
Revision Total Hip Arthroplasty Utilizing an Acetabular Reinforcement Ring with a Metal Augment: A Minimum Eight-Year Follow-Up Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection and Data Collection
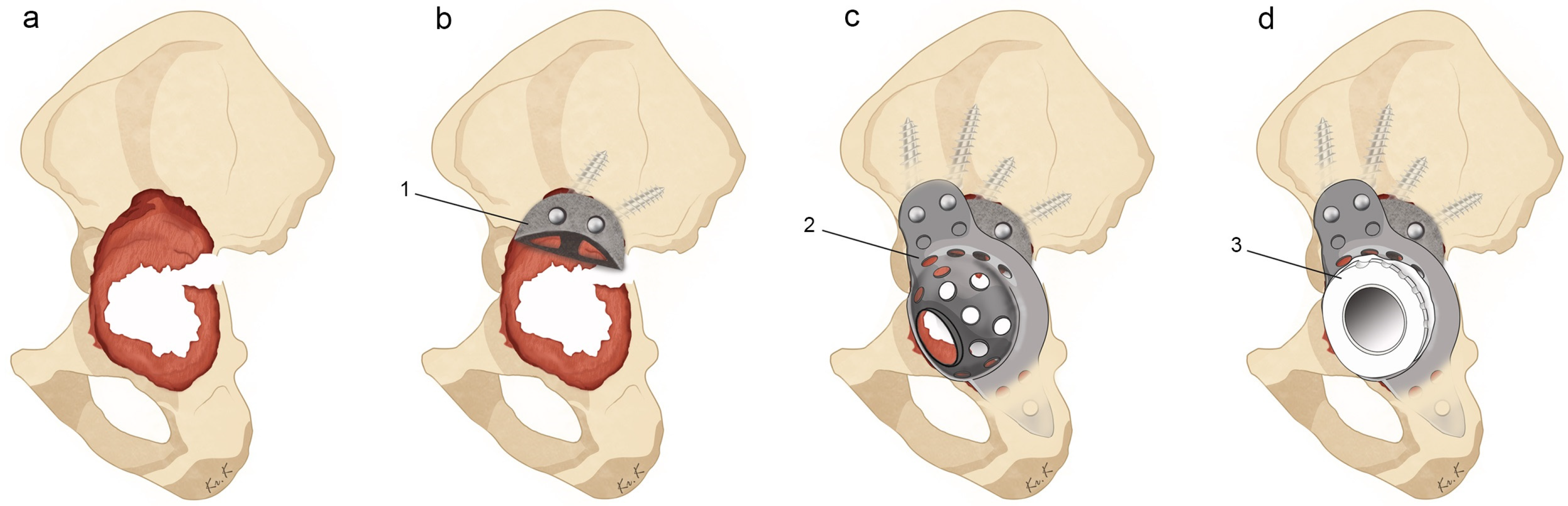
2.2. Surgical Technique
2.3. Postoperative Management
2.4. Statistics
3. Results
3.1. Patient Demographics
3.2. Surgical Details and Postoperative Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pulido, L.; Rachala, S.R.; Cabanela, M.E. Cementless acetabular revision: Past, present, and future. Revision total hip arthroplasty: The acetabular side using cementless implants. Int. Orthop. 2011, 35, 289–298. [Google Scholar] [CrossRef]
- Kurtz, S.M.; Ong, K.L.; Lau, E.; Bozic, K.J. Impact of the economic downturn on total joint replacement demand in the United States: Updated projections to 2021. J. Bone Jt. Surg. Am. 2014, 96, 624–630. [Google Scholar] [CrossRef] [PubMed]
- Kurtz, S.; Ong, K.; Lau, E.; Mowat, F.; Halpern, M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J. Bone Jt. Surg. Am. 2007, 89, 780–785. [Google Scholar] [CrossRef]
- Kummerant, J.; Wirries, N.; Derksen, A.; Budde, S.; Windhagen, H.; Floerkemeier, T. The etiology of revision total hip arthroplasty: Current trends in a retrospective survey of 3450 cases. Arch. Orthop. Trauma. Surg. 2020, 140, 1265–1273. [Google Scholar] [CrossRef] [PubMed]
- Riviere, C.; Vendittoli, P.A. (Eds.) Personalized Hip and Knee Joint Replacement; Springer: Cham, Switzerland, 2020. [Google Scholar]
- Zhang, R.; Lin, J.; Chen, F.; Liu, W.; Chen, M. Clinical and radiological outcomes in three-dimensional printing assisted revision total hip and knee arthroplasty: A systematic review. J. Orthop. Surg. Res. 2021, 16, 495. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Liu, Y.B.; Ma, M.Y.; Cao, Z.; Kong, X.P.; Chai, W. Revision Total Hip Arthroplasty with Severe Acetabular Defect: A Preliminary Exploration and Attempt of Robotic-Assisted Technology. Orthop. Surg. 2022, 14, 1912–1917. [Google Scholar] [CrossRef]
- Berry, D.J.; Lewallen, D.G.; Hanssen, A.D.; Cabanela, M.E. Pelvic discontinuity in revision total hip arthroplasty. J. Bone Jt. Surg. Am. 1999, 81, 1692–1702. [Google Scholar] [CrossRef]
- Totoribe, K.; Chosa, E.; Yamako, G.; Zhao, X.; Ouchi, K.; Hamada, H.; Deng, G. Acetabular reinforcement ring with additional hook improves stability in three-dimensional finite element analyses of dysplastic hip arthroplasty. J. Orthop. Surg. Res. 2018, 13, 313. [Google Scholar] [CrossRef]
- Chen, W.M.; Engh, C.A.J.; Hopper, R.H.J.; McAuley, J.P.; Engh, C.A. Acetabular revision with use of a bilobed component inserted without cement in patients who have acetabular bone-stock deficiency. J. Bone Jt. Surg. Am. 2000, 82, 197–206. [Google Scholar] [CrossRef]
