
Association between a Marine Healing Program and Metabolic Syndrome Components and Mental Health Indicators
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
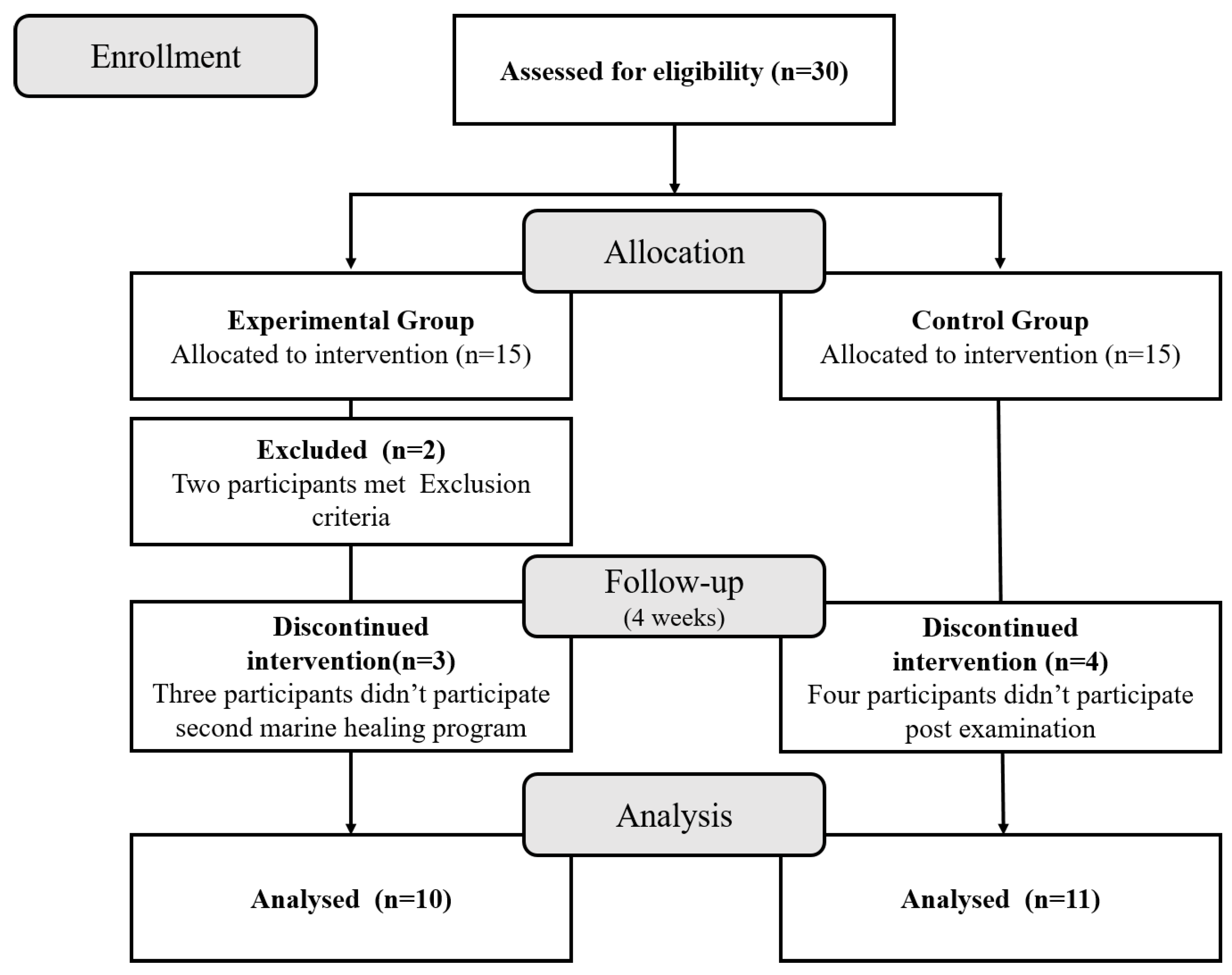
2.1. Participants
2.2. Study Design
2.3. Study Site
2.4. Program Setup and Progress
2.5. Anthropometric Indicators
2.6. Biochemical Indicators
2.7. Mental Health Indicators
2.8. Statistical Analysis
3. Results
3.1. Demographic and Clinical Data
3.2. Comparison of Pre- and Post-Test Results in the Experimental Group: Normal Variables
3.3. Comparison of Pre- and Post-Test Results in the Experimental Group: Non-Normal Variables
3.4. Comparison of Pre- and Post-Test Results in the Control Group: Normal Variables
3.5. Comparison of Pre- and Post-Test Results in the Control Group: Non-Normal Variables
3.6. Comparison of Pre- and Post-Test Results between the Experimental and Control Groups
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z. The metabolic syndrome. Lancet 2005, 365, 1415–1428. [Google Scholar] [CrossRef] [PubMed]
- Huang, P.L. A comprehensive definition for metabolic syndrome. Dis. Model. Mech. 2009, 2, 231–237. [Google Scholar] [CrossRef]
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.; Loria, C.M.; Smith, S.C., Jr. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef] [PubMed]
- Saklayen, M.G. The Global Epidemic of the Metabolic Syndrome. Curr. Hypertens. Rep. 2018, 20, 12. [Google Scholar] [CrossRef]
- Huh, J.H.; Kang, D.R.; Kim, J.Y.; Koh, K.K. Metabolic Syndrome Fact Sheet 2021: Executive Report. Cardiometab. Syndr. J. 2021, 1, 125–134. [Google Scholar] [CrossRef]
- Douma, S.; Petidis, K.; Doumas, M.; Papaefthimiou, P.; Triantafyllou, A.; Kartali, N.; Papadopoulos, N.; Vogiatzis, K.; Zamboulis, C. Prevalence of primary hyperaldosteronism in resistant hypertension: A retrospective observational study. Lancet 2008, 371, 1921–1926. [Google Scholar] [CrossRef]
- Mottillo, S.; Filion, K.B.; Genest, J.; Joseph, L.; Pilote, L.; Poirier, P.; Rinfret, S.; Schiffrin, E.L.; Eisenberg, M.J. The metabolic syndrome and cardiovascular risk a systematic review and meta-analysis. J. Am. Coll. Cardiol. 2010, 56, 1113–1132. [Google Scholar] [CrossRef]
- Esposito, K.; Chiodini, P.; Colao, A.; Lenzi, A.; Giugliano, D. Metabolic syndrome and risk of cancer: A systematic review and meta-analysis. Diabetes Care 2012, 35, 2402–2411. [Google Scholar] [CrossRef]
