
How Do Brown Seaweeds Work on Biomarkers of Dyslipidemia? A Systematic Review with Meta-Analysis and Meta-Regression

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data sources and Search Strategy
2.2. Eligibility Criteria
2.3. Data Extraction and Measurement Outcomes
2.4. Data and Statistical Analyses
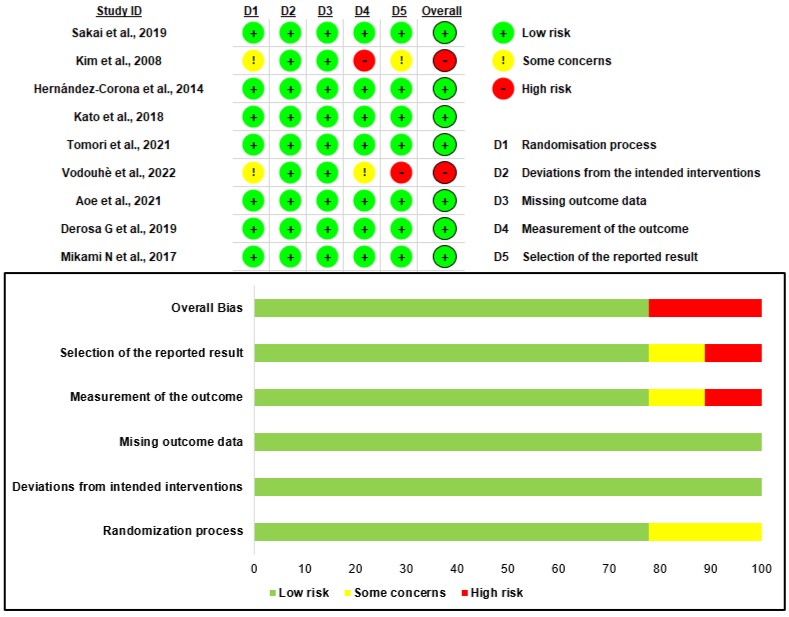
2.5. Quality Assessment
3. Results
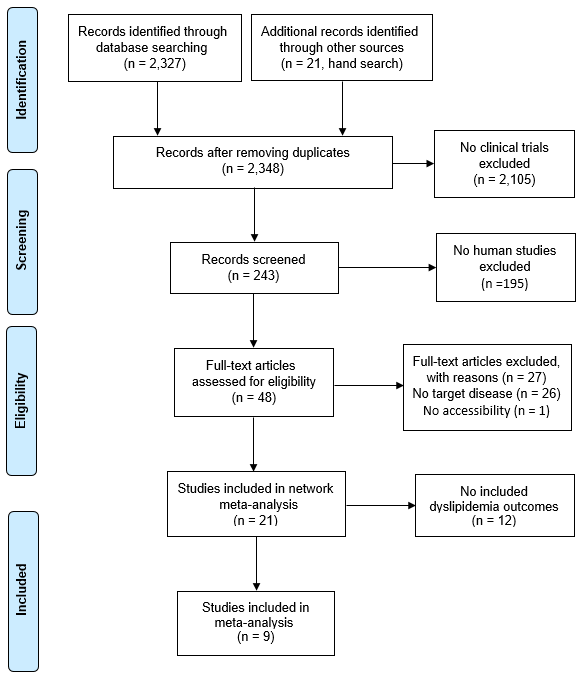
3.1. Study Selection

| Study | Geographic Location | Sample Size | Age | Type of Brown Seaweed | Dosage | Duration | Measured Outcomes |
|---|---|---|---|---|---|---|---|
| Kim 2008 [13] | Korea | 20 | 40–70 years | Laminaria japonica (Sea tangle) | 48 g | 4 weeks and 2 h | ↑ HDL-Cho, ↓ T-Cho, LDL-Cho, TG |
| Hernandez-Corona 2014 [33] | Mexico | 25 | 30–60 years | (No name given) Fucoidan extract | 500 mg | 3 months and 2 h | ↓ T-Cho, LDL-Cho |
