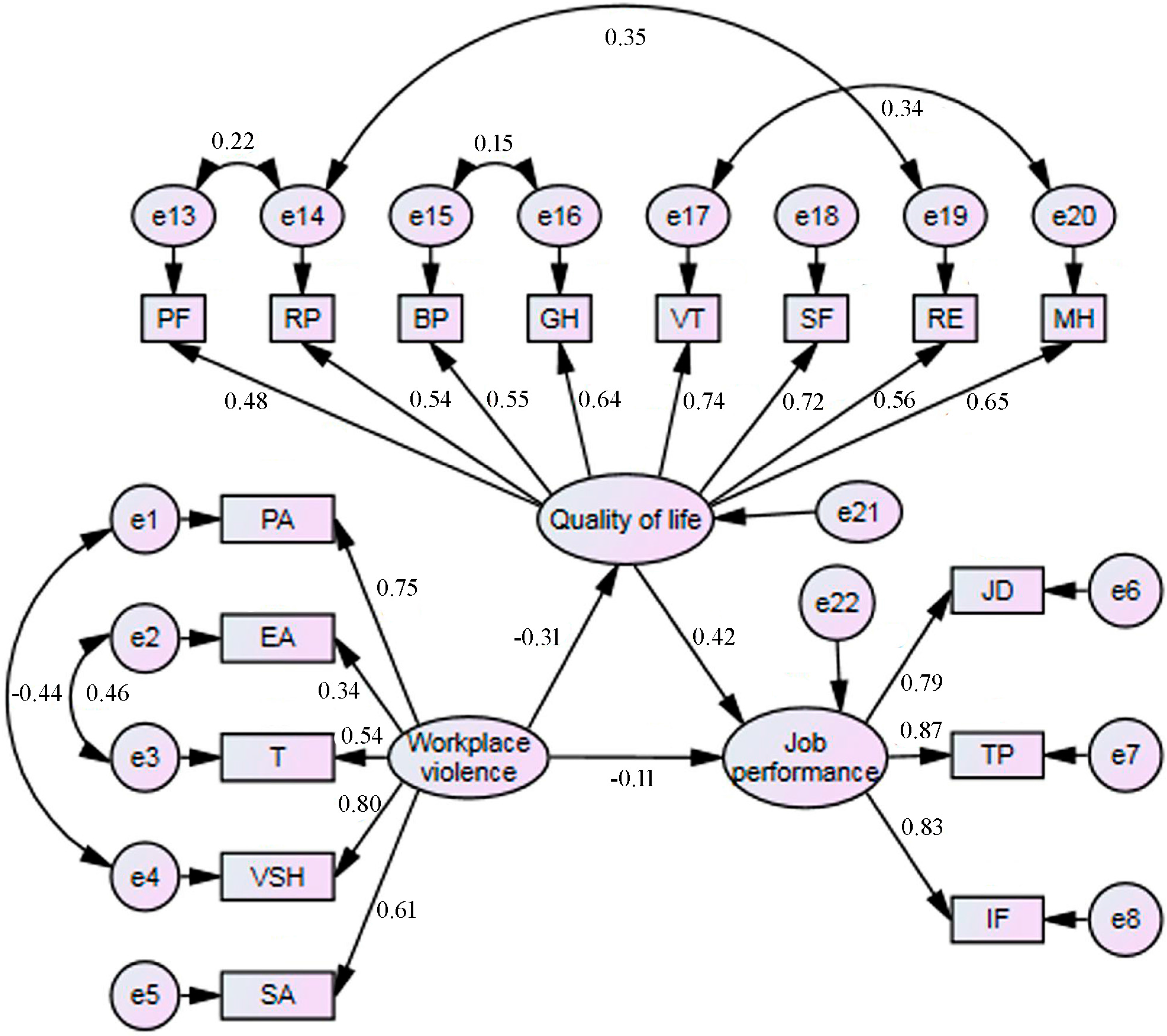
p < 0.001), the modified model (final model) was constructed and is shown in
Figure 2.
Table 5 provides path coefficients between various structural variables. Fit indices of the final model are presented in
Table 6, which revealed a good fit of the data.
As can be seen from
Figure 2 and
Table 5, workplace violence had a negative effect on job performance, which was mediated by QOL. The total effect (
β = −0.243) of workplace violence on job performance was comprised of not only its direct effect (
β = −0.113), but also the indirect effect (
β = −0.130) generated by QOL.
Figure 1.
