
Comparison of C-Arm-Free Oblique Lumbar Interbody Fusion L5-S1 (OLIF51) with Transforaminal Lumbar Interbody Fusion L5-S1 (TLIF51) for Adult Spinal Deformity
 , , ,
, , ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Operation Procedure
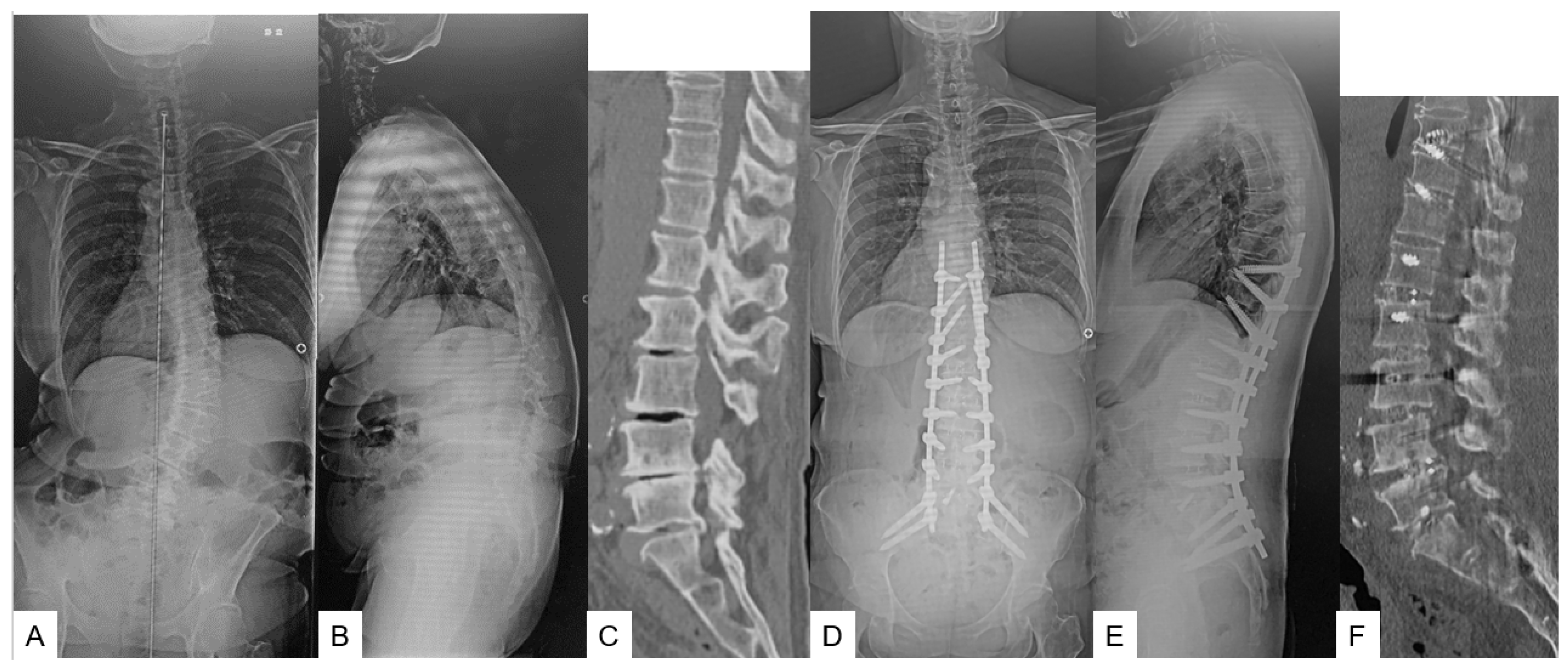
2.1.1. Primary Surgery (OLIF L1-S1 in Group O or OLIF L1-5 in Group T) (Figure 1) [9]

2.1.2. Secondary Surgery (T10-SAI in Group O or T10-SAI + TLIF51 in Group T) (Figure 1)
2.2. Clinical Assessment and Evaluation
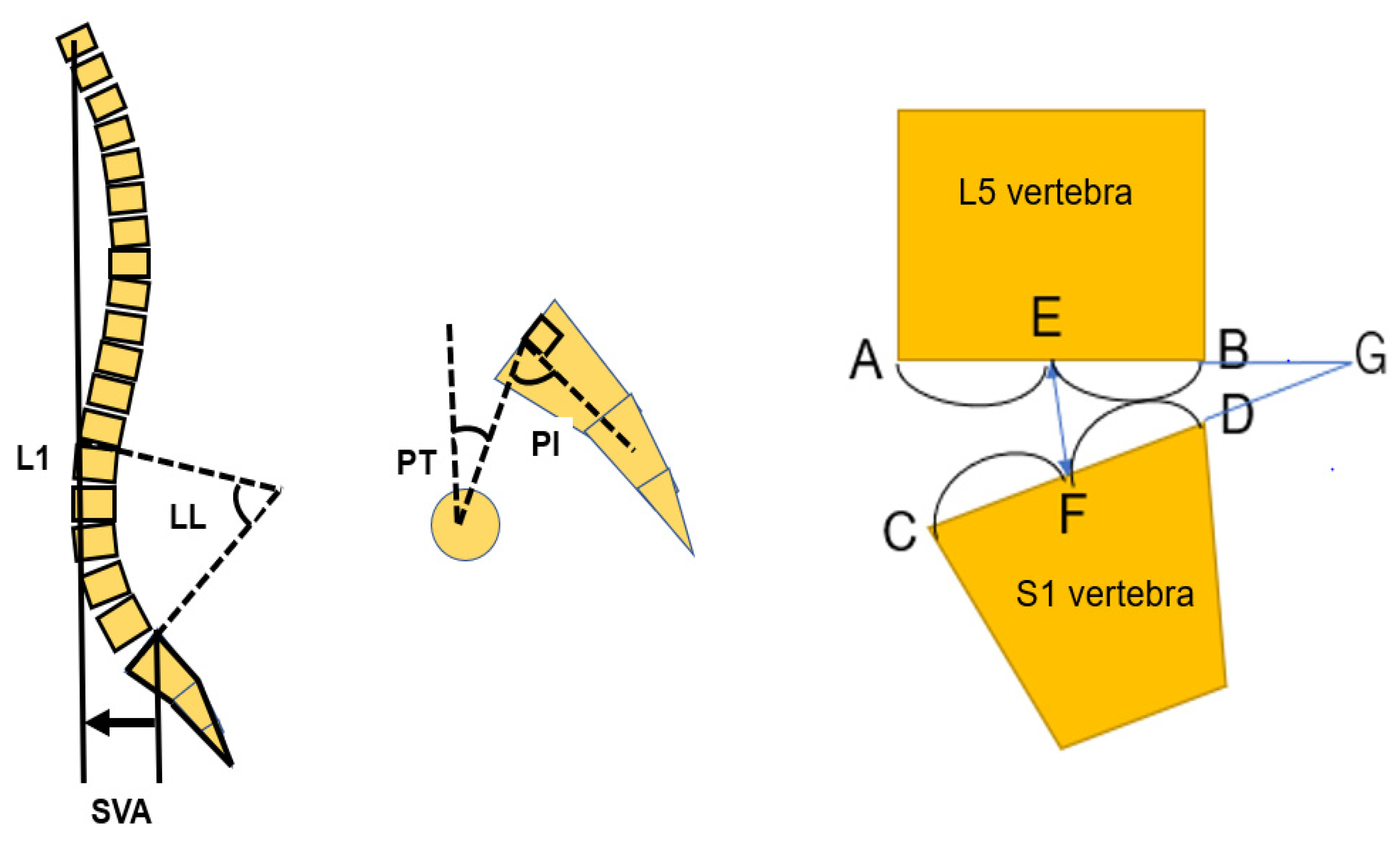
2.3. Radiographic Evaluation
2.4. Statistical Evaluation
3. Results
3.1. Patients Demographics
3.2. Clinical Evaluation
3.3. Radiographic Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aebi, M. The Adult Scoliosis. Eur. Spine J. 2005, 14, 925–948. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.S.; Shaffrey, C.I.; Bess, S.; Shamji, M.F.; Brodke, D.; Lenke, L.G.; Fehlings, M.G.; Lafage, V.; Schwab, F.; Vaccaro, A.R.; et al. Recent and Emerging Advances in Spinal Deformity. Clin. Neurosurg. 2017, 80, S77–S85. [Google Scholar] [CrossRef]
- Schwab, F.; Dubey, A.; Gamez, L.; Benchikh, A.; Fegoun, E.; Hwang, K.; Pagala, M.; Farcy, J.-P. Adult Scoliosis: Prevalence, SF-36, and Nutritional Parameters in an Elderly Volunteer Population. Spine 2003, 28, 602–606. [Google Scholar] [CrossRef]
- Sakaguchi, T.; Tanaka, M.; Sake, N.; Latka, K.; Fujiwara, Y.; Arataki, S.; Yamauchi, T.; Takamatsu, K.; Yasuda, Y.; Nakagawa, M.; et al. The Most Significant Factor Affecting Gait and Postural Balance in Patients’ Activities of Daily Living Following Corrective Surgery for Deformity of the Adult Spine. Medicina 2022, 58, 1118. [Google Scholar] [CrossRef] [PubMed]
- Diebo, B.G.; Lavian, J.D.; Murray, D.P.; Liu, S.; Shah, N.V.; Beyer, G.A.; Segreto, F.A.; Bloom, L.; Vasquez-Montes, D.; Day, L.M.; et al. The Impact of Comorbid Mental Health Disorders on Complications Following Adult Spinal Deformity Surgery with Minimum 2-Year Surveillance. Spine 2018, 43, 1176–1183. [Google Scholar] [CrossRef] [PubMed]
- Uotani, K.; Tanaka, M.; Sonawane, S.; Ruparel, S.; Fujiwara, Y.; Arataki, S.; Yamauchi, T.; Misawa, H. Comparative Study of Bilateral Dual Sacral-Alar-Iliac Screws versus Bilateral Single Sacral-Alar-Iliac Screw for Adult Spine Deformities. World Neurosurg. 2021, 156, e300–e306. [Google Scholar] [CrossRef]
