

A Quantitative Assessment of Cerebral Hemodynamic Perturbations Associated with Long R-R Intervals in Atrial Fibrillation: A Pilot-Case-Based Experience
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Anticoagulation Protocol and Drug Therapy
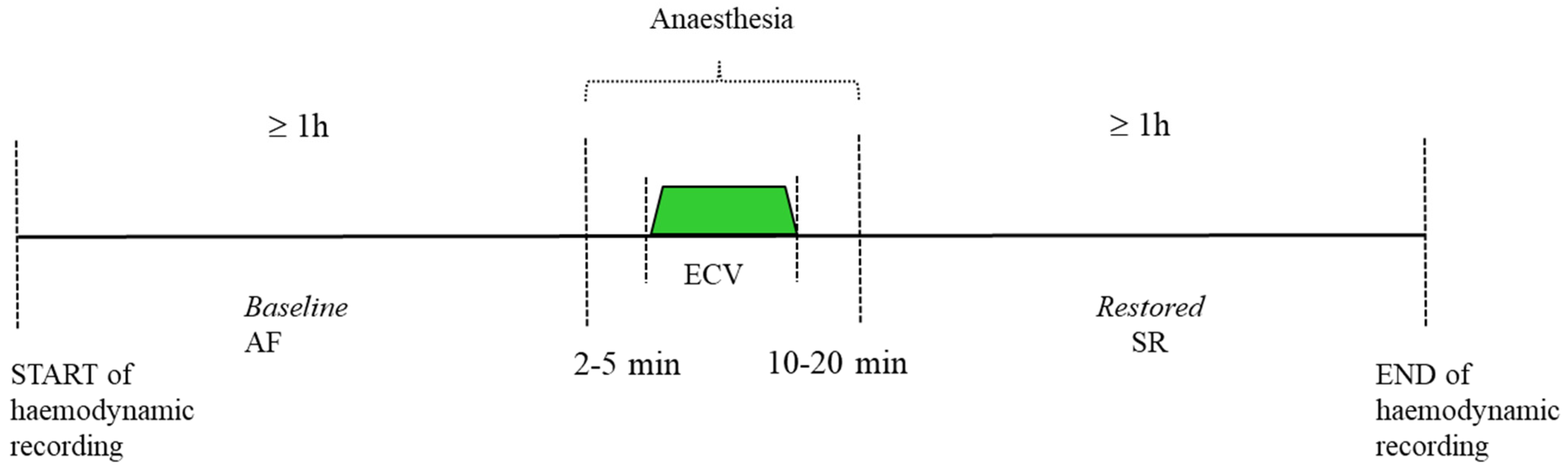
2.3. Electrical Cardioversion and Monitoring
- Cerebral hemodynamic measurements
- b.
- Systemic hemodynamic measurements
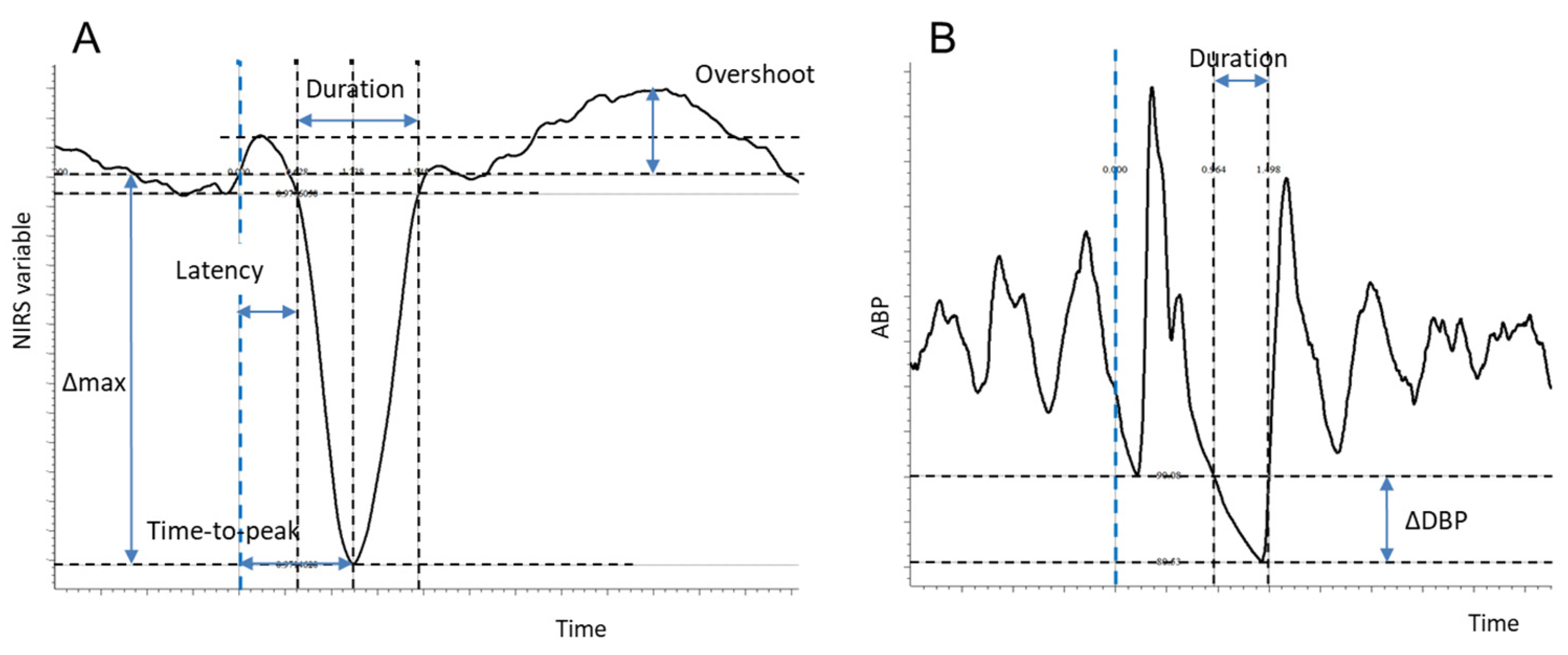
2.4. Analysis
- (a)
- Latency of the response: the time taken to reach 5% of Δmax from the trigger;
- (b)
- Time to peak: the time taken to reach the maximum effect (Δmax) from the trigger;
- (c)
- Duration: the time taken to return to the basal (pre-trigger) level from the beginning of the response (latency);
- (d)
- Overshoot: only for the TOI and Hb(diff), the occurrence of a positive overshoot following the recovery of the initial decrease was detected if the signal exceeded the maximum baseline value and was quantified as the difference between the maximum achieved value and the basal level.
- (a)
- ⊗DBP: the difference between the diastolic blood pressure (DBP) of the cardiac cycle preceding the trigger and the DBP of the cardiac cycle corresponding to the trigger;
- (b)
- Latency: the time taken to reach the diastolic level of the previous cardiac cycle;
- (c)
- Duration: the time taken from the ABP of the trigger’s cardiac cycle to return to the DBP level of the previous cardiac cycle from the beginning of the response (latency).
2.5. Statistics
3. Results



4. Discussion
4.1. Effect on Cerebral Hemodynamics
4.2. The Active Cerebrovascular Response to the Hypotensive Insult
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Saglietto, A.; Scarsoglio, S.; Ridolfi, L.; Gaita, F.; Anselmino, M. Higher ventricular rahte during atrial fibrillation relates to increased cerebral hypoperfusions and hypertensive events. Sci. Rep. 2019, 9, 3779. [Google Scholar] [CrossRef]
- Saglietto, A.; Scarsoglio, S.; Canova, D.; Roatta, S.; Gianotto, N.; Piccotti, A.; Franzin, S.; Gaita, F.; De Ferrari, G.M.; Ridolfi, L.; et al. Increased beat-to-beat variability of cerebral microcirculatory perfusion during atrial fibrillation: A near-infrared spectroscopy study. EP Eur. 2021, 23, 1219–1226. [Google Scholar] [CrossRef]
- Zhai, Y.; Hu, F.; Yuan, L.; Ye, X.; Shi, W.; Yang, R.; Cao, Y.; Sun, J.; He, J.; Xu, F. Atrial fibrillation increases the risk of all-cause dementia, Alzheimer’s disease, and vascular dementia: A cohort study of 373, 415 participants in the UK Biobank. J. Affect. Disord. 2024, 351, 323–330. [Google Scholar] [CrossRef]
