


Exploring the Effectiveness of Biological Therapy in Patients with Psoriasis: Body Image and Quality of Life

Abstract
:1. Introduction
2. Materials and Methods
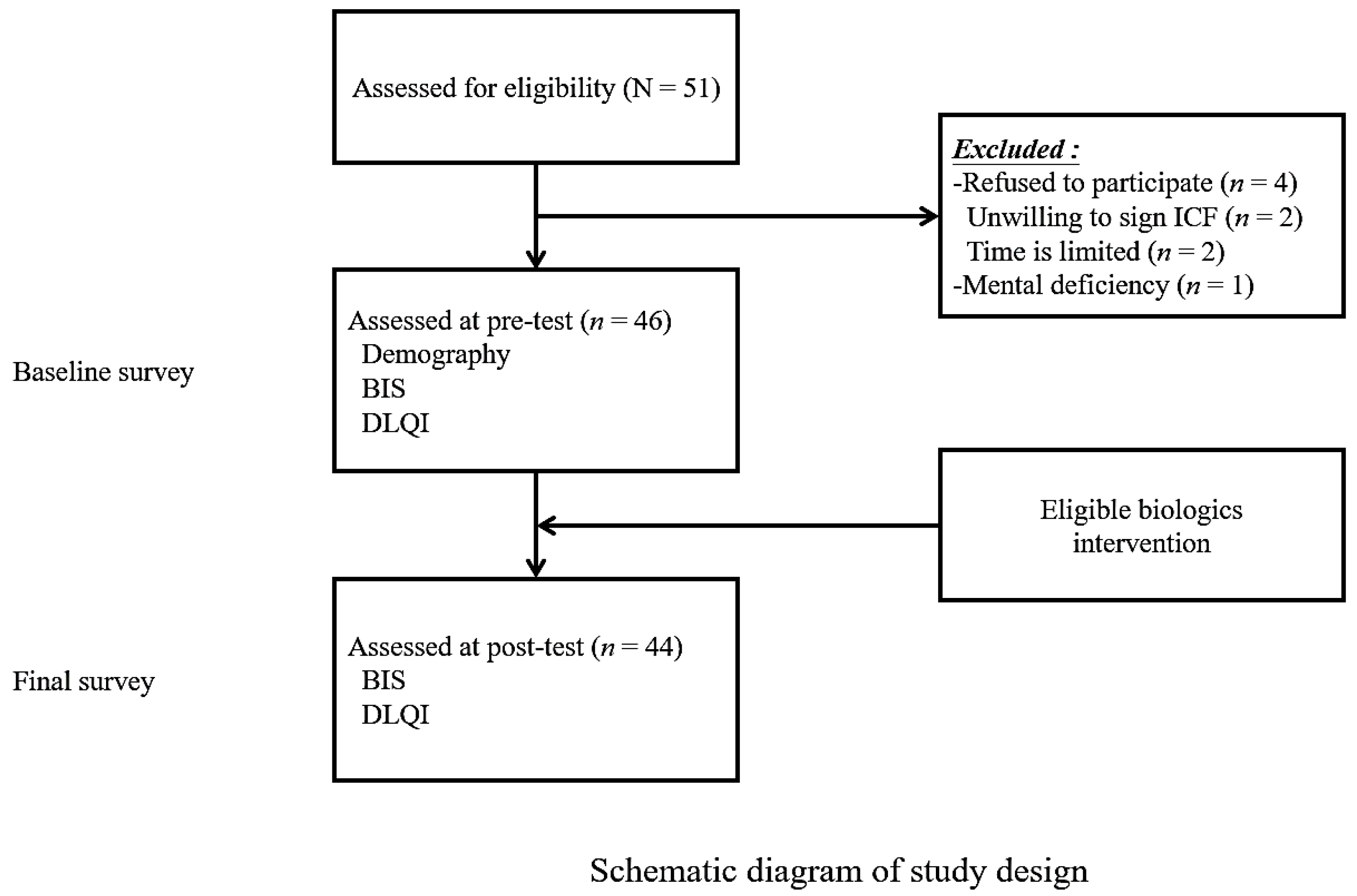
2.1. Study Design
- Individuals diagnosed with psoriasis based on diagnostic criteria and confirmed by dermatologists or rheumatologists.
