
Echocardiographic Myocardial Work: A Novel Method to Assess Left Ventricular Function in Patients with Coronary Artery Disease and Diabetes Mellitus
 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Principles of Myocardial Work
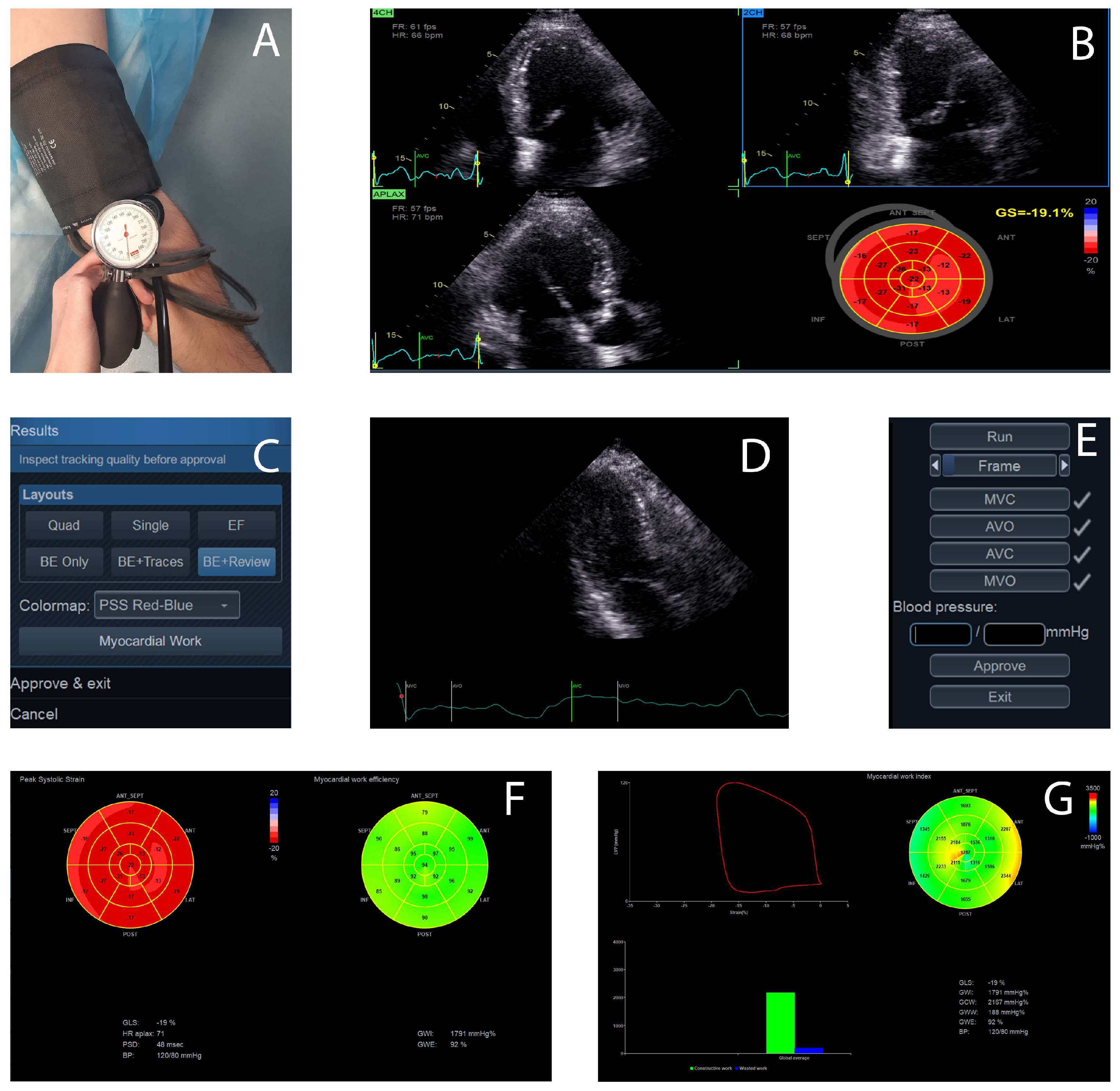
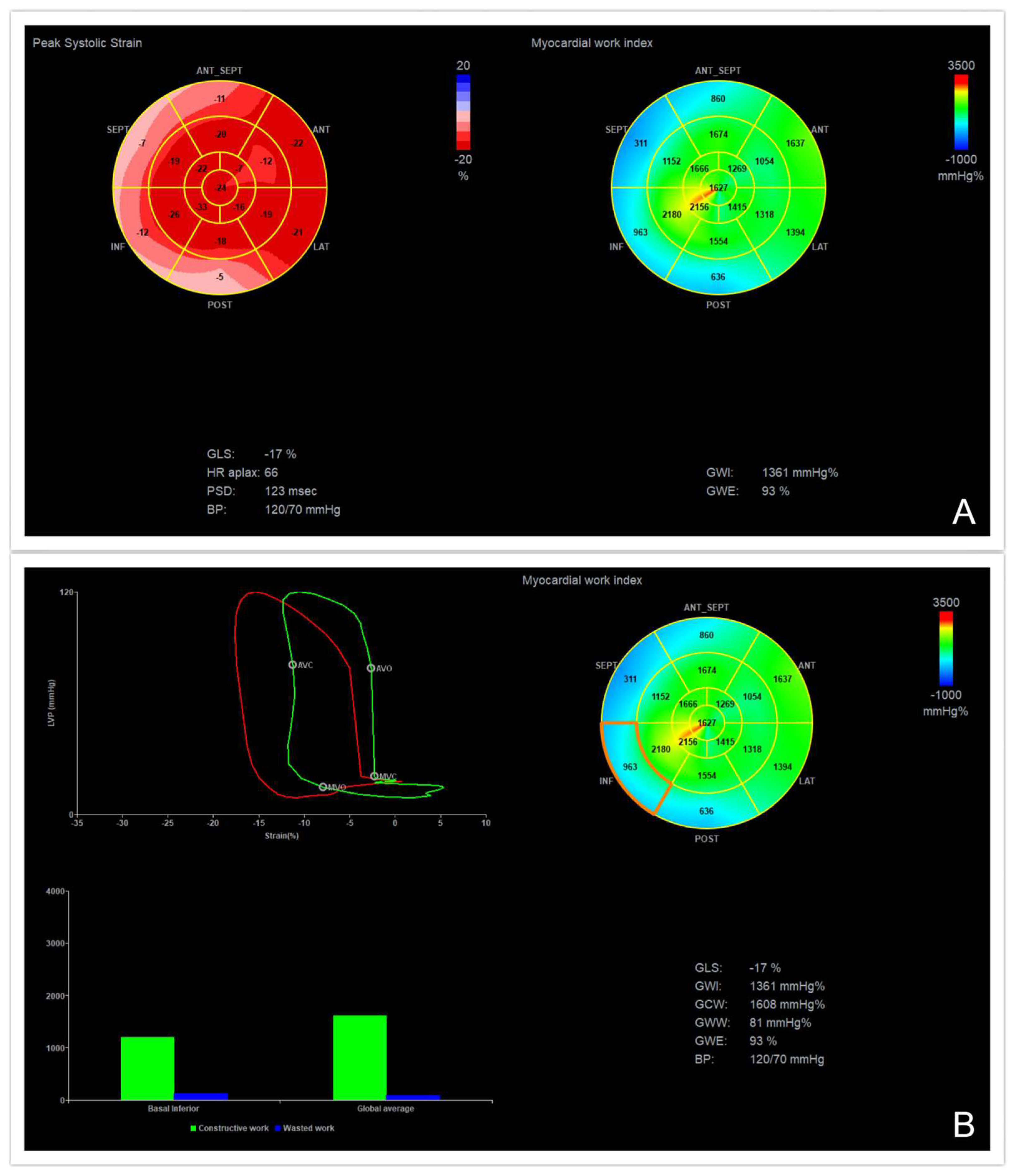
3. Practical Assessment of Myocardial Work
4. Normal Ranges of Myocardial Work Parameters
5. Myocardial Work in Coronary Artery Disease
5.1. Chronic Coronary Syndromes
5.2. Acute Coronary Syndromes
5.2.1. Non-ST-Segment Elevation Myocardial Infarction
5.2.2. ST-Segment Elevation Myocardial Infarction
6. Diabetes Mellitus
7. Other Clinical Implications of Myocardial Work
8. Limitations of the Method and Future Directions
9. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ralapanawa, U.; Sivakanesan, R. Epidemiology and the magnitude of coronary artery disease and acute coronary syndrome: A narrative review. J. Epidemiol. Glob. Health 2021, 11, 169–177. [Google Scholar] [CrossRef]
- Kenny, H.C.; Abel, E.D. Heart Failure in Type 2 Diabetes Mellitus. Circ. Res. 2019, 124, 121–141. [Google Scholar] [CrossRef]
- Bastos, M.B.; Burkhoff, D.; Maly, J.; Daemen, J.; den Uil, C.A.; Ameloot, K.; Lenzen, M.; Mahfoud, F.; Zijlstra, F.; Schreuder, J.J.; et al. Invasive left ventricle pressure-volume analysis: Overview and practical clinical implications. Eur. Heart J. 2020, 41, 1286–1297. [Google Scholar] [CrossRef]
- Abawi, D.; Rinaldi, T.; Faragli, A.; Pieske, B.; Morris, D.A.; Kelle, S.; Tschöpe, C.; Zito, C.; Alogna, A. The non-invasive assessment of myocardial work by pressure-strain analysis: Clinical applications. Heart Fail. Rev. 2022, 27, 1261–1279. [Google Scholar] [CrossRef]