- Carbone, G.; Ercolano, E.; Bencivenga, L.; Palaia, M.E.; Scognamiglio, F.; Rengo, G.; Femminella, G.D. Atrial Fibrillation and Dementia: Focus on Shared Pathophysiological Mechanisms and Therapeutic Implications. J. Am. Med. Dir. Assoc. 2024, 25, 465–469. [Google Scholar] [CrossRef]
- Calvert, P.; Gupta, D.; Lip, G.Y.H. The neurocognitive effects of atrial fibrillation: Benefits of the ABC pathway. Eur. Heart J.-Cardiovasc. Pharmacother. 2023, 9, 413–420. [Google Scholar] [CrossRef]
- Al-Rawi, P.G.; Kirkpatrick, P.J. Tissue oxygen index: Thresholds for cerebral ischemia using near-infrared spectroscopy. Stroke 2006, 37, 2720–2725. [Google Scholar] [CrossRef]
- Quaresima, V.; Sacco, S.; Totaro, R.; Ferrari, M. Noninvasive measurement of cerebral hemoglobin oxygen saturation using two near infrared spectroscopy approaches. J. Biomed. Opt. 2000, 5, 201–205. [Google Scholar] [CrossRef]
- Fadel, P.J.; Keller, D.M.; Watanabe, H.; Raven, P.B.; Thomas, G.D. Noninvasive assessment of sympathetic vasoconstriction in human and rodent skeletal muscle using near-infrared spectroscopy and Doppler ultrasound. J. Appl. Physiol. 2004, 96, 1323–1330. [Google Scholar] [CrossRef]
- Fantini, S.; Sassaroli, A.; Tgavalekos, K.T.; Kornbluth, J. Cerebral blood flow and autoregulation: Current measurement techniques and prospects for noninvasive optical methods. Neurophotonics 2016, 3, 031411. [Google Scholar] [CrossRef]
- Camm, A.J.; Kirchhof, P.; Lip, G.Y.H.; Schotten, U.; Savelieva, I.; Ernst, S.; Van Gelder, I.C.; Al-Attar, N.; Hindricks, G.; Prendergast, B.; et al. Guidelines for the management of atrial fibrillation. Europace 2010, 1360–1420. [Google Scholar]
- Toso, E.; Blandino, A.; Sardi, D.; Battaglia, A.; Garberoglio, L.; Miceli, S.; Azzaro, G.; Capello, A.L.; Gaita, F. Electrical cardioversion of persistent atrial fibrillation: Acute and long-term results stratified according to arrhythmia duration. Pacing Clin. Electrophysiol. 2012, 35, 1126–1134. [Google Scholar] [CrossRef]
- Wutzler, A.; Nee, J.; Boldt, L.H.; Kühnle, Y.; Gräser, S.; Schröder, T.; Haverkamp, W.; Storm, C. Improvement of cerebral oxygen saturation after successful electrical cardioversion of atrial fibrillation. Europace 2014, 16, 189–194. [Google Scholar] [CrossRef]
- Barrett, O.S.H.; Macdonald, S.P.J.; Playford, D.A. Near-infrared spectroscopy-based microcirculatory assessment in acute atrial fibrillation. Anaesth. Intensive Care 2015, 43, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Toso, E.; Iannaccone, M.; Caponi, D.; Rotondi, F.; Santoro, A.; Gallo, C.; Scaglione, M.; Gaita, F. Does antiarrhythmic drugs premedication improve electrical cardioversion success in persistent atrial fibrillation? J. Electrocardiol. 2017, 50, 294–300. [Google Scholar] [CrossRef] [PubMed]