- Park, M.; Park, Y.; Kim, S.; Park, S.; Seol, H.; Woo, S.; Cho, S.; Lim, D.-S. Introduction and effectiveness of The Seoul Metabolic Syndrome Management. Public Health Aff. 2017, 1, 25–39. [Google Scholar] [CrossRef]
- Twohig-Bennett, C.; Jones, A. The health benefits of the great outdoors: A systematic review and meta-analysis of greenspace exposure and health outcomes. Environ Res 2018, 166, 628–637. [Google Scholar] [CrossRef]
- Ochiai, H.; Ikei, H.; Song, C.; Kobayashi, M.; Takamatsu, A.; Miura, T.; Kagawa, T.; Li, Q.; Kumeda, S.; Imai, M.; et al. Physiological and psychological effects of forest therapy on middle-aged males with high-normal blood pressure. Int. J. Environ. Res. Public Health 2015, 12, 2532–2542. [Google Scholar] [CrossRef]
- Ohtsuka, Y.; Yabunaka, N.; Takayama, S. Shinrin-yoku (forest-air bathing and walking) effectively decreases blood glucose levels in diabetic patients. Int. J. Biometeorol. 1998, 41, 125–127. [Google Scholar] [CrossRef]
- Lim, K.H.; Nam, K.J.; Rah, Y.C.; Cha, J.; Lee, S.J.; Lee, M.G.; Choi, J. The Effect of Natural Ocean Sound Exposure and Ocean-Side Relaxation on Chronic Tinnitus Patients: A Pilot Study in Korea. Ear Nose Throat J. 2021, 100, Np256–Np262. [Google Scholar] [CrossRef]
- Lee, S.H.H.J.; Lee, S.J.; Choi, H.Y.; Baek, J.H.; Kim, J.G. Comparison of seaweed pack and mudpack as treatment for knee osteoarthritis: A prospective randomized controlled study. Phys. Ther. Rehabil. Sci. 2019, 8, 22–31. [Google Scholar] [CrossRef]
- Kim, M.; Lee, K.H.; Han, S.H.; Lee, S.J.; Kim, C.G.; Choi, J.H.; Hwang, S.H.; Park, S.B. Effect of Peat Intervention on Pain and Gait in Patients with Knee Osteoarthritis: A Prospective, Double-Blind, Randomized, Controlled Study. Evid Based Complement Altern. Med. 2020, 2020, 8093526. [Google Scholar] [CrossRef] [PubMed]
- Park, H.-J.; Kong, E.-B.; Hong, S.-H.; Lee, A.-Y.; Lee, S.-J.; Hong, S.-C. The Effects of Peat-Pack Poultice and Salt Groundwater Foot Bath in Taean-gun on Depression and Pain in Single Parent Family. J. Korean Soc. Matern Child Health 2021, 25, 73–79. [Google Scholar] [CrossRef]
- Tschentscher, M.; Niederseer, D.; Niebauer, J. Health benefits of Nordic walking: A systematic review. Am. J. Prev. Med. 2013, 44, 76–84. [Google Scholar] [CrossRef]
- Oh, J.-H.; Hwang, N.-R.; Cha, Y.-J.; Lee, E.-B.; Choi, K.-H.; Seo, H.-J. The Reliability and Validity of the Korean Version of Behavioral Activation for Depression Scale. JKNA 2017, 56, 89–97. [Google Scholar] [CrossRef]
