
Three Logistic Predictive Models for the Prediction of Mortality and Major Pulmonary Complications after Cardiac Surgery
 , , , ,
, , , ,
Abstract
:1. Background
2. Materials and Methods
2.1. Statistical Analysis
2.2. Sample Size Calculation
3. Results
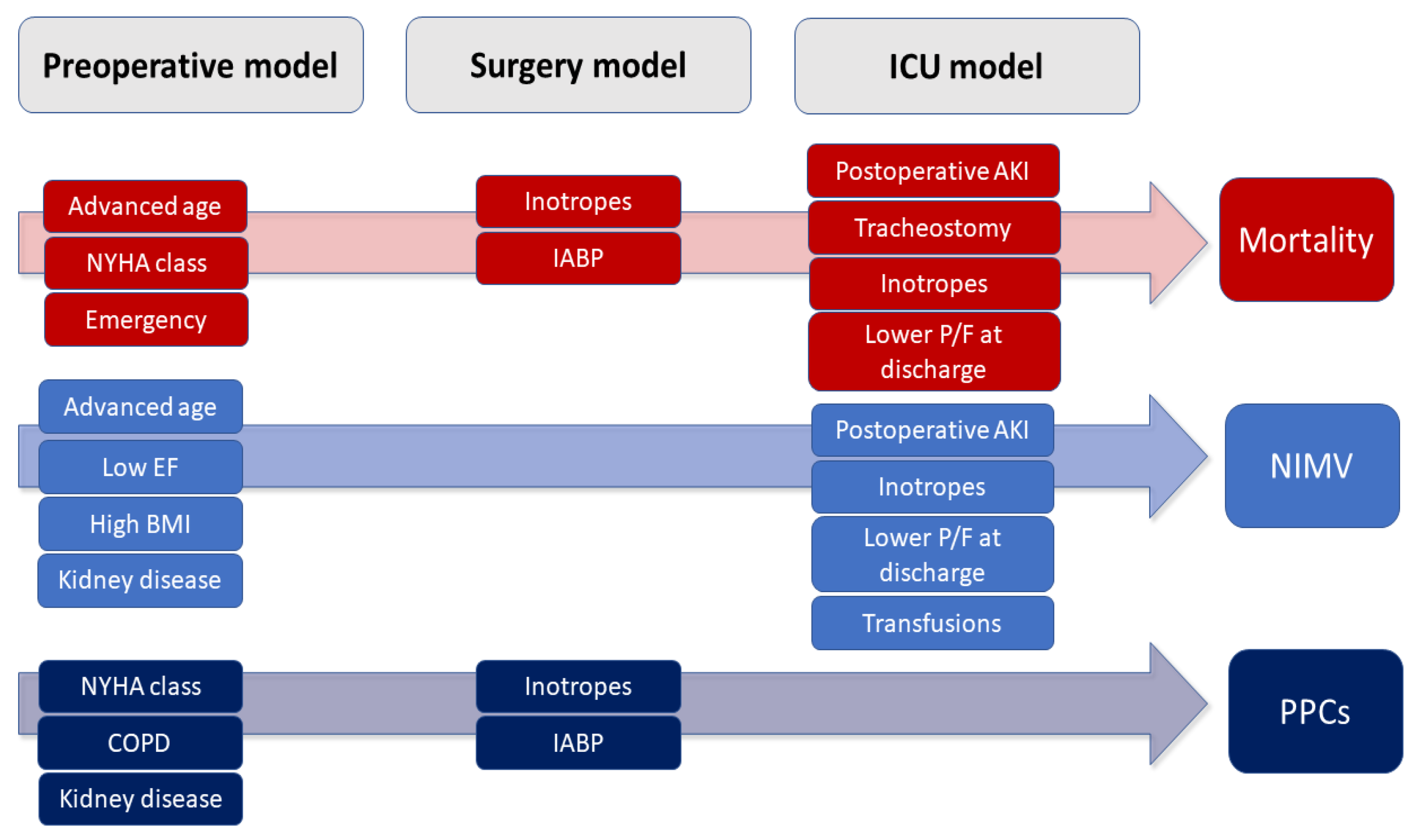
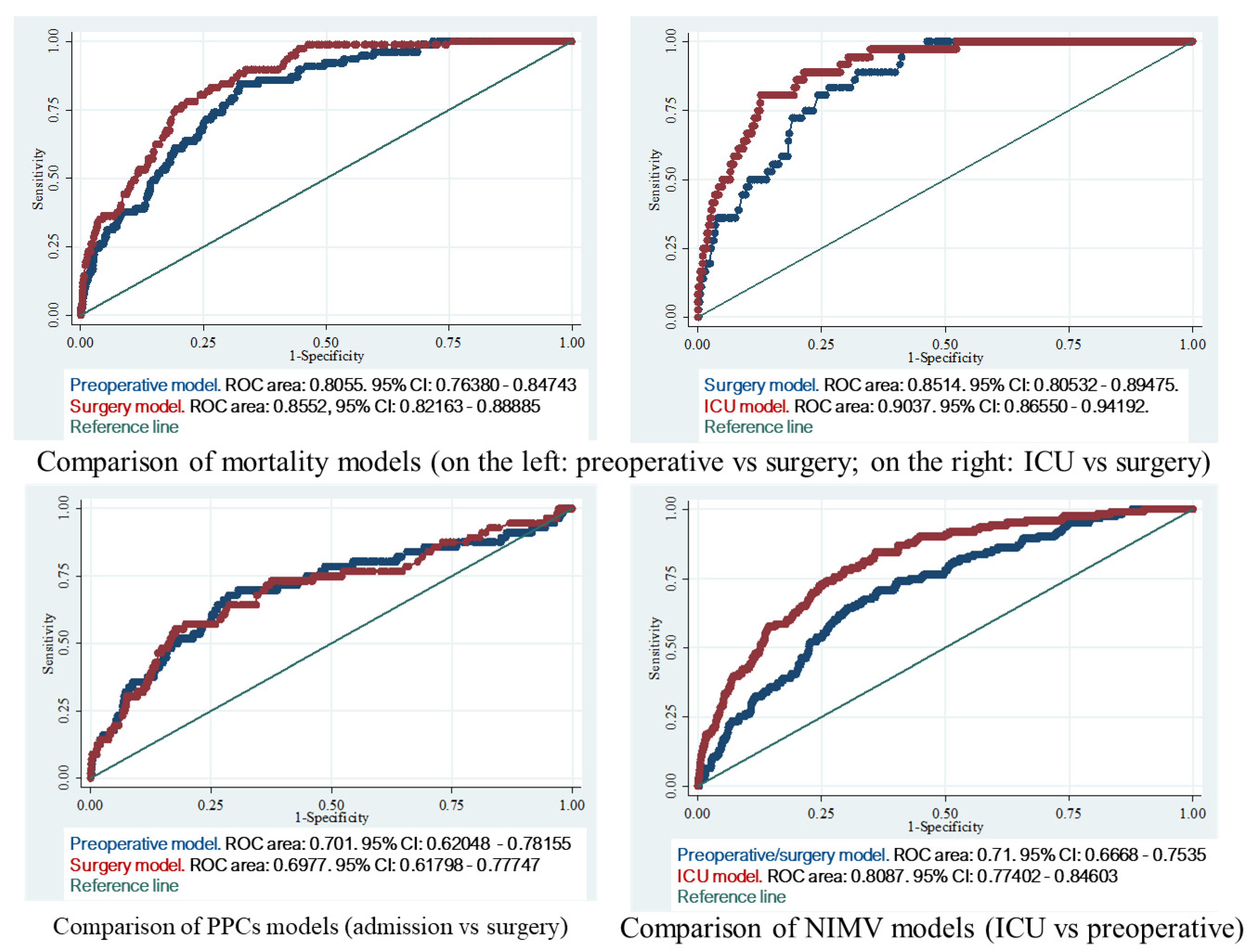
3.1. In-Hospital Mortality Predictive Models
3.1.1. Preoperative Model
3.1.2. Surgery Model
3.1.3. ICU Model
3.2. Postoperative NIMV Predictive Models
3.2.1. Preoperative/Surgery Model
3.2.2. ICU Model
3.3. Postoperative Pulmonary Complication Predictive Model
3.3.1. Preoperative Model
3.3.2. Surgery Model
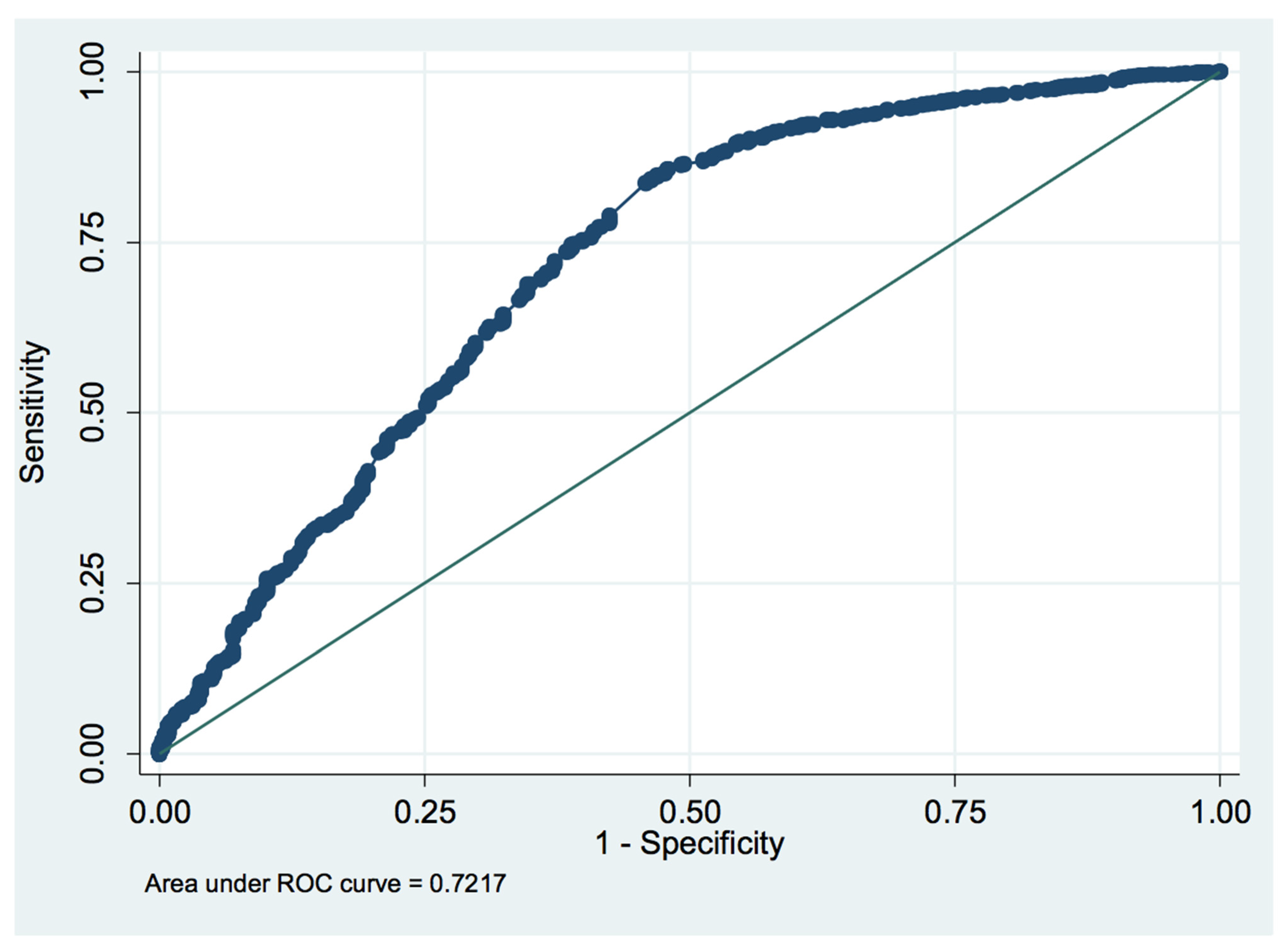
3.4. ROC Curve Analysis of the PaO2/FiO2 Ratio
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Puskas, J.D.; Kilgo, P.D.; Thourani, V.H.; Lattouf, O.M.; Chen, E.; Vega, J.D.; Guyton, R.A.; Halkos, M. The society of thoracic surgeons 30-day predicted risk of mortality score also predicts long-term survival. Ann. Thorac. Surg. 2012, 93, 26–35. [Google Scholar] [CrossRef]
- Barili, F.; Pacini, D.; Capo, A.; Rasovic, O.; Grossi, C.; Alamanni, F.; Di Bartolomeo, R.; Parolari, A. Does EuroSCORE II perform better than its original versions? A multicentre validation study. Eur. Heart J. 2013, 34, 22–29. [Google Scholar] [PubMed] [Green Version]
- Hemmes, S.N.T.; Canet, J.; Hedenstierna, G.; Jaber, S.; Hiesmayr, M.; Hollmann, M.W.; Mills, G.H.; Melo, M.F.V.; Pearse, R.; Putensen, C.; et al. The LAS VEGAS risk score for prediction of postoperative pulmonary complications. Eur. J. Anaesthesiol. 2018, 35, 691–701. [Google Scholar] [CrossRef]