- Canova, D.; Roatta, S.; Bosone, D.; Micieli, G. Inconsistent detection of changes in cerebral blood volume by near infrared spectroscopy in standard clinical tests. J. Appl. Physiol. 2011, 110, 1646–1655. [Google Scholar] [CrossRef] [PubMed]
- Wagner, B.P.; Pfenninger, J. Dynamic cerebral autoregulatory response to blood pressure rise measured by near-infrared spectroscopy and intracranial pressure. Crit. Care Med. 2002, 30, 2014–2021. [Google Scholar] [CrossRef]
- Delpy, D.T.; Cope, M. Quantification in tissue near-infrared spectroscopy. Philos. Trans. R. Soc. B Biol. Sci. 1997, 352, 649. [Google Scholar] [CrossRef]
- Saglietto, A.; Scarsoglio, S.; Canova, D.; De Ferrari, G.M.; Ridolfi, L.; Anselmino, M. Beat-to-beat finger photoplethysmography in atrial fibrillation patients undergoing electrical cardioversion. Sci. Rep. 2023, 13, 6751. [Google Scholar] [CrossRef] [PubMed]
- Shoemaker, L.N.; Milej, D.; Sajid, A.; Mistry, J.; Lawrence, K.S.; Shoemaker, J.K. Characterization of cerebral macro- and microvascular hemodynamics during transient hypotension. J. Appl. Physiol. 2023, 135, 717–725. [Google Scholar] [CrossRef]
- Tzeng, Y.C.; MacRae, B.A.; Ainslie, P.N.; Chan, G.S.H. Fundamental relationships between blood pressure and cerebral blood flow in humans. J. Appl. Physiol. 2014, 117, 1037–1048. [Google Scholar] [CrossRef]
- Davis, M.J. Perspective: Physiological role(s) of the vascular myogenic response. Microcirculation 2012, 19, 99–114. [Google Scholar] [CrossRef]
- Brassard, P.; Roy, M.A.; Burma, J.S.; Labrecque, L.; Smirl, J.D. Quantification of dynamic cerebral autoregulation: Welcome to the jungle! Clin. Auton. Res. 2023, 33, 791–810. [Google Scholar] [CrossRef]
- Aaslid, R.; Newell, D.W.; Stooss, R.; Sorteberg, W.; Lindegaard, K.F. Assessment of cerebral autoregulation dynamics from simultaneous arterial and venous transcranial Doppler recordings in humans. Stroke 1991, 22, 1148–1154. [Google Scholar] [CrossRef]
- Kainerstorfer, J.M.; Sassaroli, A.; Tgavalekos, K.T.; Fantini, S. Cerebral autoregulation in the microvasculature measured with near-infrared spectroscopy. J. Cereb. Blood Flow. Metab. 2015, 35, 959–966. [Google Scholar] [CrossRef]
- Parthasarathy, A.B.; Gannon, K.P.; Baker, W.B.; Favilla, C.G.; Balu, R.; Kasner, S.E.; Yodh, A.G.; Detre, J.A.; Mullen, M.T. Dynamic autoregulation of cerebral blood flow measured non-invasively with fast diffuse correlation spectroscopy. J. Cereb. Blood Flow. Metab. 2018, 38, 230–240. [Google Scholar] [CrossRef]
