
Atrial Pacing Negatively Affects Left Atrial Morphological and Functional Parameters Similarly to Atrioventricular Dyssynchrony
Abstract
:1. Introduction
2. Materials and Methods
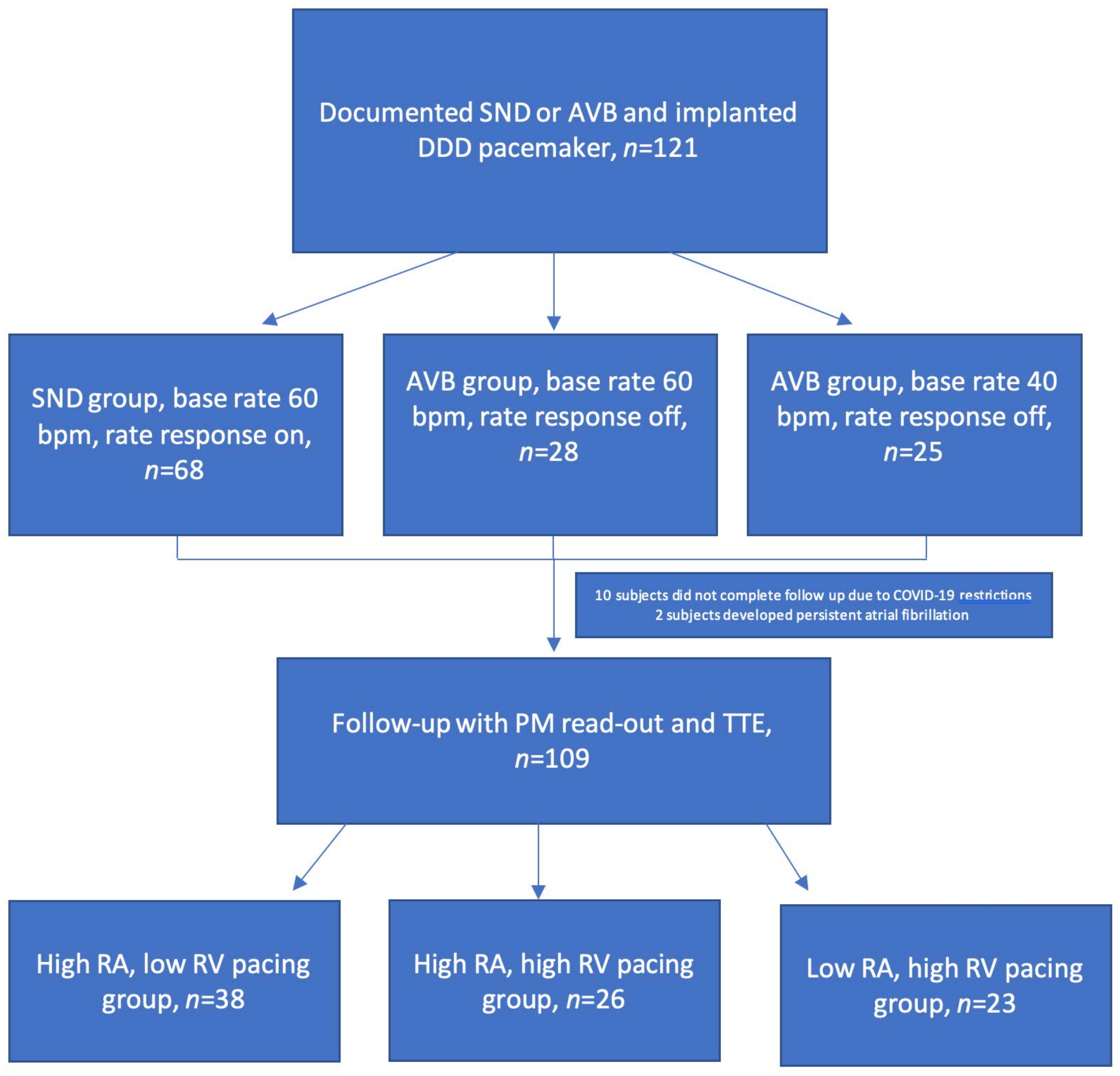
2.1. Study Subjects
2.2. Echocardiography
2.3. Left Atrium Analysis
2.4. Follow-Up Visit Procedure
2.5. Statistical Analysis
3. Results
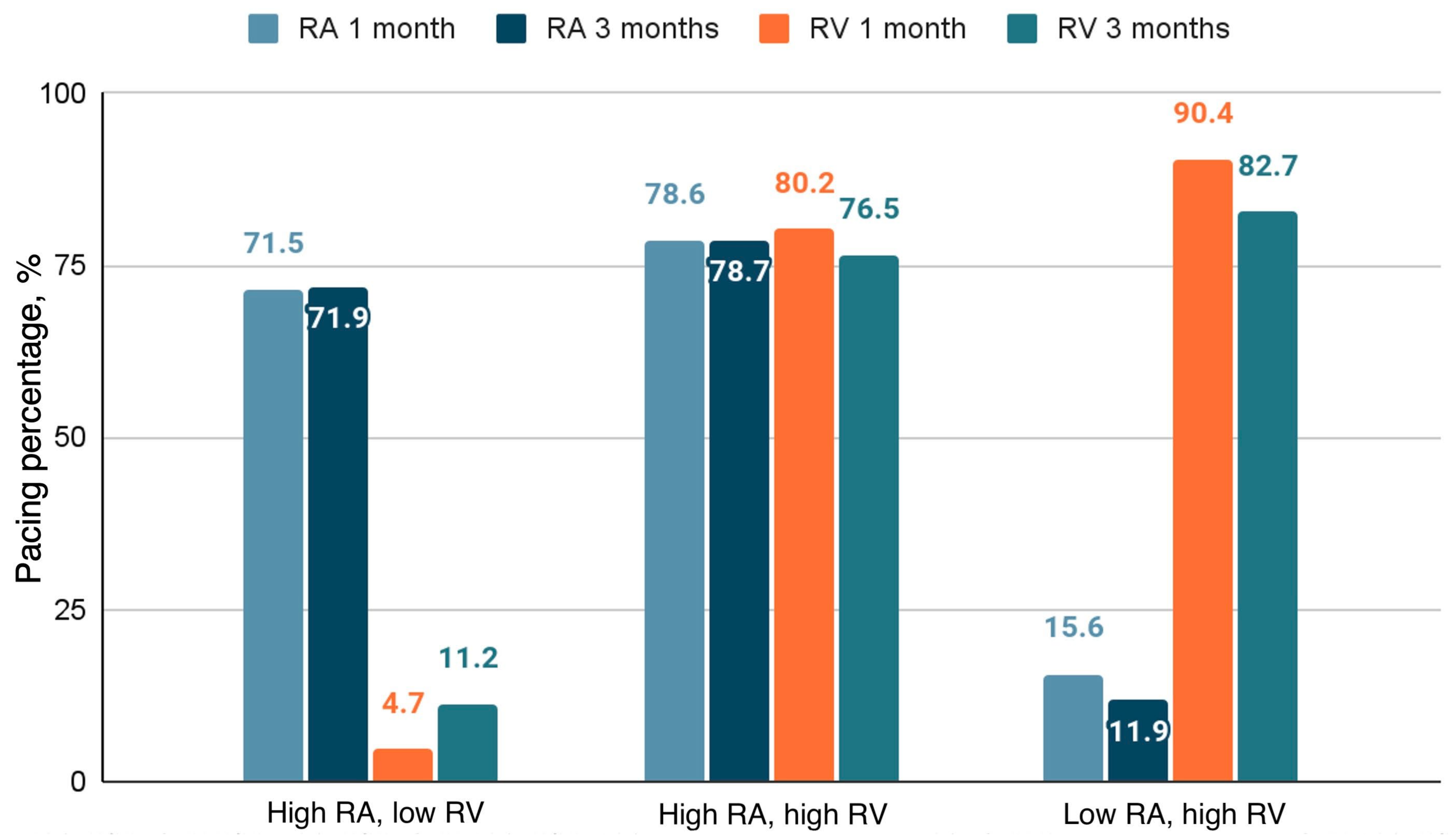
3.1. Pacing Distribution
3.2. Baseline Parameters


3.3. Follow-Up
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Glikson, M.; Nielsen, J.C.; Kronborg, M.B.; Michowitz, Y.; Auricchio, A.; Barbash, I.M.; Barrabés, J.A.; Boriani, G.; Braunschweig, F.; Brignole, M.; et al. 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy. Eur. Heart J. 2021, 42, 3427–3520. [Google Scholar] [CrossRef] [PubMed]
- Nikolaidou, T.; Fox, D.J.; Brown, B.D. Bradycardia pacing. Medicine 2018, 46, 646–651. [Google Scholar] [CrossRef]
- Kerr, C.R.; Connolly, S.J.; Abdollah, H.; Roberts, R.S.; Gent, M.; Yusuf, S.; Gillis, A.M.; Tang, A.S.; Talajic, M.; Klein, G.J.; et al. Canadian Trial of Physiological Pacing: Effects of physiological pacing during long-term follow-up. Circulation 2004, 109, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Brenyo, A.; Goldenberg, I.; Barsheshet, A. The Downside of Right Ventricular Apical Pacing. Ind. Pacing Electrophysiol. J. 2012, 12, 102–113. [Google Scholar] [CrossRef] [PubMed]
- Sweeney, M.O.; Hellkamp, A.S.; Ellenbogen, K.A.; Greenspon, A.J.; Freedman, R.A.; Lee, K.L.; Lamas, G.A.; MOde Selection Trial Investigators. Adverse Effect of Ventricular Pacing on Heart Failure and Atrial Fibrillation Among Patients With Normal Baseline QRS Duration in a Clinical Trial of Pacemaker Therapy for Sinus Node Dysfunction. Circulation 2003, 107, 2932–2937. [Google Scholar] [CrossRef]
- Sharma, A.D.; Rizo-Patron, C.; Hallstrom, A.P.; O’Neill, G.P.; Rothbart, S.; Martins, J.B.; Roelke, M.; Steinberg, J.S.; Greene, H.L.; DAVID Investigators. Percent right ventricular pacing predicts outcomes in the DAVID trial. Heart Rhythm. 2005, 2, 830–834. [Google Scholar] [CrossRef]
- Wilkoff, B.L.; Cook, J.R.; Epstein, A.E.; Greene, H.L.; Hallstrom, A.P.; Hsia, H.; Kutalek, S.P.; Sharma, A.; Dual Chamber and VVI Implantable Defibrillator Trial Investigators. Dual-Chamber Pacing or Ventricular Backup Pacing in Patients With an Implantable Defibrillator. JAMA 2002, 288, 3115–3123. [Google Scholar] [CrossRef]
