
Evaluation of Paraspinal Muscle Degeneration on Pain Relief after Percutaneous Epidural Adhesiolysis in Patients with Degenerative Lumbar Spinal Disease

Abstract
:1. Introduction
2. Materials and Methods
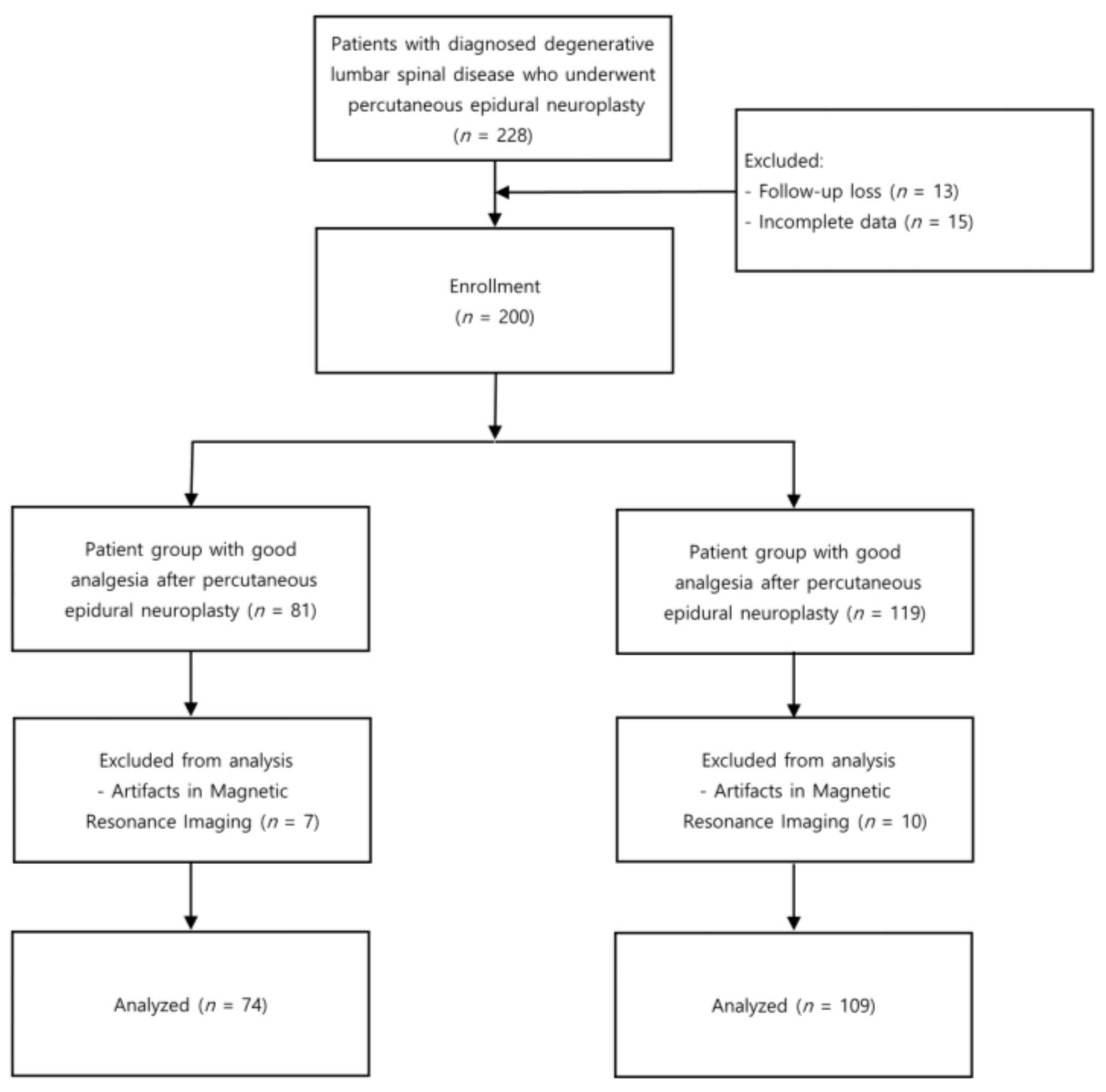
2.1. Study Population
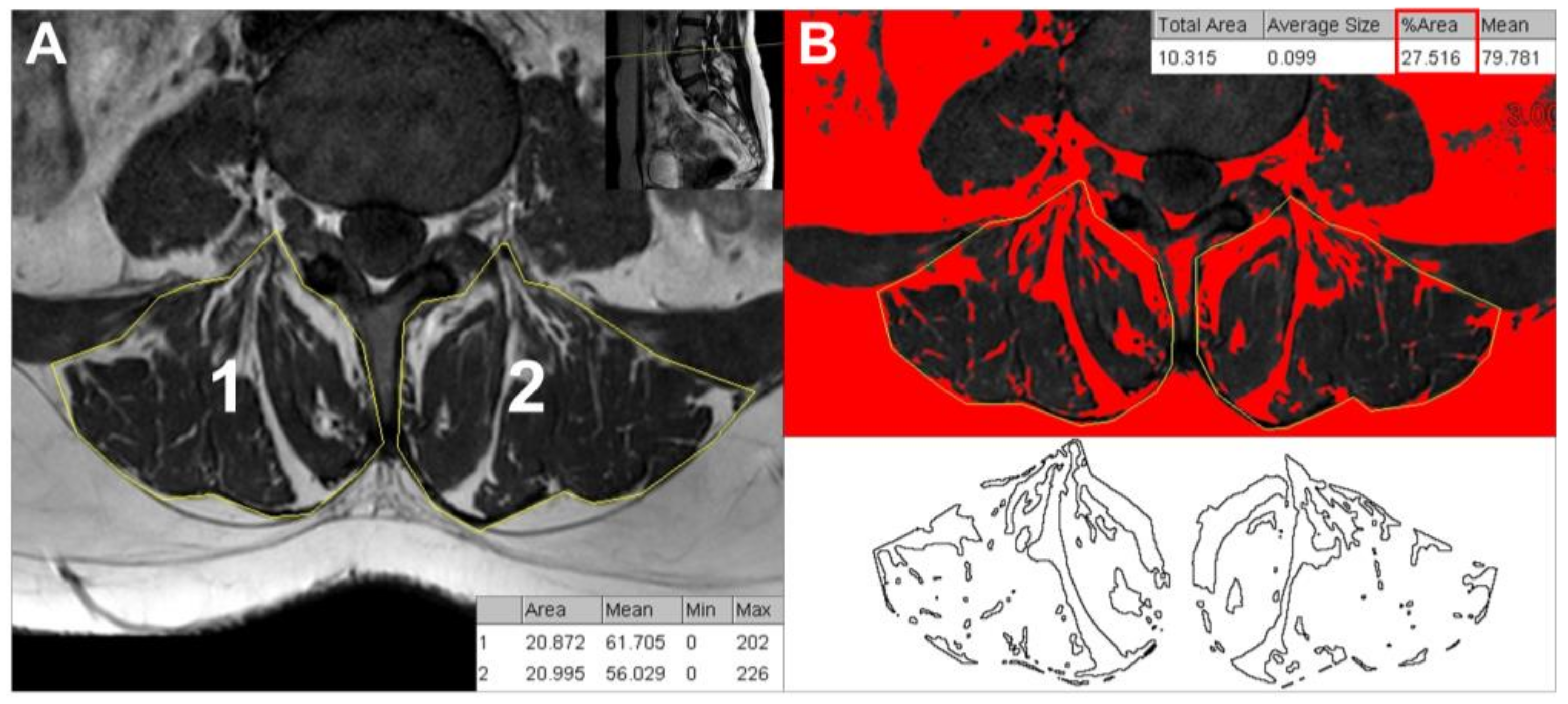
2.2. CSA and Fatty Infiltration Measures
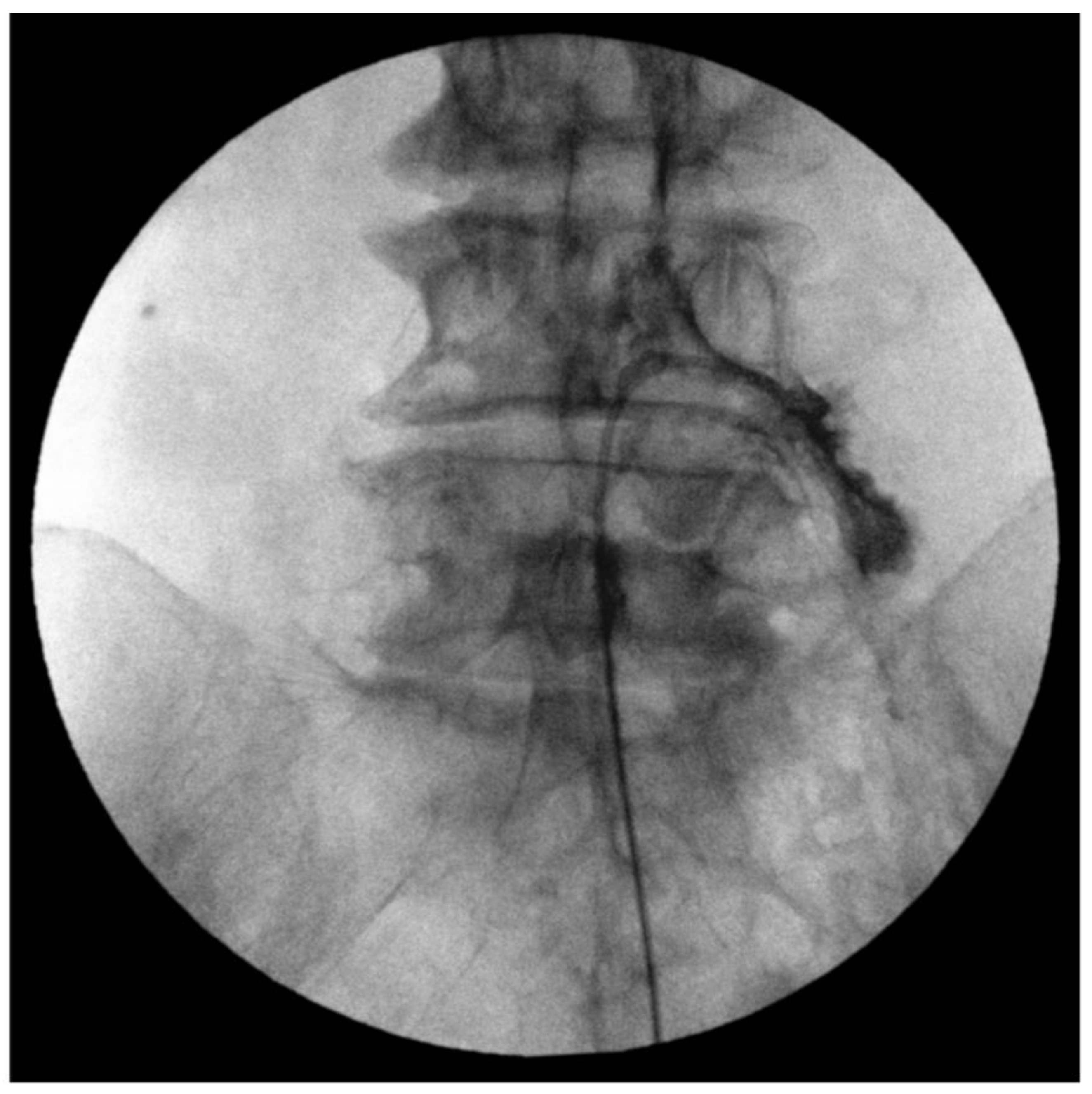
2.3. Fluoroscopy-Guided Lumbar Percutaneous Epidural Adhesiolysis
2.4. Patient Characteristics and Clinical Data Measurements
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [Green Version]
- Weiner, D.K.; Haggerty, C.L.; Kritchevsky, S.B.; Harris, T.; Simonsick, E.M.; Nevitt, M.; Newman, A.; Health, Aging, and Body Composition Research Group. How does low back pain impact physical function in independent, well-functioning older adults? Evidence from the Health ABC Cohort and implications for the future. Pain Med. 2003, 4, 311–320. [Google Scholar] [CrossRef] [Green Version]
- Lee, F.; Jamison, D.E.; Hurley, R.W.; Cohen, S.P. Epidural lysis of adhesions. Korean J. Pain 2014, 27, 3–15. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Correa-De-Araujo, R.; Addison, O.; Miljkovic, I.; Goodpaster, B.H.; Bergman, B.C.; Clark, R.V.; Elena, J.W.; Esser, K.A.; Ferrucci, L.; Harris-Love, M.O.; et al. Myosteatosis in the Context of Skeletal Muscle Function Deficit: An Interdisciplinary Workshop at the National Institute on Aging. Front. Physiol. 2020, 11, 963. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Rho, M.; Yoon, K.B.; Jo, M.; Lee, D.W.; Kim, S.H. Influence of cross-sectional area and fat infiltration of paraspinal muscles on analgesic efficacy of epidural steroid injection in elderly patients. Pain Pr. 2022, 22, 621–630. [Google Scholar] [CrossRef] [PubMed]