- Almashrafi, A.; Elmontsri, M.; Aylin, P. Systematic review of factors influencing length of stay in ICU after adult cardiac surgery. BMC Health Serv. Res. 2016, 16, 318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magnusson, L.; Zemgulis, V.; Wicky, S.; Tydén, H.; Thelin, S.; Hedenstierna, G. Atelectasis is a major cause of hypoxemia and shunt after cardiopulmonary bypass: An experimental study. Anesthesiology 1997, 87, 1153–1163. [Google Scholar] [PubMed]
- Weiss, Y.G.; Merin, G.; Koganov, E.; Ribo, A.; Oppenheim-Eden, A.; Medalion, B.; Peruanski, M.; Reider, E.; Bar-Ziv, J.; Hanson, W.C.; et al. Postcardiopulmonary bypass hypoxemia: A prospective study on incidence, risk factors, and clinical significance. J. Cardiothorac. Vasc. Anesth. 2000, 14, 506–513. [Google Scholar] [CrossRef]
- Canet, J.; Gallart, L.; Gomar, C.; Paluzie, G.; Vallès, J.; Castillo, J.; Sabaté, S.; Mazo, V.; Briones, Z.; Sanchis, J.; et al. Prediction of postoperative pulmonary complications in a population-based surgical cohort. Anesthesiology 2010, 113, 1338–1350. [Google Scholar]
- Wynne, R.; Botti, M. Postoperative pulmonary dysfunction in adults after cardiac surgery with cardiopulmonary bypass: Clinical significance and implications for practice. Am. J. Crit. Care 2004, 13, 384–393. [Google Scholar] [CrossRef]
- Pizov, R.; Weiss, Y.G.; Oppenheim-Eden, A.; Glickman, H.; Goodman, S.; Koganov, Y.; Barak, V.; Merin, G.; Kramer, M.R. High oxygen concentration exacerbates cardiopulmonary bypass-induced lung injury. J. Cardiothorac. Vasc. Anesth. 2000, 14, 519–523. [Google Scholar] [CrossRef]
- Bignami, E.; Guarnieri, M.; Saglietti, F.; Belletti, A.; Trumello, C.; Giambuzzi, I.; Monaco, F.; Alfieri, O. Mechanical Ventilation During Cardiopulmonary Bypass. J. Cardiothorac. Vasc. Anesth. 2016, 30, 1668–1675. [Google Scholar] [CrossRef]