- Patel, J.V.; Masonis, J.L.; Bourne, R.B.; Rorabeck, C.H. The fate of cementless jumbo cups in revision hip arthroplasty. J. Arthroplast. 2003, 18, 129–133. [Google Scholar] [CrossRef]
- Bozic, K.J.; Freiberg, A.A.; Harris, W.H. The high hip center. Clin. Orthop. Relat. Res. 2004, 420, 101–105. [Google Scholar] [CrossRef]
- Fryhofer, G.W.; Ramesh, S.; Sheth, N.P. Acetabular reconstruction in revision total hip arthroplasty. J. Clin. Orthop. Trauma. 2020, 11, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Baauw, M.; van Hooff, M.L.; Spruit, M. Current Construct Options for Revision of Large Acetabular Defects: A Systematic Review. JBJS Rev. 2016, 4, e2. [Google Scholar] [CrossRef] [PubMed]
- Gibon, E.; Kerboull, L.; Courpied, J.P.; Hamadouche, M. Acetabular reinforcement rings associated with allograft for severe acetabular defects. Int. Orthop. 2019, 43, 561–571. [Google Scholar] [CrossRef]
- Rosson, J.; Schatzker, J. The use of reinforcement rings to reconstruct deficient acetabula. J. Bone Jt. Surg. Br. Vol. 1992, 74, 716–720. [Google Scholar] [CrossRef] [PubMed]
- Gross, A.E.; Goodman, S. The current role of structural grafts and cages in revision arthroplasty of the hip. Clin. Orthop. Relat. Res. 2004, 429, 193–200. [Google Scholar] [CrossRef]
- Goodman, S.; Saastamoinen, H.; Shasha, N.; Gross, A. Complications of ilioischial reconstruction rings in revision total hip arthroplasty. J. Arthroplast. 2004, 19, 436–446. [Google Scholar] [CrossRef]
- Gerber, A.; Pisan, M.; Zurakowski, D.; Isler, B. Ganz reinforcement ring for reconstruction of acetabular defects in revision total hip arthroplasty. J. Bone Jt. Surg. Am. 2003, 85, 2358–2364. [Google Scholar] [CrossRef]
- Hsu, C.C.; Hsu, C.H.; Yen, S.H.; Wang, J.W. Use of the Burch-Schneider cage and structural allografts in complex acetabular deficiency: 3- to 10-year follow up. Kaohsiung J. Med. Sci. 2015, 31, 540–547. [Google Scholar] [CrossRef]
- Makinen, T.J.; Fichman, S.G.; Watts, E.; Kuzyk, P.R.; Safir, O.A.; Gross, A.E. The role of cages in the management of severe acetabular bone defects at revision arthroplasty. Bone Jt. J. 2016, 98-B, 73–77. [Google Scholar] [CrossRef]
- Regis, D.; Sandri, A.; Bonetti, I. Acetabular reconstruction with the Burch-Schneider antiprotrusio cage and bulk allografts: Minimum 10-year follow-up results. Biomed. Res. Int. 2014, 2014, 194076. [Google Scholar] [CrossRef] [PubMed]
- Saleh, K.J.; Jaroszynski, G.; Woodgate, I.; Saleh, L.; Gross, A.E. Revision total hip arthroplasty with the use of structural acetabular allograft and reconstruction ring: A case series with a 10-year average follow-up. J. Arthroplast. 2000, 15, 951–958. [Google Scholar] [CrossRef] [PubMed]