- Xie, D.; Zhang, J.; Ding, W.; Yang, S.; Yang, D.; Ma, L.; Zhang, J. Abnormal change of paravertebral muscle in adult degenerative scoliosis and its association with bony structural parameters. Eur. Spine J. 2019, 28, 1626–1637. [Google Scholar] [CrossRef]
- Chen, J.; Li, J.; Sheng, B.; Li, L.; Wu, S. Does preoperative morphology of multifidus influence the surgical outcomes of stand-alone lateral lumbar interbody fusion for lumbar spondylolisthesis? Clin. Neurol. Neurosurg. 2022, 215, 107177. [Google Scholar] [CrossRef]
- Park, S.-H.; Ji, G.Y.; Cho, P.G.; Shin, D.A.; Yoon, Y.S.; Kim, K.N.; Oh, C.H. Clinical Significance of Epidurography Contrast Patterns after Adhesiolysis during Lumbar Percutaneous Epidural Neuroplasty. Pain Res. Manag. 2018, 2018, 6268045. [Google Scholar] [CrossRef] [Green Version]
- Chang, M.C.; Lee, D.G. Outcome of Transforaminal Epidural Steroid Injection According to the Severity of Lumbar Foraminal Spinal Stenosis. Pain Physician 2018, 21, 67–72. [Google Scholar] [CrossRef]
- Lee, G.Y.; Lee, J.W.; Choi, H.S.; Oh, K.J.; Kang, H.S. A new grading system of lumbar central canal stenosis on MRI: An easy and reliable method. Skelet. Radiol. 2011, 40, 1033–1039. [Google Scholar] [CrossRef] [Green Version]
- Farrar, J.T.; Young, J.P., Jr.; LaMoreaux, L.; Werth, J.L.; Poole, R.M. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain 2001, 94, 149–158. [Google Scholar] [CrossRef]
- Choi, E.; Nahm, F.; Lee, P.-B. Evaluation of prognostic predictors of percutaneous adhesiolysis using a Racz catheter for post lumbar surgery syndrome or spinal stenosis. Pain Physician 2013, 16, E531–E536. [Google Scholar] [PubMed]