- Russell, K.; Eriksen, M.; Aaberge, L.; Wilhelmsen, N.; Skulstad, H.; Remme, E.W.; Haugaa, K.H.; Opdahl, A.; Fjeld, J.G.; Gjesdal, O.; et al. A novel clinical method for quantification of regional left ventricular pressure-strain loop area: A non-invasive index of myocardial work. Eur. Heart J. 2012, 33, 724–733. [Google Scholar] [CrossRef]
- Delhaas, T.; Arts, T.; Prinzen, F.W.; Reneman, R.S. Regional fibre stress-fibre strain area as an estimate of regional blood flow and oxygen demand in the canine heart. J. Physiol. 1994, 477, 481–496. [Google Scholar] [CrossRef]
- Moya, A.; Buytaert, D.; Penicka, M.; Bartunek, J.; Vanderheyden, M. State-of-the-Art: Noninvasive Assessment of Left Ventricular Function Through Myocardial Work. J. Am. Soc. Echocardiogr. 2023, 36, 1027–1042. [Google Scholar] [CrossRef]
- Marzlin, N.; Hays, A.G.; Peters, M.; Kaminski, A.; Roemer, S.; O’Leary, P.; Kroboth, S.; Harland, D.R.; Khandheria, B.K.; Tajik, A.J.; et al. Myocardial Work in Echocardiography. Circ. Cardiovasc. Imaging 2023, 16, e014419. [Google Scholar] [CrossRef] [PubMed]
- Smiseth, O.A.; Donal, E.; Penicka, M.; Sletten, O.J. How to measure left ventricular myocardial work by pressure–strain loops. Eur. Heart J. Cardiovasc. Imaging 2021, 22, 259–461. [Google Scholar] [CrossRef]
- Samset, E. Evaluation of Segmental Myocardial Work in the Left Ventricle. 2017. Available online: https://www.gehealthcare.com/-/media/8cab29682ace4ed7841505f813001e33.pdf (accessed on 17 October 2023).