- Rabin, R.; de Charro, F. EQ-5D: A measure of health status from the EuroQol Group. Ann. Med. 2001, 33, 337–343. [Google Scholar] [CrossRef]
- Bae, J.M.; Jeong, E.K.; Yoo, T.W.; Huh, B.Y.; Kim, C.H. A quick measurement of stress in outpatient clinic setting. J. Korean Acad. Fam. Med. 1992, 13, 809–820. [Google Scholar]
- Donnelly, J.E.; Blair, S.N.; Jakicic, J.M.; Manore, M.M.; Rankin, J.W.; Smith, B.K. American College of Sports Medicine Position Stand. Appropriate physical activity intervention strategies for weight loss and prevention of weight regain for adults. Med. Sci. Sport. Exerc. 2009, 41, 459–471. [Google Scholar] [CrossRef]
- Lee, I.M.; Djoussé, L.; Sesso, H.D.; Wang, L.; Buring, J.E. Physical activity and weight gain prevention. JAMA 2010, 303, 1173–1179. [Google Scholar] [CrossRef] [PubMed]
- Jakicic, J.M.; Powell, K.E.; Campbell, W.W.; Dipietro, L.; Pate, R.R.; Pescatello, L.S.; Collins, K.A.; Bloodgood, B.; Piercy, K.L. Physical Activity and the Prevention of Weight Gain in Adults: A Systematic Review. Med. Sci. Sport. Exerc. 2019, 51, 1262–1269. [Google Scholar] [CrossRef] [PubMed]
- Thomas, D.M.; Bouchard, C.; Church, T.; Slentz, C.; Kraus, W.E.; Redman, L.M.; Martin, C.K.; Silva, A.M.; Vossen, M.; Westerterp, K.; et al. Why do individuals not lose more weight from an exercise intervention at a defined dose? An energy balance analysis. Obes. Rev. 2012, 13, 835–847. [Google Scholar] [CrossRef] [PubMed]
- Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [CrossRef] [PubMed]
- Aadahl, M.; Kjaer, M.; Jørgensen, T. Associations between overall physical activity level and cardiovascular risk factors in an adult population. Eur. J. Epidemiol. 2007, 22, 369–378. [Google Scholar] [CrossRef]
- Wing, R.R.; Lang, W.; Wadden, T.A.; Safford, M.; Knowler, W.C.; Bertoni, A.G.; Hill, J.O.; Brancati, F.L.; Peters, A.; Wagenknecht, L. Benefits of modest weight loss in improving cardiovascular risk factors in overweight and obese individuals with type 2 diabetes. Diabetes Care 2011, 34, 1481–1486. [Google Scholar] [CrossRef]
- Kodama, S.; Tanaka, S.; Saito, K.; Shu, M.; Sone, Y.; Onitake, F.; Suzuki, E.; Shimano, H.; Yamamoto, S.; Kondo, K.; et al. Effect of aerobic exercise training on serum levels of high-density lipoprotein cholesterol: A meta-analysis. Arch Intern. Med. 2007, 167, 999–1008. [Google Scholar] [CrossRef]