- Cho, K.J.; Bridwell, K.H.; Lenke, L.G.; Berra, A.; Baldus, C. Comparison of Smith-Petersen versus pedicle subtraction osteotomy for the correction of fixed sagittal imbalance. Spine 2005, 30, 2030–2037. [Google Scholar] [CrossRef]
- Iyer, S.; Nemani, V.M.; Kim, H.J. A review of complications and outcomes following vertebral column resection in adults. Asian Spine J. 2016, 10, 601–609. [Google Scholar] [CrossRef]
- Kim, Y.J.; Bridwell, K.H.; Lenke, L.G.; Rhim, S.; Cheh, G. Pseudarthrosis in long adult spinal deformity instrumentation and fusion to the sacrum: Prevalence and risk factor analysis of 144 cases. Spine 2006, 31, 2329–2336. [Google Scholar] [CrossRef]
- Buchowski, J.M.; Bridwell, K.H.; Lenke, L.G.; Kuhns, C.A.; Lehman, R.A., Jr.; Kim, Y.J.; Stewart, D.; Baldus, C. Neurologic complications of lumbar pedicle subtraction osteotomy: A 10-year assessment. Spine 2007, 32, 2245–2252. [Google Scholar] [CrossRef]
- Pateder, D.B.; Gonzales, R.A.; Kebaish, K.M.; Cohen, D.B.; Chang, J.-Y.; Kostuik, J.P. Short-Term Mortality and Its Association With Independent Risk Factors in Adult Spinal Deformity Surgery. Spine 2008, 33, 1224–1228. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.S.; Sansur, C.A.; Donaldson, W.F.; Perra, J.H.; Mudiyam, R.; Choma, T.J.; Zeller, R.D.; Knapp, D.R.; Noordeen, H.H.; Berven, S.H.; et al. Short-Term Morbidity and Mortality Associated with Correction of Thoracolumbar Fixed Sagittal Plane Deformity: A Report from the Scoliosis Research Society Morbidity and Mortality Committee. Spine 2011, 36, 958–964. [Google Scholar] [CrossRef] [PubMed]
- Chang, M.C.; Kim, G.U.; Choo, Y.J.; Lee, G.W. Transforaminal Lumbar Interbody Fusion (TLIF) versus Oblique Lumbar Interbody Fusion (OLIF) in Interbody Fusion Technique for Degenerative Spondylolisthesis: A Systematic Review and Meta-Analysis. Life 2021, 11, 696. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, M.; Fujiwara, Y.; Uotani, K.; Maste, P.; Yamauchi, T. C-Arm–Free Circumferential Minimally Invasive Surgery for Adult Spinal Deformity: Technical Note. World Neurosurg. 2020, 143, 235–246. [Google Scholar] [CrossRef]