- Ilardi, F.; D’Andrea, A.; D’Ascenzi, F.; Bandera, F.; Benfari, G.; Esposito, R.; Malagoli, A.; Mandoli, G.E.; Santoro, C.; Russo, V.; et al. Myocardial Work by Echocardiography: Principles and Applications in Clinical Practice. J. Clin. Med. 2021, 10, 4521. [Google Scholar] [CrossRef]
- Papadopoulos, K.; Ozden, T.O.; Mitrousi, K.; Ikonimidis, I. Myocardial work: Methodology and clinical applications. Diagnostics 2021, 11, 573. [Google Scholar] [CrossRef]
- Manganaro, R.; Marchetta, S.; Dulgheru, R.; Ilardi, F.; Sugimoto, T.; Robinet, S.; Cimino, S.; Go, Y.Y.; Bernard, A.; Kacharava, G.; et al. Echocardiographic reference ranges for normal non-invasive myocardial work indices: Results from the EACVI NORRE study. Eur. Heart J. Cardiovasc. Imaging 2019, 20, 582–590. [Google Scholar] [CrossRef]
- Morbach, C.; Sahiti, F.; Tiffe, T.; Cejka, V.; Eichner, F.A.; Gelbrich, G.; Heuschmann, P.U.; Störk, S.; STAAB Consortium. Myocardial work–correlation patterns and reference values from the population-based STAAB cohort study. PLoS ONE 2020, 15, 0239684. [Google Scholar] [CrossRef]
- Galli, E.; John-Matthwes, B.; Rousseau, C.; Schnell, F.; Leclercq, C.; Donal, E. Echocardiographic reference ranges for myocardial work in healthy subjects: A preliminary study. Echocardiography 2019, 36, 1814–1824. [Google Scholar] [CrossRef]
- Olsen, F.J.; Skaarup, K.G.; Lassen, M.C.H.; Johansen, N.D.; Sengeløv, M.; Jensen, G.B.; Schnohr, P.; Marott, J.L.; Søgaard, P.; Gislason, G.; et al. Normal Values for Myocardial Work Indices Derived from Pressure-Strain Loop Analyses: From the CCHS. Circ. Cardiovasc. Imaging 2022, 15, e013712. [Google Scholar] [CrossRef]
- Skaarup, K.G.; Lassen, M.C.H.; Johansen, N.D.; Olsen, F.J.; Lind, J.N.; Jørgensen, P.G.; Jensen, G.; Schnohr, P.; Prescott, E.; Søgaard, P.; et al. Age- and sex-based normal values of layer-specific longitudinal and circumferential strain by speckle tracking echocardiography: The Copenhagen City Heart Study. Eur. Heart J. Cardiovasc. Imaging 2022, 23, 629–640. [Google Scholar] [CrossRef]
- Lindstrom, M.; DeCleene, N.; Dorsey, H.; Fuster, V.; Johnson, C.O.; LeGrand, K.E.; Mensah, G.A.; Razo, C.; Stark, B.; Varieur, T.J.; et al. Global Burden of Cardiovascular Diseases and Risks Collaboration, 1990–2021. J. Am. Coll. Cardiol. 2022, 80, 2372–2425. [Google Scholar] [CrossRef]
- World Heart Report 2023: Confronting the World’s Number One Killer; World Heart Federation: Geneva, Switzerland, 2023.
- Shahjehan, R.D.; Bhutta, B.S. Coronary Artery Disease; StatPearls: Treasure Island, FL, USA, 2023. [Google Scholar]
- Choi, J.O.; Cho, S.W.; Song, Y.B.; Cho, S.J.; Song, B.G.; Lee, S.C.; Park, S.W. Longitudinal 2D strain at rest predicts the presence of left main and three vessel coronary artery disease in patients without regional wall motion abnormality. Eur. J. Echocardiogr. 2009, 10, 695–701. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Wang, H.; Feng, H.; Wu, T.; Yang, Y.; Gao, D.; Sun, L. Afterload-related reference values for myocardial work indices. Cardiovasc. Ultrasound 2021, 24, 24. [Google Scholar] [CrossRef] [PubMed]
- Edwards, N.F.A.; Scalia, G.M.; Shiino, K.; Sabapathy, S.; Anderson, B.; Chamberlain, R.; Khandheria, B.K.; Chan, J. Global myocardial work is superior to global longitudinal strain to predict significant coronary artery disease in patients with normal left ventricular function and wall motion. J. Am. Soc. Echocardiogr. 2019, 32, 947–957. [Google Scholar] [CrossRef] [PubMed]
- Sabatino, J.; De Rosa, S.; Leo, I.; Strangio, A.; Spaccarotella, C.; Polimeni, A.; Sorrentino, S.; Di Salvo, G.; Indolfi, C. Prediction of Significant Coronary Artery Disease Through Advanced Echocardiography: Role of Non-invasive Myocardial Work. Front. Cardiovasc. Med. 2021, 24, 719603. [Google Scholar] [CrossRef]
- Zhang, J.; Liu, Y.; Deng, Y.; Zhu, Y.; Sun, R.; Lu, S. Non-invasive Global and Regional Myocardial Work Predicts High-Risk Stable Coronary Artery Disease Patients with Normal Segmental Wall Motion and Left Ventricular Function. Front. Cardiovasc. Med. 2021, 28, 711547. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.; Guo, Y.; Wang, X.; Yang, C.; Li, Y.; Meng, X.; Pei, Z.; Zhang, R.; Zhong, Y.; Wang, F. Myocardial Work by Speckle Tracking Echocardiography Accurately Assesses Left Ventricular Function of Coronary Artery Disease Patients. Front. Cardiovasc. Med. 2021, 5, 727389. [Google Scholar] [CrossRef] [PubMed]