- Participants undergoing biologic treatment, including the following:
- (1)
- First-time recipients of biologic treatment.
- (2)
- Individuals experiencing a psoriasis recurrence after discontinuing biologic treatment and subsequently resuming it.
- (3)
- Those transitioning to a different type of biologic treatment.
- Age 20 years or older, mentally alert, and capable of communicating in Mandarin or Taiwanese.
- Willingness to participate in the study and the ability to sign the informed consent form.
2.2. Sociodemographic Data
2.3. Body Image Scale, BIS
2.4. Dermatology Life Quality Index, DLQI
2.5. Data Processing and Statistical Analysis
3. Results
3.1. Sociodemographic Analysis of the Study Population
3.2. Psoriasis Poses a Negative Impact on Body Image
3.3. Differential Impact of Sociodemographic Variables on Quality of Life
3.4. Intervention with Biologic Agents Significantly Improves the Overall Body Image and Quality of Life
3.5. Positive Correlation between Body Image and Quality of Life
4. Discussion
4.1. Psoriasis and Body Image
4.2. Psoriasis and QoL
4.3. Psoriasis, Body Image, QoL, and Biologic Therapy
- Individual differences: Participants may have diverse responses to the intervention, with some individuals experiencing significant improvements in quality of life, while others may not experience the same level of change.
- Small sample size: The recruitment of a relatively limited sample of 44 participants means that individual response variations can have a more pronounced impact on the standard deviation.
- External influences: Uncontrollable factors, such as environmental impacts or additional treatments, could have influenced participants’ post-test scores outside the scope of the study.
4.4. Placebo Effect of Topical Therapy
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Boehncke, W.-H. Etiology and Pathogenesis of Psoriasis. Rheum. Dis. Clin. N. Am. 2015, 41, 665–675. [Google Scholar] [CrossRef]
- Ferreli, C.; Pinna, A.L.; Pilloni, L.; Tomasini, C.F.; Rongioletti, F. Histopathological aspects of psoriasis and its uncommon variants. G. Ital. Dermatol. Venereol. 2018, 153, 173–184. [Google Scholar] [CrossRef]
- Queiro, R.; Tejón, P.; Alonso, S.; Coto, P. Age at disease onset: A key factor for understanding psoriatic disease. Rheumatology 2013, 53, 1178–1185. [Google Scholar] [CrossRef]
- Boehncke, W.-H.; Schön, M.P. Psoriasis. Lancet 2015, 386, 983–994. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, C.E.M.; Van Der Walt, J.M.; Ashcroft, D.M.; Flohr, C.; Naldi, L.; Nijsten, T.; Augustin, M. The global state of psoriasis disease epidemiology: A workshop report. Br. J. Dermatol. 2017, 177, e4–e7. [Google Scholar] [CrossRef]
- Tsai, T.-F.; Wang, T.-S.; Hung, S.-T.; Tsai, P.I.-C.; Schenkel, B.; Zhang, M.; Tang, C.-H. Epidemiology and comorbidities of psoriasis patients in a national database in Taiwan. J. Dermatol. Sci. 2011, 63, 40–46. [Google Scholar] [CrossRef]
- World Health Organization. Global Report on Psoriasis. World Health Organization. 2016. Available online: https://apps.who.int/iris/handle/10665/204417 (accessed on 8 March 2022).