- Xie, J.-M.; Fang, F.; Zhang, Q.; Chan, J.Y.-S.; Yip, G.W.-K.; Sanderson, J.E.; Lam, Y.-Y.; Yan, B.P.; Yu, C.-M. Left atrial remodeling and reduced atrial pump function after chronic right ventricular apical pacing in patients with preserved ejection fraction. Int. J. Cardiol. 2012, 157, 364–369. [Google Scholar] [CrossRef]
- Johner, N.; Namdar, M.; Shah, D.C. Intra- and interatrial conduction abnormalities: Hemodynamic and arrhythmic significance. J. Interv. Card. Electrophysiol. 2018, 52, 293–302. [Google Scholar] [CrossRef]
- Stefanadis, C.; Dernellis, J.; Toutouzas, P. A clinical appraisal of left atrial function. Eur. Heart J. 2001, 22, 22–36. [Google Scholar] [CrossRef]
- Karayannis, G.; Kitsios, G.; Kotidis, H.; Triposkiadis, F. Left atrial remodelling contributes to the progression of asymptomatic left ventricular systolic dysfunction to chronic symptomatic heart failure. Heart Fail. Rev. 2008, 13, 91–98. [Google Scholar] [CrossRef]
- Rossi, A.; Gheorghiade, M.; Triposkiadis, F.; Solomon, S.D.; Pieske, B.; Butler, J. Left Atrium in Heart Failure with Preserved Ejection Fraction. Circ. Heart Fail. 2014, 7, 1042–1049. [Google Scholar] [CrossRef] [PubMed]
- Martens, P.; Deferm, S.; Bertrand, P.B.; Verbrugge, F.H.; Ramaekers, J.; Verhaert, D.; Dupont, M.; Vandervoort, P.M.; Mullens, W. The Detrimental Effect of RA Pacing on LA Function and Clinical Outcome in Cardiac Resynchronization Therapy. JACC Cardiovasc. Imaging 2020, 13, 895–906. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.M.; Cho, K.I.; Cha, T.J.; Heo, J.H.; Kim, H.S.; Lee, J.W. Left atrial responses to acute right ventricular apical pacing in patients with sick sinus syndrome. Echocardiography 2013, 30, 1042–1050. [Google Scholar] [CrossRef]
- Viezelis, M.; Neverauskaite-Piliponiene, G.; Marcinkeviciene, A.; Teleisyte, E.; Kazakevicius, T.; Zabiela, V.; Kviesulaitis, V.; Jurkevicius, R.; Puodziukynas, A. Atrial Pacing Affects Left Atrial Morphological and Functional Parameters Early after Pacemaker Implantation. Medicina 2022, 58, 1283. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 233–271. [Google Scholar] [CrossRef] [PubMed]
- Hoit, B.D. Left Atrial Size and Function. J. Am. Coll. Cardiol. 2014, 63, 493–505. [Google Scholar] [CrossRef]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F., 3rd; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2016, 29, 277–314. [Google Scholar] [CrossRef] [PubMed]