- Garbuz, D.; Morsi, E.; Gross, A.E. Revision of the Acetabular Component of a Total Hip Arthroplasty with a Massive Structural Allograft. Study with a Minimum Five-Year Follow-up*. J. Bone Jt. Surg. Br. 1996, 78, 693–697. [Google Scholar] [CrossRef] [PubMed]
- Kosashvili, Y.; Backstein, D.; Safir, O.; Lakstein, D.; Gross, A.E. Acetabular revision using an anti-protrusion (ilio-ischial) cage and trabecular metal acetabular component for severe acetabular bone loss associated with pelvic discontinuity. J. Bone Jt. Surg. Br. 2009, 91, 870–876. [Google Scholar] [CrossRef] [PubMed]
- Lachiewicz, P.F.; Soileau, E.S. Tantalum components in difficult acetabular revisions. Clin. Orthop. Relat. Res. 2010, 468, 454–458. [Google Scholar] [CrossRef] [PubMed]
- Abolghasemian, M.; Tangsataporn, S.; Sternheim, A.; Backstein, D.; Safir, O.; Gross, A.E. Combined trabecular metal acetabular shell and augment for acetabular revision with substantial bone loss: A mid-term review. Bone Jt. J. 2013, 95-B, 166–172. [Google Scholar] [CrossRef]
- Amenabar, T.; Rahman, W.A.; Hetaimish, B.M.; Kuzyk, P.R.; Safir, O.A.; Gross, A.E. Promising Mid-term Results with a Cup-cage Construct for Large Acetabular Defects and Pelvic Discontinuity. Clin. Orthop. Relat. Res. 2016, 474, 408–414. [Google Scholar] [CrossRef]
- Beckmann, N.A.; Weiss, S.; Klotz, M.C.; Gondan, M.; Jaeger, S.; Bitsch, R.G. Loosening after acetabular revision: Comparison of trabecular metal and reinforcement rings. A systematic review. J. Arthroplast. 2014, 29, 229–235. [Google Scholar] [CrossRef]
- Boscainos, P.J.; Kellett, C.F.; Maury, A.C.; Backstein, D.; Gross, A.E. Management of periacetabular bone loss in revision hip arthroplasty. Clin. Orthop. Relat. Res. 2007, 465, 159–165. [Google Scholar] [CrossRef]
- Levine, B. A New Era in Porous Metals: Applications in Orthopaedics. Adv. Eng. Mater. 2008, 10, 788–792. [Google Scholar] [CrossRef]
- Xiong, C.; Meng, D.; Ni, R.; Cai, H. Metal Augments Used in Revision Hip Arthroplasty: A Systematic Review and Single-Arm Meta-Analysis. J. Arthroplast. 2023, 38, 389–396.e1. [Google Scholar] [CrossRef] [PubMed]
- Baecker, H.; Hardt, S.; Abdel, M.P.; Perka, C. Tantalum Augments Combined with Antiprotrusio Cages for Massive Acetabular Defects in Revision Arthroplasty. Arthroplast. Today 2020, 6, 704–709. [Google Scholar] [CrossRef] [PubMed]
- Garceau, S.P.; Warschawski, Y.; Joly, D.; Safir, O.A.; Gross, A.E.; Kuzyk, P.R. Hip Arthroplasty with the Use of a Reconstruction Cage and Porous Metal Augment to Treat Massive Acetabular Bone Loss: A Midterm Follow-Up. J. Arthroplast. 2022, 37, S636–S641. [Google Scholar] [CrossRef] [PubMed]