- Chang, Y.T.; Chen, T.J.; Liu, P.C.; Chen, Y.C.; Chen, Y.J.; Huang, Y.L.; Jih, J.S.; Chen, C.C.; Lee, D.D.; Wang, W.J.; et al. Epidemiological Study of Psoriasis in the National Health Insurance Database in Taiwan. Acta Derm. Venereol. 2009, 89, 262–266. [Google Scholar] [CrossRef] [PubMed]
- Tsai, T.F. Current Status and Prospect for Psoriasis Treatment in Taiwan. Dermatol. Sin. 2005, 23, 69–80. [Google Scholar] [CrossRef]
- Ho, C.C.; Hung, C.T.; Ko, Y.M.; Wang, Y.H.; Cheng, S.Y.; Hwu, L.J. A Study of Relationships among body Image, Anxiety, Depression and Quality of life in Patients with Psoriasis. Cheng Ching Med. J. 2020, 16, 23–32. [Google Scholar]
- Chang, J.Y.; Hsu, Y.M. A brief discussion on biological agents for the treatment of psoriasis. Chang. Nurs. 2018, 25, 11–12. [Google Scholar] [CrossRef]
- Grän, F.; Kerstan, A.; Serfling, E.; Goebeler, M.; Muhammad, K. Current Developments in the Immunology of Psoriasis. Yale J. Biol. Med. 2020, 93, 97–110. [Google Scholar]
- Armstrong, A.W.; Read, C. Pathophysiology, Clinical Presentation, and Treatment of Psoriasis: A Review. JAMA 2020, 323, 1945–1960. [Google Scholar] [CrossRef] [PubMed]
- Rosińska, M.; Rzepa, T.; Szramka-Pawlak, B.; Żaba, R. Body image and depressive symptoms in person suffering from psoriasis. Psychiatr. Polska 2017, 51, 1145–1152. [Google Scholar] [CrossRef]
- Petraškienė, R.; Valiukevičienė, S.; Macijauskienė, J. Associations of the quality of life and psychoemotional state with sociodemographic factors in patients with psoriasis. Medicina 2016, 52, 238–243. [Google Scholar] [CrossRef] [PubMed]
- Cohen, B.E.; Martires, K.J.; Ho, R.S. Psoriasis and the risk of depression in the US population: National Health and Nutrition Examination Survey 2009–2012. JAMA Dermatol. 2016, 152, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, A.; Jarvis, S.; Boehncke, W.; Rajagopalan, M.; Fernández-Peñas, P.; Romiti, R.; Bewley, A.; Vaid, B.; Huneault, L.; Fox, T.; et al. Patient perceptions of clear/almost clear skin in moderate-to-severe plaque psoriasis: Results of the Clear About Psoriasis worldwide survey. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 2200–2207. [Google Scholar] [CrossRef]
- Nazik, H.; Nazik, S.; Gul, F.C. Body Image, Self-esteem, and Quality of Life in Patients with Psoriasis. Indian Dermatol. Online J. 2017, 8, 343–346. [Google Scholar] [CrossRef]
- Rzeszutek, M.; Podkowa, K.; Pięta, M.; Pankowski, D.; Cyran-Stemplewska, S. Comparative study of life satisfaction among patients with psoriasis versus healthy comparison group: The explanatory role of body image and resource profiles. Qual. Life Res. 2021, 30, 181–191. [Google Scholar] [CrossRef]
- Yang, H.-J.; Yang, K.-C. Impact of psoriasis on quality of life in Taiwan. Dermatol. Sin. 2015, 33, 146–150. [Google Scholar] [CrossRef]
- Lee, Y.W.; Park, E.J.; Kwon, I.H.; Kim, K.J. Impact of Psoriasis on Quality of Life: Relationship between Clinical Response to Therapy and Change in Health-related Quality of Life. Ann. Dermatol. 2010, 22, 389–396. [Google Scholar] [CrossRef]
- Fortes, C.; Mastroeni, S.; Leffondré, K.; Sampogna, F.; Melchi, F.; Mazzotti, E.; Pasquini, P.; Abeni, D. Relationship Between Smoking and the Clinical Severity of Psoriasis. Arch. Dermatol. 2005, 141, 1580–1584. [Google Scholar] [CrossRef] [PubMed]