- Ostman, C.; Smart, N.A.; Morcos, D.; Duller, A.; Ridley, W.; Jewiss, D. The effect of exercise training on clinical outcomes in patients with the metabolic syndrome: A systematic review and meta-analysis. Cardiovasc. Diabetol. 2017, 16, 110. [Google Scholar] [CrossRef]
- Kim, M.S.; Kim, J.Y.; Choi, W.H.; Lee, S.S. Effects of seaweed supplementation on blood glucose concentration, lipid profile, and antioxidant enzyme activities in patients with type 2 diabetes mellitus. Nutr. Res. Pract. 2008, 2, 62–67. [Google Scholar] [CrossRef]
- Brewer, H.B., Jr. Increasing HDL Cholesterol Levels. N Engl. J. Med. 2004, 350, 1491–1494. [Google Scholar] [CrossRef] [PubMed]
- Hokanson, J.E.; Austin, M.A. Plasma triglyceride level is a risk factor for cardiovascular disease independent of high-density lipoprotein cholesterol level: A meta-analysis of population-based prospective studies. J. Cardiovasc. Risk 1996, 3, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Skinner, H.A.; Holt, S.; Schuller, R.; Roy, J.; Israel, Y. Identification of alcohol abuse using laboratory tests and a history of trauma. Ann. Intern. Med. 1984, 101, 847–851. [Google Scholar] [CrossRef] [PubMed]
- Peterson, K. Biomarkers for alcohol use and abuse--a summary. Alcohol. Res. Health 2004, 28, 30–37. [Google Scholar] [PubMed]
- Wannamethee, G.; Ebrahim, S.; Shaper, A.G. Gamma-glutamyltransferase: Determinants and association with mortality from ischemic heart disease and all causes. Am. J. Epidemiol. 1995, 142, 699–708. [Google Scholar] [CrossRef]
- Lee, D.S.; Evans, J.C.; Robins, S.J.; Wilson, P.W.; Albano, I.; Fox, C.S.; Wang, T.J.; Benjamin, E.J.; D’Agostino, R.B.; Vasan, R.S. Gamma glutamyl transferase and metabolic syndrome, cardiovascular disease, and mortality risk: The Framingham Heart Study. Arter. Thromb. Vasc. Biol. 2007, 27, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Yu Jeong, A.; Lee, J.-H.; Shin, S.-H.; Cho, H.-Y.; Yoo, M.; Shin, H.-J.; Kim, S.-H.; Kim, H.-J.; Yook, Y.-S.; Lee, S.-J. Effects of Meaning-Centered and Mindfulness-Based Stress Management Program with Using Marine Resources on the Improvement of Emotion, Sleep Quality, Quality of Life and Cognitive Function in Family Caregiver of Patients with Severe Physical Disability: Preliminary Study. Korean J. Psychosom. Med. 2019, 27, 191–201. [Google Scholar] [CrossRef]


{kind=link}
| Week 1 | Week 2 | Week 3 | Week 4 | |
|---|---|---|---|---|
| Lifestyle intervention | Experimental group | Experimental group | Experimental group | Experimental group |