- Mäkinen, T.J.; Abolghasemian, M.; Watts, E.; Fichman, S.G.; Kuzyk, P.; Safir, O.A.; Gross, A.E. Management of massive acetabular bone defects in revision arthroplasty of the hip using a reconstruction cage and porous metal augment. Bone Jt. J. 2017, 99-B, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Wang, Q.; Liu, P.; Ge, J.; Zhang, Q.; Guo, W.; Wang, W. Clinical and radiological outcomes of jumbo cup in revision total hip arthroplasty: A systematic review. Front. Surg. 2022, 9, 929103. [Google Scholar] [CrossRef] [PubMed]
- Paprosky, W.G.; Perona, P.G.; Lawrence, J.M. Acetabular defect classification and surgical reconstruction in revision arthroplasty. A 6-year follow-up evaluation. J. Arthroplast. 1994, 9, 33–44. [Google Scholar] [CrossRef]
- Telleria, J.J.; Gee, A.O. Classifications in brief: Paprosky classification of acetabular bone loss. Clin. Orthop. Relat. Res. 2013, 471, 3725–3730. [Google Scholar] [CrossRef]
- DeLee, J.G.; Charnley, J. Radiological demarcation of cemented sockets in total hip replacement. Clin. Orthop. Relat. Res. 1976, 121, 20–32. [Google Scholar] [CrossRef]
- Lim, S.J.; Lee, K.H.; Park, S.H.; Park, Y.S. Medium-term results of cementation of a highly cross-linked polyethylene liner into a well-fixed acetabular shell in revision hip arthroplasty. J. Arthroplast. 2014, 29, 634–637. [Google Scholar] [CrossRef]
- Schreurs, B.W.; Keurentjes, J.C.; Gardeniers, J.W.; Verdonschot, N.; Slooff, T.J.; Veth, R.P. Acetabular revision with impacted morsellised cancellous bone grafting and a cemented acetabular component: A 20- to 25-year follow-up. J. Bone Jt. Surg. Br. 2009, 91, 1148–1153. [Google Scholar] [CrossRef]
- Schlegel, U.J.; Bitsch, R.G.; Pritsch, M.; Aldinger, P.R.; Mau, H.; Breusch, S.J. Acetabular reinforcement rings in revision total hip arthroplasty: Midterm results in 298 cases. Orthopade 2008, 37, 904–913. [Google Scholar] [CrossRef] [PubMed]
- Russell, S.P.; O’Neill, C.J.; Fahey, E.J.; Guerin, S.; Gul, R.; Harty, J.A. Trabecular Metal Augments for Severe Acetabular Defects in Revision Hip Arthroplasty: A Long-Term Follow-Up. J. Arthroplast. 2021, 36, 1740–1745. [Google Scholar] [CrossRef] [PubMed]
- Del Gaizo, D.J.; Kancherla, V.; Sporer, S.M.; Paprosky, W.G. Tantalum augments for Paprosky IIIA defects remain stable at midterm followup. Clin. Orthop. Relat. Res. 2012, 470, 395–401. [Google Scholar] [CrossRef] [PubMed]
- Davies, J.H.; Laflamme, G.Y.; Delisle, J.; Fernandes, J. Trabecular metal used for major bone loss in acetabular hip revision. J. Arthroplast. 2011, 26, 1245–1250. [Google Scholar] [CrossRef]