- Alexander, V.; Jorrit, H.; Rogier, D.; Denise, V.; Frederique, P.; Marcel, L.; Sacha, Z.; Margreeth, V.; Marcus, S.; Nicole, J. Transfusion-related acute lung injury in cardiac surgery patients is characterized by pulmonary inflammation and coagulopathy: A prospective nested case-control study*. Crit. Care Med. 2012, 40, 2813. [Google Scholar]
- Vlaar, A.P.J.; Cornet, A.D.; Hofstra, J.J.; Porcelijn, L.; Beishuizen, A.; Kulik, W.; Vroom, M.B.; Schultz, M.J.; Groeneveld, A.B.J.; Juffermans, N.P. The effect of blood transfusion on pulmonary permeability in cardiac surgery patients: A prospective multicenter cohort study. Transfusion 2012, 52, 82–90. [Google Scholar]
- Vlaar, A.P.J.; Hofstra, J.J.; Determann, R.M.; Veelo, D.P.; Paulus, F.; Kulik, W.; Korevaar, J.; de Mol, B.A.; Koopman, M.M.W.; Porcelijn, L.; et al. The incidence, risk factors, and outcome of transfusion-related acute lung injury in a cohort of cardiac surgery patients: A prospective nested case-control study. Blood 2011, 117, 4218–4225. [Google Scholar]
- Totonchi, Z.; Baazm, F.; Chitsazan, M.; Seifi, S.; Chitsazan, M. Predictors of prolonged mechanical ventilation after open heart surgery. J. Cardiovasc. Thorac. Res. 2014, 6, 211–216. [Google Scholar] [CrossRef] [Green Version]
- Bartz, R.R.; Ferreira, R.G.; Schroder, J.N.; Davies, J.; Liu, W.W.; Camara, A.; Welsby, I.J. Prolonged pulmonary support after cardiac surgery: Incidence, risk factors and outcomes: A retrospective cohort study. J. Crit. Care 2015, 30, 940–944. [Google Scholar]
- Rezaianzadeh, A.; Maghsoudi, B.; Tabatabaee, H.; Keshavarzi, S.; Bagheri, Z.; Sajedianfard, J.; Gerami, H.; Rasouli, J. Factors associated with extubation time in coronary artery bypass grafting patients. PeerJ 2015, 3, e1414. [Google Scholar]