| Control group | Control group | Control group | Control group | |
| Marine healing program (2 nights, 3 days) | Experimental group | Experimental group |
| 1st | 2nd | |||||
|---|---|---|---|---|---|---|
| Time | Oct 30 | Oct 31 | Nov 01 | Nov 10 | Nov 11 | Nov 12 |
| 07:30~ 08:30 | Breakfast (seaweed and low salt) | Breakfast (seaweed and low salt) | Breakfast (seaweed and low salt) | Post-test | ||
| 09:00~ 10:30 | PA in the pine forest | White sand Pilates | PA in the pine forest | |||
| 10:30~ 12:00 | Terrainkur on white sandy beach | Terrainkur on white sandy beach | Terrainkur on white sandy beach | |||
| 12:00~ 13:00 | Lunch (seaweed and low salt) | Lunch (seaweed and low salt) | Lunch (seaweed and low salt) | |||
| 13:00~ 14:00 | Orientation | Sea breeze aerosol | Orientation | Sea breeze aerosol | ||
| 14:00~ 15:00 | Medical examination | Medical examination | ||||
| 15:00~ 16:00 | Introduction to marine healing program | Tideland experience | Sea breeze aerosol | White sand Pilates | ||
| 16:00~ 17:00 | PA in the pine forest | Nordic walking at beach | Terrainkur on white sandy beach | |||
| 17:00~ 18:00 | ||||||
| 18:00~ 19:00 | Dinner (seaweed and low salt) | Dinner (seaweed and low salt) | Dinner (seaweed and low salt) | Dinner (seaweed and low salt) | ||
| 19:00~ 20:00 | Peat heat pack intervention | Aromatherapy | Peat heat pack intervention | Aromatherapy | ||
| Variable | Experimental | Control | p-Value | ||
|---|---|---|---|---|---|
| Average | SD | Average | SD | ||
| Sex F(M), n | 6(4) | 10(1) | 0.120 | ||
| Age (years) | 68.10 | 7.16 | 64.36 | 9.28 | 0.318 |
| Height (cm) | 157.87 | 7.08 | 153.46 | 7.31 | 0.178 |
| Body weight (kg) | 63.68 | 7.42 | 64.56 | 8.75 | 0.809 |
| WC (cm) | 92.25 | 6.11 | 94.96 | 7.08 | 0.363 |
| SMM (kg) | 24.61 | 5.24 | 21.33 | 3.20 | 0.096 |
| BFM (kg) | 20.41 | 7.10 | 25.06 | 8.39 | 0.189 |
| BMI (kg/m2) | 25.56 | 2.68 | 27.45 | 4.03 | 0.227 |
| PBF (%) | 31.81 | 9.20 | 38.24 | 8.85 | 0.119 |
| SBP (mmHg) | 152.70 | 22.34 | 148.27 | 22.86 | 0.659 |
| DBP (mmHg) | 81.60 | 15.95 | 82.27 | 19.95 | 0.933 |
| FBG (mg/dL) | 121.50 | 23.80 | 107.91 | 12.97 | 0.116 |
| HbA1c (%) | 5.70 | 0.72 | 5.92 | 0.66 | 0.479 |
| AST (IU/L) | 25.30 | 5.87 | 27.18 | 4.26 | 0.408 |
| ALT (IU/L) | 20.50 | 9.10 | 26.91 | 10.23 | 0.147 |
| Total cholesterol (mg/dL) | 176.30 | 45.87 | 167.73 | 35.96 | 0.637 |
| TG (mg/dL) | 113.10 | 57.22 | 103.73 | 33.43 | 0.648 |
