

Prognostic Tools for Older Women with Breast Cancer: A Systematic Review


Abstract
:1. Introduction
2. Methods
2.1. Information Sources and Search Strategy
2.2. Eligibility Criteria
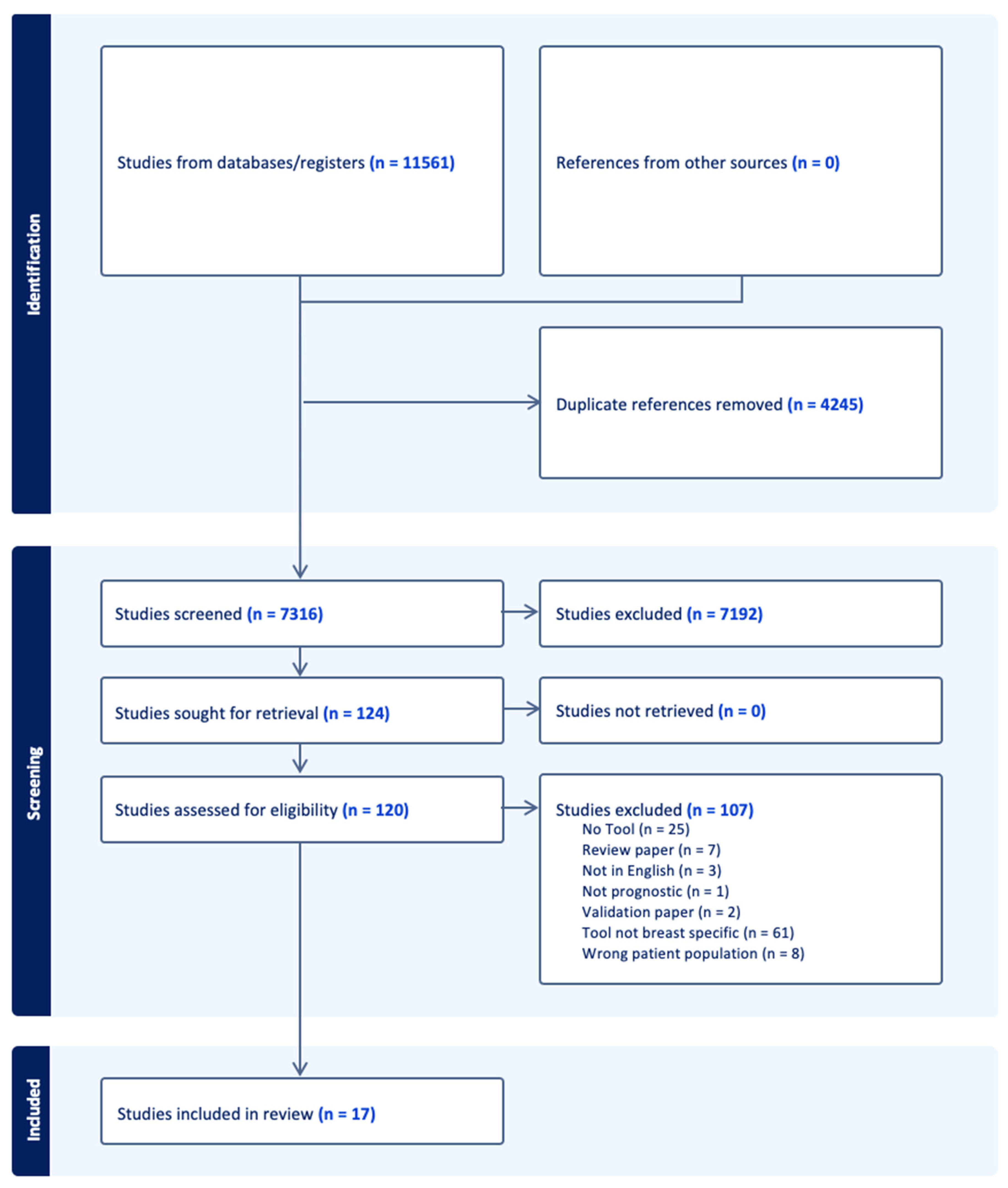
2.3. Study Selection
2.4. Data Extraction
2.5. Quality Assessment
2.6. Data Synthesis
3. Results
3.1. Prognostic Models for Adjuvant Radiation
3.2. Prognostic Models for Patients Undergoing Chemotherapy
3.3. Prognostic Models for Patients Having Surgery
3.4. Prognostic Models for Patients on Endocrine Therapy
3.5. Prognostic Models to Determine Frailty of Patients
3.6. Prognostic Models to Determine the Risk of Mortality in Patients
3.7. Risk of Bias and Applicability of the Included Studies
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Search Strategy Report for a Systematic Review of Prognostic Tools for Older Patients with Breast Cancer

{kind=link}
| Set # | Search Strategy | Results |
|---|---|---|
| #1 Elderly | “Aged”[Mesh] OR “Health Services for the Aged”[Mesh] OR Aged[tiab] OR aging[tiab] OR older[tiab] OR oldest[tiab] OR senior[tiab] OR seniors[tiab] OR Geriatrics[tiab] OR geriatric[tiab] OR Elderly[tiab] OR elder[tiab] OR elders[tiab] OR centenarian[tiab] OR centenarians[tiab] OR nonagenarian[tiab] OR nonagenarians[tiab] OR octogenarian[tiab] OR octogenarians[tiab] | 4,320,864 |
| #2 Breast Cancer | “Breast Neoplasms”[Mesh] OR ((breast[tiab] OR breasts[tiab] OR mammary[tiab] OR lobular[tiab]) AND (cancer[tiab] OR cancers[tiab] OR neoplasm[tiab] OR neoplasms[tiab] OR carcinoma[tiab] OR carcinomas[tiab] OR tumor[tiab] OR tumors[tiab] OR tumour[tiab] OR tumours[tiab] OR malignant[tiab] OR malignancy[tiab] OR malignancies[tiab] OR neoplasia[tiab] OR cancerous[tiab])) | 492,408 |
| #3 Tools | Tool[tiab] OR tools[tiab] OR instrument[tiab] OR instruments[tiab] OR PORTRET[tw] OR RSClin[tw] OR NSQIP[tw] OR “CARG-TT”[tw] OR CRASH[tw] OR “CARG-BC”[tw] | 1,119,339 |
| #4 Patients | “patients”[mesh] OR Patient[tiab] OR patients[tiab] OR woman[tiab] OR women[tiab] | 8,628,783 |
| #5 | #1 AND #2 AND #3 AND #4 | 3655 |
| Validation string | 23389352 OR 7091475 OR 16904902 OR 22433762 OR 11786579 OR 20308657 OR 25071125 OR 27048496 OR 36098027 OR 33444080 OR 22734034 | 5/11 |
| Exemplar articles retrieved: 1: Magnuson A, Sedrak MS, Gross CP, Tew WP, Klepin HD, Wildes TM, Muss HB, Dotan E, Freedman RA, O’Connor T, Dale W, Cohen HJ, Katheria V, Arsenyan A, Levi A, Kim H, Mohile S, Hurria A, Sun CL. Development and Validation of a Risk Tool for Predicting Severe Toxicity in Older Adults Receiving Chemotherapy for Early- Stage Breast Cancer. J Clin Oncol. 2021 Feb 20;39(6):608–618. doi:10.1200/JCO.20.02063. Epub 2021 Jan 14. PMID: 33444080; PMCID: PMC8189621. [14] 2: van der Plas-Krijgsman WG, Giardiello D, Putter H, Steyerberg EW, Bastiaannet E, Stiggelbout AM, Mooijaart SP, Kroep JR, Portielje JEA, Liefers GJ, de Glas NA. Development and validation of the PORTRET tool to predict recurrence, overall survival, and other-cause mortality in older patients with breast cancer in the Netherlands: a population-based study. Lancet Healthy Longev. 