- Wynne, R. Variable definitions: Implications for the prediction of pulmonary complications after adult cardiac surgery. Eur. J. Cardiovasc. Nurs. 2004, 3, 43–52. [Google Scholar]
- Cislaghi, F.; Condemi, A.M.; Corona, A. Predictors of prolonged mechanical ventilation in a cohort of 3269 CABG patients. Minerva. Anestesiol. 2007, 73, 615–621. [Google Scholar]
- Cislaghi, F.; Condemi, A.M.; Corona, A. Predictors of prolonged mechanical ventilation in a cohort of 5123 cardiac surgical patients. Eur. J. Anaesthesiol. 2009, 26, 396–403. [Google Scholar]
- Ji, Q.; Mei, Y.; Wang, X.; Feng, J.; Cai, J.; Ding, W. Risk factors for pulmonary complications following cardiac surgery with cardiopulmonary bypass. Int. J. Med. Sci. 2013, 10, 1578–1583. [Google Scholar]
- Hill, A.D.; Fowler, R.A.; Burns, K.E.A.; Rose, L.; Pinto, R.L.; Scales, D.C. Long-Term Outcomes and Health Care Utilization after Prolonged Mechanical Ventilation. Ann. Am. Thorac. Soc. 2017, 14, 355–362. [Google Scholar]
- Litwinowicz, R.; Bartus, K.; Drwila, R.; Kapelak, B.; Konstanty-Kalandyk, J.; Sobczynski, R.; Wierzbicki, K.; Bartuś, M.; Chrapusta, A.; Timek, T.; et al. In-hospital mortality in cardiac surgery patients after readmission to the intensive care unit: A single-center experience with 10,992 patients. J. Cardiothorac. Vasc. Anesth. 2015, 29, 570–575. [Google Scholar] [PubMed]
- Ranieri VI, T.O.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L. Acute respiratory distress syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar]
- Esteve, F.; Lopez-Delgado, J.C.; Javierre, C.; Skaltsa, K.; Carrio, M.L.L.; Rodríguez-Castro, D.; Torrado, H.; Farrero, E.; Diaz-Prieto, A.; Ventura, J.L.L.; et al. Evaluation of the PaO2/FiO2 ratio after cardiac surgery as a predictor of outcome during hospital stay. BMC Anesthesiol. 2014, 14, 83. [Google Scholar]