| HDL-C (mg/dL) | 55.80 | 13.13 | 57.27 | 14.49 | 0.811 |
| LDL-C (mg/dL) | 101.80 | 39.63 | 96.73 | 34.68 | 0.758 |
| GGT (IU/L) | 20.20 | 7.97 | 24.73 | 11.42 | 0.31 |
| UAC (mg/dL) | 4.88 | 0.92 | 4.55 | 0.93 | 0.431 |
| HADS (score) | 10.80 | 7.33 | 12.27 | 6.92 | 0.641 |
| EQ-5D-3L (score) | 7.30 | 1.34 | 7.09 | 1.81 | 0.769 |
| BEPSI (score) | 9.40 | 2.63 | 10.27 | 3.50 | 0.529 |
| CSRS (score) | 10.60 | 13.01 | 8.91 | 8.96 | 0.730 |
| Variable | Average | SD | t | df | p-Value | |
|---|---|---|---|---|---|---|
| Height (cm) | pre | 157.87 | 1.33 | −0.74 | 9 | 0.479 |
| post | 158.18 | |||||
| Body weight (kg) | pre | 63.68 | 1.03 | 3.23 | 9 | 0.010 ** |
| post | 62.63 | |||||
| WC (cm) | pre | 92.25 | 4.18 | 1.02 | 9 | 0.333 |
| post | 90.90 | |||||
| SBP (mmHg) | pre | 152.70 | 17.29 | 3.38 | 9 | 0.008 ** |
| post | 134.20 | |||||
| DBP (mmHg) | pre | 81.60 | 13.71 | 0.81 | 9 | 0.440 |
| post | 78.10 | |||||
| FBG (mg/dL) | pre | 121.50 | 13.38 | 0.87 | 9 | 0.405 |
| post | 117.80 | |||||
| HbA1c (%) | pre | 5.70 | 0.2 | 2.26 | 9 | 0.050 * |
| post | 5.56 | |||||
| AST (IU/L) | pre | 25.30 | 3.28 | −0.87 | 9 | 0.408 |
| post | 26.20 | |||||
| Total cholesterol (mg/dL) | pre | 176.30 | 11.11 | 1.03 | 9 | 0.332 |
| post | 172.70 | |||||
| TG (mg/dL) | pre | 113.10 | 39.84 | 2.67 | 9 | 0.026 * |
| post | 79.50 | |||||
| HDL-C (mg/dL) | pre | 55.80 | 3.34 | −3.51 | 9 | 0.007 ** |
| post | 59.50 | |||||
| LDL-C (mg/dL) | pre | 101.80 | 10.56 | −0.03 | 9 | 0.977 |
| post | 101.90 | |||||
| UAC (mg/dL) | pre | 4.88 | 0.48 | −3.33 | 9 | 0.009 ** |
| post | 5.39 | |||||
| HADS (score) | pre | 10.80 | 4.84 | 2.29 | 9 | 0.048 * |
| post | 7.30 | |||||
| EQ-5D-3L (score) | pre | 7.30 | 1.78 | 2.49 | 9 | 0.034 * |
| post | 5.90 |
| Variable | Average | SD | t | df | p-Value | |
|---|---|---|---|---|---|---|
| Body weight (kg) | pre | 64.56 | 8.75 | −1.73 | 10 | 0.115 |
| post | 64.85 | 8.98 | ||||
| SMM (kg) | pre | 21.33 | 3.20 | −1.70 | 10 | 0.120 |
| post | 22.13 | 3.06 | ||||
| BFM (kg) | pre | 25.06 | 8.39 | 1.36 | 10 | 0.204 |
| post | 23.97 | 8.08 | ||||
| PBF (%) | pre | 38.24 | 8.85 | 1.42 | 10 | 0.186 |
| post | 36.38 | 8.51 | ||||
| HbA1c (%) | pre | 5.92 | 0.66 | 1.58 | 10 | 0.146 |
| post | 5.84 | 0.64 | ||||
| AST (IU/L) | pre | 27.18 | 4.26 | −0.99 | 10 | 0.344 |
| post | 28.36 | 4.93 | ||||
| ALT (IU/L) | pre | 26.91 | 10.23 | −1.17 | 10 | 0.267 |
| post | 28.00 | 11.53 | ||||