- Perkisas, S.; Lamers, S.; Degerickx, R.; Van Mieghem, E.; Vandewoude, M.; Verhoeven, V.; De Cock, A.-M. The relation between mortality, intramuscular adipose tissue and sarcopenia in hospitalized geriatric patients. Eur. Geriatr. Med. 2018, 9, 801–807. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Yu, K.; Shyh-Chang, N.; Jiang, Z.; Liu, T.; Ma, S.; Luo, L.; Guang, L.; Liang, K.; Ma, W.; et al. Pathogenesis of sarcopenia and the relationship with fat mass: Descriptive review. J. Cachex-Sarcopenia Muscle 2022, 13, 781–794. [Google Scholar] [CrossRef]
- Hysing, E.-B.; Smith, L.; Thulin, M.; Karlsten, R.; Bothelius, K.; Gordh, T. Detection of systemic inflammation in severely impaired chronic pain patients and effects of a multimodal pain rehabilitation program. Scand. J. Pain 2019, 19, 235–244. [Google Scholar] [CrossRef]
- James, G.; Chen, X.; Diwan, A.; Hodges, P.W. Fat infiltration in the multifidus muscle is related to inflammatory cytokine expression in the muscle and epidural adipose tissue in individuals undergoing surgery for intervertebral disc herniation. Eur. Spine J. 2021, 30, 837–845. [Google Scholar] [CrossRef]
- Gellhorn, A.C.; Suri, P.; Rundell, S.D.; Olafsen, N.; Carlson, M.J.; Johnson, S.; Fry, A.; Annaswamy, T.M.; Gilligan, C.; Comstock, B.; et al. Lumbar Muscle Cross-Sectional Areas Do Not Predict Clinical Outcomes in Adults with Spinal Stenosis: A Longitudinal Study. PMR 2017, 9, 545–555. [Google Scholar] [CrossRef]
- Stanuszek, A.; Jędrzejek, A.; Gancarczyk-Urlik, E.; Kołodziej, I.; Pisarska-Adamczyk, M.; Milczarek, O.; Trompeta, J.; Chrobak, W. Preoperative paraspinal and psoas major muscle atrophy and paraspinal muscle fatty degeneration as factors influencing the results of surgical treatment of lumbar disc disease. Arch. Orthop. Trauma Surg. 2022, 142, 1375–1384. [Google Scholar] [CrossRef]
- Crawford, R.J.; Volken, T.; Ni Mhuiris, Á.; Bow, C.C.; Elliott, J.M.; Hoggarth, M.A.; Samartzis, D. Geography of Lumbar Paravertebral Muscle Fatty Infiltration: The Influence of Demographics, Low Back Pain, and Disability. Spine 2019, 44, 1294–1302. [Google Scholar] [CrossRef]