- Mahajan, V.; Dhattarwal, N.; Chauhan, P.; Mehta, K.; Sharma, R.; Sharma, A.; Singh, V.; Sharma, J.; Hooda, S. The association of alcohol use disorder and chronic plaque psoriasis: Results of a pilot study. Indian Dermatol. Online J. 2021, 12, 128–133. [Google Scholar] [CrossRef] [PubMed]
- Rakhesh, S.; D′Souza, M.; Sahai, A. Quality of life in psoriasis: A study from south India. Indian J. Dermatol. Venereol. Leprol. 2008, 74, 600–606. [Google Scholar] [CrossRef]
- Colombo, D.; Perego, R. Quality of Life in Psoriasis. In Psoriasis—Types, Causes and Medication; IntechOpen: London, UK, 2013. [Google Scholar] [CrossRef]
- Feldman, S.R.; Goffe, B.; Rice, G.; Mitchell, M.; Kaur, M.; Robertson, D.; Sierka, D.; Bourret, J.A.; Evans, T.S.; Gottlieb, A. The Challenge of Managing Psoriasis: Unmet Medical Needs and Stakeholder Perspectives. Am. Health Drug Benefits 2016, 9, 504–513. [Google Scholar]
- Ghorbanibirgani, A.; Fallahi-Khoshknab, M.; Zarea, K.; Abedi, H. The Meaning of Coping with Psoriasis: A Phenomenological Study. Jundishapur J. Chronic Dis. Care 2016, 5, e36781. [Google Scholar] [CrossRef]
- Huang, Y.-H.; Chiu, T.-M.; Ho, J.-C.; Chen, C.-C.; Hui, R.C.-Y.; Lai, P.-J.; Tsai, T.-F.J.D.S. Patient’s perception and importance of clear/almost clear skin in moderate-to-severe plaque psoriasis: Results of clear about psoriasis survey in Taiwan. Dermatol. Sin. 2019, 37, 12–18. [Google Scholar]
- Augustin, M.; Krüger, K.; Radtke, M.; Schwippl, I.; Reich, K. Disease Severity, Quality of Life and Health Care in Plaque-Type Psoriasis: A Multicenter Cross-Sectional Study in Germany. Dermatology 2008, 216, 366–372. [Google Scholar] [CrossRef]
- Mahler, R.; Jackson, C.; Ijacu, H. The Burden of Psoriasis and Barriers to Satisfactory Care: Results from a Canadian Patient Survey. J. Cutan. Med. Surg. 2009, 13, 283–293. [Google Scholar] [CrossRef]
- Patel, N.; Nadkarni, A.; Cardwell, L.A.; Vera, N.; Frey, C.; Patel, N.; Feldman, S.R. Psoriasis, depression, and inflammatory overlap: A review. Am. J. Clin. Dermatol. 2017, 18, 613–620. [Google Scholar] [CrossRef] [PubMed]
- Mease, P.J.; Menter, M.A. Quality-of-life issues in psoriasis and psoriatic arthritis: Outcome measures and therapies from a dermatological perspective. J. Am. Acad. Dermatol. 2006, 54, 685–704. [Google Scholar] [CrossRef]
- Hjalte, F.; Carlsson, K.S.; Schmitt-Egenolf, M. Sustained Psoriasis Area and Severity Index, Dermatology Life Quality Index and EuroQol-5D response of biological treatment in psoriasis: 10 years of real-world data in the Swedish National Psoriasis Register. Br. J. Dermatol. 2018, 178, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Roberts, M.S.; Cheruvu, H.S.; Mangion, S.E.; Alinaghi, A.; Benson, H.A.; Mohammed, Y.; Holmes, A.; van der Hoek, J.; Pastore, M.; Grice, J.E. Topical drug delivery: History, percutaneous absorption, and product development. Adv. Drug Deliv. Rev. 2021, 177, 113929. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Sociodemographic Variables | n | % | Cumulative % |
|---|---|---|---|
| Gender | |||
| Males | 33 | 75.00 | 75.00 |