- Ranucci, M.; Ballotta, A.; La Rovere, M.T.; Castelvecchio, S. Surgical and Clinical Outcome Research (SCORE) Group. Postoperative hypoxia and length of intensive care unit stay after cardiac surgery: The underweight paradox? PLoS ONE 2014, 9, e93992. [Google Scholar]
- Bellini, V.; Valente, M.; Bertorelli, G.; Pifferi, B.; Craca, M.; Mordonini, M.; Lombardo, G.; Bottani, E.; Del Rio, P.; Bignami, E. Machine learning in perioperative medicine: A systematic review. J. Anesth. Analg. Crit. Care 2022, 2, 2. [Google Scholar]
- Chadaga, K.; Prabhu, S.; Bhat, V.; Sampathila, N.; Umakanth, S.; Chadaga, R. A Decision Support System for Diagnosis of COVID-19 from Non-COVID-19 Influenza-like Illness Using Explainable Artificial Intelligence. Bioengineering 2023, 10, 439. [Google Scholar]
- Khanna, V.V.; Chadaga, K.; Sampathila, N.; Prabhu, S.; Bhandage, V.; Hegde, G.K. A distinctive explainable machine learning framework for detection of polycystic ovary syndrome. Appl. Syst. Innov. 2023, 6, 32. [Google Scholar]
- Olper, L.; Bignami, E.; Di Prima, A.L.; Albini, S.; Nascimbene, S.; Cabrini, L.; Giovanni, L.; Alfieri, O. Continuous Positive Airway Pressure Versus Oxygen Therapy in the Cardiac Surgical Ward: A Randomized Trial. J. Cardiothorac. Vasc. Anesth. 2017, 31, 115–121. [Google Scholar]
- Ladha, K.; Melo MF, V.; McLean, D.J.; Wanderer, J.P.; Grabitz, S.D.; Kurth, T.; Eikermann, M. Intraoperative protective mechanical ventilation and risk of postoperative respiratory complications: Hospital based registry study. BMJ 2015, 351, h3646. [Google Scholar]
- World Medical Association. Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. In Proceedings of the 64th WMA General Assembly, Fortaleza, Brazil, 19 October 2013.