- Urrutia, J.; Besa, P.; Lobos, D.; Campos, M.; Arrieta, C.; Andia, M.; Uribe, S. Lumbar paraspinal muscle fat infiltration is independently associated with sex, age, and inter-vertebral disc degeneration in symptomatic patients. Skelet. Radiol. 2018, 47, 955–961. [Google Scholar] [CrossRef]
- Kim, H.-K.; Kim, C.-H. Quality Matters as Much as Quantity of Skeletal Muscle: Clinical Implications of Myosteatosis in Cardiometabolic Health. Endocrinol. Metab. 2021, 36, 1161–1174. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Park, S.W.; Kim, Y.B.; Nam, T.K.; Lee, Y.S. The fatty degeneration of lumbar paraspinal muscles on computed tomography scan according to age and disc level. Spine J. 2017, 17, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Crawford, R.J.; Elliott, J.M.; Volken, T. Change in fatty infiltration of lumbar multifidus, erector spinae, and psoas muscles in asymptomatic adults of Asian or Caucasian ethnicities. Eur. Spine J. 2017, 26, 3059–3067. [Google Scholar] [CrossRef] [PubMed]
- Hsu, E.; Atanelov, L.; Plunkett, A.R.; Chai, N.; Chen, Y.; Cohen, S.P. Epidural Lysis of Adhesions for Failed Back Surgery and Spinal Stenosis. Obstet. Anesth. Dig. 2014, 118, 215–224. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Age < 65 Group | p-Value | Age ≥ 65 Group | p-Value | ||
|---|---|---|---|---|---|---|
| Good Analgesia (n = 36) | Poor Analgesia (n = 40) | Good Analgesia (n = 38) | Poor Analgesia (n = 69) | |||
| Patient characteristics | ||||||
| Age, years | 53.69 ± 8.97 (33–64) | 55.30 ± 9.26 (24–64) | 0.446 | 75.29 ± 6.73 (65–91) | 73.90 ± 5.68 (65–88) | 0.259 |
| Sex, M/F | 21 (58.3%) /15 (41.7%) | 18 (45.0%) /22 (55.0%) | 0.246 | 16 (42.1%) /22 (57.9%) | 28 (40.6%) /41 (59.4%) | 0.878 |