| Mikami 2017 [34] | Japan | 40 | 30–77 years | Fucoxanthin | 220 mg | 8 weeks | ↑ HDL-Cho, ↓ LDL-Cho |
| Kato 2018 [27] | Japan | 30 | ≥20 years | (No name given) Calcium alginate extract | Ca-Alg 5%, 3.2 g Ca-Alg 8%, 5.0 g | 2 h | ↓ T-Cho, LDL-Cho, TG |
| Derosa 2019 [31] | Italy | 164 | >18 years | Ascophyllum nodosum, Fucus vesiculosus | - | 6 months | ↑ HDL-Cho, ↓ T-Cho, LDL-Cho, TG |
| Sakai 2019 [30] | Japan | 28 | 59.10 ± 13.24 years | Mozuku fucoidan extract | 1620 mg | 3 months | ↓ T-Cho |
| Aoe 2021 [29] | Japan | 48 | 20–59 years | Laminaria japonica/alginate | 6 g kelp powder/d 3.3 g alginate/d | 2 months | ↓ T-Cho, LDL-Cho |
| Tomori 2021 [28] | Japan | 40 | 47.0 ± 7.6 years | Fucoidan derived from Okinawa mozuku (South product, Uruma, Japan) | 3.0 g | 16 weeks | ↑ HDL-Cho |