2021 Nov;2(11):e704-e711. doi: 10.1016/S2666-7568(21)00229-4. Epub 2021 Nov 3. PMID:36098027. [26] 3: Kanatas A, Velikova G, Roe B, Horgan K, Ghazali N, Shaw RJ, Rogers SN. Patient-reported outcomes in breast oncology: a review of validated outcome instruments. Tumori. 2012 Nov;98(6):678–88. doi: 10.1177/030089161209800602. PMID: 23389352. 4: Albert JM, Liu DD, Shen Y, Pan IW, Shih YC, Hoffman KE, Buchholz TA, Giordano SH, Smith BD. Nomogram to predict the benefit of radiation for older patients with breast cancer treated with conservative surgery. J Clin Oncol. 2012 Aug 10;30(23):2837–43. doi: 10.1200/JCO.2011.41.0076. Epub 2012 Jun 25. PMID: 22734034; PMCID: PMC3410401. [10] 5: Maratia S, Cedillo S, Rejas J. Assessing health-related quality of life in patients with breast cancer: a systematic and standardized comparison of available instruments using the EMPRO tool. Qual Life Res. 2016 Oct;25(10):2467–2480. doi: 10.1007/s11136-016-1284-8. Epub 2016 Apr 5. PMID:27048496. |
| Set # | Search Strategy | Results |
|---|---|---|
| #1 Elderly | ‘aged’/exp OR ‘elderly care’/exp OR Aged:ti,ab OR aging:ti,ab OR older:ti,ab OR oldest:ti,ab OR senior:ti,ab OR seniors:ti,ab OR Geriatrics:ti,ab OR geriatric:ti,ab OR Elderly:ti,ab OR elder:ti,ab OR elders:ti,ab OR centenarian:ti,ab OR centenarians:ti,ab OR nonagenarian:ti,ab OR nonagenarians:ti,ab OR octogenarian:ti,ab OR octogenarians:ti,ab | 4,909,255 |
| #2 Breast Cancer | ‘breast tumor’/exp OR ((breast:ti,ab OR breasts:ti,ab OR mammary:ti,ab OR lobular:ti,ab) AND (cancer:ti,ab OR cancers:ti,ab OR neoplasm:ti,ab OR neoplasms:ti,ab OR carcinoma:ti,ab OR carcinomas:ti,ab OR tumor:ti,ab OR tumors:ti,ab OR tumour:ti,ab OR tumours:ti,ab OR malignant:ti,ab OR malignancy:ti,ab OR malignancies:ti,ab OR neoplasia:ti,ab OR cancerous:ti,ab)) | 768,102 |
| #3 Tools | Tool:ti,ab OR tools:ti,ab OR instrument:ti,ab OR instruments:ti,ab OR PORTRET:ti,ab OR RSClin:ti,ab OR NSQIP:ti,ab OR ‘CARG TT’:ti,ab OR CRASH:ti,ab OR ‘CARG BC’:ti,ab | 1,482,656 |
| #4 Patients | ‘patient’/exp OR Patient:ti,ab OR patients:ti,ab OR woman:ti,ab OR women:ti,ab | 13,110,015 |
| #5 | #1 AND #2 AND #3 AND #4 | 5276 |
| #6 | #1 AND #2 AND #3 AND #4 AND [humans]/lim | 5208 |
| #7 | #1 AND #2 AND #3 AND #4 AND [humans]/lim AND ([article]/lim OR [article in press]/lim OR [conference paper]/lim OR [review]/lim) | 4294 |
| Set # | Search Strategy | Results |
|---|---|---|
| #1 Elderly | TS = (Aged OR aging OR older OR oldest OR senior OR seniors OR Geriatrics OR geriatric OR Elderly OR elder OR elders OR centenarian OR centenarians OR nonagenarian OR nonagenarians OR octogenarian OR octogenarians) | 5,230,284 |
| #2 Breast Cancer | TS = ((breast OR breasts OR mammary OR lobular) AND (cancer OR cancers OR neoplasm OR neoplasms OR carcinoma OR carcinomas OR tumor OR tumors OR tumour OR tumours OR malignant OR malignancy OR malignancies OR neoplasia OR cancerous)) | 713,188 |
| #3 Tools | TS = (Tool OR tools OR instrument OR instruments OR PORTRET OR RSClin OR NSQIP OR CARG-TT OR CRASH OR CARG-BC) | 2,594,136 |