| Females | 11 | 25.00 | 100.00 |
| Age | |||
| 40 years old and younger | 9 | 20.45 | 20.45 |
| 41 to 50 years old | 20 | 45.45 | 65.91 |
| 51 years old and older | 15 | 34.09 | 100.00 |
| Education level | |||
| High school or below | 22 | 50.00 | 50.00 |
| College or above | 22 | 50.00 | 100.00 |
| Socioeconomic status * | |||
| High | 2 | 4.55 | 4.55 |
| Middle to high | 14 | 31.82 | 36.36 |
| Middle | 17 | 38.64 | 75.00 |
| Middle to low | 11 | 25.00 | 100.00 |
| Marital status | |||
| Single | 11 | 25.00 | 25.00 |
| Married | 27 | 61.36 | 86.36 |
| Other | 6 | 13.64 | 100.00 |
| Religion | |||
| None | 23 | 52.27 | 52.27 |
| Buddhism | 10 | 22.73 | 75.00 |
| Taoism | 11 | 25.00 | 100.00 |
| Income | |||
| <19,999 NTD | 5 | 11.36 | 11.36 |
| 20,000–39,999 NTD | 14 | 31.82 | 43.18 |
| 40,000–59,999 NTD | 12 | 27.27 | 70.45 |
| >60,000 NTD | 13 | 29.55 | 100.00 |
| Chronic diseases | |||
| No | 19 | 43.18 | 43.18 |
| Yes | 25 | 56.82 | 100.00 |
| Major locations of psoriatic lesions | |||
| Scalp | 8 | 18.18 | 18.18 |
| Face | 8 | 18.18 | 36.36 |
| Trunk | 12 | 27.27 | 63.64 |
| Limbs | 16 | 36.36 | 100.00 |
| BMI groups ** | |||
| Healthy body weight | 11 | 25.00 | 25.00 |
| Non-healthy body weight | 33 | 75.00 | 100.00 |
| Smoking | |||
| Non-smoker | 25 | 56.82 | 56.82 |
| Current smoker | 15 | 34.09 | 90.91 |
| Former smoker | 4 | 9.09 | 100.00 |
| Alcohol consumption | |||
| No | 30 | 68.18 | 68.18 |
| Yes | 11 | 25.00 | 93.18 |
| Quit | 3 | 6.82 | 100.00 |
| Regular exercise | |||
| No | 20 | 45.45 | 45.45 |
| Yes | 24 | 54.55 | 100.00 |
| PASI severity | |||
| Mild | 10 | 22.73 | 22.73 |
| Moderate to severe | 34 | 77.27 | 100.00 |
| Total sample size | 44 |
| Sociodemographic Variables | Subgroup | N | Average | Standard Deviation | t-Value | p-Value |
|---|---|---|---|---|---|---|
| Gender | Male | 33 | 18.21 | 6.19 | −1.233 | 0.225 |
| Female | 11 | 20.91 | 6.56 | |||
| Educational level | High school or below | 22 | 21.95 | 4.41 | 3.652 ** | 0.001 |
| College or above | 22 | 15.82 | 6.53 | |||
| Chronic diseases | No | 19 | 17.42 | 6.34 | −1.353 | 0.183 |
| Yes | 25 | 20.00 | 6.20 | |||
| BMI groups | Healthy body weight | 11 | 19.27 | 5.37 | 0.231 | 0.818 |
| Non-healthy body weight | 33 | 18.76 | 6.68 | |||
| Regular exercise | No | 20 | 18.15 | 6.68 | −0.701 | 0.487 |
| Yes | 24 | 19.50 | 6.08 | |||
| PASI severity | Mild | 10 | 17.60 | 5.42 | −0.728 | 0.471 |
| Moderate to severe | 34 | 19.26 | 6.59 | |||
| Age | 40 years old and younger | 9 | 17.78 | 9.00 | 0.466 # | 0.631 |
| 41 to 50 years old | 20 | 18.45 | 5.83 | |||
| 51 years old and older | 15 | 20.13 | 5.26 | |||
| Socioeconomic status | Middle to high | 16 | 15.88 | 7.16 | 3.316 * # & | 0.046 |
| Middle | 17 | 21.12 | 4.27 | |||
| Middle to low | 11 | 19.82 | 6.46 | |||
| Marital status | Single | 11 | 18.09 | 5.56 | 1.931# | 0.158 |
| Married | 27 | 18.19 | 6.72 | |||
| Other | 6 | 23.50 | 4.18 | |||
| Religion | None | 23 | 16.57 | 6.52 | 3.891# * $ | 0.028 |
| Buddhism | 10 | 22.30 | 6.85 | |||
| Taoism | 11 | 20.64 | 2.94 | |||
| Income | <19,999 NTD | 5 | 16.00 | 6.60 | 1.525 # | 0.223 |
| 20,000–39,999 NTD | 14 | 21.50 | 4.97 | |||
| 40,000–59,999 NTD | 12 | 17.08 | 5.21 | |||