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Med. 2017, 43, 304–377. [Google Scholar]
- Ranucci, M.; Castelvecchio, S.; Conte, M.; Megliola, G.; Speziale, G.; Fiore, F.; Guarracino, F.; Scolletta, S.; Escobar, R.M.; Falco, M.; et al. The easier, the better: Age, creatinine, ejection fraction score for operative mortality risk stratification in a series of 29,659 patients undergoing elective cardiac surgery. J. Thorac. Cardiovasc. Surg. 2011, 142, 581–586. [Google Scholar]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar]
- Peduzzi, P.; Concato, J.; Kemper, E.; Holford, T.R.; Feinstein, A.R. A simulation study of the number of events per variable in logistic regression analysis. J. Clin. Epidemiol. 1996, 49, 1373–1379. [Google Scholar]
- Hosmer, D.W., Jr.; Lemeshow, S.; Sturdivant, R.X. Applied Logistic Regression; John Wiley & Sons: Hoboken, NJ, USA, 2013. [Google Scholar]
- Roques, F.; Michel, P.; Goldstone, A.R.; Nashef, S.A.M. The logistic EuroSCORE. Eur. Heart J. 2003, 24, 881–882. [Google Scholar] [CrossRef]
- Shahian, D.M.; Jacobs, J.P.; Badhwar, V.; Kurlansky, P.A.; Furnary, A.P.; Cleveland, J.C., Jr.; Lobdell, K.W.; Vassileva, C.; von Ballmoos, M.C.W.; Thourani, V.H.; et al. The Society of Thoracic Surgeons 2018 Adult Cardiac Surgery Risk Models: Part 1—Background, Design Considerations, and Model Development. Ann. Thorac. Surg. 2018, 105, 1411–1418. [Google Scholar] [CrossRef] [Green Version]
- Kapadohos, T.; Angelopoulos, E.; Vasileiadis, I.; Nanas, S.; Kotanidou, A.; Karabinis, A.; Marathias, K.; Routsi, C. Determinants of prolonged intensive care unit stay in patients after cardiac surgery: A prospective observational study. J. Thorac. Dis. 2017, 9, 70–79. [Google Scholar]
- Bignami, E.; Guarnieri, M.; Saglietti, F.; Maglioni, E.M.; Scolletta, S.; Romagnoli, S.; De Paulis, S.; Paternoster, G.; Trumello, C.; Meroni, R.; et al. Different strategies for mechanical VENTilation during CardioPulmonary Bypass (CPBVENT 2014): Study protocol for a randomized controlled trial. Trials 2017, 18, 264. [Google Scholar]
- Abbott TE, F.; Fowler, A.J.; Pelosi, P.; De Abreu, M.G.; Møller, A.M.; Canet, J.; Creagh-Brown, B.; Mythen, M.; Gin, T.; Lalu, M.M.; et al. A systematic review and consensus definitions for standardised end-points in perioperative medicine: Pulmonary complications. Br. J. Anaesth. 2018, 120, 1066–1079. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Variable | Training Set (7448 (66%) Cases) | Test Set (3837 (34%) Cases) |
|---|---|---|
| Age, yrs | 67.98 ± 14.00 | 67.59 ± 13.98 |
| Male sex, n (%) | 4394 (59%) | 2302 (60%) |
| BMI, kg/m2 | 25.45 ± 3.97 | 25.46 ± 3.00 |
| Preoperative EF, % | 56.23 ± 9.00 | 56.19 ± 9.99 |
| NYHA class > II, n (%) | (28.20%) | 1082 (28.20%) |
| Preoperative comorbidities | ||
| COPD, n (%) | 476 (6.39%) | 252 (6.56%) |
| Hypertension, n (%) | 3706 (49.75%) | 2003 (52.19%) |
| Type II Diabetes, n (%) | 779 (10.46%) | 426 (11.10%) |
| Preoperative creatinine, mg/dL | 0.98 ± 0.68 | 0.98 ± 0.66 |
| Chronic renal failure, n (%) | 1418 (19%) | 789 (20%) |
| Peripheral vasculopathy, n (%) | 1089 (14.63%) | 518 (13.50%) |
