
Pupillary Pain Index Predicts Postoperative Pain but Not the Effect of Peripheral Regional Anaesthesia in Patients Undergoing Total Hip or Total Knee Arthroplasty: An Observational Study
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. Perioperative Management
2.3. Pupillometry Measurement
2.4. Bias
2.5. Sample-Size Calculation
2.6. Outcomes
- -
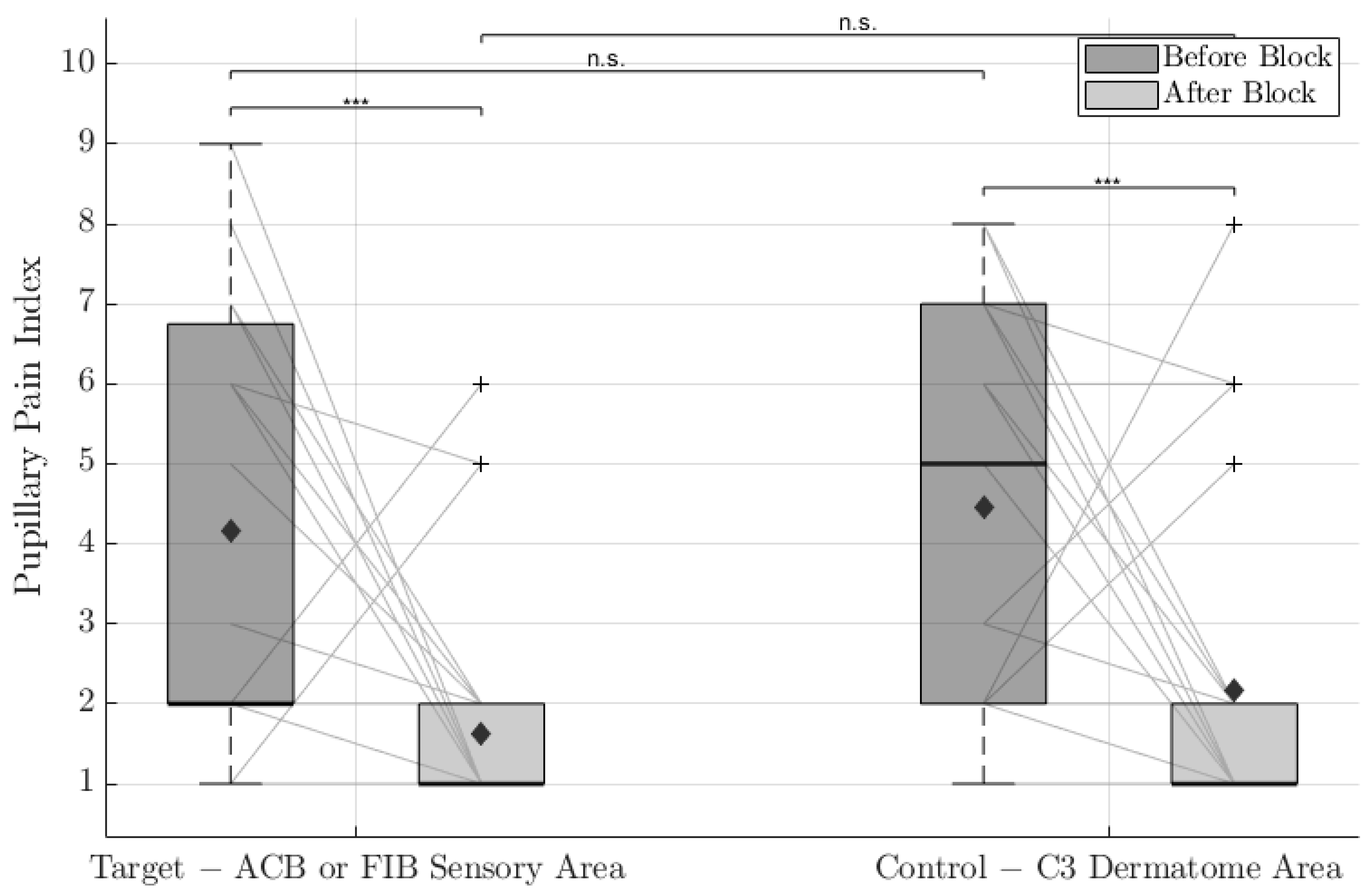
- The differences between PPIs before and after peripheral block insertion.