| #4 Patients | TS = (Patient OR patients OR woman OR women) | 8,611,148 |
| #5 | #1 AND #2 AND #3 AND #4 | 3612 |
References
- Giaquinto, A.N.; Sung, H.; Miller, K.D.; Kramer, J.L.; Newman, L.A.; Minihan, A.; Jemal, A.; Siegel, R.L. Breast Cancer Statistics, 2022. CA A Cancer J. Clin. 2022, 72, 524–541. [Google Scholar] [CrossRef]
- Lodi, M.; Scheer, L.; Reix, N.; Heitz, D.; Carin, A.J.; Thiébaut, N.; Neuberger, K.; Tomasetto, C.; Mathelin, C. Breast cancer in elderly women and altered clinico-pathological characteristics: A systematic review. Breast Cancer Res. Treat. 2017, 166, 657–668. [Google Scholar] [CrossRef] [PubMed]
- Plichta, J.K.; Thomas, S.M.; Vernon, R.; Fayanju, O.M.; Rosenberger, L.H.; Hyslop, T.; Hwang, E.S.; Greenup, R.A. Breast cancer tumor histopathology, stage at presentation, and treatment in the extremes of age. Breast Cancer Res. Treat. 2020, 180, 227–235. [Google Scholar] [CrossRef]
- Pu, S.; Xie, P.; Chen, H.; Li, Y.; He, J.; Zhang, H. Evaluation of outcome of chemotherapy for breast cancer patients older than 70 years: A SEER-based study. Front. Oncol. 2023, 13, 992573. [Google Scholar] [CrossRef] [PubMed]
- Moons, K.G.; Royston, P.; Vergouwe, Y.; Grobbee, D.E.; Altman, D.G. Prognosis and prognostic research: What, why, and how? BMJ 2009, 338, b375. [Google Scholar] [CrossRef] [PubMed]
- Moons, K.G.; de Groot, J.A.; Bouwmeester, W.; Vergouwe, Y.; Mallett, S.; Altman, D.G.; Reitsma, J.B.; Collins, G.S. Critical appraisal and data extraction for systematic reviews of prediction modeling studies: The CHARMS checklist. PLoS Med. 2014, 11, e1001744. [Google Scholar] [CrossRef]
- Wolff, R.F.; Moons, K.G.; Riley, R.D.; Whiting, P.F.; Westwood, M.; Collins, G.S.; Reitsma, J.B.; Kleijnen, J.; Mallett, S.; PROBAST Group. PROBAST: A tool to assess the risk of bias and applicability of prediction model studies. Ann. Intern. Med. 2019, 170, 51–58. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Abujarad, F.; Wang, S.-Y.; Ulrich, D.; Mougalian, S.S.; Killelea, B.K.; Fraenkel, L.; Gross, C.P.; Evans, S.B. Building a Digital Health Risk Calculator for Older Women with Early-Stage Breast Cancer; Springer International Publishing: Berlin/Heidelberg, Germany, 2021; pp. 389–402. [Google Scholar] [CrossRef]
- Albert, J.M.; Liu, D.D.; Shen, Y.; Pan, I.W.; Shih, Y.C.T.; Hoffman, K.E.; Buchholz, T.A.; Giordano, S.H.; Smith, B.D. Nomogram to predict the benefit of radiation for older patients with breast cancer treated with conservative surgery. J. Clin. Oncol. 2012, 30, 2837–2843. [Google Scholar] [CrossRef]
- Chen, K.; Su, F.; Jacobs, L.K. A Nomogram to Predict the Benefit of Radiation Therapy After Breast-Conserving Surgery in Elderly Patients with Stage I & ER-Negative, or Stage II/III Disease. Ann. Surg. Oncol. 2015, 22, 3497–3503. [Google Scholar] [CrossRef]
- Wang, S.Y.; Abujarad, F.; Chen, T.; Evans, S.B.; Killelea, B.K.; Mougalian, S.S.; Fraenkel, L.; Gross, C.P. “Radiotherapy for older women (ROW)”: A risk calculator for women with early-stage breast cancer. J. Geriatr. Oncol. 2020, 11, 850–859. [Google Scholar] [CrossRef] [PubMed]