- Mummaneni, P.V.; Shaffrey, C.I.; Lenke, L.G.; Park, P.; Wang, M.Y.; La Marca, F.; Smith, J.S.; Mundis, G.M.; Okonkwo, D.O.; Moal, B.; et al. The minimally invasive spinal deformity surgery algorithm: A reproducible rational framework for decision making in minimally invasive spinal deformity surgery. Neurosurg. Focus 2014, 36, E6. [Google Scholar] [CrossRef]
- Phillips, F.M.; Isaacs, R.E.; Rodgers, W.B.; Park, P.; Wang, M.Y.; La Marca, F.; Smith, J.S.; Mundis, G.M.; Okonkwo, D.O.; Moal, B.; et al. Adult degenerative scoliosis treated with XLIF: Clinical and radiographical results of a prospective multicenter study with 24-month follow-up. Spine 2013, 38, 1853–1861. [Google Scholar] [CrossRef]
- Anand, N.; Baron, E.M.; Thaiyananthan, G.; Khalsa, K.; Goldstein, T.B. Minimally Invasive Multilevel Percutaneous Correction and Fusion for Adult Lumbar Degenerative Scoliosis A Technique and Feasibility Study. J Spinal Disord. Technol. 2008, 21, 459–467. [Google Scholar] [CrossRef]
- Zhu, L.; Wang, J.W.; Zhang, L.; Feng, X.M. Outcomes of Oblique Lateral Interbody Fusion for Adult Spinal Deformity: A Systematic Review and Meta-Analysis. Glob. Spine J. 2022, 12, 142–154. [Google Scholar] [CrossRef]
- Tanaka, M.; Singh, M.; Fujiwara, Y.; Uotani, K.; Oda, Y.; Arataki, S.; Yamauchi, T.; Takigawa, T.; Ito, Y. Comparison of Navigated Expandable Vertebral Cage with Conventional Expandable Vertebral Cage for Minimally Invasive Lumbar/Thoracolumbar Corpectomy. Medicina 2022, 58, 364. [Google Scholar] [CrossRef]
- Ames, C.P.; Scheer, J.K.; Lafage, V.; Smith, J.S.; Bess, S.; Berven, S.H.; Mundis, G.M.; Sethi, R.K.; Deinlein, D.A.; Coe, J.D.; et al. Adult Spinal Deformity: Epidemiology, Health Impact, Evaluation, and Management. Spine Deform. 2016, 4, 310–322. [Google Scholar] [CrossRef]
- Tanaka, M.; Ruparel, S.; Oda, Y.; Fujiwara, Y.; Shama, S.; Uotani, K.; Arataki, S.; Yamauchi, T.; Sake, N. C-arm-Free Simultaneous OLIF51 and Percutaneous Pedicle Screw Fixation in a Single Lateral Position. J. Vis. Exp. 2022, 187, e63572. [Google Scholar] [CrossRef]
- Lenke, L.G.; Fehlings, M.G.; Shaffrey, C.I.; Cheung, K.M.C.; Carreon, L.; Dekutoski, M.B.; Schwab, F.J.; Boachie-Adjei, O.; Kebaish, K.M.; Ames, C.P.; et al. Neurologic Outcomes of Complex Adult Spinal Deformity Surgery. Spine 2016, 41, 204–212. [Google Scholar] [CrossRef] [PubMed]