- -
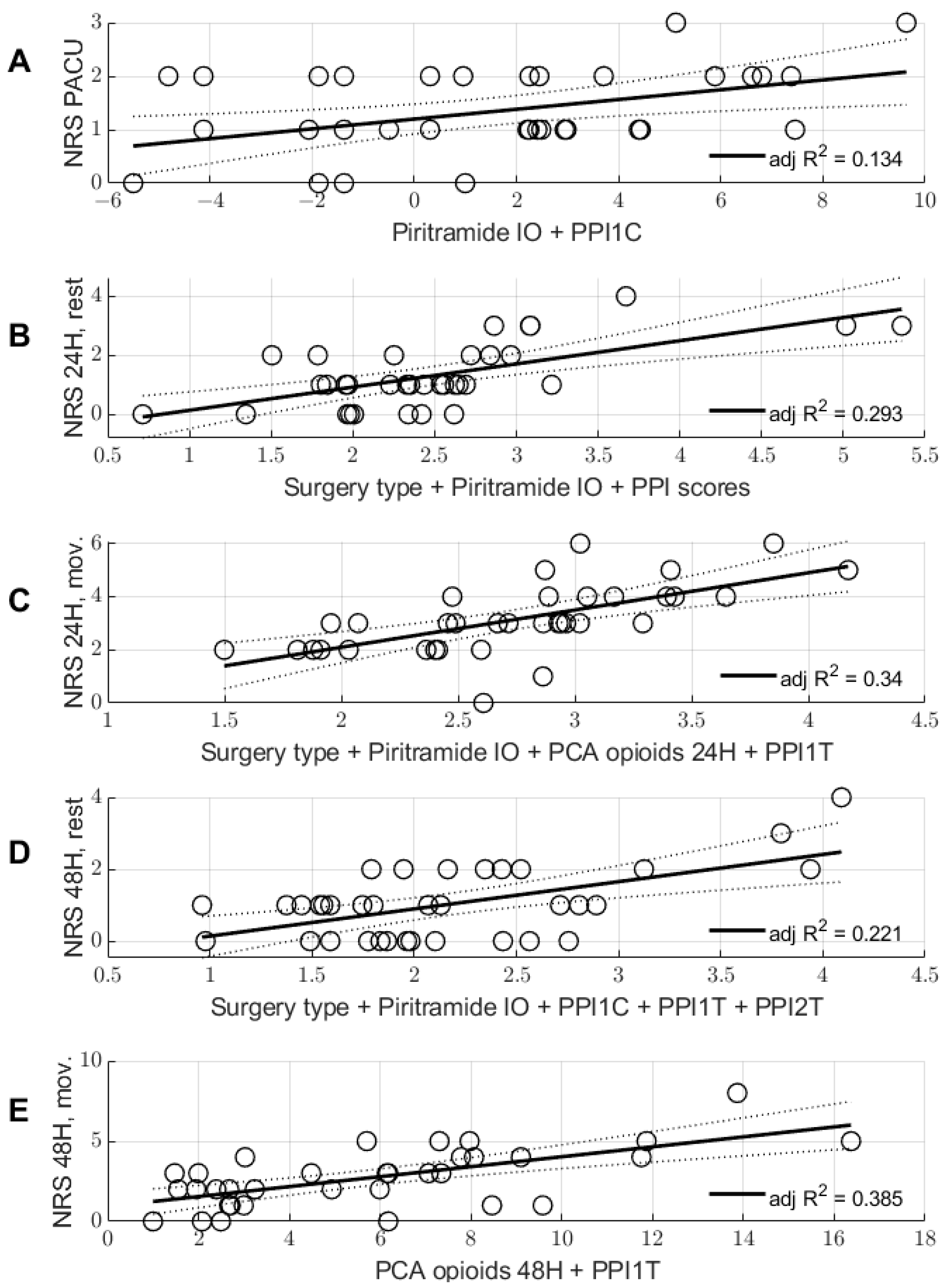
- The relationship between PPIs and NRS scales (PACU, 24 and 48 h, at rest and in movement).