- Kurt, M.; Wang, J.; Torre-Amione, G.; Nagueh, S.F. Left Atrial Function in Diastolic Heart Failure. Circ. Cardiovasc. Imaging 2009, 2, 10–15. [Google Scholar] [CrossRef]
- Lin, Y.S.; Guo, G.B.; Chen, Y.L.; Tsai, T.H.; Pan, K.L.; Liu, W.H.; Chen, M.C. Atrial enlargement in symptomatic heart block patients with preserved left ventricular function: Possibly related to atrioventricular dyssynchrony. Int. J. Cardiol. 2011, 148, 280–284. [Google Scholar] [CrossRef]
- Sparks, P.B.; Mond, H.G.; Vohra, J.K.; Yapanis, A.G.; Grigg, L.E.; Kalman, J.M. Mechanical remodeling of the left atrium after loss of atrioventricular synchrony. A long-term study in humans. Circulation 1999, 100, 1714–1721. [Google Scholar] [CrossRef] [PubMed]
- Kılıçaslan, B.; Vatansever Ağca, F.; Kılıçaslan, E.E.; Kınay, O.; Tigen, K.; Cakır, C.; Nazlı, C.; Ergene, O. Comparison of DDD versus VVIR pacing modes in elderly patients with atrioventricular block. Turk Kardiyol. Dern. Ars. 2012, 40, 331–336. [Google Scholar] [CrossRef] [PubMed]
- Ouali, S.; Neffeti, E.; Ghoul, K.; Hammas, S.; Kacem, S.; Gribaa, R.; Remedi, F.; Boughzela, E. DDD versus VVIR pacing in patients, ages 70 and over, with complete heart block. Pacing. Clin. Electrophysiol. 2010, 33, 583–589. [Google Scholar] [CrossRef] [PubMed]
- Rossi, A.; Cicoira, M.; Florea, V.G.; Golia, G.; Florea, N.D.; Khan, A.A.; Murray, S.T.; Nguyen, J.T.; O’Callaghan, P.; Anand, I.S.; et al. Chronic heart failure with preserved left ventricular ejection fraction: Diagnostic and prognostic value of left atrial size. Int. J. Cardiol. 2006, 110, 386–392. [Google Scholar] [CrossRef] [PubMed]
- Kronborg, M.B.; Frausing, M.H.J.P.; Malczynski, J.; Riahi, S.; Haarbo, J.; Holm, K.F.; Larroudé, C.E.; Albertsen, A.E.; Svendstrup, L.; Hintze, U.; et al. Atrial pacing minimization in sinus node dysfunction and risk of incident atrial fibrillation: A randomized trial. Eur. Heart J. 2023, 44, 4246–4255. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.Y.; Tsai, W.C.; Liu, Y.W.; Li, W.H.; Li, Y.H.; Tsai, L.M.; Lin, L.J. Long-term effect of septal or apical pacing on left and right ventricular function after permanent pacemaker implantation. Echocardiography 2013, 30, 812–819. [Google Scholar] [CrossRef] [PubMed]