- Pellisé, F.; Vila-Casademunt, A.; Ferrer, M.; Domingo-Sàbat, M.; Bagó, J.; Pérez-Grueso, F.J.S.; Alanay, A.; Mannion, A.F.; Acaroglu, E. Impact on Health Related Quality of Life of Adult Spinal Deformity (ASD) Compared with Other Chronic Conditions. Eur. Spine J. 2015, 24, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Bess, S.; Line, B.; Fu, K.M.; Mccarthy, I.; Lafage, V.; Schwab, F.; Shaffrey, C.; Ames, C.; Akbarnia, B.; Jo, H.; et al. The Health Impact of Symptomatic Adult Spinal Deformity: Comparison of Deformity Types to United States Population Norms and Chronic Diseases. Spine 2016, 41, 224–233. [Google Scholar] [CrossRef] [PubMed]
- Swank, S.; Lonstein, J.E.; Moe, J.H.; Winter, R.B.; Bradford, D.S. Surgical Treatment of Adult Scoliosis. A Review of Two Hundred and Twenty-Two Cases. J. Bone Jt. Surg. Am. 1981, 63, 268–287. [Google Scholar] [CrossRef]
- Fowles, J.V.; Drummond, D.S.; L’Ecuyer, S.; Roy, L.; Kassab, M.T. Untreated Scoliosis in the Adult. Clin. Orthop. Relat. Res. 1978, 134, 212–217. [Google Scholar] [CrossRef]
- Kostuik, J.; Isreal, J.; Hall, J. Scoliosis Surgery in Adults. Clin. Orthop. Relat. Res. 1978, 134, 225–234. [Google Scholar] [CrossRef]
- Schwab, F.; Dubey, A.; Pagala, M.; Gamez, L.; Farcy, J.P. Adult Scoliosis: A Health Assessment Analysis by SF-36; and NutritionalParameters in an Elderly Volunteer Population. Spine 2005, 30, 1082–1085. [Google Scholar] [CrossRef]
- Glassman, S.D.; Hamill, C.L.; Bridwell, K.H.; Schwab, F.J.; Dimar, J.R.; Lowe, T.G. The Impact of Perioperative Complications on Clinical Outcome in Adult Deformity Surgery. Spine 2007, 32, 2764–2770. [Google Scholar] [CrossRef]
- Smith, J.S.; Shaffrey, C.I.; Klineberg, E.; Lafage, V.; Schwab, F.; Lafage, R.; Kim, H.J.; Hostin, R.; Mundis, G.M.; Gupta, M.; et al. Complication Rates Associated with 3-Column Osteotomy in 82 Adult Spinal Deformity Patients: Retrospective Review of a Prospectively Collected Multicenter Consecutive Series with 2-Year Follow-Up. J. Neurosurg. Spine 2017, 27, 444–457. [Google Scholar] [CrossRef]