| Body mass index, kg/m2 | 24.30 (22.99;27.00) | 24.88 (22.47;26.19) | 0.999 | 25.15 (23.26;26.78) | 24.21 (23.28;27.12) | 0.728 |
| <25 | 22 (61.1%) | 21 (52.5%) | 0.450 | 17 (44.7%) | 42 (60.9%) | 0.108 |
| ≥25 | 14 (38.9%) | 19 (47.5%) | 21 (55.3%) | 27 (39.1%) | ||
| Comorbid medical disease, n | ||||||
| Cardiovascular disease | 10 (27.8%) | 15 (37.5%) | 0.465 | 34 (89.5%) | 60 (87.0%) | 0.703 |
| Diabetes mellitus | 5 (13.9%) | 5 (12.8%) | 0.892 | 15 (39.5%) | 20 (29.0%) | 0.268 |
| Osteopenia/osteoporosis | 1 (2.8%) | 2 (5.0%) | 0.622 | 4 (10.5%) | 5 (7.2%) | 0.560 |
| Spine surgery history, n | 9 (25.0%) | 6 (15.0%) | 0.277 | 6 (15.8%) | 10 (14.5%) | 0.857 |
| Pain-related data | ||||||
| Pain duration, months | 3.00 (1.00;10.75) | 4.50 (2.00;12.00) | 0.143 | 6.00 (2.00;12.00) | 7.00 (3.00;30.00) | 0.305 |
| Baseline pain score, NRS 0–10 | 7.42 ± 1.68 | 6.48 ± 2.08 | 0.034 | 7.34 ± 1.76 | 5.70 ± 1.79 | <0.001 |
| NRS < 7 | 10 (27.8%) | 20 (50.0%) | 0.048 | 13 (34.2%) | 46 (66.7%) | 0.001 |
| NRS ≥ 7 | 26 (72.2%) | 20 (50.0%) | 25 (65.8%) | 23 (33.3%) | ||
| Opioid usage, n | 23 (63.9%) | 29 (72.5%) | 0.466 | 32 (84.2%) | 51 (73.9%) | 0.222 |
| Presence of NIC, n | 12 (33.3%) | 13 (32.5%) | 0.938 | 20 (52.6%) | 44 (63.8%) | 0.261 |
| Presence of radiating pain, n | 33 (91.7%) | 38 (95.0%) | 0.558 | 38 (100.0%) | 63 (91.3%) | 0.061 |
| Good effect of previous ESI, n | 16 (44.4%) | 16 (40.0%) | 0.817 | 18 (47.4%) | 33 (47.8%) | 0.964 |
| Pre-procedural MRI findings, n | ||||||
| Herniated disc | 31 (86.1%) | 37 (92.5%) | 0.365 | 37 (97.4%) | 62 (89.9%) | 0.157 |
| Foraminal stenosis | 0.999 | 0.264 | ||||
| None to mild | 27 (75.0%) | 30 (75.0%) | 15 (39.5%) | 35 (50.7%) | ||
| Moderate to severe | 9 (25.0%) | 10 (25.0%) | 23 (60.5%) | 34 (49.3%) | ||