| Vodouhe 2022 [32] | Canada | 56 | 18–70 years | Ascophyllum nodosum and Fucus vesiculosus Extract | 500 mg | 3 months | ↓T-Cho, LDL-Cho |
3.2. Quality Assessment
3.3. Outcomes
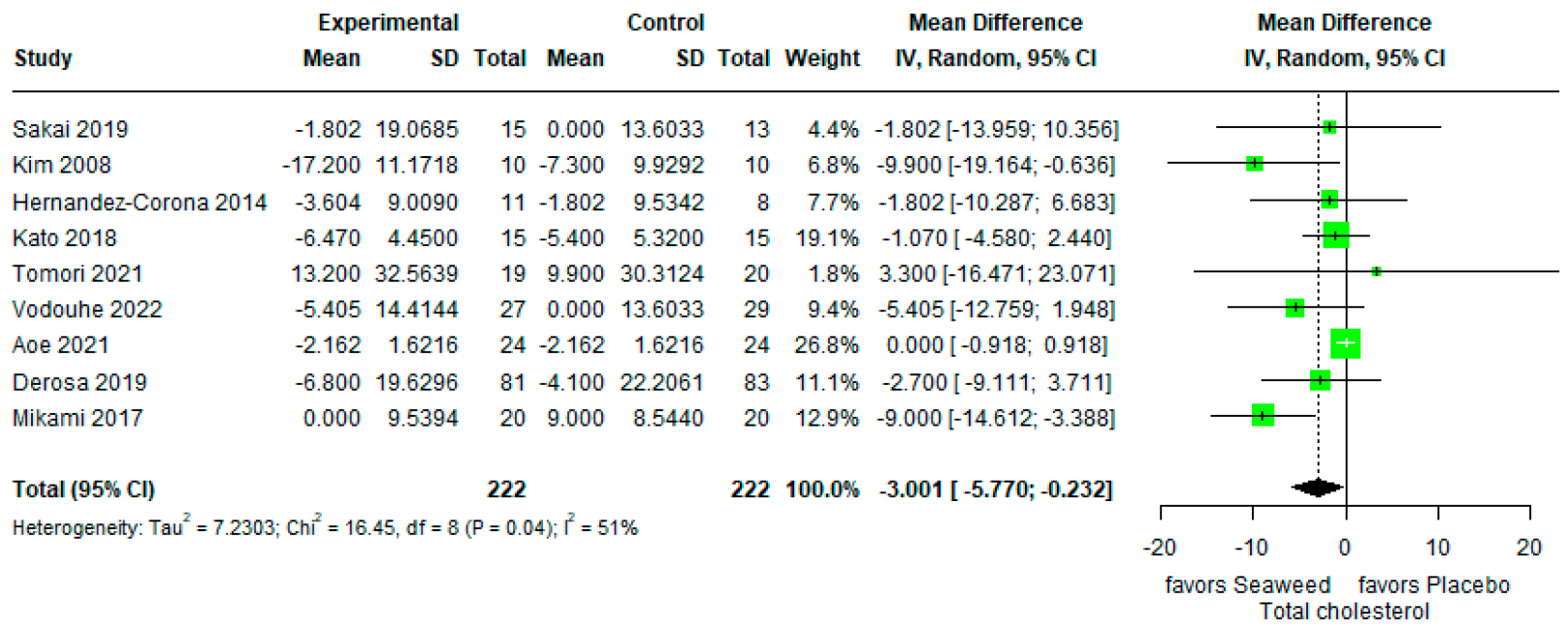
3.3.1. Total Cholesterol
3.3.2. HDL Cholesterol
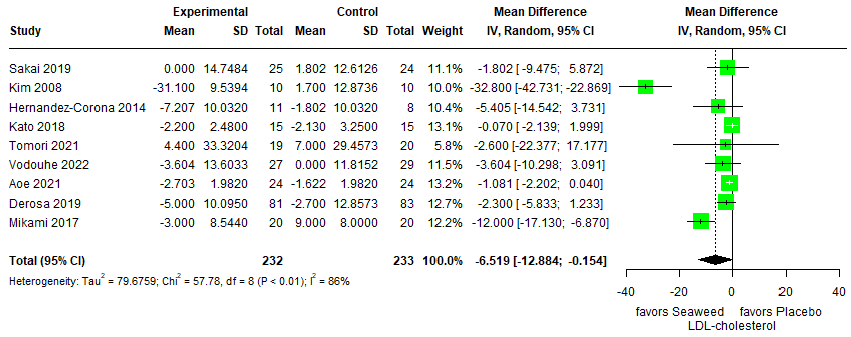
3.3.3. LDL Cholesterol
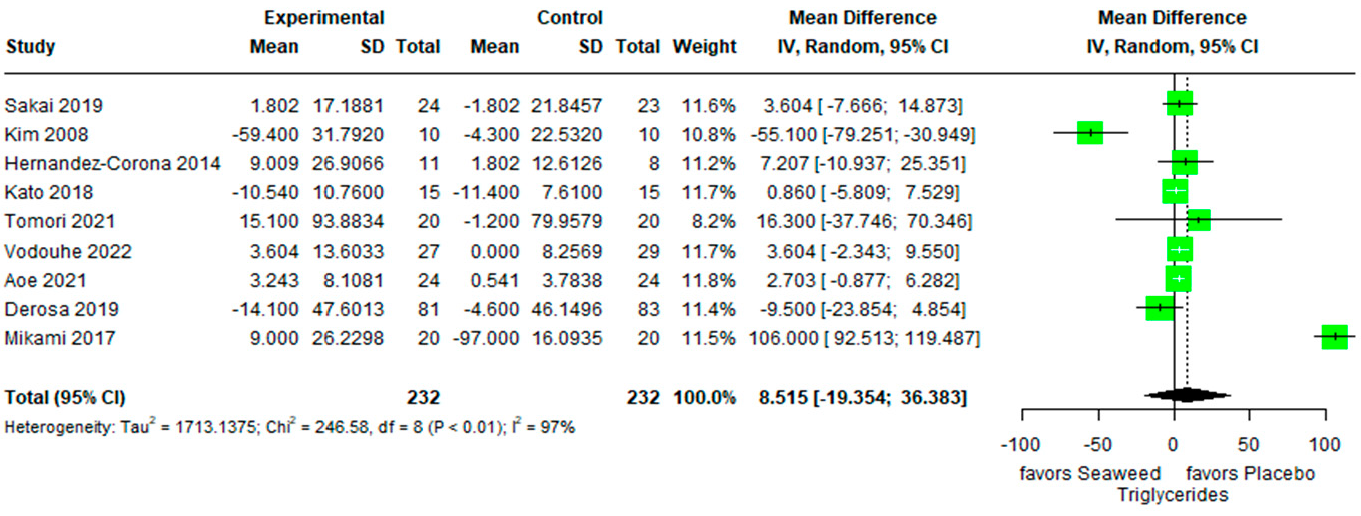
3.3.4. Triglycerides
3.4. Meta-Regression
3.5. Evidence
3.5.1. Evidence of Ascophyllum nodosum/Fucus vesiculosus
3.5.2. Evidence of Fucoidan
3.5.3. Evidence of Laminaria japonica and Undaria pinnatifida
3.5.4. Evidence of Calcium Alginate
3.5.5. Evidence of Fucoxanthin
3.6. Risk of Bias Assessment
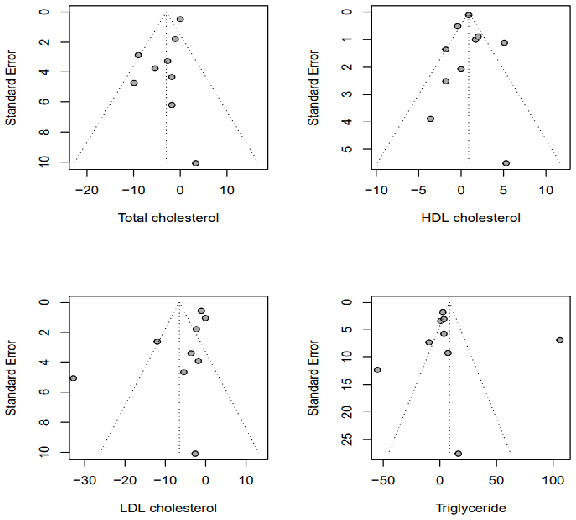
3.7. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Noncommunicable Diseases: World Health Organization. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 14 February 2023).