- Rades, D.; Conde, A.J.; Garcia, R.; Cacicedo, J.; Segedin, B.; Perpar, A.; Schild, S.E. A new instrument for estimation of survival in elderly patients irradiated for metastatic spinal cord compression from breast cancer. Radiat. Oncol. 2015, 10, 173. [Google Scholar] [CrossRef] [PubMed]
- Magnuson, A.; Sedrak, M.S.; Gross, C.P.; Tew, W.P.; Klepin, H.D.; Wildes, T.M.; Muss, H.B.; Dotan, E.; Freedman, R.A.; O’Connor, T.; et al. Development and Validation of a Risk Tool for Predicting Severe Toxicity in Older Adults Receiving Chemotherapy for Early-Stage Breast Cancer. J. Clin. Oncol. 2021, 39, 608–618. [Google Scholar] [CrossRef] [PubMed]
- Zhou, C.; Xu, L.; Du, Z.; Lv, Q. Geriatric Early-Stage Triple-Negative Breast Cancer Patients in Low-risk Population: Omitting Chemotherapy Based on Nomogram. Clin. Breast Cancer 2022, 22, 771–780. [Google Scholar] [CrossRef] [PubMed]
- Coradini, D.; Biganzoli, E.; Boracchi, P.; Bombardieri, E.; Seregni, E.; De Palo, G.; Martelli, G.; Di Fronzo, G. Effect of steroid receptors, pS2 and cathepsin D on the outcome of elderly breast cancer patients: An exploratory investigation. Int. J. Cancer 1998, 79, 305–311. [Google Scholar] [CrossRef]
- Lemij, A.A.; van der Plas-Krijgsman, W.G.; Bastiaannet, E.; Merkus, J.W.S.; van Dalen, T.; Vulink, A.J.E.; van Gerven, L.; Guicherit, O.R.; Linthorst-Niers, E.M.H.; Lans, T.E.; et al. Predicting postoperative complications and their impact on quality of life and functional status in older patients with breast cancer. Br. J. Surg. 2022, 109, 595–602. [Google Scholar] [CrossRef]
- Soubeyran, I.; Quénel, N.; Coindre, J.-M.; Bonichon, F.; Durand, M.; Wafflart, J.; Mauriac, L. pS2 protein: A marker improving prediction of response to neoadjuvant tamoxifen in post-menopausal breast cancer patients. Br. J. Cancer 1996, 74, 1120–1125. [Google Scholar] [CrossRef]
- Moreau-Bachelard, C.; Campion, L.; Robert, M.; Kerdraon, O.; Renaudeau, C.; Aumont, M.; Classe, J.-M.; Campone, M.; Frénel, J.-S. Development of a Prognostic Tool to Guide the Decision to Extend Adjuvant Aromatase Inhibitors for up to Ten Years in Postmenopausal Early Breast Cancer Patients. Cancers 2020, 12, 3725. [Google Scholar] [CrossRef]
- Brouwers, B.; Dalmasso, B.; Hatse, S.; Laenen, A.; Kenis, C.; Swerts, E.; Neven, P.; Smeets, A.; Schöffski, P.; Wildiers, H. Biological ageing and frailty markers in breast cancer patients. Aging 2015, 7, 319–333. [Google Scholar] [CrossRef]
- Fleming, S.T.; Rastogi, A.; Dmitrienko, A.; Johnson, K.D. A comprehensive prognostic index to predict survival based on multiple comorbidities: A focus on breast cancer. Med. Care 1999, 37, 601–614. [Google Scholar] [CrossRef]
- Lu, X.; Li, X.; Ling, H.; Gong, Y.; Guo, L.; He, M.; Sun, H.; Hu, X. Nomogram for Predicting Breast Cancer-Specific Mortality of Elderly Women with Breast Cancer. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2020, 26, e925210. [Google Scholar] [CrossRef]
- Ward, S.E.; Holmes, G.R.; Morgan, J.L.; Broggio, J.W.; Collins, K.; Richards, P.D.; Reed, M.W.R.; Wyld, L. Bridging the Age Gap: A prognostic model that predicts survival and aids in primary treatment decisions for older women with oestrogen receptor-positive early breast cancer. Br. J. Surg. 2020, 107, 1625–1632. [Google Scholar] [CrossRef] [PubMed]