- Udomkiat, P.; Dorr, L.D.; Won, Y.Y.; Longjohn, D.; Wan, Z. Technical factors for success with metal ring acetabular reconstruction. J. Arthroplast. 2001, 16, 961–969. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Sex/Age | BMI * (kg/m2) | BMD * (T-Score) | Reason for Index Surgery | Reason for Final Revision Surgery | No. of Revision Surgery | Follow-Up Duration (Months) |
|---|---|---|---|---|---|---|---|
| 1 | F/44 | 24.1 | −1.1 † | Traumatic OA | Cup loosening | 2 | 112.0 |
| 2 | M/71 | 21.6 | −3.3 | Femoral Neck Fx | All component loosening | 3 | 112.0 |
| 3 | F/69 | 34.1 | −2.1 | Traumatic OA | Cup loosening | 2 | 106.7 |
| 4 | M/65 | 28.1 | −2.6 | Femoral Neck Fx | All component loosening + ceramic liner Fx | 1 | 96.0 |
| 5 | M/58 | 26.3 | −1.0 | Traumatic ONFH | Acetabular destruction after monobloc arthroplasty | 1 | 112.0 |
| 6 | M/50 | 29.0 | 0.9 | Idiopathic ONFH | Cup loosening | 2 | 107.9 |
| 7 | M/75 | 21.7 | −1.9 | Traumatic ONFH | All component loosening + ceramic liner Fx | 3 | 100.0 |
| 8 | F/71 | 26.2 | −3.1 | Traumatic OA | Cup loosening | 4 | 101.1 |
| 9 | M/60 | 24.9 | −0.7 | Septic Hip Sequalae | Cup loosening | 1 | 99.6 |
| 10 | F/80 | 19.5 | −2.8 | LCP Sequalae | Cup loosening | 3 | 96.0 |
| Case | Side | Operation | Paprosky | Implants | Additional Procedure | Final HHS | Postop Cx |
|---|---|---|---|---|---|---|---|
| 1 | Lt | Total a | 3A | B-S + TM + Mesh | GTO + Grip plate | 85 | - |
| 2 | Lt | Total | 3A | B-S + TM | Trochanter wiring | 91 | - |
| 3 | Lt | Cup b | 3B | B-S + TM | - | 73 | PJI |
| 4 | Lt | Cup | 3B | B-S + TM | - | 72 | Acute D/L |
| 5 | Lt | Total | 3A | B-S + TM | ETO + Wiring | 86 | - |
| 6 | Lt | Cup | 3A | B-S + TM | GTO + Grip plate | 90 | - |
| 7 | Lt | Cup | 3A | B-S + TM | - | 81 | - |
| 8 | Lt | Cup | 3A | B-S + TM | GTO + Grip plate | 79 | - |
| 9 | Lt | Cup | 3B | B-S + TM | GTO + Grip plate | 82 | - |
| 10 | Rt | Cup | 3B | B-S + TM + Mesh | GTO | 76 | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.S.; Kim, J.W.; Chang, J.S.; Kim, C.-H. Revision Total Hip Arthroplasty Utilizing an Acetabular Reinforcement Ring with a Metal Augment: A Minimum Eight-Year Follow-Up Study. Medicina 2023, 59, 1036. https://doi.org/10.3390/medicina59061036
Kim HS, Kim JW, Chang JS, Kim C-H. Revision Total Hip Arthroplasty Utilizing an Acetabular Reinforcement Ring with a Metal Augment: A Minimum Eight-Year Follow-Up Study. Medicina. 2023; 59(6):1036. https://doi.org/10.3390/medicina59061036
Chicago/Turabian StyleKim, Han Soul, Ji Wan Kim, Jae Suk Chang, and Chul-Ho Kim. 2023. "Revision Total Hip Arthroplasty Utilizing an Acetabular Reinforcement Ring with a Metal Augment: A Minimum Eight-Year Follow-Up Study" Medicina 59, no. 6: 1036. https://doi.org/10.3390/medicina59061036