- Cho, S.M.J.; Lee, H.; Lee, H.-H.; Baek, J.; Heo, J.E.; Joo, H.J.; Hong, S.J.; Kim, H.C. Dyslipidemia fact sheets in Korea 2020: An analysis of nationwide population-based data. J. Lipid Atheroscler. 2021, 10, 202. [Google Scholar] [CrossRef]
- Korean Statistical Information Service (KOSIS). Available online: https://kosis.kr/statHtml/statHtml.do?orgId=177&tblId=DT_11702_N103&vw_cd=MT_ETITLE&list_id=117_11702_B01&scrId=&language=en&seqNo=&lang_mode=en&obj_var_id=&itm_id=&conn_path=MT_ETITLE&path=%252Feng%252FstatisticsList%252FstatisticsListIndex.do (accessed on 13 March 2023).
- Yao, Y.S.; Li, T.D.; Zeng, Z.H. Mechanisms underlying direct actions of hyperlipidemia on myocardium: An updated review. Lipids Health Dis. 2020, 19, 23. [Google Scholar] [CrossRef] [Green Version]
- Berman, A.N.; Blankstein, R. Optimizing dyslipidemia management for the prevention of cardiovascular disease: A focus on risk assessment and therapeutic options. Curr. Cardiol. Rep. 2019, 21, 110. [Google Scholar] [CrossRef] [PubMed]
- Marrs, J.C.; Anderson, S.L. Bempedoic acid for the treatment of dyslipidemia. Drugs Context 2020, 9, 2020-6-5. [Google Scholar] [CrossRef] [PubMed]
- Opoku, S.; Gan, Y.; Fu, W.; Chen, D.; Addo-Yobo, E.; Trofimovitch, D.; Yue, W.; Yan, F.; Wang, Z.; Lu, Z. Prevalence and risk factors for dyslipidemia among adults in rural and urban China: Findings from the China National Stroke Screening and prevention project (CNSSPP). BMC Public Health 2019, 19, 1500. [Google Scholar] [CrossRef] [PubMed]
- Ni, W.-Q.; Liu, X.-L.; Zhuo, Z.-P.; Yuan, X.-L.; Song, J.-P.; Chi, H.-S.; Xu, J. Serum lipids and associated factors of dyslipidemia in the adult population in Shenzhen. Lipids Health Dis. 2015, 14, 71. [Google Scholar] [CrossRef] [Green Version]
- Lin, L.-Y.; Hsu, C.-Y.; Lee, H.-A.; Wang, W.-H.; Kurniawan, A.L.; Chao, J.C.-J. Dietary patterns in relation to components of dyslipidemia and fasting plasma glucose in adults with dyslipidemia and elevated fasting plasma glucose in Taiwan. Nutrients 2019, 11, 845. [Google Scholar] [CrossRef] [Green Version]
- McMacken, M.; Shah, S. A plant-based diet for the prevention and treatment of type 2 diabetes. J. Geriatr. Cardiol. 2017, 14, 342. [Google Scholar]
- Kim, Y.; Keogh, J.; Clifton, P. A review of potential metabolic etiologies of the observed association between red meat consumption and development of type 2 diabetes mellitus. Metabolism 2015, 64, 768–779. [Google Scholar] [CrossRef]
- Park, J.-K.; Woo, H.W.; Kim, M.K.; Shin, J.; Lee, Y.-H.; Shin, D.H.; Shin, M.-H.; Choi, B.Y. Dietary iodine, seaweed consumption, and incidence risk of metabolic syndrome among postmenopausal women: A prospective analysis of the Korean Multi-Rural Communities Cohort Study (MRCohort). Eur. J. Nutr. 2021, 60, 135–146. [Google Scholar] [CrossRef]
- Kim, M.S.; Kim, J.Y.; Choi, W.H.; Lee, S.S. Effects of seaweed supplementation on blood glucose concentration, lipid profile, and antioxidant enzyme activities in patients with type 2 diabetes mellitus. Nutr. Res. Pract. 2008, 2, 62–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.; Siddiqui, W.J. Cholesterol levels. In StatPearls; StatPearls Publishing: Tampa, FL, USA, 2021. [Google Scholar]