- Peng, Y.; Hu, T.; Cheng, L.; Tong, F.; Cao, Y.; Liu, P.; Zhou, B.; Liu, M.; Liu, H.; Guo, J.; et al. Evaluating and Balancing the Risk of Breast Cancer-Specific Death and Other Cause-Specific Death in Elderly Breast Cancer Patients. Front. Oncol. 2021, 11, 578880. [Google Scholar] [CrossRef] [PubMed]
- Vargas, A.; Holub, K.; Biete, A. Systemic inflammation in older patients with breast cancer: The missing point in geriatric evaluations to sharpen survival prediction. Clin. Transl. Oncol. Off. Publ. Fed. Span. Oncol. Soc. Natl. Cancer Inst. Mex. 2022, 24, 1800–1808. [Google Scholar] [CrossRef] [PubMed]
- van der Plas-Krijgsman, W.G.; Giardiello, D.; Putter, H.; Steyerberg, E.W.; Bastiaannet, E.; Stiggelbout, A.M.; Mooijaart, S.P.; Kroep, J.R.; Portielje, J.E.A.; Liefers, G.-J.; et al. Development and validation of the PORTRET tool to predict recurrence, overall survival, and other-cause mortality in older patients with breast cancer in the Netherlands: A population-based study. Lancet Healthy Longev. 2021, 2, e704–e711. [Google Scholar] [CrossRef] [PubMed]
- Altman, D.G.; Royston, P. What do we mean by validating a prognostic model? Stat. Med. 2000, 19, 453–473. [Google Scholar] [CrossRef]
- Collins, G.S.; de Groot, J.A.; Dutton, S.; Omar, O.; Shanyinde, M.; Tajar, A.; Voysey, M.; Wharton, R.; Yu, L.-M.; Moons, K.G.; et al. External validation of multivariable prediction models: A systematic review of methodological conduct and reporting. BMC Med. Res. Methodol. 2014, 14, 40. [Google Scholar] [CrossRef] [PubMed]
- Phung, M.T.; Tin Tin, S.; Elwood, J.M. Prognostic models for breast cancer: A systematic review. BMC Cancer 2019, 19, 230. [Google Scholar] [CrossRef]
- Cianfrocca, M.; Goldstein, L.J. Prognostic and predictive factors in early-stage breast cancer. Oncologist 2004, 9, 606–616. [Google Scholar] [CrossRef]
- Steyerberg, E.W.; Vergouwe, Y. Towards better clinical prediction models: Seven steps for development and an ABCD for validation. Eur. Heart J. 2014, 35, 1925–1931. [Google Scholar] [CrossRef]
- Hurria, A.; Togawa, K.; Mohile, S.G.; Owusu, C.; Klepin, H.D.; Gross, C.P.; Lichtman, S.M.; Gajra, A.; Bhatia, S.; Katheria, V.; et al. Predicting Chemotherapy Toxicity in Older Adults with Cancer: A Prospective Multicenter Study. J. Clin. Oncol. 2011, 29, 3457–3465. [Google Scholar] [CrossRef]
- de Glas, N.A.; Bastiaannet, E.; Engels, C.C.; de Craen, A.J.M.; Putter, H.; van de Velde, C.J.H.; Hurria, A.; Liefers, G.J.; Portielje, J.E.A. Validity of the online PREDICT tool in older patients with breast cancer: A population-based study. Br. J. Cancer 2016, 114, 395–400. [Google Scholar] [CrossRef]
- Kimmick, G.G.; Major, B.; Clapp, J.; Sloan, J.; Pitcher, B.; Ballman, K.; Barginear, M.; Freedman, R.A.; Artz, A.; Klepin, H.D.; et al. Using ePrognosis to estimate 2-year all-cause mortality in older women with breast cancer: Cancer and Leukemia Group B (CALGB) 49907 and 369901 (Alliance A151503). Breast Cancer Res. Treat. 2017, 163, 391–398. [Google Scholar] [CrossRef]