2.7. Statistical Analysis
2.8. Regression Analysis
3. Results
3.1. Primary Outcomes
3.2. Secondary Outcomes
4. Discussion
4.1. Influence of Nerve Blocks and Opioids
4.2. Preoperative Nociception
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ilfeld, B.M. Continuous peripheral nerve blocks: An update of the published evidence and comparison with novel, alternative analgesic modalities. Anesth. Analg. 2017, 124, 308–335. [Google Scholar] [CrossRef] [PubMed]
- Joshi, G.; Gandhi, K.; Shah, N.; Gadsden, J.; Corman, S.L. Peripheral nerve blocks in the management of postoperative pain: Challenges and opportunities. J. Clin. Anesth. 2016, 35, 524–529. [Google Scholar] [CrossRef] [PubMed]
- Henderson, M.; Dolan, J. Challenges, solutions, and advances in ultrasound-guided regional anaesthesia. BJA Educ. 2016, 16, 374–380. [Google Scholar] [CrossRef]
- Larson, M.D.; Behrends, M. Portable Infrared Pupillometry: A Review. Anesth. Analg. 2015, 120, 1242–1253. [Google Scholar] [CrossRef] [PubMed]
- Sabourdin, N.; Diarra, C.; Wolk, R.; Piat, V.; Louvet, N.; Constant, I. Pupillary Pain Index Changes After a Standardized Bolus of Alfentanil Under Sevoflurane Anesthesia: First Evaluation of a New Pupillometric Index to Assess the Level of Analgesia During General Anesthesia. Anesth. Analg. 2019, 128, 467–474. [Google Scholar] [CrossRef] [PubMed]
- Larson, M.D.; Sessler, D.I.; Ozaki, M.; McGuire, J.; Schroeder, M. Pupillary assessment of sensory block level during combined epidural/general anesthesia. Anesthesiology 1993, 79, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Huybrechts, I.; Barvais, L.; Ducart, A.; Engelman, E.; Schmartz, D.; Koch, M. Assessment of thoracic epidural analgesia during general anesthesia using pupillary reflex dilation: A preliminary study. J. Cardiothorac. Vasc. Anesth. 2006, 20, 664–667. [Google Scholar] [CrossRef] [PubMed]
- Duceau, B.; Baubillier, M.; Bouroche, G.; Albi-Feldzer, A.; Jayr, C. Pupillary Reflex for Evaluation of Thoracic Paravertebral Block: A Prospective Observational Feasibility Study. Anesth. Analg. 2017, 125, 1342–1347. [Google Scholar] [CrossRef] [PubMed]
- Hennies, H.H.; Friderichs, E.; Schneider, J. Receptor binding, analgesic and antitussive potency of tramadol and other selected opioids. Arzneimittelforschung 1988, 38, 877–880. [Google Scholar] [PubMed]
- Isnardon, S.; Vinclair, M.; Genty, C.; Hebrard, A.; Albaladejo, P.; Payen, J.-F. Pupillometry to detect pain response during general anaesthesia following unilateral popliteal sciatic nerve block: A prospective, observational study. Eur. J. Anaesthesiol. 2013, 30, 429–434. [Google Scholar] [CrossRef] [PubMed]