- Liang, H.-Y.; Cheng, A.; Chang, K.-C.; Berger, R.D.; Agarwal, K.; Eulitt, P.; Corretti, M.; Tomaselli, G.; Calkins, H.; Kass, D.A.; et al. Influence of Atrial Function and Mechanical Synchrony on LV Hemodynamic Status in Heart Failure Patients on Resynchronization Therapy. JACC Cardiovasc. Imaging 2011, 4, 691–698. [Google Scholar] [CrossRef]
- Cha, Y.-M.; Nishimura, R.A.; Hayes, D.L. Difference in mechanical atrioventricular delay between atrial sensing and atrial pacing modes in patients with hypertrophic and dilated cardiomyopathy: An electrical hemodynamic catheterization study. J. Interv. Card. Electrophysiol. 2002, 6, 133–140. [Google Scholar] [CrossRef]
- Matsumoto, K.; Tanaka, H.; Imanishi, J.; Tatsumi, K.; Motoji, Y.; Miyoshi, T.; Onishi, T.; Kawai, H.; Hirata, K. Preliminary observations of prognostic value of left atrial functional reserve during dobutamine infusion in patients with dilated cardiomyopathy. J. Am. Soc. Echocardiogr. 2014, 27, 430–439. [Google Scholar] [CrossRef]
- Sahebjam, M.; Zoroufian, A.; Sadeghian, H.; Roomi, Z.S.; Sardari, A.; Mirzamani, S.S.; Tokaldany, M.L.; Jalali, A. Relationship between left atrial function and size and level of left ventricular dyssynchrony in heart failure patients. Echocardiography 2013, 30, 772–777. [Google Scholar] [CrossRef] [PubMed]
- Bernheim, A.; Ammann, P.; Sticherling, C.; Burger, P.; Schaer, B.; Brunner-La Rocca, H.P.; Eckstein, J.; Kiencke, S.; Kaiser, C.; Linka, A.; et al. Right atrial pacing impairs cardiac function during resynchronization therapy: Acute effects of DDD pacing compared to VDD pacing. J. Am. Coll. Cardiol. 2005, 45, 1482–1487. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Seo, J.H.; Choi, K.H.; Lee, S.H.; Choi, J.O.; Jeon, E.S.; Yang, J.H. Prognostic Implications of Left Atrial Stiffness Index in Heart Failure Patients with Preserved Ejection Fraction. JACC Cardiovasc. Imaging 2023, 16, 435–445. [Google Scholar] [CrossRef]
- Kusumoto, F.M.; Schoenfeld, M.H.; Barrett, C.; Edgerton, J.R.; Ellenbogen, K.A.; Gold, M.R.; Goldschlager, N.F.; Hamilton, R.M.; Joglar, J.A.; Kim, R.J.; et al. 2018 ACC/AHA/HRS Guideline on the Evaluation and Management of Patients With Bradycardia and Cardiac Conduction Delay: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines, and the Heart Rhythm Society. J. Am. Coll. Cardiol. 2019, 74, 932–987. [Google Scholar] [CrossRef] [PubMed]