| >60,000 NTD | 13 | 18.85 | 7.89 | |||
| Major locations of psoriatic lesions | Scalp | 8 | 17.50 | 3.46 | 0.271 # | 0.846 |
| Face | 8 | 18.13 | 8.06 | |||
| Trunk | 12 | 19.92 | 5.57 | |||
| Limbs | 16 | 19.19 | 7.32 | |||
| Smoking | Non-smoker | 25 | 18.72 | 5.93 | 0.620 # | 0.543 |
| Current smoker | 15 | 19.93 | 6.03 | |||
| Former smoker | 4 | 16.00 | 10.23 | |||
| Alcohol consumption | No | 30 | 17.90 | 6.58 | 1.298 # | 0.284 |
| Yes | 11 | 21.45 | 4.32 | |||
| Quit | 3 | 19.33 | 9.29 |
| Aspect | Gender | N | Average | Standard Deviation | t-Value | p-Value |
|---|---|---|---|---|---|---|
| Quality of Life | M | 33 | 16.09 | 7.86 | −0.603 | 0.550 |
| F | 11 | 17.73 | 7.59 | |||
| Disease Symptoms | M | 33 | 4.15 | 1.50 | −0.777 | 0.441 |
| F | 11 | 4.55 | 1.29 | |||
| Daily Activities | M | 33 | 3.27 | 1.92 | −0.416 | 0.680 |
| F | 11 | 3.55 | 1.75 | |||
| Leisure Activities | M | 33 | 3.09 | 1.89 | 0.562 | 0.577 |
| F | 11 | 2.73 | 1.74 | |||
| Work and Study | M | 33 | 1.33 | 1.19 | −2.130 * | 0.039 |
| F | 11 | 2.18 | 0.98 | |||
| Interpersonal Relationships | M | 33 | 2.15 | 1.86 | −0.874 | 0.387 |
| F | 11 | 2.73 | 2.00 | |||
| Treatment | M | 33 | 2.09 | 0.95 | 0.259 | 0.797 |
| F | 11 | 2.00 | 1.18 |
| Pre-Test | Post-Test | t-Value | p-Value | |||
|---|---|---|---|---|---|---|
| (1)M | (2)SD | (1)M | (2)SD | |||
| Body Image | 18.89 | 6.32 | 4.93 | 4.09 | 14.205 *** | 0.000 |
| Aspect | Pre-Test | Post-Test | t-Value | p-Value | ||
|---|---|---|---|---|---|---|
| (1)M | (2)SD | (1)M | (2)SD | |||
| Disease Symptoms | 4.25 | 0.98 | 1.45 | 1.07 | 13.408 *** | 0.000 |
| Daily Activities | 3.34 | 0.75 | 1.87 | 0.97 | 7.956 *** | 0.000 |
| Leisure Activities | 3.00 | 0.50 | 1.84 | 0.76 | 8.128 *** | 0.000 |
| Work and Study | 1.55 | 0.27 | 1.19 | 0.62 | 6.404 *** | 0.000 |
| Interpersonal Relationships | 2.30 | 0.34 | 1.89 | 0.68 | 6.681 *** | 0.000 |
| Treatment | 2.07 | 0.36 | 1.00 | 0.49 | 11.286 *** | 0.000 |
| Quality of Life | 16.50 | 3.20 | 7.74 | 3.64 | 10.556 *** | 0.000 |
| Pre-Test Body Image | |
|---|---|
| Pre-test quality of life Significance (two tailed) | 0.726 ** 0.000 |
| Post-Test Body Image | |
|---|---|
| Post-test quality of life Significance (two tailed) | 0.690 ** 0.000 |
| Variable | Non-Standardized Coefficient | Standardized Coefficient | T | p-Value | ||
|---|---|---|---|---|---|---|
| B | Beta | |||||
| Body Image | 0.888 | 0.726 | 6.841 | 0.000 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, C.-L.; Chang, Y.-C.; Yao, W.-T.; Chiang, T.-I. Exploring the Effectiveness of Biological Therapy in Patients with Psoriasis: Body Image and Quality of Life. Medicina 2024, 60, 160. https://doi.org/10.3390/medicina60010160
Wu C-L, Chang Y-C, Yao W-T, Chiang T-I. Exploring the Effectiveness of Biological Therapy in Patients with Psoriasis: Body Image and Quality of Life. Medicina. 2024; 60(1):160. https://doi.org/10.3390/medicina60010160
Chicago/Turabian StyleWu, Chia-Lien, Ya-Ching Chang, Wen-Teng Yao, and Tsay-I Chiang. 2024. "Exploring the Effectiveness of Biological Therapy in Patients with Psoriasis: Body Image and Quality of Life" Medicina 60, no. 1: 160. https://doi.org/10.3390/medicina60010160