The original model. (β: standardized path coefficient. The direct effect: β = −0.105, workplace violence → job performance. The indirect effect: β = −0.160, workplace violence → quality of life → job performance. The total effect: β = −0.26, workplace violence on job performance, consisted of a direct effect (β = −0.105) and an indirect effect (β = −0.160), which was mediated by quality of life. PA: physical assault; EA: emotional abuse; T threat; VSH: verbal sexual harassment; SA: sexual assault. JD: job dedication; TP: task performance; IF: interpersonal facilitation. PF: physical functioning; RP: role limitations due to physical problems; BP: bodily pain; GH: general health; VT: vitality; SF: social functioning; RE: role limitations due to emotional problems; MH: mental health.)
Figure 1.
The original model. (β: standardized path coefficient. The direct effect: β = −0.105, workplace violence → job performance. The indirect effect: β = −0.160, workplace violence → quality of life → job performance. The total effect: β = −0.26, workplace violence on job performance, consisted of a direct effect (β = −0.105) and an indirect effect (β = −0.160), which was mediated by quality of life. PA: physical assault; EA: emotional abuse; T threat; VSH: verbal sexual harassment; SA: sexual assault. JD: job dedication; TP: task performance; IF: interpersonal facilitation. PF: physical functioning; RP: role limitations due to physical problems; BP: bodily pain; GH: general health; VT: vitality; SF: social functioning; RE: role limitations due to emotional problems; MH: mental health.)
Figure 2.
The final model. (β: standardized path coefficient. The direct effect: β = −0.113, workplace violence → job performance. The indirect effect: β = −0.130, workplace violence → quality of life → job performance. The total effect: β = −0.243, workplace violence on job performance, consisted of a direct effect (β = −0.113) and an indirect effect (β = −0.130), which was mediated by quality of life. PA: physical assault; EA: emotional abuse; T threat; VSH: verbal sexual harassment; SA: sexual assault. JD: job dedication; TP: task performance; IF: interpersonal facilitation. PF: physical functioning; RP: role limitations due to physical problems; BP: bodily pain; GH: general health; VT: vitality; SF: social functioning; RE: role limitations due to emotional problems; MH: mental health.)
Figure 2.
The final model. (β: standardized path coefficient. The direct effect: β = −0.113, workplace violence → job performance. The indirect effect: β = −0.130, workplace violence → quality of life → job performance. The total effect: β = −0.243, workplace violence on job performance, consisted of a direct effect (β = −0.113) and an indirect effect (β = −0.130), which was mediated by quality of life. PA: physical assault; EA: emotional abuse; T threat; VSH: verbal sexual harassment; SA: sexual assault. JD: job dedication; TP: task performance; IF: interpersonal facilitation. PF: physical functioning; RP: role limitations due to physical problems; BP: bodily pain; GH: general health; VT: vitality; SF: social functioning; RE: role limitations due to emotional problems; MH: mental health.)
Table 1.
Basic demographic characteristics of the whole sample and subgroups according to exposure to workplace violence.
Table 1.
Basic demographic characteristics of the whole sample and subgroups according to exposure to workplace violence.
| | Entire Sample (n = 1404) | Workplace Violence Cases (n = 725) a | Statistics |
|---|
| | n | % | n | % | χ2 | p |
| Gender | | | 725 | 51.64 | 1.017 | 0.334 |
| Male | 375 | 26.71 | 202 | 53.87 | | |
| Female | 1029 | 73.29 | 523 | 50.83 | | |
| Age group, years | | | | | 12.713 | 0.005 |
| 20~29 | 410 | 29.20 | 222 | 54.15 | | |
| 30~39 | 671 | 47.79 | 352 | 52.46 | | |
| 40~49 | 241 | 17.17 | 124 | 51.45 | | |
| ≥50 | 82 | 5.84 | 27 | 32.93 | | |
| Marital status | | | | | 1.004 | 0.605 |
| Married | 1070 | 76.21 | 553 | 51.68 | | |
| Single | 310 | 22.08 | 162 | 52.26 | | |
| Divorce/widowed | 24 | 1.71 | 10 | 41.67 | | |
| Education level | | | | | 14.185 | 0.001 |
| Professional school | 156 | 11.11 | 64 | 41.03 | | |
| Junior college | 444 | 31.26 | 214 | 48.20 | | |
| College or above | 804 | 57.26 | 447 | 55.60 | | |
| Occupation | | | | | 11.389 | 0.003 |
| General practitioner | 568 | 40.46 | 306 | 53.87 | | |
| Nurse | 565 | 40.24 | 304 | 53.81 | | |
| Others | 271 | 19.30 | 115 | 42.44 | | |
| Employment | | | | | 1.721 | 0.423 |
| Permanent | 526 | 37.46 | 275 | 52.28 | | |
| contract | 817 | 58.19 | 414 | 50.67 | | |
| Other | 61 | 4.34 | 36 | 59.02 | | |
| Monthly income, RMB | | | | | 15.349 | 0.002 |
| <2000 | 122 | 8.69 | 49 | 40.16 | | |
| 2000~3999 | 539 | 38.39 | 262 | 48.61 | | |
| 4000~5999 | 444 | 31.62 | 238 | 53.60 | | |
| ≥6000 | 299 | 21.30 | 176 | 58.86 | | |
Table 2.