- Aissou, M.; Snauwaert, A.; Dupuis, C.; Atchabahian, A.; Aubrun, F.; Beaussier, M. Objective assessment of the immediate postoperative analgesia using pupillary reflex measurement: A prospective and observational study. Anesthesiology 2012, 116, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Neice, A.E.; Behrends, M.; Bokoch, M.P.; Seligman, K.M.; Conrad, N.M.; Larson, M.D. Prediction of opioid analgesic efficacy by measurement of pupillary unrest. Anesth. Analg. 2017, 124, 915–921. [Google Scholar] [CrossRef] [PubMed]
- Werner, M.U.; Duun, P.; Kehlet, H. Prediction of Postoperative Pain by Preoperative Nociceptive Responses to Heat Stimulation. Anesthesiology 2004, 100, 115–119. [Google Scholar] [CrossRef] [PubMed]
- Martinez, V.; Fletcher, D.; Bouhassira, D.; Sessler, D.I.; Chauvin, M. The evolution of primary hyperalgesia in orthopedic surgery: Quantitative sensory testing and clinical evaluation before and after total knee arthroplasty. Anesth. Analg. 2007, 105, 815–821. [Google Scholar] [CrossRef] [PubMed]
- Lundblad, H.; Kreicbergs, A.; Jansson, K.-Å. Prediction of persistent pain after total knee replacement for osteoarthritis. J. Bone Jt. Surg. Br. Vol. 2008, 90, 166–171. [Google Scholar] [CrossRef] [PubMed]
- Aasvang, E.K.; Hansen, J.B.; Kehlet, H. Can Preoperative Electrical Nociceptive Stimulation Predict Acute Pain After Groin Herniotomy? J. Pain 2008, 9, 940–944. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, P.R.; Nørgaard, L.; Rasmussen, L.S.; Kehlet, H. Prediction of post-operative pain by an electrical pain stimulus. Acta Anaesthesiol. Scand. 2007, 51, 582–586. [Google Scholar] [CrossRef] [PubMed]
- Coderre, T.J.; Katz, J.; Vaccarino, A.L.; Melzack, R. Contribution of central neuroplasticity to pathological pain: Review of clinical and experimental evidence. Pain 1993, 52, 259–285. [Google Scholar] [CrossRef] [PubMed]
- Coderre, T.J.; Katz, J. Peripheral and central hyperexcitability: Differential signs and symptoms in persistent pain. Behav. Brain Sci. 1997, 20, 404–419. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameter | N = 35 |
|---|---|
| Age, years | 69.2 (47–90) |
| Body mass index | 29 (19.4–46.9) |
| Surgery type, n (%): | |
| Total hip replacement | 18 (51.4%) |
| Total knee replacement | 17(48.6%) |
| Anaesthesia type, n (%): | |
| General anaesthesia | 32 (91.4%) |
| Total intravenous anaesthesia | 3 (8.6%) |
| Regional anaesthesia type, n (%): | |
| Fascia iliaca block | 27 (77.1%) |
| Adductor canal block | 8 (22.9%) |
| Anaesthesia time, min | 211.7 ± 47.5 |
| Surgery time, min | 131.4 ± 95 |
| Intraoperative opioids: | |
| Remifentanil dose ratio | 7.3 ± 4.8 |
| Fentanyl, mg | 0.33 ± 0.13 |
| Piritramide in MED, mg | 4.48 ± 3.36 |
| Postoperative opioids dosage: | |
| 24-h PO opioids in MED, mg | 21.17 ± 13.18 |
| 48-h PO opioids in MED, mg | 28.25 ± 39.09 |
| PCA type, n (%): | |
| Tramadol | 16(45.7%) |
| Piritramide | 19 (54.3%) |
| Postoperative NRS: | |
| NRS PACU | 1.34 ± 0.8 |
| NRS 24 h, rest | 1.31 ± 1.08 |
| NRS 24 h, movement | 3.1 ± 1.3 |