- Khan, N.R.; Clark, A.J.; Lee, S.L.; Venable, G.T.; Rossi, N.B.; Foley, K.T. Surgical Outcomes for Minimally Invasive vs Open Transforaminal Lumbar Interbody Fusion: An Updated Systematic Review and Meta-Analysis. Neurosurgery 2015, 77, 847–874. [Google Scholar] [CrossRef] [PubMed]
- Vora, D.; Kinnard, M.; Falk, D.; Hoy, M.; Gupta, S.; Piper, C.; Yu, W.; Siddiqui, F.; O’Brien, J. A Comparison of Narcotic Usage and Length of Post-Operative Hospital Stay in Open versus Minimally Invasive Lumbar Interbody Fusion with Percutaneous Pedicle Screws. J. Spine Surg. 2018, 4, 516–521. [Google Scholar] [CrossRef] [PubMed]
- McGirt, M.J.; Parker, S.L.; Mummaneni, P.; Knightly, J.; Pfortmiller, D.; Foley, K.; Asher, A.L. Is the Use of Minimally Invasive Fusion Technologies Associated with Improved Outcomes after Elective Interbody Lumbar Fusion? Analysis of a Nationwide Prospective Patient-Reported Outcomes Registry. Spine J. 2017, 17, 922–932. [Google Scholar] [CrossRef] [PubMed]
- Gelb, D.E.; Lenke, L.G.; Bridwell, K.H.; Blanke, K.; McEnery, K.W. An analysis of sagittal spinal alignment in 100 asymptomatic middle and older aged volunteers. Spine 1995, 20, 1351–1358. [Google Scholar] [CrossRef]
- Harrison, D.E.; Harrison, D.D.; Cailliet, R.; Janik, T.J.; Holland, B. Radiographic Analysis of Lumbar Lordosis Centroid, Cobb, TRALL, and Harrison Posterior Tangent Methods. Spine 2001, 26, E235–E242. [Google Scholar] [CrossRef]
- Maruo, K.; Ha, Y.; Inoue, S.; Samuel, S.; Okada, E.; Hu, S.S.; Deviren, V.; Burch, S.; William, S.; Ames, C.P.; et al. Predictive Factors for Proximal Junctional Kyphosis in Long Fusions to the Sacrum in Adult Spinal Deformity. Spine 2013, 38, E1469–E1476. [Google Scholar] [CrossRef]
- Lafage, R.; Obeid, I.; Liabaud, B.; Bess, S.; Burton, D.; Smith, J.S.; Jalai, C.; Hostin, R.; Shaffrey, C.I.; Ames, C.; et al. Location of Correction within the Lumbar Spine Impacts Acute Adjacent-Segment Kyphosis. J. Neurosurg. Spine 2019, 30, 69–77. [Google Scholar] [CrossRef]
- Choi, W.S.; Kim, J.S.; Hur, J.W.; Seong, J.H. Minimally Invasive Transforaminal Lumbar Interbody Fusion Using Banana-Shaped and Straight Cages: Radiological and Clinical Results from a Prospective Randomized Clinical Trial. Clin. Neurosurg. 2018, 82, 289–297. [Google Scholar] [CrossRef]