Univariate analysis between whether or not one experienced workplace violence.
Table 2.
Univariate analysis between whether or not one experienced workplace violence.
| | Entire sample (n = 1404) | Workplace Violence Cases (n = 725) a | Non-Workplace Violence cases (n = 679) | Statistics |
|---|
| | m | sd | m | sd | m | sd | t | p |
| Job performance | 76.02 | 10.22 | 74.64 | 10.84 | 77.48 | 9.30 | −5.257 | <0.001 |
| JD | 27.11 | 4.18 | 26.57 | 4.32 | 27.70 | 3.94 | −5.098 | <0.001 |
| TP | 24.09 | 3.64 | 23.69 | 3.88 | 24.52 | 3.32 | −4.267 | <0.001 |
| IF | 24.81 | 3.66 | 24.38 | 3.94 | 25.27 | 3.28 | −4.585 | <0.001 |
| Quality of life | 75.60 | 14.71 | 71.85 | 15.55 | 79.60 | 12.60 | −10.218 | <0.001 |
| PF | 89.78 | 11.97 | 88.57 | 12.81 | 91.07 | 10.86 | −3.935 | <0.001 |
| RP | 77.12 | 35.22 | 70.69 | 37.69 | 83.98 | 30.97 | −7.194 | <0.001 |
| BP | 87.95 | 13.80 | 85.73 | 14.74 | 90.32 | 12.29 | −6.320 | <0.001 |
| GH | 64.37 | 19.98 | 60.82 | 20.76 | 68.17 | 18.40 | −7.008 | <0.001 |
| VT | 66.88 | 16.52 | 63.42 | 16.86 | 70.57 | 15.32 | −8.293 | <0.001 |
| SF | 78.22 | 17.97 | 74.84 | 18.67 | 81.83 | 16.45 | −7.419 | <0.001 |
| RE | 74.00 | 37.00 | 66.80 | 38.80 | 81.69 | 33.34 | −7.686 | <0.001 |
| MH | 66.46 | 15.30 | 63.93 | 15.91 | 69.15 | 14.15 | −6.481 | <0.001 |
Table 3.
Correlation matrix for the study variables.
Table 3.
Correlation matrix for the study variables.
| | Workplace Violence | Job Performance | Quality of Life |
|---|
| Workplace violence | 1.0 | | |
| Job performance | −0.205 *** | 1.0 | |
| Quality of life | −0.313 *** | 0.365 *** | 1.0 |
Table 4.
Regression analysis among variables.
Table 4.
Regression analysis among variables.
| | Independent Variable | Dependent Variable | β a | t | p |
|---|
| | Workplace violence | Job performance | −0.205 | −7.836 | <0.001 |
| | | Job dedication | −0.197 | −7.524 | <0.001 |
| | | Task performance | −0.166 | −6.318 | <0.001 |
| | | Interpersonal facilitation | −0.181 | −6.908 | <0.001 |
| | Workplace violence | Quality of life | −0.313 | −12.351 | <0.001 |
| Workplace violence, Quality of life | Job performance b | −0.100 | −3.853 | <0.001 |
| 0.333 | 12.795 | <0.001 |
Table 5.
The path coefficients between structural variables.
Table 5.
The path coefficients between structural variables.
| Path | Before Correction | After Correction |
|---|
| β a | t | p | Β a | t | p |
|---|
| Quality of life | ← | Workplace violence | −0.391 | −9.435 | <0.001 | −0.313 | −7.660 | <0.001 |
| Job performance | ← | Workplace violence | −0.105 | −3.099 | 0.002 | −0.113 | −3.626 | <0.001 |
| Job performance | ← | Quality of life | 0.410 | 10.368 | <0.001 | 0.417 | 10.473 | <0.001 |
Table 6.
Fit indices for the structural models a.
Table 6.
Fit indices for the structural models a.
| | χ2 | χ2/df | SRMR | RMSEA | GFI | NFI | TFI | CFI |
|---|
| The original model | 1077.454 | 9.598 | 0.055 | 0.078 | 0.948 | 0.913 | 0.894 | 0.921 |
| The final model | 405.336 | 4.267 | 0.050 | 0.048 | 0.965 | 0.951 | 0.952 | 0.962 |


 ,
, 


{kind=link}
{kind=link}