- Biffi, M.; Melissano, D.; Rossi, P. The OPTI-MIND study: A prospective, observational study of pacemaker patients according to pacing modality and primary indications. Europace 2014, 16, 689–697. [Google Scholar] [CrossRef]
- Wang, M.; Siu, C.W.; Lee, K.L.; Yue, W.S.; Yan, G.H.; Lee, S.; Lau, C.P.; Tse, H.F. Effects of right low atrial septal vs. right atrial appendage pacing on atrial mechanical function and dyssynchrony in patients with sinus node dysfunction and paroxysmal atrial fibrillation. Europace 2011, 13, 1268–1274. [Google Scholar] [CrossRef]
- Laurent, G.; Eicher, J.C.; Mathe, A.; Bertaux, G.; Barthez, O.; Debin, R.; Billard, C.; Philip, J.L.; Wolf, J.E. Permanent left atrial pacing therapy may improve symptoms in heart failure patients with preserved ejection fraction and atrial dyssynchrony: A pilot study prior to a national clinical research programme. Eur. J. Heart Fail. 2013, 15, 85–93. [Google Scholar] [CrossRef]
- Prakash, A.; Saksena, S.; Ziegler, P.D.; Lokhandwala, T.; Hettrick, D.A.; Delfaut, P.; Nanda, N.C.; Wyse, D.G. Dual site right atrial pacing can improve the impact of standard dual chamber pacing on atrial and ventricular mechanical function in patients with symptomatic atrial fibrillation: Further observations from the dual site atrial pacing for prevention of atrial fibrillation trial. J. Interv. Card. Electrophysiol. 2005, 12, 177–187. [Google Scholar] [CrossRef]
- Dabrowska-Kugacka, A.; Lewicka-Nowak, E.; Ruciński, P.; Zagozdzon, P.; Raczak, G.; Kutarski, A. Atrial electromechanical sequence and contraction synchrony during single- and multisite atrial pacing in patients with brady-tachycardia syndrome. Pacing. Clin. Electrophysiol. 2009, 32, 591–603. [Google Scholar] [CrossRef]
- Habel, N.; Infeld, M.; Bernknopf, J.; Meyer, M.; Lustgarten, D. Rationale and design of the PACE HFpEF trial: Physiologic accelerated pacing as a holistic treatment of heart failure with preserved ejection fraction. Heart Rhythm. O2 2023, 5, 41–49. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| High A Low V a (n = 38) | High A High V b (n = 26) | Low A High V c (n = 23) | p | |
|---|---|---|---|---|
| Age, years | 73.6 ± 10.2 | 78.7 ± 8.3 | 73.7 ± 9.8 | 0.104 |
| Male, n (%) | 12 (31.7) | 11 (42.3) | 9 (39.1) | 0.658 |
| BSA, m2 | 1.89 ± 0.2 | 1.91 ± 0.22 | 1.98 ± 0.23 | 0.472 |
| BMI, kg/m2 | 28.4 ± 4.2 | 29.0 ± 5.8 | 30.3 ± 5.8 | 0.494 |