- Dillon, J.; Thomas, S.M.; Rosenberger, L.H.; DiLalla, G.; Fayanju, O.M.; Menendez, C.S.; Hwang, E.S.; Plichta, J.K. Mortality in Older Patients with Breast Cancer Undergoing Breast Surgery: How Low is “Low Risk”? Ann. Surg. Oncol. 2021, 28, 5758–5767. [Google Scholar] [CrossRef]
- Plichta, J.K.; Rushing, C.N.; Lewis, H.C.; Rooney, M.M.; Blazer, D.G.; Thomas, S.M.; Hwang, E.S.; Greenup, R.A. Implications of missing data on reported breast cancer mortality. Breast Cancer Res. Treat. 2023, 197, 177–187. [Google Scholar] [CrossRef] [PubMed]

| Tool | Authors | Year of Publication | Minimum Patient Age | Number of Patients in Development Cohort | Source of Data for Development Cohort | Number of Patients in Validation Cohort * | Source of Data for Validation Cohort * |
|---|---|---|---|---|---|---|---|
| Nomogram for benefit from RT | Albert et al. [10] | 2012 | 66 | 16,092 | SEER | ||
| Nomogram for benefit from RT | Chen et al. [11] | 2015 | 70 | 9079 | SEER | ||
| Radiation for Older Women | Wang et al. [12] | 2020 | 65 | 0 | 56,700 simulations | ||
| Tool for spinal metastasis benefit from RT | Rades et al. [13] | 2015 | 65 | 218 | University of Lübeck, Germany | ||
| Cancer and Aging Research Group-Breast Cancer score | Magnuson et al. [14] | 2021 | 65 | 283 | HOPE | 190 | HOPE |
| Nomogram for omitting chemotherapy in TNBC | Zhou et al. [15] | 2022 | 65 | 6482 | SEER | ||
| Tumor markers for post-surgical DFS | Coradini et al. [16] | 1998 | 70 | 83 | National Tumor Institute, Italy | ||
| Model for postoperative complications | Lemij et al. [17] | 2022 | 70 | 547 | CLIMB | 2727 | Bridging the Age Gap Study |
| Tumor markers for response to neoadjuvant Tamoxifen | Soubeyran et al. [18] | 1996 | postmenopausal | 208 | Bergonie Institue, France | ||
| Clinical Treatment Score post-5 years | Moreau-Bachelard et al. [19] | 2020 | postmenopausal | 1105 | BERENIS | ||
| Biomarkers for frailty | Brouwers et al. [20] | 2015 | 70 | 162 | University Hospitals Leuven | ||
| Comprehensive Prognosis Index | Fleming et al. [21] | 1999 | 67 | 848 | Kentucky Cancer Registry | ||
| Nomogram for survival | Lu et al. [22] | 2020 | 65 | 20,798 | SEER | 4443 | SEER |
| Age Gap | Ward et al. [23] | 2020 | 70 | 23,842 | West Midlands Cancer Intelligence Unit and Northern and Yorkshire Cancer Registry and Information Service registries, UK | 14,562 | Eastern Cancer Registration and Information Centre |
| Nomogram for survival | Peng et al. [24] | 2021 | 70 | 420 | Peking University People’s Hospital, China | ||
| Inflammatory markers for survival | Vargas et al. [25] | 2022 | 70 | 148 | Diego Portales University, Chile | ||
| PORTRET | Van der Plas-Krigsman et al. [26] | 2021 | 70 | 2744 | FOCUS | 13,631 | Netherlands Cancer Registry |
| Tool | Authors | Eligibility Criteria | Outcome Predicted | Number of Predictive Factors | Predictive Factors |
|---|---|---|---|---|---|
| Nomogram for benefit from RT | Albert et al. [10] | any unilateral breast cancer treated with BCS | mastectomy-free survival benefit from adjuvant RT | 6 | age, race, tumor size, ER status, RT, nodal pathology |