- Pan, J.C.; Lyu, L.J.; Liu, Q.D.; Yang, W.; Li, X.H.; Han, Y.M.; Sun, J.Y.; Dong, M.; Zhang, P.F.; Zhang, M. Association between resting myocardial work indices and stress myocardial perfusion in patients with angina and non-obstructive coronary artery disease. Quant. Imaging Med. Surg. 2023, 13, 4563–4577. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Xu, Y.; Zhou, B.; Zhao, C.; Ma, C.; Wei, C.; Hu, S.; Zou, C. Comparison of Application Value of Global Longitudinal Strain and Myocardial Work in Predicting Severe Coronary Artery Stenosis by Echocardiography. Authorea, 2023; preprint. [Google Scholar] [CrossRef]
- Collet, J.P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef] [PubMed]
- Bauer, D.; Toušek, P. Risk Stratification of Patients with Acute Coronary Syndrome. J. Clin. Med. 2021, 10, 4574. [Google Scholar] [CrossRef] [PubMed]
- Byrne, R.A.; Rossello, X.; Coughlan, J.J.; Barbato, E.; Berry, C.; Chieffo, A.; Claeys, M.J.; Dan, G.A.; Dweck, M.R.; Galbraith, M.; et al. 2023 ESC Guidelines for the management of acute coronary syndromes. Eur. Heart J. Acute Cardiovasc. Care 2023, 22, zuad107. [Google Scholar] [CrossRef] [PubMed]
- Ren, F.; Xue, T.; Tang, G.; Zhang, M.; Zhao, J.; Chen, Y.; Fan, J.; Yu, M.; Zhang, J. Assessment of Myocardial Work of the Left Ventricle before and after PCI in Patients with Non-ST-Segment Elevation Acute Coronary Syndrome by Pressure-Strain Loop Technology. Comput. Math. Methods Med. 2022, 2022, 8026689. [Google Scholar] [CrossRef]
- Qin, Y.; Wu, X.; Wang, J.; Li, Y.; Ding, X.; Guo, D.; Jiang, Z.; Zhu, W.; Cai, Q.; Lu, X. Value of territorial work efficiency estimation in non-ST-segment-elevation acute coronary syndrome: A study with non-invasive left ventricular pressure-strain loops. Int. J. Cardiovasc. Imaging 2021, 37, 1255–1265. [Google Scholar] [CrossRef]
- Roleder, T.; Smolka, G.; Pysz, P.; Kozyra, A.; Ochała, A. Non-ST elevation myocardial infarction related to total coronary artery occlusion—Prevalence and patient characteristics. Postep. Kardiol. Interwencyjnej 2015, 11, 9–13. [Google Scholar] [CrossRef]
- Boe, E.; Russell, K.; Eek, C.; Eriksen, M.; Remme, E.W.; Smiseth, O.A.; Skulstad, H. Non-invasive myocardial work index identifies acute coronary occlusion in patients with non-ST-segment elevation-acute coronary syndrome. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 1247–1255. [Google Scholar] [CrossRef] [PubMed]
- Butcher, S.C.; Lustosa, R.P.; Abou, R.; Marsan, N.A.; Bax, J.J.; Delgado, V. Prognostic implications of left ventricular myocardial work index in patients with ST-segment elevation myocardial infarction and reduced left ventricular ejection fraction. Eur. Heart J. Cardiovasc. Imaging 2022, 23, 699–707. [Google Scholar] [CrossRef] [PubMed]
- Meimoun, P.; Abdani, S.; Stracchi, V.; Elmkies, F.; Boulanger, J.; Botoro, T.; Zemir, H.; Clerc, J. Usefulness of Noninvasive Myocardial Work to Predict Left Ventricular Recovery and Acute Complications after Acute Anterior Myocardial Infarction Treated by Percutaneous Coronary Intervention. J. Am. Soc. Echocardiogr. 2020, 33, 1180–1190. [Google Scholar] [CrossRef]
- El Mahdiui, M.; van der Bijl, P.; Abou, R.; Ajmone Marsan, N.; Delgado, V.; Bax, J.J. Global Left Ventricular Myocardial Work Efficiency in Healthy Individuals and Patients with Cardiovascular Disease. J. Am. Soc. Echocardiogr. 2019, 32, 1120–1127. [Google Scholar] [CrossRef]
- Lustosa, R.P.; Butcher, S.C.; van der Bijl, P.; El Mahdiui, M.; Montero-Cabezas, J.M.; Kostyukevich, M.V.; Rocha De Lorenzo, A.; Knuuti, J.; Ajmone, M.N.; Bax, J.J.; et al. Global Left Ventricular Myocardial Work Efficiency and Long-Term Prognosis in Patients After ST-Segment-Elevation Myocardial Infarction. Circ. Cardiovasc. Imaging 2021, 14, e012072. [Google Scholar] [CrossRef] [PubMed]
- Coisne, A.; Fourdinier, V.; Lemesle, G.; Delsart, P.; Aghezzaf, S.; Lamblin, N.; Schurtz, G.; Verdier, B.; Ninni, S.; Delobelle, A.; et al. Clinical significance of myocardial work parameters after acute myocardial infarction. Eur. Heart J. Open 2022, 2, oeac037. [Google Scholar] [CrossRef] [PubMed]
- Kramer, D.G.; Trikalinos, T.A.; Kent, D.M.; Antonopoulos, G.V.; Konstam, M.A.; Udelson, J.E. Quantitative evaluation of drug or device effects on ventricular remodeling as predictors of therapeutic effects on mortality in patients with heart failure and reduced ejection fraction: A meta-analytic approach. J. Am. Coll. Cardiol. 2010, 56, 392–406. [Google Scholar] [CrossRef] [PubMed]