| Smoking habits, n (%) | 1,279,504 (17.17%) | 653 (17.01%) |
| Stroke, n (%) | (6.76%) | 279 (7.27%) |
| Timing of surgery | ||
| Emergency or urgency, n (%) | 63 (0.85%) | 32 (0.85%) |
| Planned, n (%) | 7385 (99.15%) | 3805 (99.15%) |
| Type of surgery | ||
| Valvular surgery, n (%) | 2944 (39.53%) | 1535 (39.99%) |
| Coronary surgery, n (%) | 991 (13.30%) | 476 (12.42%) |
| Ascending aorta aneurysm surgery, n (%) | 236 (3.17%) | 106 (2.77%) |
| Other surgical procedures, n (%) | 343 (4.60%) | 172 (4.48%) |
| Combined surgery (two or more procedures), n (%) | 2934 (39.40%) | 1548 (40.35%) |
| Variable | Preoperative Value |
|---|---|
| Age, y | 67.55 ± 13.97 |
| Male sex, n (%) | 9844 (87.2%) |
| Height, cm | 169 ± 9 |
| Weight, kg | 73 ± 13 |
| BMI, kg/m2 | 25.46 ± 3.95 |
| Preoperative EF, % | 56.41% ± 9.77 |
| NYHA class > II, n (%) | |
| Preoperative comorbidities | |
| COPD, n (%) | 920 (8.1%) |
| Hypertension, n (%) | 7.248 (64.2%) |
| Type II Diabetes, n (%) | 1.528 (13.5%) |
| Preoperative creatinine, mg/dL | 0.98 ± 0.67 |
| Chronic renal failure, n (%) | 1161 (10.2%) |
| Peripheral vasculopathy, n (%) | 2036 (18.0%) |
| Smoking habits, n (%) | 2443 (21.6%) |
| Stroke, n (%) | 989 (8.8%) |
| Timing of surgery | |
| Emergency or urgency, n (%) | 214 (1.9%) |
| Planned, n (%) | 11,071 (98.1%) |
| Surgery type | |
| Valvular surgery, n (%) | 5178 (45.88%) |
| Coronary surgery, n (%) | 1814 (16.07%) |
| Ascending aorta aneurysm surgery, n (%) | 420 (3.71%) |
| Other surgical procedures, n (%) | 999 (8.85%) |
| Combined surgery (two or more procedures), n (%) | 5564 (49.31%) |
| Models for Mortality | Models for NIMV | Models for PPC | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Preoperative models | Predictive Variable | Odds Ratio | 95% CI | p-Value | Predictive Variable | Odds Ratio | 95% CI | p-Value | Predictive Variable | Odds Ratio | 95% CI | p-Value |
| Age | 1.05 | 1.02–1.08 | <0.001 | Age | 1.04 | 1.02–1.06 | <0.001 | COPD | 2.63 | 1.31–5.28 | 0.007 | |
| Preoperative EF | 0.97 | 0.95–0.99 | 0.011 | Preoperative EF | 0.97 | 0.96–1.00 | 0.023 | Creatinine | 1.48 | 1.19–1.83 | <0.001 | |
| NYHA class | 2.97 | 1.63–5.41 | <0.001 | BMI | 1.10 | 1.05–1.15 | <0.001 | EF | 0.97 | 0.95–0.99 | 0.004 | |
| Elective surgery | 0.29 | 0.90–0.91 | 0.036 | Preoperative Creatinine | 1.26 | 1.01–1.58 | 0.043 | NYHA class | 1.81 | 1.05–3.14 | 0.033 | |
| Random effect variable | SD | SE | p | Random effect variable | SD | SE | p | Random effect variable | SD | SE | p | |
| Year of surgery | <0.001 | 0.37 | 1.000 | Year of surgery | 0.53 | 0.18 | <0.001 | Year of surgery | 0.28 | 0.20 | 0.176 | |
| Surgery models | Predictive Variable | Odds Ratio | 95% CI | p-Value | Predictive Variable | Odds Ratio | 95% CI | p-Value | Predictive Variable | Odds Ratio | 95% CI | p-Value |
| Inotropes in the operating room | 3.09 | 1.45–6.6 | 0.003 | Age | 1.04 | 1.02–1.06 | <0.001 | Inotropes in the operating room | 2.79 | 1.38–5.64 | 0.004 | |
| IABP in the operating room | 3.91 | 1.90–8.04 | <0.001 | Preoperative EF | 0.97 | 0.96–1.00 | 0.023 | IABP in the operating room | 2.64 | 1.02–6.81 | 0.045 | |