- Ma, H.; Shieh, K.-J. Cholesterol and human health. Am. J. Sci. 2006, 2, 46–50. [Google Scholar]
- Cardoso, S.M.; Pereira, O.R.; Seca, A.M.; Pinto, D.C.; Silva, A.M. Seaweeds as preventive agents for cardiovascular diseases: From nutrients to functional foods. Mar. Drugs 2015, 13, 6838–6865. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gabbia, D.; De Martin, S. Brown seaweeds for the management of metabolic syndrome and associated diseases. Molecules 2020, 25, 4182. [Google Scholar] [CrossRef]
- André, R.; Pacheco, R.; Bourbon, M.; Serralheiro, M.L. Brown algae potential as a functional food against hypercholesterolemia. Foods 2021, 10, 234. [Google Scholar] [CrossRef]
- Hong, I.K.; Jeon, H.; Lee, S.B. Comparison of red, brown and green seaweeds on enzymatic saccharification process. J. Ind. Eng. Chem. 2014, 20, 2687–2691. [Google Scholar] [CrossRef]
- Thomas, I.; Siew, L.Q.; Watts, T.J.; Haque, R. Seaweed allergy. J. Allergy Clin. Immunol. 2019, 7, 714–715. [Google Scholar] [CrossRef]
- Kuda, T.; Goto, H.; Yokovama, M.; Fujii, T. Fermentable dietary fiber in dried products of brown algae and their effects on cecal microflora and levels of plasma lipid in rats. Fish. Sci. 1998, 64, 582–588. [Google Scholar] [CrossRef] [Green Version]
- Murai, U.; Yamagishi, K.; Sata, M.; Kokubo, Y.; Saito, I.; Yatsuya, H.; Ishihara, J.; Inoue, M.; Sawada, N.; Iso, H. Seaweed intake and risk of cardiovascular disease: The Japan Public Health Center–based Prospective (JPHC) Study. Am. J. Clin. Nutr. 2019, 110, 1449–1455. [Google Scholar] [CrossRef]
- Yokota, T.; Nomura, K.; Nagashima, M.; Kamimura, N. Fucoidan alleviates high-fat diet-induced dyslipidemia and atherosclerosis in ApoEshl mice deficient in apolipoprotein E expression. J. Nutr. Biochem. 2016, 32, 46–54. [Google Scholar] [CrossRef]
- Ruqqia, K.; Sultana, V.; Ara, J.; Ehteshamul-Haque, S.; Athar, M. Hypolipidaemic potential of seaweeds in normal, triton-induced and high-fat diet-induced hyperlipidaemic rats. J. Appl. Phycol. 2015, 27, 571–579. [Google Scholar] [CrossRef]
- Sterne, J.; Savović, J.; Page, M.; Elbers, R.; Blencowe, N.; Boutron, I.; Cates, C.; Cheng, H.; Corbett, M.; Eldridge, S. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, T.; Lu, C.; Li, H.; Xing, X.; Deng, X.; Li, X.; Wang, Y.; Niu, J.; Liu, Y.; Yang, K. The reporting quality and risk of bias of randomized controlled trials of acupuncture for migraine: Methodological study based on STRICTA and RoB 2.0. Complement. Ther. Med. 2020, 52, 102433. [Google Scholar] [CrossRef]
- Kato, T.; Idota, Y.; Shiragami, K.; Koike, M.; Nishibori, F.; Tomokane, M.; Seki, T.; Itabashi, K.; Hakoda, K.; Takahashi, H. Randomized, double-blind, crossover clinical trial of the effect of calcium alginate in noodles on postprandial blood glucose level. Biol. Pharm. Bull. 2018, 41, 1367–1371. [Google Scholar] [CrossRef] [Green Version]