- Lustosa, R.P.; van der Bijl, P.; El Mahdiui, M.; Montero-Cabezas, J.M.; Kostyukevich, M.V.; Ajmone, M.N.; Bax, J.J.; Delgado, V. Noninvasive Myocardial Work Indices 3 Months after ST-Segment Elevation Myocardial Infarction: Prevalence and Characteristics of Patients with Postinfarction Cardiac Remodeling. J. Am. Soc. Echocardiogr. 2020, 33, 1172–1179. [Google Scholar] [CrossRef]
- Lustosa, R.P.; Fortuni, F.; van der Bijl, P.; Mahdiui, M.E.; Montero-Cabezas, J.M.; Kostyukevich, M.V.; Knuuti, J.; Marsan, N.A.; Delgado, V.; Bax, J.J. Changes in Global Left Ventricular Myocardial Work Indices and Stunning Detection 3 Months After ST-Segment Elevation Myocardial Infarction. Am. J. Cardiol. 2021, 157, 15–21. [Google Scholar] [CrossRef]
- Jin, W.; Wang, L.; Zhu, T.; Ma, Y.; Yu, C.; Zhang, F. Usefulness of echocardiographic myocardial work in evaluating the microvascular perfusion in STEMI patients after revascularization. BMC Cardiovasc. Disord. 2022, 22, 218. [Google Scholar] [CrossRef]
- Parlavecchio, A.; Vetta, G.; Caminiti, R.; Ajello, M.; Magnocavallo, M.; Vetta, F.; Foti, R.; Crea, P.; Micari, A.; Carerj, S.; et al. Which is the best Myocardial Work index for the prediction of coronary artery disease? A data meta-analysis. Echocardiography 2023, 40, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Guha, K.; McDonagh, T. Heart failure epidemiology: European perspective. Curr. Cardiol. Rev. 2013, 9, 123–127. [Google Scholar] [CrossRef] [PubMed]
- Sarma, S.; Mentz, R.J.; Kwasny, M.J.; Fought, A.J.; Huffman, M.; Subacius, H.; Nodari, S.; Konstam, M.; Swedberg, K.; Maggioni, A.P.; et al. Association between diabetes mellitus and post-discharge outcomes in patients hospitalized with heart failure: Findings from the EVEREST trial. Eur. J. Heart Fail. 2013, 15, 194–202. [Google Scholar] [CrossRef]
- Dei Cas, A.; Khan, S.S.; Butler, J.; Mentz, R.J.; Bonow, R.O.; Avogaro, A.; Tschoepe, D.; Doehner, W.; Greene, S.J.; Senni, M.; et al. Impact of diabetes on epidemiology, treatment, and outcomes of patients with heart failure. JACC Heart Fail. 2015, 3, 136–145. [Google Scholar] [CrossRef] [PubMed]
- Liao, L.; Shi, B.; Ding, Z.; Chen, L.; Dong, F.; Li, J.; Zhong, Y.; Xu, J. Echocardiographic study of myocardial work in patients with type 2 diabetes mellitus. BMC Cardiovasc. Disord. 2022, 22, 59. [Google Scholar] [CrossRef] [PubMed]
- Huang, D.; Cui, C.; Zheng, Q.; Li, Y.; Liu, Y.; Hu, Y.; Wang, Y.; Liu, R.; Liu, L. Quantitative Analysis of Myocardial Work by Non-invasive Left Ventricular Pressure-Strain Loop in Patients with Type 2 Diabetes Mellitus. Front. Cardiovasc. Med. 2021, 8, 733339. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Li, L.; Huang, J.; Fan, L. Assessment of subclinical left ventricle myocardial dysfunction using global myocardial work in type 2 diabetes mellitus patients with preserved left ventricle ejection fraction. Diabetol. Metab. Syndr. 2022, 14, 17. [Google Scholar] [CrossRef] [PubMed]
- Klaeboe, L.G.; Edvardsen, T. Echocardiographic assessment of left ventricular systolic function. J. Echocardiogr. 2019, 17, 10–16. [Google Scholar] [CrossRef]
- Tadic, M.; Cuspidi, C.; Pencic, B.; Grassi, G.; Celic, V. Myocardial work in hypertensive patients with and without diabetes: An echocardiographic study. J. Clin. Hypertens 2020, 22, 2121–2127. [Google Scholar] [CrossRef]
- Jankowski, P.; Bilo, G.; Kawecka-Jaszcz, K. The pulsatile component of blood pressure: Its role in the pathogenesis of atherosclerosis. Blood Press. 2007, 16, 238–245. [Google Scholar] [CrossRef]
- Prenner, S.B.; Chirinos, J.A. Arterial stiffness in diabetes mellitus. Atherosclerosis 2015, 238, 370–379. [Google Scholar] [CrossRef] [PubMed]
- Cao, W.; Deng, Y.; Lv, L.; Liu, X.; Luo, A.; Yin, L.; Li, Z. Assessment of left ventricular function in patients with type 2 diabetes mellitus by non-invasive myocardial work. Front. Endocrinol. 2023, 14, 1241307. [Google Scholar] [CrossRef] [PubMed]
- Ikonomidis, I.; Pavlidis, G.; Thymis, J.; Birba, D.; Kalogeris, A.; Kousathana, F.; Kountouri, A.; Balampanis, K.; Parissis, J.; Andreadou, I.; et al. Effects of glucagon-like peptide-1 receptor agonists, sodium-glucose cotransporter-2 inhibitors, and their combination on endothelial glycocalyx, arterial function, and myocardial work index in patients with type 2 diabetes mellitus after 12-month treatment. J. Am. Heart Assoc. 2020, 9, e015716. [Google Scholar] [CrossRef] [PubMed]
- Lembo, M.; Santoro, C.; Casciano, O.; Capone, V.; Fedele, T.; Luciano, F.; Canonico, M.; Buonauro, A.; Esposito, R.; Galderisi, M. Impact of diastolic blood pressure on speckle tracking derived myocardial work components in a population of normotensive and untreated hypertensive patients. Eur. Heart J. 2020, 41, 2700. [Google Scholar] [CrossRef]