- Scholkmann, F.; Kleiser, S.; Metz, A.J.; Zimmermann, R.; Mata Pavia, J.; Wolf, U.; Wolf, M. A review on continuous wave functional near-infrared spectroscopy and imaging instrumentation and methodology. Neuroimage 2014, 85 Pt 1, 6–27. [Google Scholar] [CrossRef]
- Moerman, A.T.; Vandenheuvel, M.; Tuybens, P.J.; Van Gompel, C.; De Hert, S.G. Incongruous effect of phenylephrine on changes in cerebral blood volume measured by near-infrared spectroscopy (NIRS) indicating extracranial contamination. J. Clin. Monit. Comput. 2022, 36, 745–750. [Google Scholar] [CrossRef] [PubMed]
- Grassi, B.; Quaresima, V. Near-infrared spectroscopy and skeletal muscle oxidative function in vivo in health and disease: A review from an exercise physiology perspective. J. Biomed. Opt. 2016, 21, 091313. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| THI (%) | TOI (%) | tHb (mmol/L) | O2Hb (mmol/L) | HHbdecrease * (mmol/L) | HHbincrease (mmol/L) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | St Dev | Mean | St Dev | Mean | St Dev | Mean | St Dev | Mean | St Dev | Mean | St Dev | |
| Dmax | −0.92 | 0.46 | −0.79 | 0.37 | −0.68 | 0.22 | −0.62 | 0.20 | −0.07 | 0.04 | 0.14 | 0.09 |
| latency (s) | 0.68 | 0.13 | 0.81 | 0.28 | 0.73 | 0.10 | 0.74 | 0.11 | 0.69 | 0.16 | 2.06 | 0.62 |
| time to peak (s) | 1.41 | 0.24 | 2.71 | 0.47 | 1.43 | 0.21 | 1.52 | 0.36 | 1.24 | 0.25 | 3.49 | 0.56 |
| duration (s) | 1.86 | 0.80 | 5.17 | 0.94 | 3.91 | 0.89 | 4.90 | 1.03 | 1.20 | 0.56 | 5.66 | 2.12 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Canova, D.; Roatta, S.; Saglietto, A.; Scarsoglio, S.; Gianotto, N.R.; Piccotti, A.; De Ferrari, G.M.; Ridolfi, L.; Anselmino, M. A Quantitative Assessment of Cerebral Hemodynamic Perturbations Associated with Long R-R Intervals in Atrial Fibrillation: A Pilot-Case-Based Experience. Medicina 2024, 60, 531. https://doi.org/10.3390/medicina60040531
Canova D, Roatta S, Saglietto A, Scarsoglio S, Gianotto NR, Piccotti A, De Ferrari GM, Ridolfi L, Anselmino M. A Quantitative Assessment of Cerebral Hemodynamic Perturbations Associated with Long R-R Intervals in Atrial Fibrillation: A Pilot-Case-Based Experience. Medicina. 2024; 60(4):531. https://doi.org/10.3390/medicina60040531
Chicago/Turabian StyleCanova, Daniela, Silvestro Roatta, Andrea Saglietto, Stefania Scarsoglio, Nefer Roberta Gianotto, Alessandro Piccotti, Gaetano Maria De Ferrari, Luca Ridolfi, and Matteo Anselmino. 2024. "A Quantitative Assessment of Cerebral Hemodynamic Perturbations Associated with Long R-R Intervals in Atrial Fibrillation: A Pilot-Case-Based Experience" Medicina 60, no. 4: 531. https://doi.org/10.3390/medicina60040531