| Medical history | ||||
| Hypertension, n (%) | 35 (92.1) | 24 (92.3) | 21 (91.3) | 0.991 |
| Diabetes mellitus, n (%) | 3 (7.9) | 5 (19.2) | 4 (17.4) | 0.366 |
| PAF, n (%) | 15 (39.4) | 10 (38.5) | 8 (34.8) | 0.933 |
| CAD, n (%) | 14 (36.8) | 8 (30.8) | 8 (34.8) | 0.881 |
| Chronic renal failure, n (%) | 2 (5.2) | 3 (11.5) | 1 (4.3) | 0.532 |
| Medications | ||||
| ACE inhibitors/ARB, n (%) | 36 (94.7) | 24 (92.3) | 21 (91.3) | 0.861 |
| BAB, n (%) | 29 (76.3) | 20 (76.9) | 18 (78.2) | 0.985 |
| MRA, n (%) | 10 (26.3) | 6 (23.1) | 6 (26.1) | 0.953 |
| non-MRA diuretic, n (%) | 17 (44.7) | 13 (50.0) | 10 (43.4) | 0.882 |
| Non-dihydropyridine CCB, n (%) | 1 (2.6) | 0 (0) | 0 (0) | 0.521 |
| Statin, n (%) | 12 (31.6) | 10 (38.5) | 9 (39.1) | 0.784 |
| LV parameters | ||||
| LVEDD, mm | 49.2 ± 4.5 | 49.8 ± 5.1 | 51.2 ± 5.7 | 0.360 |
| LVEDD index, mL/m2 | 26.2 ± 2.2 | 26.4 ± 2.6 | 25.6 ± 2.9 | 0.867 |
| LV EF, % | 58.4 ± 4.9 | 58.9 ± 5.0 | 57.6 ± 5.2 | 0.768 |
| E/A | 0.89 ± 0.37 | 0.84 ± 0.43 | 0.85 ± 0.41 | 0.856 |
| E/e′ | 8.4 ± 2.6 | 10.4 ± 4.5 | 9.8 ± 4.0 | 0.547 |
| High A Low V a (n = 38) | High A High V b (n = 26) | Low A High V c (n = 23) | p | |
|---|---|---|---|---|
| Volumes | ||||
| LAmax, mL | 73.2 ± 17.3 | 77.8 ± 24.2 | 76.1 ± 26.1 | 0.684 |
| LAmax index, mL/m2 | 38.7 ± 7.9 | 40.6 ± 10.8 | 37.8 ± 10.5 | 0.558 |
| LAp, mL | 53.7 ± 14.3 | 53.4 ± 19.3 | 55.1 ± 18.5 | 0.939 |
| LAp index, mL/m2 | 28.3 ± 6.8 | 27.8 ± 8.9 | 27.5 ± 7.6 | 0.914 |
| LAmin, mL | 38.2 ± 11.8 | 40.3 ± 16.7 | 42.2 ± 15.1 | 0.592 |
| LAmin index, mL/m2 | 20.2 ± 5.9 | 20.9 ± 7.7 | 21.0 ± 6.4 | 0.861 |
| Emptying fractions | ||||
| Total, % | 48.1 ± 8.2 | 47.3 ± 9.0 | 44.4 ± 7.8 | 0.133 |
| Passive, % | 26.7 ± 8.2 | 28.8 ± 9.1 | 27.2 ± 8.4 | 0.634 |
| Active, % | 29.2 ± 8.7 | 25.8 ± 10.4 | 23.7 ± 5.8 | 0.450 |
| Strains | ||||
| Reservoir, % | 25.9 ± 10.3 | 20.3 ± 8.9 | 21.4 ± 10.4 | 0.054 |
| Conduit, % | −11.9 ± 5.3 | −8.8 ± 4.3 | −10.4 ± 8.1 | 0.090 |
| Contractile, % | −14.0 ± 9.0 | −11.4 ± 8.5 | −10.9 ± 8.6 | 0.345 |
| Stiffness index | 0.41 ± 0.27 | 0.72 ± 0.67 | 0.62 ± 0.58 | 0.040 |
| Baseline | 1 Month | 3 Months | p Baseline vs. 1 Month | p Baseline vs. 3 Months | |
|---|---|---|---|---|---|
| Volumes | |||||
| LAmax, mL | 73.2 ± 17.3 | 77.8 ± 21.1 | 75.8 ± 20.1 | 0.442 | 0.367 |
| LAmax index, mL/m2 | 38.7 ± 7.9 | 41.0 ± 10.4 | 40.1 ± 10.0 | 0.424 | 0.376 |