- Li, X.; Liu, Q.; Bao, W.; Li, M.; Zhang, Y.; Wan, X.; Zhang, M. Impact of blood pressure changes on myocardial work indices in hypertensive patients in a day. J. Clin. Hypertens 2022, 24, 3–14. [Google Scholar] [CrossRef]
- Jaglan, A.; Roemer, S.; Perez Moreno, A.C.; Khandheria, B.K. Myocardial work in Stage 1 and 2 hypertensive patients. Eur. Heart J. Cardiovasc. Imaging 2021, 22, 744–750. [Google Scholar] [CrossRef]
- Tadic, M.; Cuspidi, C.; Pencic, B.; Vukomanovic, V.; Taddei, S.; Grassi, G.; Celic, V. Association between myocardial work and functional capacity in patients with arterial hypertension: An echocardiographic study. Blood Press. 2021, 30, 188–195. [Google Scholar] [CrossRef]
- Loncaric, F.; Marciniak, M.; Nunno, L.; Mimbrero, M.; Fernandes, J.F.; Fabijanovic, D.; Sanchis, L.; Doltra, A.; Montserrat, S.; Cikes, M.; et al. Distribution of myocardial work in arterial hypertension: Insights from non-invasive left ventricular pressure-strain relations. Int. J. Cardiovasc. Imaging 2021, 37, 145–154. [Google Scholar] [CrossRef]
- Chan, J.; Edwards, N.F.A.; Khandheria, B.K.; Shiino, K.; Sabapathy, S.; Anderson, B.; Chamberlain, R.; Scalia, G.M. A new approach to assess myocardial work by non-invasive left ventricular pressure-strain relations in hypertension and dilated cardiomyopathy. Eur. Heart J. Cardiovasc. Imaging 2019, 20, 31–39. [Google Scholar] [CrossRef]
- Cui, C.; Li, Y.; Liu, Y.; Huang, D.; Hu, Y.; Wang, Y.; Ma, L.; Liu, L. Association between echocardiographic noninvasive myocardial work indices and myocardial fibrosis in patients with dilated cardiomyopathy. Front. Cardiovasc. Med. 2021, 8, 704251. [Google Scholar] [CrossRef]
- Fortuni, F.; Butcher, S.C.; van der Kley, F.; Lustosa, R.P.; Karalis, I.; de Weger, A.; Priori, S.G.; van der Bijl, P.; Bax, J.J.; Delgado, V.; et al. Left ventricular myocardial work in patients with severe aortic stenosis. J. Am. Soc. Echocardiogr. 2021, 34, 257–266. [Google Scholar] [CrossRef] [PubMed]
- Jain, R.; Bajwa, T.; Roemer, S.; Huisheree, H.; Allaqaband, S.Q.; Kroboth, S.; Perez Moreno, A.C.; Tajik, A.J.; Khandheria, B.K. Myocardial work assessment in severe aortic stenosis undergoing transcatheter aortic valve replacement. Eur. Heart J. Cardiovasc. Imaging 2021, 22, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Ilardi, F.; Postolache, A.; Dulgheru, R.; Marchetta, S.; Cicenia, M.; Lancellotti, P. Prognostic role of global work index in asymptomatic patients with aortic stenosis. Eur. Heart J. 2020, 41, 2020. [Google Scholar] [CrossRef]
- Calvillo-Arguelles, O.; Thampinathan, B.; Somerset, E.; Shalmon, T.; Amir, E.; Steve Fan, C.P.; Moon, S.; Abdel-Qadir, H.; Thevakumaran, Y.; Day, J.; et al. Diagnostic and prognostic value of myocardial work indices for identification of cancer therapy–related cardiotoxicity. JACC Cardiovasc. Imaging 2022, 15, 1361–1376. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.L.; Chan, Y.H.; Wu, V.C.; Lee, H.F.; Hsiao, F.C.; Chu, P.H. Incremental prognostic value of global myocardial work over ejection fraction and global longitudinal strain in patients with heart failure and reduced ejection fraction. Eur. Heart J. Cardiovasc. Imaging 2021, 22, 348–356. [Google Scholar] [CrossRef] [PubMed]
- Hedwig, F.; Soltani, S.; Stein, J.; Schoenrath, F.; Potapov, E.; Knosalla, C.; Falk, V.; Knebel, F.; Knierim, J. Global work index correlates with established prognostic parameters of heart failure. Echocardiography 2020, 37, 412–420. [Google Scholar] [CrossRef] [PubMed]
- Bouali, Y.; Donal, E.; Gallard, A.; Laurin, C.; Hubert, A.; Bidaut, A.; Leclercq, C.; Galli, E. Prognostic Usefulness of Myocardial Work in Patients with Heart Failure and Reduced Ejection Fraction Treated by Sacubitril/Valsartan. Am. J. Cardiol. 2020, 125, 1856–1862. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.; Qin, Y.; Ding, X.; Zhang, M.; Zhu, W.; Wang, J.; Leng, C.; Lu, X.; Cai, Q. Association between left ventricular geometry and global myocardial work in patients with heart failure with preserved ejection fraction: Assessment using strain-pressure loop. Int. J. Cardiovasc. Imaging 2023, 39, 319–329. [Google Scholar] [CrossRef]
- Zhu, M.; Wang, Y.; Cheng, Y.; Su, Y.; Chen, H.; Shu, X. The value of noninvasive myocardial work indices derived from left ventricular pressure-strain loops in predicting the response to cardiac resynchronization therapy. Quant. Imaging Med. Surg. 2021, 11, 1406–1420. [Google Scholar] [CrossRef]