- Tomori, M.; Nagamine, T.; Miyamoto, T.; Iha, M. Effects of Ingesting Fucoidan Derived from Cladosiphon okamuranus Tokida on Human NK Cells: A Randomized, Double-Blind, Parallel-Group, Placebo-Controlled Pilot Study. Mar. Drugs 2021, 19, 340. [Google Scholar] [CrossRef]
- Aoe, S.; Yamanaka, C.; Ohtoshi, H.; Nakamura, F.; Fujiwara, S. Effects of daily kelp (Laminaria japonica) intake on body composition, serum lipid levels, and thyroid hormone levels in healthy japanese adults: A randomized, double-blind study. Mar. Drugs 2021, 19, 352. [Google Scholar] [CrossRef]
- Sakai, C.; Abe, S.; Kouzuki, M.; Shimohiro, H.; Ota, Y.; Sakinada, H.; Takeuchi, T.; Okura, T.; Kasagi, T.; Hanaki, K. A randomized placebo-controlled trial of an oral preparation of high molecular weight fucoidan in patients with type 2 diabetes with evaluation of taste sensitivity. Yonago Acta Med. 2019, 62, 14–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Derosa, G.; Pascuzzo, M.D.; D’Angelo, A.; Maffioli, P. Ascophyllum nodosum, Fucus vesiculosus and chromium picolinate nutraceutical composition can help to treat type 2 diabetic patients. Diabetes Metab. Syndr. Obes. Targets Ther. 2019, 12, 1861–1865. [Google Scholar] [CrossRef] [Green Version]
- Vodouhè, M.; Marois, J.; Guay, V.; Leblanc, N.; Weisnagel, S.J.; Bilodeau, J.-F.; Jacques, H. Marginal Impact of Brown Seaweed Ascophyllum nodosum and Fucus vesiculosus Extract on Metabolic and Inflammatory Response in Overweight and Obese Prediabetic Subjects. Mar. Drugs 2022, 20, 174. [Google Scholar] [CrossRef]
- Hernández-Corona, D.M.; Martínez-Abundis, E.; González-Ortiz, M. Effect of fucoidan administration on insulin secretion and insulin resistance in overweight or obese adults. J. Med. Food 2014, 17, 830–832. [Google Scholar] [CrossRef]
- Mikami, N.; Hosokawa, M.; Miyashita, K.; Sohma, H.; Ito, Y.M.; Kokai, Y. Reduction of HbA1c levels by fucoxanthin-enriched akamoku oil possibly involves the thrifty allele of uncoupling protein 1 (UCP1): A randomised controlled trial in normal-weight and obese Japanese adults. J. Nutr. Sci. 2017, 6, e5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiménez-Escrig, A.; Sánchez-Muniz, F. Dietary fibre from edible seaweeds: Chemical structure, physicochemical properties and effects on cholesterol metabolism. Nutr. Res. 2000, 20, 585–598. [Google Scholar] [CrossRef]
- Calvert, R.; Schneeman, B.; Satchithanandam, S.; Cassidy, M.; Vahouny, G. Dietary fiber and intestinal adaptation: Effects on intestinal and pancreatic digestive enzyme activities. Am. J. Clin. Nutr. 1985, 41, 1249–1256. [Google Scholar] [CrossRef]
- Miettinen, T.A.; Puska, P.; Gylling, H.; Vanhanen, H.; Vartiainen, E. Reduction of serum cholesterol with sitostanol-ester margarine in a mildly hypercholesterolemic population. N. Engl. J. Med. 1995, 333, 1308–1312. [Google Scholar] [CrossRef] [Green Version]
- Wang, W.; Onnagawa, M.; Yoshie, Y.; Suzuki, T. Binding of bile salts to soluble and insoluble dietary fibers of seaweeds. Fish. Sci. 2001, 67, 1169–1173. [Google Scholar] [CrossRef]