| LAp, mL | 53.7 ± 14.3 | 55.5 ± 16.2 | 57.3 ± 17.5 | 0.294 | 0.161 |
| LAp index, mL/m2 | 28.3 ± 6.8 | 29.3 ± 8.2 | 30.2 ± 8.4 | 0.261 | 0.186 |
| LAmin, mL | 38.2 ± 11.8 | 41.3 ± 14.6 | 42.7 ± 13.7 | 0.169 | 0.038 |
| LAmin index, mL/m2 | 20.2 ± 5.9 | 21.7 ± 7.3 | 22.6 ± 7.5 | 0.190 | 0.039 |
| Emptying fractions | |||||
| Total, % | 48.1 ± 8.2 | 47.6 ± 8.6 | 44.9 ± 9.8 | 0.678 | 0.033 |
| Passive, % | 26.7 ± 8.2 | 28.6 ± 9.4 | 24.5 ± 9.7 | 0.398 | 0.401 |
| Active, % | 29.2 ± 8.7 | 26.5 ± 8.5 | 25.7 ± 8.9 | 0.076 | 0.043 |
| Strains | |||||
| Reservoir, % | 25.9 ± 10.3 | 24.4 ± 9.5 | 21.1 ± 9.9 | 0.315 | 0.003 |
| Conduit, % | −11.9 ± 5.3 | −11.8 ± 6.4 | −10.0 ± 5.3 | 0.798 | 0.086 |
| Contractile, % | −14.0 ± 9.0 | −12.7 ± 7.0 | −11.1 ± 7.8 | 0.342 | 0.018 |
| Stiffness index | 0.41 ± 0.27 | 0.46 ± 0.33 | 0.67 ± 0.65 | 0.478 | 0.001 |
| Mitral inflow | |||||
| E/A | 0.89 ± 0.37 | 1.02 ± 0.44 | 0.99 ± 0.43 | 0.008 | 0.043 |
| E/e′ | 8.4 ± 2.6 | 9.2 ± 4.5 | 9.0 ± 4.0 | 0.598 | 0.914 |
| Baseline | 1 Month | 3 Months | p Baseline vs. 1 Month | p Baseline vs. 3 Months | |
|---|---|---|---|---|---|
| Volumes | |||||
| LAmax, mL | 77.8 ± 24.2 | 85.5 ± 24.1 | 87.4 ± 19.6 | 0.012 | 0.085 |
| LAmax index, mL/m2 | 40.6 ± 10.8 | 44.5 ± 10.3 | 45.4 ± 10.2 | 0.015 | 0.073 |
| LAp, mL | 53.4 ± 19.3 | 61.6 ± 18.2 | 62.5 ± 19.6 | 0.001 | 0.086 |
| LAp index, mL/m2 | 27.8 ± 8.9 | 32.1 ± 8.1 | 32.1 ± 8.4 | 0.001 | 0.052 |
| LAmin, mL | 40.3 ± 16.7 | 43.6 ± 15.9 | 45.8 ± 15.8 | 0.047 | 0.224 |
| LAmin index, mL/m2 | 20.9 ± 7.7 | 22.7 ± 7.5 | 23.3 ± 8.0 | 0.032 | 0.224 |
| Emptying fractions | |||||
| Total, % | 47.3 ± 9.0 | 49.8 ± 8.7 | 48.3 ± 9.5 | 0.482 | 0.964 |
| Passive, % | 28.8 ± 9.1 | 27.9 ± 8.4 | 28.6 ± 9.7 | 0.634 | 0.914 |
| Active, % | 25.8 ± 10.4 | 27.4 ± 9.4 | 27.6 ± 7.8 | 0.631 | 0.573 |
| Strains | |||||
| Reservoir, % | 20.3 ± 8.9 | 18.9 ± 7.9 | 18.7 ± 8.3 | 0.112 | 0.231 |
| Conduit, % | −8.8 ± 4.3 | −8.5 ± 4.6 | −8.4 ± 5.3 | 0.513 | 0.738 |
| Contractile, % | −11.4 ± 8.5 | −10.3 ± 7.8 | −10.0 ± 7.5 | 0.385 | 0.988 |
| Stiffness index | 0.72 ± 0.67 | 0.79 ± 0.63 | 0.90 ± 0.89 | 0.096 | 0.340 |
| Mitral inflow | |||||
| E/A | 0.84 ± 0.43 | 1.02 ± 0.41 | 1.05 ± 0.46 | 0.021 | 0.365 |
| E/e′ | 10.4 ± 4.5 | 10.6 ± 4.8 | 11.5 ± 4.7 | 0.864 | 0.512 |
| Baseline | 1 Month | 3 Months | p Baseline vs. 1 Month | p Baseline vs. 3 Months | |