- Hah, R.; Kang, H.P. Lateral and Oblique Lumbar Interbody Fusion—Current Concepts and a Review of Recent Literature. Curr. Rev. Musculoskelet. Med. 2019, 12, 305–310. [Google Scholar] [CrossRef]
- Meng, B.; Bunch, J.; Burton, D.; Wang, J. Lumbar interbody fusion: Recent advances in surgical techniques and bone healing strategies. Eur. Spine J. 2021, 30, 22–33. [Google Scholar] [CrossRef]
- Chandra, V.V.; Prasad, B.C.M.; Hanu, T.G.; Kale, P.G. Comparison between Oblique Lumbar Interbody Fusion (OLIF) and Minimally Invasive Transforaminal Lumbar Interbody Fusion (MISTLIF) for Lumbar Spondylolisthesis. Neurol. India 2022, 70, 127–134. [Google Scholar]
- Woods, K.R.; Billys, J.B.; Hynes, R.A. Technical description of oblique lateral interbody fusion at L1-L5 (OLIF25) and at L5-S1 (OLIF51) and evaluation of complication and fusion rates. Spine J. 2017, 17, 545–553. [Google Scholar] [CrossRef] [PubMed]
- Zairi, F.; Sunna, T.P.; Westwick, H.J.; Weil, A.G.; Wang, Z.; Boubez, G.; Boubez, G.; Shedid, D. Mini-open oblique lumbar interbody fusion (OLIF) approach for multilevel discectomy and fusion involving L5-S1: Preliminary experience. Orthop. Traumatol. Surg. Res. 2017, 103, 295–299. [Google Scholar] [CrossRef] [PubMed]
- Mun, H.Y.; Ko, M.J.; Kim, Y.B.; Park, S.W. Usefulness of Oblique Lateral Interbody Fusion at L5-S1 Level Compared to Transforaminal Lumbar Interbody Fusion. J. Korean Neurosurg. Soc. 2020, 63, 723–729. [Google Scholar] [CrossRef] [PubMed]
- Matsukura, Y.; Yoshii, T.; Morishita, S.; Sakai, K.; Hirai, T.; Yuasa, M.; Inose, H.; Kawabata, A.; Utagawa, K.; Hashimoto, J.; et al. Comparison of Lateral Lumbar Interbody Fusion and Posterior Lumbar Interbody Fusion as Corrective Surgery for Patients with Adult Spinal Deformity—A Propensity Score Matching Analysis. J. Clin. Med. 2021, 10, 4737. [Google Scholar] [CrossRef]
- Ohtori, S.; Mannoji, C.; Orita, S.; Yamauchi, K.; Eguchi, Y.; Ochiai, N.; Kishida, S.; Kuniyoshi, K.; Aoki, Y.; Nakamura, J.; et al. Mini-open anterior retroperitoneal lumbar interbody fusion: Oblique lateral interbody fusion for degenerated lumbar spinal kyphoscoliosis. Asian Spine J. 2015, 9, 565–572. [Google Scholar] [CrossRef]
- Silvestre, C.; Mac-Thiong, J.M.; Hilmi, R.; Roussouly, P. Complications and morbidities of mini-open anterior retroperitoneal lumbar interbody fusion: Oblique lumbar interbody fusion in 179 patients. Asian Spine J. 2012, 6, 89–97. [Google Scholar] [CrossRef]