| Central stenosis | 0.594 | 0.096 | ||||
| None to mild | 29 (80.6%) | 30 (75.0%) | 24 (63.2%) | 32 (46.4%) | ||
| Moderate to severe | 7 (19.4%) | 10 (25.0%) | 14 (36.8%) | 37 (53.6%) | ||
| Spondylolisthesis | 4 (11.1%) | 4 (10.0%) | 0.876 | 4 (10.5%) | 18 (26.1%) | 0.058 |
| Transition to spine surgery within 1 year, n | 6 (16.7%) | 7 (17.9%) | 0.884 | 8 (21.1%) | 12 (17.6%) | 0.667 |
| Paraspinal muscle CSA, cm2 | ||||||
| Right | 21.98 ± 4.87 | 20.81 ± 5.90 | 0.351 | 18.99 ± 3.44 | 19.82 ± 3.93 | 0.275 |
| Left | 21.87 ± 4.92 | 20.94 ± 6.00 | 0.461 | 18.43 ± 4.52 | 19.05 ± 4.00 | 0.462 |
| Total | 43.85 ± 9.55 | 41.74 ± 11.77 | 0.397 | 37.42 ± 7.53 | 38.87 ± 7.73 | 0.349 |
| Fatty infiltration% | ||||||
| Right | 0.281 | 0.053 | ||||
| <10% | 8 (22.2%) | 7 (17.5%) | 5 (13.2%) | 15 (21.7%) | ||
| 10–50% | 22 (61.1%) | 20 (50.0%) | 23 (60.5%) | 25 (36.2%) | ||
| ≥50% | 6 (16.7%) | 13 (32.5%) | 10 (26.3%) | 29 (42.0%) | ||
| Left | 0.429 | 0.016 | ||||
| <10% | 7 (19.4%) | 13 (32.5%) | 13 (34.2%) | 11 (15.9%) | ||
| 10–50% | 22 (61.1%) | 21 (52.5%) | 23 (60.5%) | 46 (66.7%) | ||
| ≥50% | 7 (19.4%) | 6 (15.0%) | 2 (5.3%) | 12 (17.4%) | ||
| Total | 0.785 | 0.029 | ||||
| <10% | 7 (19.4%) | 10 (25.0%) | 9 (23.7%) | 8 (11.6%) | ||
| 10–50% | 22 (61.1%) | 24 (60.0%) | 25 (65.8%) | 43 (62.3%) | ||
| ≥50% | 7 (19.4%) | 6 (15.0%) | 4 (10.5%) | 18 (26.1%) | ||
| Male | Female | |||||
|---|---|---|---|---|---|---|
| Age ≥ 65 group | Good analgesia (n = 16) | Poor analgesia (n = 28) | p-value | Good analgesia (n = 22) | Poor analgesia (n = 41) | p-value |
| Paraspinal muscle CSA, cm2 | 40.54 ± 6.70 | 42.89 ± 7.65 | 0.313 | 35.15 ± 7.41 | 36.13 ± 6.58 | 0.588 |
| Fatty infiltration% | 0.895 | 0.040 | ||||
| <10% | 4 (25.0%) | 5 (17.9%) | 5 (22.7%) | 3 (7.3%) | ||