| Nomogram for benefit from RT | Chen et al. [11] | stage I & ER- or stage II/III breast cancer treated with BCS | BCSS benefit from adjuvant RT | 6 | ER status, PR status, tumor grade, T stage, N stage, race |
| Radiation for Older Women | Wang et al. [12] | early stage, ER+, LN-negative breast cancer treated with BCS | OS and local recurrence benefit from adjuvant RT | 16 | age, BMI, cigarette use, COPD, other cancer, CJF, DM, difficulty walking several blocks, difficult managing finances, difficulty bathing, difficulty pushing/pulling large objects, tumor grade, tumor size, ER status, margin, LN, additional health conditions, additional breast cancer factors |
| Tool for spinal metastasis benefit from RT | Rades et al. [13] | any breast cancer metastasized to the spinal cord | OS benefit from spinal RT | 9 | fractionation regimen, age, time from breast cancer diagnosis to RT of MSCC, visceral metastases, other bone metastases, time developing motor deficits, pre-radiotherapy ambulatory status, number of involved vertebrae, and Eastern Cooperative Oncology Group (ECOG) performance score |
| Cancer and Aging Research Group-Breast Cancer score | Magnuson et al. [14] | stage I–III breast cancer | likelihood of grade 3–5 chemotherapy toxicity | 8 | stage, use of anthracyclines, treatment duration, hemoglobin, liver function, number of falls in last 6 months, ability to walk 1 mile, present of support person for crisis |
| Nomogram for omitting chemotherapy in TNBC | Zhou et al. [15] | T1-2, N0-1, M0 TNBC | OS and BCSS benefit from chemotherapy | 7 | age, married status, grade, T-stage, N-stage, RT, BCS |
| Tumor markers for post-surgical DFS | Coradini et al. [16] | any M0 breast cancer treated with surgery | post-surgical DFS | 3 | PR, pS2, cathepsin D |
| Model for postoperative complications | Lemij et al. [17] | any M0 breast cancer | likelihood of post-surgical complication | 5 | age, polypharmacy, BMI, type of breast surgery, type of axillary surgery |
| Tumor markers for response to neoadjuvant Tamoxifen | Soubeyran et al. [18] | any M0 breast cancer | tumor regression in repones to tamoxifen | 2 | ER, pS2 |
| Clinical Treatment Score post-5 years | Moreau-Bachelard et al. [19] | early, ER+ breast cancer treated with ≥4.5 years of tamoxifen | risk of distance recurrence after 5 years of tamoxifen | 4 | tumor grade, age, tumor size, number of LN involved |
| Biomarkers for frailty | Brouwers et al. [20] | any M0 breast cancer | Leuven Oncogeriatric Frailty Score | 1 | plasma IL-6 |
| Comprehensive Prognosis Index | Fleming et al. [21] | any breast cancer | 1-year BCSD and OCSD | 15 | age, cancer stage, acute MI/unstable angina, CHF, cerebrovascular disease/stroke, dementia, hemiplegia/paraplegia, other neurologic disorder, mild-moderate pulmonary disease, mild-moderate renal disease, severe ESRD, mild-moderate gallbladder/pancreas disease, severe gallbladder/pancreas disease, any other cancer, coagulopathy |