- Tan, Y.; Tanaka, M.; Sonawane, S.; Uotani, K.; Oda, Y.; Fujiwara, Y.; Arataki, S.; Yamauchi, T.; Takigawa, T.; Ito, Y. Comparison of Simultaneous Single-Position Oblique Lumbar Interbody Fusion and Percutaneous Pedicle Screw Fixation with Posterior Lumbar Interbody Fusion Using o-Arm Navigated Technique for Lumbar Degenerative Diseases. J. Clin. Med. 2021, 10, 4938. [Google Scholar] [CrossRef]
- Park, S.W.; Ko, M.J.; Kim, Y.B.; le Huec, J.C. Correction of Marked Sagittal Deformity with Circumferential Minimally Invasive Surgery Using Oblique Lateral Interbody Fusion in Adult Spinal Deformity. J. Orthop. Surg. Res. 2020, 15, 436. [Google Scholar] [CrossRef]
- Kotani, Y.; Ikeura, A.; Tokunaga, H.; Saito, T. Single-Level Controlled Comparison of OLIF51 and Percutaneous Screw in Lateral Position versus MIS-TLIF for Lumbosacral Degenerative Disorders: Clinical and Radiologic Study. J. Orthop. Sci. 2021, 26, 756–764. [Google Scholar] [CrossRef]
- Dorward, I.G.; Lenke, L.G.; Bridwell, K.H.; O’Leary, P.T.; Stoker, G.E.; Pahys, J.M.; Kang, M.M.; Sides, B.A.; Koester, L.A. Transforaminal versus Anterior Lumbar Interbody Fusion in Long Deformity Constructs: A Matched Cohort Analysis. Spine 2013, 38, E755–E762. [Google Scholar] [CrossRef] [PubMed]
- Spiker, W.R.; Goz, V.; Brodke, D.S. Lumbar Interbody Fusions for Degenerative Spondylolisthesis: Review of Techniques, Indications, and Outcomes. Glob. Spine J. 2019, 9, 77–84. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group O (N = 13) | Group T (N = 41) | p Value | |
|---|---|---|---|
| L5-S1 fusion | OLIF51 | MIS-TLIF51 | |
| Patients | Man 0, Woman 13 | Man 4, Woman 37 | 0.243 |
| Age (year) | 74.6 ± 3.2 | 70.5 ± 6.6 | 0.023 * |
| BMI (kg/m2) | 22.7 ± 3.7 | 23.0 ± 4.2 | 0.715 |
| SVA (mm) | 100.8 ± 58.2 | 95.1 ± 55.8 | 0.934 |
| PI (°) | 57.5 ± 7.4 | 49.6 ± 11.3 | 0.035 * |
| PT (°) | 39.2 ± 9.4 | 33.0 ± 11.2 | 0.062 |
| PI-LL (°) | 46.4 ± 21.3 | 37.0 ± 22.2 | 0.185 |
| Disease | None | Parkinson 1, CP 1 |
| Group O (N = 13) | Group T (N = 41) | p Value | |
|---|---|---|---|
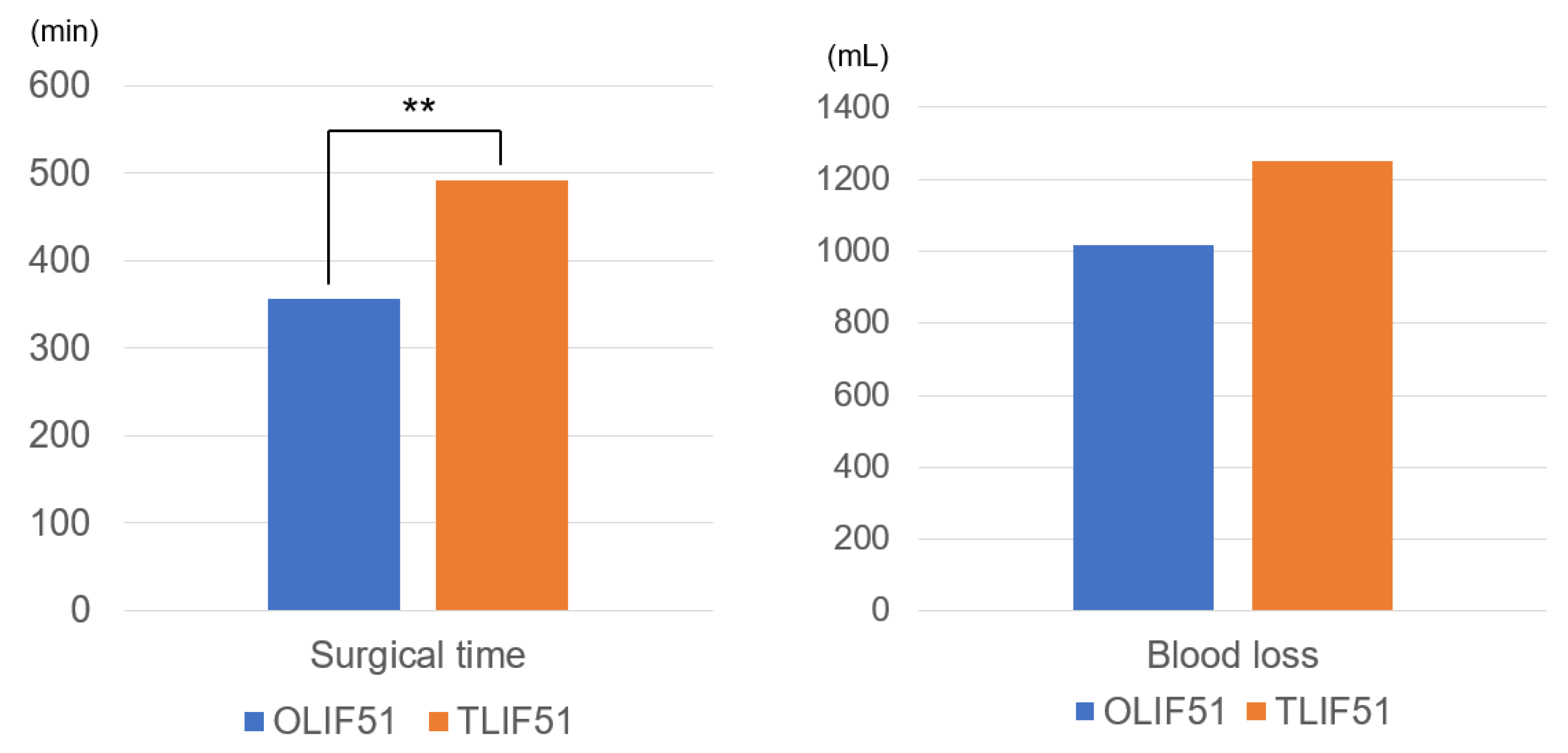
| Surgical time (minutes) | 356 ± 176 | 492 ± 94 | 0.003 ** |