- Ren, D.; Noda, H.; Amano, H.; Nishino, T.; Nishizawa, K. Study on antihypertensive and antihyperlipidemic effects of marine algae. Fish. Sci. 1994, 60, 83–88. [Google Scholar] [CrossRef] [Green Version]
- Beppu, F.; Hosokawa, M.; Niwano, Y.; Miyashita, K. Effects of dietary fucoxanthin on cholesterol metabolism in diabetic/obese KK-A y mice. Lipids Health Dis. 2012, 11, 112. [Google Scholar] [CrossRef] [Green Version]
- Miyashita, K.; Beppu, F.; Hosokawa, M.; Liu, X.; Wang, S. Nutraceutical characteristics of the brown seaweed carotenoid fucoxanthin. Arch. Biochem. Biophys. 2020, 686, 108364. [Google Scholar] [CrossRef]
- Yamagata, K. Prevention of cardiovascular disease through modulation of endothelial cell function by dietary seaweed intake. Phytomed. Plus 2021, 1, 100026. [Google Scholar] [CrossRef]
- Huang, L.; Wen, K.; Gao, X.; Liu, Y. Hypolipidemic effect of fucoidan from Laminaria japonica in hyperlipidemic rats. Pharm. Biol. 2010, 48, 422–426. [Google Scholar] [CrossRef]
- Park, J.; Yeom, M.; Hahm, D.-H. Fucoidan improves serum lipid levels and atherosclerosis through hepatic SREBP-2-mediated regulation. J. Pharmacol. Sci. 2016, 131, 84–92. [Google Scholar] [CrossRef] [Green Version]
- Huang, H.; Liao, D.; Pu, R.; Cui, Y. Quantifying the effects of spirulina supplementation on plasma lipid and glucose concentrations, body weight, and blood pressure. Diabetes Metab. Syndr. Obes. Targets Ther. 2018, 11, 729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mao, W.; Li, B.; Gu, Q.; Fang, Y.; Xing, H. Preliminary studies on the chemical characterization and antihyperlipidemic activity of Polysaccharide from the brown alga Sargassum fusiforme. In Asian Pacific Phycology in the 21st Century: Prospects and Challenges; Springer: Berlin/Heidelberg, Germany, 2004; pp. 263–266. [Google Scholar]
- Zhang, R.; Zhang, X.; Tang, Y.; Mao, J. Composition, isolation, purification and biological activities of Sargassum fusiforme polysaccharides: A review. Carbohydr. Polym. 2020, 228, 115381. [Google Scholar] [CrossRef]
- Cuong, H.D.; Thuy, T.T.T.; Huong, T.T.; Ly, B.M.; Van, T.T.T. Structure and hypolipidaemic activity of fucoidan extracted from brown seaweed Sargassum henslowianum. Nat. Prod. Res. 2015, 29, 411–415. [Google Scholar] [CrossRef] [PubMed]
- Gabbia, D.; Roverso, M.; Zanotto, I.; Colognesi, M.; Sayaf, K.; Sarcognato, S.; Arcidiacono, D.; Zaramella, A.; Realdon, S.; Ferri, N. A Nutraceutical Formulation Containing Brown Algae Reduces Hepatic Lipid Accumulation by Modulating Lipid Metabolism and Inflammation in Experimental Models of NAFLD and NASH. Mar. Drugs 2022, 20, 572. [Google Scholar] [CrossRef] [PubMed]
- Yoon, N.Y.; Kim, H.R.; Chung, H.Y.; Choi, J.S. Anti-hyperlipidemic effect of an edible brown algae, Ecklonia stolonifera, and its constituents on poloxamer 407-induced hyperlipidemic and cholesterol-fed rats. Arch. Pharm. Res. 2008, 31, 1564–1571. [Google Scholar] [CrossRef]
- Choi, E.-K.; Park, S.-H.; Ha, K.-C.; Noh, S.-o.; Jung, S.-J.; Chae, H.-J.; Chae, S.-W.; Park, T.-S. Clinical trial of the hypolipidemic effects of a brown alga Ecklonia cava extract in patients with hypercholesterolemia. Int. J. Pharmacol. 2015, 11, 798–805. [Google Scholar] [CrossRef]