| Total cholesterol (mg/dL) | pre | 167.73 | 35.96 | 2.50 | 10 | 0.031 * |
| post | 156.55 | 33.80 | ||||
| HDL-C (mg/dL) | pre | 57.27 | 14.49 | 0.49 | 10 | 0.633 |
| post | 56.36 | 11.49 | ||||
| UAC (mg/dL) | pre | 4.55 | 0.93 | −1.65 | 10 | 0.130 |
| post | 4.74 | 0.93 | ||||
| HADS (score) | pre | 12.27 | 6.92 | 2.45 | 10 | 0.034 * |
| post | 7.82 | 5.74 | ||||
| CSRS (score) | pre | 8.91 | 8.96 | −0.12 | 10 | 0.910 |
| post | 9.27 | 9.47 |
| Variable | Group | Pre-Test | Post-Test | Pre-Post | t | df | p-Value | ||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||||||
| Body weight (kg) | Exp. | 63.68 | 7.42 | 62.63 | 6.73 | 1.05 | 3.761 | 19 | 0.001 *** |
| Cont. | 64.56 | 8.75 | 64.85 | 8.98 | −0.29 | ||||
| HbA1c (%) | Exp. | 5.70 | 0.72 | 5.56 | 0.65 | 0.14 | 0.725 | 19 | 0.477 |
| Cont. | 5.92 | 0.66 | 5.84 | 0.64 | 0.08 | ||||
| AST (IU/L) | Exp. | 25.30 | 5.87 | 26.20 | 4.42 | −0.90 | 0.177 | 19 | 0.861 |
| Cont. | 27.18 | 4.26 | 28.36 | 4.93 | −1.18 | ||||
| Total cholesterol (mg/dL) | Exp. | 176.30 | 45.87 | 172.70 | 44.71 | 3.60 | −1.314 | 19 | 0.204 |
| Cont. | 167.73 | 35.96 | 156.55 | 33.80 | 11.18 | ||||
| HDL-C (mg/dL) | Exp. | 55.80 | 13.13 | 59.50 | 10.98 | −3.70 | −2.168 | 15.73 | 0.046 * |
| Cont. | 57.27 | 14.49 | 56.36 | 11.49 | 0.91 | ||||
| UAC (mg/dL) | Exp. | 4.88 | 0.92 | 5.39 | 0.84 | −0.51 | −1.764 | 19 | 0.094 |
| Cont. | 4.55 | 0.93 | 4.74 | 0.93 | −0.18 | ||||
| HADS (score) | Exp. | 10.80 | 7.33 | 7.30 | 6.31 | 3.50 | −0.398 | 19 | 0.695 |
| Cont. | 12.27 | 6.92 | 7.82 | 5.74 | 4.46 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Byeon, W.-J.; Lee, S.-J.; Khil, T.-G.; Jeong, A.-Y.; Han, B.-D.; Sohn, M.-S.; Choi, J.-W.; Kim, Y.-H. Association between a Marine Healing Program and Metabolic Syndrome Components and Mental Health Indicators. Medicina 2023, 59, 1263. https://doi.org/10.3390/medicina59071263
Byeon W-J, Lee S-J, Khil T-G, Jeong A-Y, Han B-D, Sohn M-S, Choi J-W, Kim Y-H. Association between a Marine Healing Program and Metabolic Syndrome Components and Mental Health Indicators. Medicina. 2023; 59(7):1263. https://doi.org/10.3390/medicina59071263
Chicago/Turabian StyleByeon, Woo-Jin, Sung-Jae Lee, Tae-Gyu Khil, Ah-Young Jeong, Byoung-Duck Han, Min-Sung Sohn, Jae-Wook Choi, and Yang-Hyun Kim. 2023. "Association between a Marine Healing Program and Metabolic Syndrome Components and Mental Health Indicators" Medicina 59, no. 7: 1263. https://doi.org/10.3390/medicina59071263