| Blood loss (mL) | 1016 ± 601 | 1252 ± 667 | 0.274 |
| Postoperative ODI (%) | 22.4 ± 17.4 | 38.5 ± 20.4 | 0.131 |
| Postoperative VAS (mm) | 22.5 ± 6.5 | 39.8 ± 7.4 | 0.198 |
| Complication | |||
| PJK (+/−) | 4/9 | 17/24 | 0.491 |
| Rod breakage (+/−) | 2/11 | 3/38 | 0.382 |
| SSI (+/−) | 1/12 | 1/40 | 0.400 |
| Reoperation (+/−) | 2/11 | 8/33 | 0.570 |
| Group O (N = 13) | Group T (N = 41) | p Value | |
|---|---|---|---|
| Preoperative L5-S1 angle (°) | 12.0 ± 5.4 | 10.5 ± 4.7 | 0.459 |
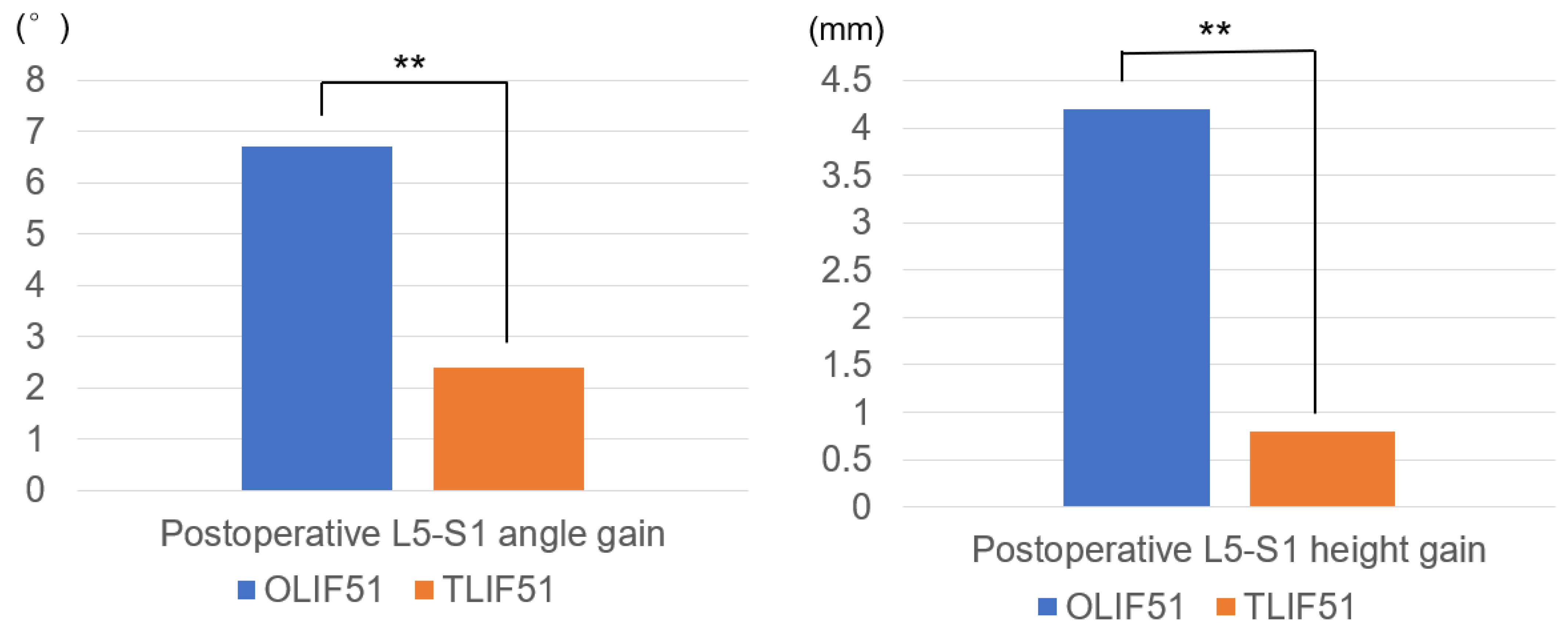
| Postoperative L5-S1 angle gain (°) | 9.4 ± 4.7 | 1.6 ± 5.1 | 0.0001 ** |
| Preoperative L5-S1 height (mm) | 7.1 ± 2.2 | 8.6 ± 2.5 | 0.052 |
| Postoperative L5-S1 height gain (mm) | 4.2 ± 2.9 | 0.8 ± 1.9 | 0.0002 ** |
| Preoperative SVA (mm) | 100.8 ± 58.2 | 95.1 ± 55.8 | 0.943 |
| Postoperative SVA (mm) | 43.7 ± 37.5 | 17.8 ± 37.8 | 0.046 * |
| Preoperative PI-LL (°) | 46.4 ± 21.3 | 37.0 ± 22.2 | 0.185 |
| Postoperative PI-LL (°) | 8.69 ± 9.9 | 0.35 ± 12.8 | 0.025 * |
| Preoperative PT (°) | 39.2 ± 9.4 | 33.0 ± 11.2 | 0.062 |
| Postoperative PT (°) | 17.7 ± 4.3 | 14.4 ± 9.8 | 0.107 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tanaka, M.; Sonawane, S.; Meena, U.; Lu, Z.; Fujiwara, Y.; Taoka, T.; Uotani, K.; Oda, Y.; Sakaguchi, T.; Arataki, S. Comparison of C-Arm-Free Oblique Lumbar Interbody Fusion L5-S1 (OLIF51) with Transforaminal Lumbar Interbody Fusion L5-S1 (TLIF51) for Adult Spinal Deformity. Medicina 2023, 59, 838. https://doi.org/10.3390/medicina59050838
Tanaka M, Sonawane S, Meena U, Lu Z, Fujiwara Y, Taoka T, Uotani K, Oda Y, Sakaguchi T, Arataki S. Comparison of C-Arm-Free Oblique Lumbar Interbody Fusion L5-S1 (OLIF51) with Transforaminal Lumbar Interbody Fusion L5-S1 (TLIF51) for Adult Spinal Deformity. Medicina. 2023; 59(5):838. https://doi.org/10.3390/medicina59050838
Chicago/Turabian StyleTanaka, Masato, Sumeet Sonawane, Umesh Meena, Zhichao Lu, Yoshihiro Fujiwara, Takuya Taoka, Koji Uotani, Yoshiaki Oda, Tomoyoshi Sakaguchi, and Shinya Arataki. 2023. "Comparison of C-Arm-Free Oblique Lumbar Interbody Fusion L5-S1 (OLIF51) with Transforaminal Lumbar Interbody Fusion L5-S1 (TLIF51) for Adult Spinal Deformity" Medicina 59, no. 5: 838. https://doi.org/10.3390/medicina59050838