- Galli, E.; Leclercq, C.; Fournet, M.; Hubert, A.; Bernard, A.; Smiseth, O.A.; Mabo, P.; Samset, E.; Hernandez, A.; Donal, E. Value of Myocardial Work Estimation in the Prediction of Response to Cardiac Resynchronization Therapy. J. Am. Soc. Echocardiogr. 2018, 31, 220–230. [Google Scholar] [CrossRef]
- Van der Bijl, P.; Vo, N.M.; Kostyukevich, M.V.; Mertens, B.; Ajmone Marsan, N.; Delgado, V.; Bax, J.J. Prognostic implications of global, left ventricular myocardial work efficiency before cardiac resynchronization therapy. Eur. Heart J. Cardiovasc. Imaging 2019, 20, 1388–1394. [Google Scholar] [CrossRef]
- Vecera, J.; Penicka, M.; Eriksen, M.; Russell, K.; Bartunek, J.; Vanderheyden, M.; Smiseth, O.A. Wasted septal work in left ventricular dyssynchrony: A novel principle to predict response to cardiac resynchronization therapy. Eur. Heart J. Cardiovasc. Imaging 2016, 17, 624–632. [Google Scholar] [CrossRef] [PubMed]
- Clemmensen, T.S.; Eiskjaer, H.; Mikkelsen, F.; Granstam, S.O.; Flachskampf, F.A.; Sørensen, J.; Poulsen, S.H. Left ventricular pressure-strain-derived myocardial work at rest and during exercise in patients with cardiac amyloidosis. J. Am. Soc. Echocardiogr. 2020, 33, 573–582. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.Z.; Wang, X.L.; Zhang, C.Q. Quantitative assessment of left ventricular myocardial work in chronic kidney disease patients by a novel non-invasive pressure-strain loop analysis method. Int. J. Cardiovasc. Imaging 2021, 37, 1567–1575. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.W.; Hsieh, W.T.; Huang, C.Y.; Huang, C.C.; Liang, H.Y.; Wang, G.J. Estimated left ventricular pressure-myocardial strain loop as an index of cardiac work predicts all-cause mortality in patients receiving regular hemodialysis. J. Diabetes Complicat. 2021, 35, 107890. [Google Scholar] [CrossRef] [PubMed]
- Zhong, X.F.; Chen, L.X.; Liu, L.X.; Peng, G.J.; Luo, S.Y.; Liu, D.S.; Xu, J.F.; Liu, Y.Y. Early detect left ventricular subclinical myocardial dysfunction in patients with systemic lupus erythematosus by a left ventricular pressure-strain loop. Lupus 2022, 31, 596–605. [Google Scholar] [CrossRef] [PubMed]
- Minhas, A.S.; Gilotra, N.A.; Goerlich, E.; Metkus, T.; Garibaldi, B.T.; Sharma, G.; Bavaro, N.; Phillip, S.; Michos, E.D.; Hays, A.G. Myocardial Work Efficiency, A Novel Measure of Myocardial Dysfunction, Is Reduced in COVID-19 Patients and Associated with In-Hospital Mortality. Front. Cardiovasc. Med. 2021, 8, 667721. [Google Scholar] [CrossRef] [PubMed]
- Sonaglioni, A.; Nicolosi, G.L.; Trevisan, R.; Lombardo, M.; Grasso, E.; Gensini, G.F.; Ambrosio, G. The influence of pectus excavatum on cardiac kinetics and function in otherwise healthy individuals: A systematic review. Int. J. Cardiol. 2023, 381, 135–144. [Google Scholar] [CrossRef]
- Dobrovie, M.; Bėzy, S.; Ünlü, S.; Chakraborty, B.; Petrescu, A.; Duchenne, J.; Beela, A.S.; Voigt, J.U. How does regional hypertrophy affect strain measurements with different speckle-tracking methods? J. Am. Soc. Echocardiogr. 2019, 32, 1444–1450. [Google Scholar] [CrossRef]
- Russell, K.; Eriksen, M.; Aaberge, L.; Wilhelmsen, N.; Skulstad, H.; Gjesdal, O.; Edvardsen, T.; Smiseth, O.A. Assessment of wasted myocardial work: A novel method to quantify energy loss due to uncoordinated left ventricular contractions. Am. J. Physiol. Heart Circ. Physiol. 2013, 305, 996–1003. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study | Age (Years) | Gender | GWI, mmHg% | GCW, mmHg% | GWW, mmHg% | GWE, % |
|---|---|---|---|---|---|---|
| EACVI NORRE study [13] * | 20–40 | Male | 1758 ± 270 | 2186 ± 240 | 99 (68–144.5) | 95 (93–97) |
| Female | 1800 ± 251 | 2109 ± 289 | 90 (48–145) | 95 (94–97) | ||
| 40–60 | Male | 1900 ± 317 | 2267 ± 327 | 89 ± (58–122.5) | 96 (95–97) | |
| Female | 2027 ± 341 | 2329 ± 365 | 76 (51–118) | 96 (95–97) | ||
| ≥60 | Male | 1866 ± 286 | 2226 ± 328 | 85 (49–129) | 96 (94–97) | |
| Female | 2002 ± 270 | 2338 ± 386 | 90 (48–145) | 95 (94–97) | ||
| STAAB [14] ** | ≤45 | Male | 2141 (2099–2183) | 2366 (2330–2402) | 73 (70–76) | 96 (96–96) |
| Female | 2206 (2168–2245) | |||||
| >45 | Male | 2187 (2149–2224) | 2457 (2428–2486) | - | - | |
| Female | 2252 (2220–2284) | |||||
| Galli et al. [15] * | ≤25 | Male | 1912 ± 217 | 2231 ± 217 | 93 (64–115) | 95 (95–97) |
| Female | 1923 ± 276 | 2172 ± 238 | 114 (69–154) | 95 (93–96) | ||