| 10–50% | 10 (62.5%) | 19 (67.9%) | 15 (68.2%) | 24 (58.5%) | ||
| ≥50% | 2 (12.5%) | 4 (14.3%) | 2 (9.1%) | 14 (34.1%) | ||
| Age < 65 group | Good analgesia (n = 21) | Poor analgesia (n = 18) | p-value | Good analgesia (n = 15) | Poor analgesia (n = 22) | p-value |
| Paraspinal muscle CSA, cm2 | 49.78 ± 12.22 | 48.71 ± 8.53 | 0.749 | 37.05 ± 6.25 | 35.16 ± 5.97 | 0.360 |
| Fatty infiltration% | 0.646 | 0.789 | ||||
| <10% | 6 (28.6%) | 7 (38.9%) | 1 (6.7%) | 3 (13.6%) | ||
| 10–50% | 12 (57.1%) | 10 (55.6%) | 10 (66.7%) | 14 (63.6%) | ||
| ≥50% | 3 (14.3%) | 1 (5.6%) | 4 (26.7%) | 5 (22.7%) | ||
| Adjusted Odds Ratio | 95% Confidence Intervals | p-Value | |
|---|---|---|---|
| Baseline pain score, <7 on NRS | 4.039 | 1.594–10.233 | 0.003 |
| Spondylolisthesis, yes | 4.074 | 1.144–14.511 | 0.030 |
| Total fatty infiltration% | |||
| <10% (reference) | 1.000 | ||
| ≥50% | 6.576 | 1.300–33.268 | 0.023 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, M.; Kim, S.H.; Jo, M.; Jung, H.E.; Bae, J.; Kim, H.J. Evaluation of Paraspinal Muscle Degeneration on Pain Relief after Percutaneous Epidural Adhesiolysis in Patients with Degenerative Lumbar Spinal Disease. Medicina 2023, 59, 1118. https://doi.org/10.3390/medicina59061118
Kang M, Kim SH, Jo M, Jung HE, Bae J, Kim HJ. Evaluation of Paraspinal Muscle Degeneration on Pain Relief after Percutaneous Epidural Adhesiolysis in Patients with Degenerative Lumbar Spinal Disease. Medicina. 2023; 59(6):1118. https://doi.org/10.3390/medicina59061118
Chicago/Turabian StyleKang, Misun, Shin Hyung Kim, Minju Jo, Hyun Eom Jung, Jungbin Bae, and Hee Jung Kim. 2023. "Evaluation of Paraspinal Muscle Degeneration on Pain Relief after Percutaneous Epidural Adhesiolysis in Patients with Degenerative Lumbar Spinal Disease" Medicina 59, no. 6: 1118. https://doi.org/10.3390/medicina59061118