| NRS 48 h, rest | 1.03 ± 1 |
| NRS 48 h, movement | 2.7 ± 1.8 |
| NRS PACU. Adjusted R Squared for the Model = 0.134, p-Value = 0.038 | VIF | |
| Piritramide perioperative in MED, mg | 0.066 (0.012–0.121, p = 0.019) | 1.01 |
| Control PPI before block | −0.063 (−0.161–0.035, p = 0.199) | 1.01 |
| NRS 24 h at rest. Adjusted R squared for the model = 0.293, p value = 0.013 | ||
| Surgery type | 0.626 (−0.067–1.318), p = 0.075 | 1.215 |
| Piritramide perioperative in MED, mg | 0.096 (0.02–0.173), p = 0.015 | 1.319 |
| Control PPI before block | −0.126 (−0.315–0.063), p = 0.183 | 2.536 |
| Target PPI before block | 0.159 (−0.029–0.346), p = 0.094 | 2.555 |
| Control PPI after block | −0.147 (−0.337–0.042), p = 0.123 | 1.554 |
| Target PPI after block | 0.394 (0.08–0.707), p = 0.016 | 1.486 |
| NRS 24 h in movement. Adjusted R squared for the model = 0.34, p value = 0.02 | ||
| Surgery type | 1.394 (0.499–2.289), p = 0.003 | 1.485 |
| Piritramide perioperative, mg | 0.114 (0.025–0.204), p = 0.014 | 1.333 |
| PCA opioids 24 h | 0.031 (−0.004–0.066), p = 0.082 | 1.539 |
| Target PPI before block | 0.095 (−0.049–0.238), p = 0.189 | 1.098 |
| NRS 48 h at rest. Adjusted R squared for the model = 0.221, p value = 0.029 | ||
| Surgery type | 0.666 (0.011–1.321), p = 0.046 | 1.187 |
| Piritramide perioperative, mg | 0.073 (0.002–0.143), p = 0.044 | 1.235 |
| Control PPI before block | −0.191 (−0.364-−0.019), p = 0.031 | 2.304 |
| Target PPI before block | 0.151 (−0.024–0.325), p = 0.088 | 2.416 |
| Target PPI after block | 0.256 (0.001–0.511), p = 0.049 | 1.075 |
| NRS 48 h in movement. Adjusted R squared for the model = 0.385, p value < 0.001 | ||
| Target PPI before block | 0.309 (0.124–0.495), p = 0.002 | 1.032 |
| PCA opioids 48 h | 0.018 (0.005–0.03), p = 0.009 | 1.032 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kornilov, E.; Gehlen, L.; Yacobi, D.; Soehle, M.; Kowark, A.; Thudium, M. Pupillary Pain Index Predicts Postoperative Pain but Not the Effect of Peripheral Regional Anaesthesia in Patients Undergoing Total Hip or Total Knee Arthroplasty: An Observational Study. Medicina 2023, 59, 826. https://doi.org/10.3390/medicina59050826
Kornilov E, Gehlen L, Yacobi D, Soehle M, Kowark A, Thudium M. Pupillary Pain Index Predicts Postoperative Pain but Not the Effect of Peripheral Regional Anaesthesia in Patients Undergoing Total Hip or Total Knee Arthroplasty: An Observational Study. Medicina. 2023; 59(5):826. https://doi.org/10.3390/medicina59050826
Chicago/Turabian StyleKornilov, Evgeniya, Lena Gehlen, Dana Yacobi, Martin Soehle, Ana Kowark, and Marcus Thudium. 2023. "Pupillary Pain Index Predicts Postoperative Pain but Not the Effect of Peripheral Regional Anaesthesia in Patients Undergoing Total Hip or Total Knee Arthroplasty: An Observational Study" Medicina 59, no. 5: 826. https://doi.org/10.3390/medicina59050826