- Gheorghe, G.; Toth, P.P.; Bungau, S.; Behl, T.; Ilie, M.; Pantea Stoian, A.; Bratu, O.G.; Bacalbasa, N.; Rus, M.; Diaconu, C.C. Cardiovascular risk and statin therapy considerations in women. Diagnostics 2020, 10, 483. [Google Scholar] [CrossRef]
- Das, S.S.; Bharadwaj, P.; Bilal, M.; Barani, M.; Rahdar, A.; Taboada, P.; Bungau, S.; Kyzas, G.Z. Stimuli-responsive polymeric nanocarriers for drug delivery, imaging, and theragnosis. Polymers 2020, 12, 1397. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}

| Parameter | Criterion |
|---|---|
| Population | Healthy participants, participants with pre-diabetes or type 2 diabetes mellitus, participants with obesity |
| Intervention | Mozuku fucoidan extract, Laminaria japonica (Sea tangle), Fucoidan extract, Sodium alginate extract, Fucoidan derived from Okinawa mozuku |
| Comparison | Placebo |
| Outcome | Total cholesterol, HDL cholesterol, LDL cholesterol, triglycerides |
| Study design | Randomized controlled trials, clinical trials |
| Total Cholesterol | HDL Cholesterol | LDL Cholesterol | Triglyceride | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variation | k | SMD (95% CI) | p | k | SMD (95% CI) | p | k | SMD (95% CI) | p | k | SMD (95% CI) | p |
| Duration | 0.598 | 0.172 | 0.128 | 0.666 | ||||||||
| >3 months | 5 | −2.711 (−7.991–2.570) | 4 | 0.027 (−2.623–2.677) | 5 | −3.144 (−11.885–5.597) | 5 | 3.633 (−39.159–46.425) | ||||
| <3 months | 3 | −4.681 (−9.755–0.392) | 3 | 2.461 (0.184–4.737) | 3 | −13.775 (−24.314–−3.236) | 3 | 18.845 (−35.305–72.995) | ||||
| Race | 0.937 | 0.327 | 0.738 | 0.919 | ||||||||
| Asian | 5 | −4.032 (−8.852–0.788 | 5 | 2.057 (−0.193–4.307) | 5 | −10.118 (−20.527–0.291) | 5 | 15.116 (−31.827–62.058) | ||||
| Hispanic | 1 | −1.802 (−13.130–9.527) | - | - | - | 1 | −5.405 (−28.578–17.767) | 1 | 7.207 (−96.122–110.536) | |||
| Caucasian | 2 | −3.968 (−11.163–3.226) | 2 | 0.083 (−3.164–3.330) | 2 | −2.930 (−18.448–12.588) | 2 | −2.895 (−75.240–69.451) | ||||
| Female participants rate | 8 | −13.141 a (−42.559–16.316) | 0.382 | 7 | 5.994 a (−13.116–25.104) | 0.539 | 8 | −14.172 a (−70.258–41.914) | 0.620 | 8 | 86.767 a (−153.590–327.124) | 0.479 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shin, D.; Shim, S.R.; Wu, Y.; Hong, G.; Jeon, H.; Kim, C.-G.; Lee, K.J. How Do Brown Seaweeds Work on Biomarkers of Dyslipidemia? A Systematic Review with Meta-Analysis and Meta-Regression. Mar. Drugs 2023, 21, 220. https://doi.org/10.3390/md21040220
Shin D, Shim SR, Wu Y, Hong G, Jeon H, Kim C-G, Lee KJ. How Do Brown Seaweeds Work on Biomarkers of Dyslipidemia? A Systematic Review with Meta-Analysis and Meta-Regression. Marine Drugs. 2023; 21(4):220. https://doi.org/10.3390/md21040220
Chicago/Turabian StyleShin, Dayeon, Sung Ryul Shim, Yueying Wu, Gayeon Hong, Hyunyu Jeon, Choong-Gon Kim, and Kyung Ju Lee. 2023. "How Do Brown Seaweeds Work on Biomarkers of Dyslipidemia? A Systematic Review with Meta-Analysis and Meta-Regression" Marine Drugs 21, no. 4: 220. https://doi.org/10.3390/md21040220