| Nomogram for survival | Lu et al. [22] | any M0 breast cancer | 5-, 8-, and 10-year BCSD | 10 | age, marital statis, race, IDC vs. ILC, grade, T stage, N stage, ER, PR, surgery type |
| Age Gap | Ward et al. [23] | ER+ early breast cancer | 2- and 5-year BCSD and OCSD | 9 | primary surgical vs. endocrine treatment, age, Charlson co-morbidity index, frailty score, grade, nodal status, size, detected on screening vs. symptomatic, deprivation rating of postal code |
| Nomogram for survival | Peng et al. [24] | any breast cancer | 1-, 3-, and 5-year BCSD and OCSD | 10 | age, treatment with chemotherapy, number of comorbidities, HR, HER2, Ki67, T stage, N stage, receipt of surgery, receipt of RT |
| Inflammatory markers for survival | Vargas et al. [25] | any node-positive breast cancer | risk of BCSD | 5 | levels of monocytes, levels of neutrophils, neutrophil-to-lymphocytes ratio, level of eosinophils, eosinophil multiple by neutrophils-to-lymphocytes ratio |
| PORTRET | Van der Plas-Krigsman et al. [26] | operable breast cancer treated with locoregional therapy | 5-year overall mortality, 5-year OCSD, and risk of recurrence | 13 | age, size, nodal status, grade, HR, HER2, Ki67, number of comorbidities, polypharmacy, difficulty walking, sensory handicap, dementia |
| Study | Participants Selection | Predictor Factor Measurement | Outcome Measurement | Statistical Analysis | Overall Risk of Bias |
|---|---|---|---|---|---|
| Albert et al. [10] | low | low | low | low | low |
| Chen et al. [11] | low | low | low | low | low |
| Wang et al. [12] | unclear | low | low | low | high |
| Rades et al. [13] | low | low | low | high | high |
| Magnuson et al. [14] | low | low | low | low | low |
| Zhou et al. [15] | low | low | low | low | low |
| Coradini et al. [16] | low | low | low | low | low |
| Lemij et al. [17] | high | low | low | low | high |
| Soubeyran et al. [18] | low | low | low | high | high |
| Moreau-Bachelard et al. [19] | low | low | low | low | low |
| Brouwers et al. [20] | low | low | low | low | low |
| Fleming et al. [21] | low | low | low | low | low |
| Lu et al. [22] | high | low | low | low | high |
| Ward et al. [23] | low | low | low | low | low |
| Peng et al. [24] | low | low | low | low | low |
| Vargas et al. [25] | low | low | low | high | high |
| Van der Plas-Krigsman et al. [26] | low | low | low | low | low |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Record, S.M.; Chanenchuk, T.; Parrish, K.M.; Kaplan, S.J.; Kimmick, G.; Plichta, J.K. Prognostic Tools for Older Women with Breast Cancer: A Systematic Review. Medicina 2023, 59, 1576. https://doi.org/10.3390/medicina59091576
Record SM, Chanenchuk T, Parrish KM, Kaplan SJ, Kimmick G, Plichta JK. Prognostic Tools for Older Women with Breast Cancer: A Systematic Review. Medicina. 2023; 59(9):1576. https://doi.org/10.3390/medicina59091576
Chicago/Turabian StyleRecord, Sydney M., Tori Chanenchuk, Kendra M. Parrish, Samantha J. Kaplan, Gretchen Kimmick, and Jennifer K. Plichta. 2023. "Prognostic Tools for Older Women with Breast Cancer: A Systematic Review" Medicina 59, no. 9: 1576. https://doi.org/10.3390/medicina59091576