| Age | 1.06 | 1.03–1.10 | <0.001 | BMI | 1.10 | 1.05–1.15 | <0.001 | COPD | 3.74 | 1.64–8.51 | 0.002 | |
| NYHA class | 2.35 | 1.24–4.47 | 0.009 | Preoperative Creatinine | 1.26 | 1.01–1.58 | 0.043 | Preoperative creatinine | 1.39 | 1.07–1.81 | 0.014 | |
| Elective surgery | 0.22 | 0.08–0.65 | 0.006 | |||||||||
| Random effect variable | SD | SE | p | Random effect variable | SD | SE | p | Random effect variable | SD | SE | p | |
| Year of surgery | 0.24 | 0.30 | 0.320 | Year of surgery | 0.53 | 0.18 | <0.001 | Year of surgery | 0.53 | 0.25 | 1.329 | |
| ICU models | Predictive Variable | Odds Ratio | 95% CI | p-Value | Predictive Variable | Odds Ratio | 95% CI | p-Value | ||||
| Creatinine peak | 1.50 | 1.24–1.82 | <0.001 | Creatinine peak | 1.35 | 1.21–1.51 | <0.001 | |||||
| Tracheostomy | 18.08 | 7.14–45.76 | <0.001 | Inotropes | 1.60 | 1.25–2.04 | <0.001 | |||||
| Inotropes in the ICU in the ICU | 2.52 | 1.01–5.77 | 0.029 | P/F | 0.99 | 0.991–0.993 | <0.001 | |||||
| NYHA class | 2.79 | 1.35–5.78 | 0.006 | Blood transfusion | 2.41 | 1.87–3.13 | <0.001 | |||||
| Age | 1.08 | 1.03–1.12 | <0.001 | BMI | 1.07 | 1.05–1.11 | <0.001 | |||||
| P/F ratio | 0.1 | 0.99–0.1 | 0.028 | |||||||||
| Random effect variable | SD | SE | p | Random effect variable | SD | SE | p | |||||
| Year of surgery | <0.001 | 0.44 | 1.000 | Year of surgery | 0.83 | 0.18 | <0.001 | |||||
| Outcome | Incidence |
|---|---|
| Overall mortality, n (%) | 236 (2.1%) |
| Postoperative pulmonary complications, n (%) | 213 (1.9%) |
| Postoperative pulmonary complications (including the use of NIMV), n (%) | 821 (7.3%) |
| Need for NIMV before hospital discharge, n (%) | 609 (5.4%) |
| Re-intubation, n (%) | 97 (0.86%) |
| Inotropes, n (%) | 3809 (33.75%) |
| Intra-aortic balloon pump, n (%) | 395 (3.5%) |
| Blood products, n (%) | 2834 (18%) |
| Renal replacement therapy, n (%) | 175 (1.55%) |
| VA-ECMO support, n (%) | 12 (0.1%) |
| Septic shock, (%) | 56 (0.5%) |
| Length of ICU stay, days | 1 (1–3) |
| Length of hospital stay, days | 6 (5–8) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bignami, E.; Guarnieri, M.; Giambuzzi, I.; Trumello, C.; Saglietti, F.; Gianni, S.; Belluschi, I.; Di Tomasso, N.; Corti, D.; Alfieri, O.; et al. Three Logistic Predictive Models for the Prediction of Mortality and Major Pulmonary Complications after Cardiac Surgery. Medicina 2023, 59, 1368. https://doi.org/10.3390/medicina59081368
Bignami E, Guarnieri M, Giambuzzi I, Trumello C, Saglietti F, Gianni S, Belluschi I, Di Tomasso N, Corti D, Alfieri O, et al. Three Logistic Predictive Models for the Prediction of Mortality and Major Pulmonary Complications after Cardiac Surgery. Medicina. 2023; 59(8):1368. https://doi.org/10.3390/medicina59081368
Chicago/Turabian StyleBignami, Elena, Marcello Guarnieri, Ilaria Giambuzzi, Cinzia Trumello, Francesco Saglietti, Stefano Gianni, Igor Belluschi, Nora Di Tomasso, Daniele Corti, Ottavio Alfieri, and et al. 2023. "Three Logistic Predictive Models for the Prediction of Mortality and Major Pulmonary Complications after Cardiac Surgery" Medicina 59, no. 8: 1368. https://doi.org/10.3390/medicina59081368