|---|---|---|---|---|---|
| Volumes | |||||
| LAmax, mL | 76.1 ± 26.1 | 85.1 ± 25.3 | 88.1 ± 28.3 | 0.022 | 0.030 |
| LAmax index, mL/m2 | 37.8 ± 10.5 | 45.0 ± 11.1 | 43.2 ± 11.7 | 0.016 | 0.027 |
| LAp, mL | 55.1 ± 18.5 | 61.9 ± 15.9 | 62.1 ± 20.8 | 0.117 | 0.397 |
| LAp index, mL/m2 | 27.5 ± 7.6 | 31.1 ± 7.5 | 30.6 ± 8.6 | 0.091 | 0.433 |
| LAmin, mL | 42.2 ± 15.1 | 46.2 ± 13.8 | 45.0 ± 19.0 | 0.268 | 0.925 |
| LAmin index, mL/m2 | 21.0 ± 6.4 | 23.2 ± 6.8 | 22.1 ± 7.9 | 0.251 | 0.875 |
| Emptying fractions | |||||
| Total, % | 44.4 ± 7.8 | 48.3 ± 10.1 | 49.0 ± 6.1 | 0.117 | 0.064 |
| Passive, % | 27.2 ± 8.4 | 30.3 ± 9.8 | 28.5 ± 7.3 | 0.136 | 0.778 |
| Active, % | 23.7 ± 5.8 | 25.7 ± 10.3 | 28.1 ± 9.7 | 0.573 | 0.331 |
| Strains | |||||
| Reservoir, % | 21.4 ± 10.4 | 24.3 ± 11.8 | 22.5 ± 10.4 | 0.287 | 0.975 |
| Conduit strain, % | −10.4 ± 8.1 | −11.3 ± 6.8 | −11.0 ± 6.6 | 0.124 | 0.638 |
| Contractile strain, % | −10.9 ± 8.6 | −13.0 ± 10.1 | −11.5 ± 7.1 | 0.653 | 0.683 |
| Stiffness index | 0.62 ± 0.58 | 0.56 ± 0.25 | 0.73 ± 0.54 | 0.776 | 0.937 |
| Mitral inflow | |||||
| E/A | 0.85 ± 0.41 | 0.92 ± 0.43 | 0.98 ± 0.47 | 0.861 | 0.287 |
| E/e′ | 9.8 ± 4.0 | 10.2 ± 4.5 | 10.6 ± 4.2 | 0.798 | 0.913 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Viezelis, M.; Neverauskaite-Piliponiene, G.; Marcinkeviciene, A.; Kazakevicius, T.; Zabiela, V.; Kviesulaitis, V.; Jurkevicius, R.; Puodziukynas, A. Atrial Pacing Negatively Affects Left Atrial Morphological and Functional Parameters Similarly to Atrioventricular Dyssynchrony. Medicina 2024, 60, 503. https://doi.org/10.3390/medicina60030503
Viezelis M, Neverauskaite-Piliponiene G, Marcinkeviciene A, Kazakevicius T, Zabiela V, Kviesulaitis V, Jurkevicius R, Puodziukynas A. Atrial Pacing Negatively Affects Left Atrial Morphological and Functional Parameters Similarly to Atrioventricular Dyssynchrony. Medicina. 2024; 60(3):503. https://doi.org/10.3390/medicina60030503
Chicago/Turabian StyleViezelis, Mindaugas, Gintare Neverauskaite-Piliponiene, Agne Marcinkeviciene, Tomas Kazakevicius, Vytautas Zabiela, Vilius Kviesulaitis, Renaldas Jurkevicius, and Aras Puodziukynas. 2024. "Atrial Pacing Negatively Affects Left Atrial Morphological and Functional Parameters Similarly to Atrioventricular Dyssynchrony" Medicina 60, no. 3: 503. https://doi.org/10.3390/medicina60030503