| 25–35 | Male | 1927 ± 255 | 2179 ± 200 | 72 (52–120) | 96 (94–97) | |
| Female | 1954 ± 109 | 2260 ± 267 | 93 (62–112) | 95 (94–96) | ||
| 35–45 | Male | 1832 ± 252 | 2184 ± 250 | 111 (63–149) | 94 (93–97) | |
| Female | 2190 ± 206 | 2367 ± 207 | 71 (50–96) | 97 (96–98) | ||
| ≥45 | Male | 1824 ± 196 | 2174 ± 145 | 81 (69–94) | 96 (95–96) | |
| Female | 2058 ± 275 | 2350 ± 306 | 92 (59–132) | 96 (94–97) | ||
| CCHS [16] * | 32–57 | Male | 2062 ± 269 | 2229 ± 275 | 60 (42–84) | 97 (96–98) |
| Female | 2155 ± 275 | 2283 ± 286 | 68 (49–93) | 97 (95–97) |
| PARAMETER | LAD | LCX |
|---|---|---|
| GLSR (%) | −18.6 | −16.9 |
| GWIR (mmHg%) | 1814 | 1771 |
| Myocardial Work Parameter | Value | Role |
|---|---|---|
| GWE | <86% | Independent association with all-cause mortality in patients with STEMI (HR 3.167 [95% CI, 1.679–5.927]; p < 0.001) [39]. |
| GWE | <91% | Independent association with higher risk for major events in patients after an acute myocardial infarction (HR 2.94 [95% CI, 1.36–6.35]; p < 0.041) [40]. |
| GWI | <750 mmHg% | Independent association with all-cause mortality in patients with STEMI (HR 3.85 [95% CI, 1.94–7.67]; p < 0.0001) [36]. |
| Myocardial Work Parameter | Cutt-Off Value | Sensitivity (%) | Specificity (%) | Role |
|---|---|---|---|---|
| GWE | 78% | 90.5 | 85.7 | To predict critical coronary artery stenosis [24] |
| GWE | 95% | 70 | 90 | To detect reduced global stress myocardial perfusion in patients with angina and non-obstructive coronary artery disease [27] |
| Regional GWE | 96% | 73 | 70 | To predict obstructive coronary artery stenosis [33] |
| GWI | 1145 mmHg% | 86.8 | 53.7 | To predict microvascular perfusion impairments in patients with STEMI [44] |
| GWI | 1810 mmHg% | 92 | 51 | To predict significant coronary artery disease [23] |
| GWI | 1808 mmHg% | 52.6 | 87.8 | To predict high-risk, stable coronary artery disease [25] |
| GCW | 2308 mmHg% | 80.7 | 64.9 | To predict high-risk, stable coronary artery disease [25] |
| Differences | Definition and measurement | GLS | Measures the percentage change in length of the myocardium along its longitudinal axis during the cardiac cycle and quantifies the deformation of the myocardium |
| MW | A measure of the energy expended by the myocardium during the cardiac cycle and is derived from the pressure-strain loop. | ||
| Assessment | GLS | Primarily focuses on myocardial deformation and provides information about strain. It is a marker of contractile function. | |
| MW | Focuses on the mechanical work performed by the heart, providing insights into the energy expended by the myocardium during the cardiac cycle. | ||
| Parameters | GLS | Is a single parameter and represents the global longitudinal deformation of the left ventricle. | |
| MW | Is characterized by four parameters (GWI, GCW, GWW and GWE) that describe different aspects of myocardial performance. | ||
| Load dependency | GLS | Can be influenced by changes in preload and afterload. | |
| MW | Incorporates deformation and load into its analysis. | ||
| Similarities | Assessment | Both GLS and MW are assessed using speckle tracking echocardiography. | |
| Accurate measurements | Dependency on frame rate, good imaging quality and heart rate variability. | ||
| Visualization | Bull’s-eye plots are commonly used to visualize their results. | ||
| Clinical value | Both GLS and MW play a crucial role in the assessment of LV function. Both have demonstrated prognostic value in various heart diseases. | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frișan, A.-C.; Mornoș, C.; Lazăr, M.-A.; Șoșdean, R.; Crișan, S.; Ionac, I.; Luca, C.-T. Echocardiographic Myocardial Work: A Novel Method to Assess Left Ventricular Function in Patients with Coronary Artery Disease and Diabetes Mellitus. Medicina 2024, 60, 199. https://doi.org/10.3390/medicina60020199
Frișan A-C, Mornoș C, Lazăr M-A, Șoșdean R, Crișan S, Ionac I, Luca C-T. Echocardiographic Myocardial Work: A Novel Method to Assess Left Ventricular Function in Patients with Coronary Artery Disease and Diabetes Mellitus. Medicina. 2024; 60(2):199. https://doi.org/10.3390/medicina60020199
Chicago/Turabian StyleFrișan, Alexandra-Cătălina, Cristian Mornoș, Mihai-Andrei Lazăr, Raluca Șoșdean, Simina Crișan, Ioana Ionac, and Constantin-Tudor Luca. 2024. "Echocardiographic Myocardial Work: A Novel Method to Assess Left Ventricular Function in Patients with Coronary Artery Disease and Diabetes Mellitus" Medicina 60, no. 2: 199. https://doi.org/10.3390/medicina60020199